


Abstract
In patients with suspected but yet not localized neuroendocrine tumors (NETs), early diagnosis or reliable exclusion is crucial for optimal individual prognosis and therapy. Despite recourse to several imaging modalities, the definite diagnosis of NET can be challenging. Therefore, we tested 68Ga-DOTATATE PET/CT as a tool for improved diagnosis in a cohort of patients with suspected, nonlocalized NET. Methods: 68Ga-DOTATATE PET/CT recordings were obtained in 104 consecutive patients meeting at least one of the following criteria: clinical suspicion of NET (n = 70), elevated blood levels of tumor markers (n = 49), and image-based suspicion of NET (n = 53). The presence of NET was validated by histopathology (n = 49) or clinical follow-up of 107 ± 59 wk (n = 55). Results: In 36 of 104 patients (35%), NET was histologically verified, most frequently located in the small bowel (10/36), pancreas (8/36), lung (5/36), and stomach (2/36). Twelve patients had tumors of nonneuroendocrine origin, and 7 patients had benign tumors. 68Ga-DOTATATE PET/CT identified NET in 29 of the 36 cases and excluded the presence of a NET in 61 of the 68 non-NET patients, indicating a sensitivity of 81% and specificity of 90%. The PET/CT gave a false-positive result in 7 patients and a false-negative in another 7 patients, indicating positive and negative predictive values of 81% and 90%, respectively, and an accuracy of 87%. Chromogranin A levels were significantly higher in both PET-positive patients (1,841 vs. 342 ng/mL; P < 0.05) and patients with verified NET (2,214 vs. 524 ng/mL; P < 0.05). Conclusion: In patients with suspected NETs due to clinical symptoms, elevated levels of tumor markers, or indeterminate tumors suggestive of NET, 68Ga-DOTATATE PET/CT is highly accurate, thus supporting its use in clinical routine diagnostics.
Neuroendocrine tumors (NETs) are a heterogeneous class of relatively rare tumors that are of increasing incidence, possibly reflecting improved diagnostics (1). Because neuroendocrine cells are present in almost every organ, a primary NET can likewise arise in almost any tissue. Despite their lineage, most NETs do not secrete hormones (2), such that the particular symptoms caused by a given NET are often unspecific, such as abdominal discomfort arising from mass effects. Even typical endocrine symptoms of NET such as diarrhea or flushing are by no means NET-specific. Early diagnosis is mandatory for successful treatment, because the size of the primary NET (at least those in the relatively common jejuneal/ileal site) correlates with the occurrence of lymph node involvement (3). However, the subtle and ambiguous clinical manifestations of NETs can frequently hamper a timely and accurate diagnosis, despite recourse to modern laboratory diagnostics. In particular, elevated levels of chromogranin A (CgA), which is widely expressed by neuroendocrine cells, give a sensitivity of approximately 70%–85% in patients with known NET (4–6). However, elevated CgA is not sufficient for diagnosis, because it can arise from treatment with proton pump inhibitors, atrophic gastritis, renal insufficiency, and numerous other conditions (7,8).
The diagnosis of suspected NET is facilitated through the use of modalities such as CT, MRI, gastroscopy, colonoscopy, and endosonography. More specific NET detection exploits a biochemical characteristic of the cell type: high expression of somatostatin receptors (SSTR). This expression enables imaging with high sensitivity using PET with radioactively labeled somatostatin analogs such as 68Ga-DOTATATE (9,10). PET with 68Ga-labeled somatostatin ligands is well established as a tool for localizing the primary tumor in metastatic NET (11) and, thus, is recommended by a recent guideline from the European Neuroendocrine Tumor Society (12). However, there are currently no data available regarding its diagnostic value in patients with suspected NET.
In the present study, we aimed to evaluate 68Ga-DOTATATE PET in patients with clinically suspected NET, using present symptoms, elevated levels of CgA, or the presence of a suspected mass in conventional imaging. We hypothesized that 68Ga-DOTATATE PET should detect NET lesions with a high sensitivity in this patient group. We further hypothesized that negative PET results should exclude with considerable certainty the presence of NET.
