


Abstract
18F-FDG PET/CT has demonstrated substantial value in systemic staging of newly diagnosed breast cancer in women. However, it is not known whether breast cancer in male patients benefits similarly. This study assesses 18F-FDG PET/CT systemic staging in patients with newly diagnosed male breast cancer and determines detection rates for unsuspected distant metastases stratified by pre-PET/CT stage. Methods: In this Institutional Review Board–approved retrospective study, our Health Care Information System was screened for stage I–III male patients with breast cancer who underwent 18F-FDG PET/CT before systemic or radiation therapy from 2004 to 2017. Initial stage was determined by mammography, ultrasound, or surgery. 18F-FDG PET/CT was evaluated to identify unsuspected extraaxillary regional nodal and distant metastases, and a post-PET/CT stage was determined. Rates of upstaging to stage IV were determined for each initial stage. Results: During the 14-y period, 10,124 unique patients underwent 18F-FDG PET/CT for breast cancer at our institution. Of these, 106 patients were men, and 39 of these patients were imaged at initial staging and met the inclusion criteria. Median age was 62 y (range, 31–90 y), most had ductal carcinoma (95%), and most were estrogen receptor–positive (97%). In 7 of 39 patients (18%), 18F-FDG PET/CT identified previously unsuspected distant metastases, which increased patient stage to IV. This included 3 of 19 (16%) initial stage IIB patients and 4 of 12 (33%) initial stage III patients. 18F-FDG PET/CT also detected an unsuspected synchronous lymphoma in 1 patient. Conclusion: 18F-FDG PET/CT revealed previously unsuspected distant metastases in 16% of male patients with pre-PET/CT stage IIB breast cancer and 33% of those with stage III breast cancer. These rates are comparable to previously published upstaging rates in female patients. 18F-FDG PET/CT demonstrates value for systemic staging of male patients with breast cancer and should be considered for use in newly diagnosed patients, particularly those with stage IIB and III disease.
PET/CT with 18F FDG has proven clinical value in appropriately selected women with breast cancer, including for the detection of unsuspected extraaxillary regional nodal metastases and distant metastases in patients with newly diagnosed breast malignancy (1–6). This is reflected in National Comprehensive Cancer Network guidelines, which consider systemic staging with 18F-FDG PET/CT for patients with newly diagnosed stage III breast cancer (7). However, these guidelines are predominantly based on cohorts of female patients, as breast cancer is far more common among women. There is still limited information regarding the value of 18F-FDG PET/CT for male breast cancer (8–10), and no sex-specific recommendations or guidelines have been issued for the use of 18F-FDG PET/CT for initial staging of breast cancer (7,11).
Although there are many similarities between breast cancer in women and men, there are also several notable differences. Breast cancer is uncommon in men, accounting for only 1% of all breast cancers (11,12). As there are no screening guidelines for the detection of breast cancer in men, male breast cancer is often detected at more advanced stages than in women (13). At initial detection, male breast cancers are larger than those in women and nodal involvement is more common (13). Male breast cancers are also more commonly higher grade than breast cancers in women (14). Male breast cancers are almost always ductal in histology, whereas in women about 15% are lobular in histology (15,16). This is significant, as lobular breast malignancies and their metastases are less 18F-FDG–avid than ductal malignancies (17–22), and 18F-FDG PET/CT may have less impact on the systemic staging of lobular breast cancers (22). Male breast cancers are almost always estrogen receptor (ER)–positive; in women, about 80% are ER-positive. This is significant, as ER-positive tumors have been shown to demonstrate lower 18F-FDG avidity (23–25). These epidemiologic and biologic differences may affect the value of 18F-FDG PET/CT in male breast cancer as compared with female breast cancer.
Given the rarity of male breast cancer, it is not surprising that data on the use of 18F-FDG PET/CT are limited (8–10). Groheux et al. reported on 18F-FDG PET/CT in 15 men with breast cancer (9). Seven of these patients were evaluated at initial diagnosis, and among these, 2 demonstrated lesions suggestive of distant metastases. Evangelista et al. evaluated 25 men with breast cancer who underwent 18F-FDG PET/CT. Five of these patients were scanned at initial diagnosis. By report, osseous lesions were seen in 2 patients. Vatankulu et al. discussed 15 male breast cancer patients, all of whom underwent 18F-FDG PET/CT for initial staging. Again, 2 patients had lesions suggestive of distant metastases. In none of these cohorts was pre-PET/CT stage reported or histologic proof provided for the suspected distant metastases.
Given the lack of data and the absence of guidelines for 18F-FDG PET/CT in the initial staging of male breast cancer, an analysis of the value of 18F-FDG PET/CT for systemic staging of male breast cancer is warranted. In this manuscript, we retrospectively reviewed the database of a large cancer center to evaluate the value of 18F-FDG PET/CT in patients with male breast cancer, categorized the rate of distant metastasis detection by pre-PET stage, and demonstrated histologic proof for lesions suggestive of distant metastases.
MATERIALS AND METHODS
Study Design and Patients
This retrospective single-institution study was performed in compliance with the Health Insurance Portability and Accountability Act and with Institutional Review Board approval. The requirement to obtain informed consent was waived. The Memorial Sloan Kettering Cancer Center Health Care Information System was screened for patients with male breast cancer who underwent 18F-FDG PET/CT between January 2004 and December 2017, before beginning treatment with chemotherapy, hormonal therapy, or radiation therapy. Electronic medical records were reviewed, and patients with the following characteristics were excluded: known stage IV disease for the current malignancy before 18F-FDG PET/CT, symptoms suggestive of metastatic disease, prior or concurrent malignancies (except nonmelanoma skin cancer), or systemic therapy or radiation before 18F-FDG PET/CT. Surgical management of the primary breast lesion and axillary nodes was allowed. Age at diagnosis and race were recorded for each patient. Histology and grade, as well as ER, progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) receptor status were recorded for each primary tumor. Criteria for ER-positive (ER+) and HER2-positive (HER2+) immunohistochemistry and in situ hybridization were based on the recommendations of the American Society of Clinical Oncology (26,27). Tumors with positive immunochemistry for ER or PR, as well as negative for HER2, were defined as ER+/HER2-negative (HER2−) tumors. Tumors with positive immunochemistry or in situ hybridization for HER2, regardless of status of estrogen or PR, were defined as HER2+. Tumors negative for all 3 receptors were classified as triple-negative. The presence or absence of a BRCA1 or BRCA2 mutation was recorded, if known. Survival data were recorded from all patients using the Memorial Sloan Kettering Cancer Center Health Care Information System to document whether the patient was alive at each follow-up appointment and if there was a date of death.
Determination of Initial Pre-PET/CT Stage
Initial stages were determined according to the seventh edition of the American Joint Committee on Cancer Staging Manual (28). Initial clinical stage was determined from physical examination, mammography, breast ultrasound, or surgical findings.
PET/CT Imaging and Interpretation
All patients in this retrospective study underwent 18F-FDG PET/CT before systemic or radiation therapy. Before 18F-FDG injection for PET/CT, patients fasted for at least 4–6 h. Each patient was injected intravenously with 444–555 MBq of 18F-FDG when plasma glucose was less than 200 mg/dL. After 18F-FDG injection, patients rested for a scheduled 60-min uptake period followed by image acquisition on one of several GE Healthcare Discovery PET/CT systems. PET/CT scans were acquired with the patient supine, from the midskull to the midthigh. In most cases, low-dose CT scans with oral contrast were obtained. Occasionally, intravenous contrast was administered. Images were reviewed on a PACS (GE Healthcare), displaying a maximum-intensity-projection image and multiplanar PET, CT, and PET/CT fusion images. According to standard 18F-FDG PET/CT reporting, uptake was considered abnormal when it was focal, was not considered physiologic or inflammatory, and had intensity greater than the local background. Suspicion for malignancy was based on the integration of metabolic information from the PET images and anatomic information from the CT images and fused PET/CT images. PET/CT studies were reinterpreted by a radiologist dually boarded in diagnostic radiology and nuclear medicine with 13 y of PET/CT experience. Evidence of unsuspected regional extraaxillary nodal metastases and distant metastases were recorded, and if they were noted on imaging, then a new post-PET/CT stage was assigned.
Verification of Metastases
Histology was the preferred method to verify malignancy for 18F-FDG PET/CT findings. When histology was not available, follow-up imaging was used. Lesions had to show typical features of metastatic disease on initial imaging and show progression or response to treatment on follow-up imaging. Time interval between 18F-FDG PET/CT and reference standard test (biopsy or follow-up imaging) was determined.
Statistical Analysis
Medians and ranges were used to summarize continuous variables and frequencies, and percentages were used to summarize categoric variables, including distant metastases and upstaging. Race was grouped into African American, Asian, Caucasian, and other. Upstaging rates were provided by pre-PET stage along with binomial confidence intervals. The associations between clinical characteristics and upstaged to stage 4 status were assessed with the Fisher exact test and the Wilcoxon rank-sum test, where appropriate. Overall survival (OS) was calculated from time of PET scan until death. Patients alive at last follow-up were censored. OS was estimated with Kaplan–Meier methods. Two sided P values less than 0.05 were considered statistically significant, and all analyses were performed using SAS 9.4 (The SAS Institute).
RESULTS
Characteristics of Patients and Primary Breast Malignancies
Our search of the Memorial Sloan Kettering Cancer Center Health Care Information System from 2004 to 2017 identified 10,124 unique patients who had undergone 18F-FDG PET/CT for breast cancer, 106 of whom were men. Of these 106 patients, 67 were excluded for systemic or radiation therapy before 18F-FDG PET/CT, known stage IV disease before 18F-FDG PET/CT, or history of a prior malignancy. This left a cohort of 39 patients who met all inclusion and exclusion criteria. A Standards for Reporting of Diagnostic Accuracy Diagram for patients in this study is provided in Figure 1.

Standards for Reporting of Diagnostic Accuracy Diagram (STARD) for patients in this study. MSKCC = Memorial Sloan Kettering Cancer Center.
The median age of the final cohort of 39 patients with male breast cancer was 62 y (range, 31–90 y). Of these 39, 37 primary breast malignancies (95%) were ductal in histology and 38 of 39 (97%) of primary breast malignancies were ER+. As 5 of these malignancies were also HER2+, they were categorized as HER2+ tumors, whereas the 33 ER+ tumors that were negative for HER2 were categorized as ER+/HER2−. One tumor was triple-negative for ER, PR, and HER2. Patient and tumor demographics, including age, race, histology, tumor grade, receptor classification, and initial pre-PET/CT clinical stage, are summarized in Table 1.
Characteristics of Patients with Male Breast Cancer and Their Primary Tumors
Detection of Unsuspected Metastases by 18F-FDG PET/CT
18F-FDG PET/CT demonstrated findings suggestive of unsuspected distant metastases in 7 of 39 (18%, 95% confidence interval: 8%–34%) patients with male breast cancer (Figs. 2 and 3). Suspected metastatic sites included bone in 6, lung in 3, and distant nodal metastases in 3 patients. Four patients had metastatic disease involving more than one organ site. For 5 of 7 patients with 18F-FDG PET/CT findings suggestive of unsuspected distant metastases, metastases were confirmed by pathology. The time intervals between suspicious 18F-FDG PET/CT findings and pathologic confirmation in these 5 patients were 2, 7, 21, 27, and 64 d (median, 26 d). In the remaining 2 patients, metastatic disease was confirmed by follow-up imaging demonstrating resolution of 18F-FDG avidity in osseous lesions and new osseous sclerosis, consistent with treatment response to therapy and osseous healing (Fig. 3). The time interval between suspicious 18F-FDG PET/CT findings and follow-up imaging confirmation in these 2 patients was 94 and 123 d.
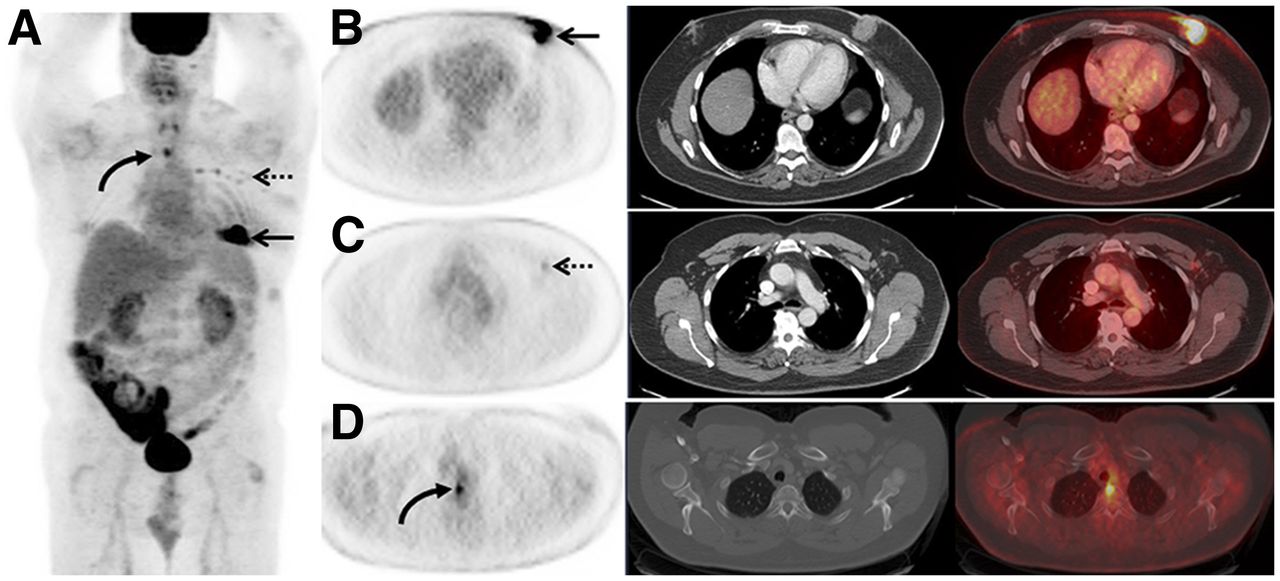
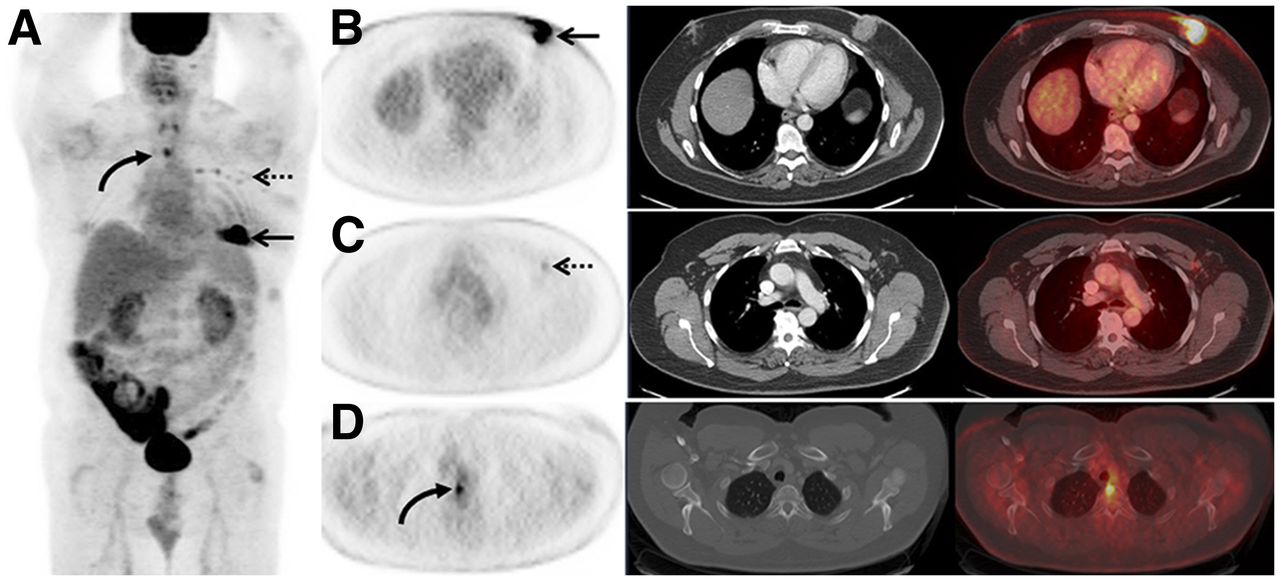
A 53-y-old man with a pre-PET/CT stage IIB breast cancer, which was upstaged to stage IV by 18F-FDG PET/CT. (A) 18F-FDG maximum-intensity-projection image demonstrates 18F-FDG avidity in left breast (arrow), left axilla (dashed arrow), as well as overlying midline chest (curved arrow). (B) Axial 18F-FDG PET, CT on soft-tissue window, and fused 18F-FDG PET/CT demonstrate the 18F-FDG–avid known primary left breast malignancy (arrow). (C) Axial 18F-FDG PET, CT on soft-tissue window, and fused 18F-FDG PET/CT demonstrate 18F-FDG–avid known left axillary nodal metastases (dashed arrow). (D) Axial 18F-FDG PET, CT on bone window, and fused 18F-FDG PET/CT demonstrate 18F-FDG avidity in midline chest on the maximum-intensity-projection image corresponding to a thoracic vertebra without CT correlate. This lesion was biopsied and proven to be a previously unsuspected osseous metastasis, increasing patient’s stage to IV. This altered patient’s management from surgical management to systemic therapy without surgical management.

A 58-y-old man with a pre-PET/CT stage IIB breast cancer, which was upstaged to stage IV on 18F-FDG PET/CT. (A) 18F-FDG maximum-intensity-projection image demonstrates mild 18F-FDG avidity in left mastectomy bed (arrow) and left axillary node (dashed arrow), as well as overlying midline chest (curved arrow). (B) Axial 18F-FDG PET, CT on bone window, and fused 18F-FDG PET/CT demonstrate an 18F-FDG–avid thoracic vertebra (curved arrow) corresponding only with small, benign-appearing sclerotic focus on CT. This patient was subsequently treated with systemic therapy. (C) Axial 18F-FDG PET, CT on bone tissue window, and fused 18F-FDG PET/CT after systemic therapy demonstrate resolution of 18F-FDG avidity (curved arrow) and increased sclerosis of the vertebra (white arrow), consistent with therapy response in an osseous metastasis and osseous healing. (D) 18F-FDG maximum-intensity-projection image after systemic therapy demonstrates persistence of 18F-FDG–avid postmastectomy inflammation (arrow) but resolution of avidity in the node and osseous metastasis.
Stratified by pre-PET/CT clinical stage, 18F-FDG PET/CT demonstrated metastases in 0 of 8 (0%) patients with pre-PET/CT stage I or IIA, 3 of 19 (16%) patients with pre-PET stage IIB, and 4 of 12 (33%) patients with pre-PET/CT stage III male breast cancer (Table 2). Ninety-five percent confidence intervals for upstaging to distant metastatic disease were 4%–40% for patients with pre-PET stage IIB and 10%–65% patients with pre-PET stage III disease.
Summary of Patients with Male Breast Cancer Upstaged by 18F-FDG PET/CT Stratified by Pre-PET/CT Stage
In no patients were unsuspected extraaxillary nodal metastases identified that resulted in a new post-PET/CT stage. No false-positives were noted for distant metastases among the patients with male breast cancer. Patients in this study were not downstaged by PET/CT results.
Associations Between Clinical Parameters and Upstaging
No significant differences were found between patients who were upstaged compared with those who were not for age (median, 56 y; range, 44–70 vs. median, 66 y; range, 31–90; P = 0.14), race (Caucasian, 86% (6/7) vs. 78% (25/32); P = 0.30), or receptor status (ER+/HER, 2%–100% (7/7) vs. 81% (26/32); P = 0.64). As only 2 patients had nonductal histologies, we did not examine the association between histology and upstaging rate. Additionally, almost half the patients (49%, 19/39) were missing BRCA status, so this was not examined further.
OS
By the end of follow-up, 7 patients had died, with a 1-y OS of 97.1% (95% confidence interval, 80.9%–99.6%) and a 5-y OS of 72.6% (95% confidence interval, 50.2%–86.1%). Median follow-up in survivors was 47.3 mo (range, 0.4–102.3 mo). As only 7 patients died, we could not formally examine the association between OS and upstaging rates on 18F-FDG PET/CT.
Synchronous Malignancies
18F-FDG PET/CT resulted in the detection of an unsuspected synchronous lymphoma in 1 patient, which was proven by pathology. It was a clinically significant lymphoma for which the patient was subsequently treated.
DISCUSSION
Our retrospective review of patients with male breast cancer demonstrates that 18F-FDG PET/CT detects unsuspected distant metastases at a rate of 16% for initial pre-PET/CT stage IIB disease and 33% for initial pre-PET/CT stage III disease. These rates are comparable to upstaging rates seen in female patients with breast cancer (1–6) and suggest a role for 18F-FDG PET/CT in the initial staging of male patients with breast cancer, particularly for those with stage IIB–III disease based on physical examination, mammography, and ultrasound. The detection of unsuspected distant metastatic disease by 18F-FDG PET/CT in these patients will increase the correct characterization of initial stage IV disease, which will result in substantial altering of treatment strategy and prognosis.
The probable impact of systemic staging with 18F-FDG PET/CT can be seen in Figures 2 and 3. The patient in Figure 1 was initially stage IIB and underwent 18F-FDG PET/CT at initial staging, before any therapy. 18F-FDG PET/CT revealed unsuspected distant metastases, and thus stage IV disease. The treatment plan for this patient was changed from surgical management to systemic therapy without surgical management. The patient in Figure 2 was also initially stage IIB and underwent 18F-FDG PET/CT after mastectomy but before further systemic or radiation therapy. 18F-FDG PET/CT reveled unsuspected distant metastases, and thus stage IV disease. If the 18F-FDG PET/CT had been performed before mastectomy, surgical management may have been foregone in lieu of systemic therapy.
No patients with stage I–IIA disease were found to have unsuspected distant metastases. Although the numbers of stage I–IIA patients were small, this is consistent with the low levels of upstaging in female patients with stage I–IIA breast malignancies (1–6). Avoiding 18F-FDG PET/CT in these early-stage patients may help maximize the clinical utility of 18F-FDG PET/CT. Even if the patient is presumed to be only stage I or IIA, signs or clinical symptoms that suggest metastatic disease may still warrant systemic staging, and the role of 18F-FDG PET/CT in this situation has not been evaluated.
In this study, there were no false-positive findings for distant metastases on 18F-FDG PET/CT. Low rates of false-positives for distant metastases have been reported in prior studies of 18F-FDG PET/CT for female patients with breast cancer (29). The low rate of false-positive findings is supported by the high proportion of pathologic proof of distant metastases in our cohort. Only 2 patients with 18F-FDG PET/CT findings suggestive of distant metastases were not pathologically proven, and these had confirmation from follow-up imaging demonstrating resolution of 18F-FDG avidity after therapy and new osseous sclerosis representing healing of metastases (Fig. 2).
Unsuspected synchronous additional malignancies have been detected on 18F-FDG PET/CT studies at rates of 1%–2% (30,31). One of the 39 patients in this study had an unsuspected synchronous malignancy on the 18F-FDG PET/CT study performed for systemic staging of primary breast cancer, and this case was pathologically proven.
The study has several limitations. The retrospective single-institution study design lends itself to biases, for example, why these patients were initially selected to undergo 18F-FDG PET/CT. The potential for selection biases, including the possibility of unappreciated data that raises the risk of distant metastases, is inherent in retrospective studies. The number of patients in the cohort was small, limiting statistical analyses. However, male breast cancer is an uncommon malignancy and compared with prior available data, the number of male patients with breast cancer who underwent 18F-FDG PET/CT at initial staging was high and pathologic proof of PET/CT findings was available in most cases. This allowed for an evaluation of upstaging rates based on pre-PET/CT stage, which was previously unavailable. An evaluation of survival was planned for patients with male breast cancer; however, there were too few deaths in the cohort to conduct formal survival comparisons.
CONCLUSION
18F-FDG PET/CT revealed previously unsuspected distant metastases in 16% of male patients with stage IIB breast cancer and in 33% of male patients with stage III breast cancer. This demonstrates the potential value of 18F-FDG PET/CT for systemic staging at initial diagnosis of male breast cancer, particularly for patients with stage IIB and III disease.
DISCLOSURE
This research was funded in part through the Susan G. Komen for the Cure Research Grant KG110441 (Gary A. Ulaner) and the NIH/NCI Cancer Center Support Grant P30 CA008748 (Biostatistics Core). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Jane Howard, Department of Medicine, Memorial Sloan Kettering Cancer Center, for database assistance and Leah Bassity, Department of Radiology, Memorial Sloan Kettering Cancer Center, for manuscript assistance.
Footnotes
Published online Sep. 20, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 16, 2018.
- Accepted for publication September 10, 2018.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.