MATERIALS AND METHODS
Study Population
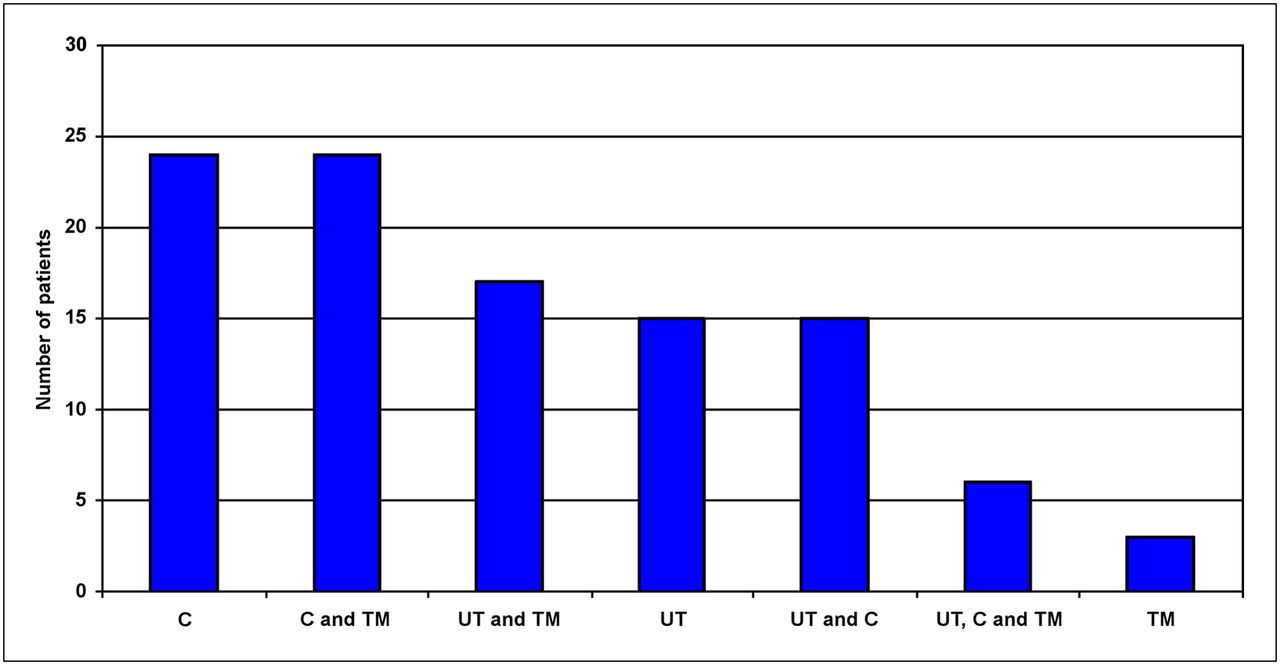
Consecutive patients (n = 104) referred for imaging during 2006–2011 were retrospectively included (52 men, 52 women; mean age ± SD, 58 ± 16 y [age range, 1–83 y]). Seventy patients were examined by PET primarily because of the clinical suspicion of NET on the basis of symptoms such as persistent diarrhea or flushing, 49 patients because of elevated levels of tumor markers, and 53 patients because of a mass suggestive of NET. Most patients presented with more than one of these findings, as indicated—along with other patient demographics—in Table 1 and Figure 1. Three patients were examined because of an isolated CgA or neuron-specific enolase elevation; all other patients with elevated tumor markers had either additional clinical symptoms (n = 30) or a suspected tumor (n = 21). The patients with clinical symptoms most often experienced diarrhea (n = 25; mean, 10/d; range, 3–20/d), flushing (n = 13), elevation of adrenocorticotropic hormone without adenoma of the pituitary gland (n = 10), severe hypoglycemia (n = 7), and various other symptoms (n = 19; e.g., osteomalacia with the suspicion of a phosphaturic tumor, suspicion of gastrinoma, or abdominal cramping).
Patient and Tumor Characteristics of Study Cohort (n = 104)

Number of patients presenting with clinical symptoms, elevated levels of tumor markers, and indeterminate tumor. C = clinical symptoms; TM = elevated levels of tumor markers; UT = indeterminate tumor.
In all but 4 patients without a mass suggestive of NET, information about prior examinations was available; these patients had a median of 2 (range, 0–6) prior examinations, including modalities such as ultrasound, CT, MRI, and endoscopy, without evidence of NET. The presence or absence of NET was confirmed by histopathology (n = 49) or by follow-up examinations (n = 55), with a mean (±SD) follow-up of 107 ± 59 wk.
PET Scans
In accordance with German law, 68Ga-DOTATATE was applied as an off-label use on compassionate grounds until 2009. German federal law has since changed such that 68Ga-DOTATATE is covered under the conditions of §13 2b pharmaceutical law, in agreement with the regulatory bodies. All patients, including those examined before 2009, had provided written, informed consent.
68Ga-DOTATATE was prepared as described previously (13). Whole-body PET scans were acquired in 3-dimensional mode using a Biograph 64 TruePoint (Siemens Medical Solutions) or a Discovery 64-slice PET/CT scanner (GE Healthcare). The emission recording sequence was initiated 60 min after intravenous injection of 200 MBq of 68Ga-DOTATATE (except 1 child, who received 50 MBq), as in previous studies (14,15). Emission data were reconstructed with attenuation correction using concurrent diagnostic CT. Two experienced nuclear medicine specialists evaluated the PET images for the presence or absence of NET by consensus. A dedicated software package (Hermes Hybrid Viewer; Hermes Medical Solutions) was used to interpret side-by-side images and view fused PET/CT images. PET images were evaluated visually for regions of pathologically increased tracer uptake that could not be attributed to normal physiologic activity. CT data were used for allocation of regions with increased radiopharmaceutical uptake to specific structures. The readers were aware of the patients’ clinical history.
Statistical Analysis
Values are presented as mean ± SD unless stated otherwise. For comparison of tumor marker levels, the Student t test was used. Multiple receiver-operating-characteristic curve analyses were conducted for the detection of optimal CgA and neuron-specific enolase thresholds.
RESULTS
Diagnosis of NET
The histologic verification of NET was made in 36 of 104 patients (35%). The most frequent locations were the small bowel (10 patients), pancreas (8 patients), lung (5 patients), and stomach (2 patients) (Table 1). Tumors were classified as non-NET in 12 patients and as benign in 7 patients.
68Ga-DOTATATE PET/CT identified 29 of 36 NETs, giving a sensitivity of 81%, and excluded the presence of a NET in 61 of 68 patients, giving a specificity of 90%. PET/CT gave a false-positive result in 7 patients, indicating a positive predictive value of 81%, and gave a false-negative result in another 7 patients, indicating a negative predictive value of 90% (Figs. 2 and 3). The detailed characteristics of the 14 patients with false-positive or -negative PET/CT results are reported in Table 2.
Patients with Incorrect Diagnoses Resulting from 68Ga-DOTATATE PET/CT Findings
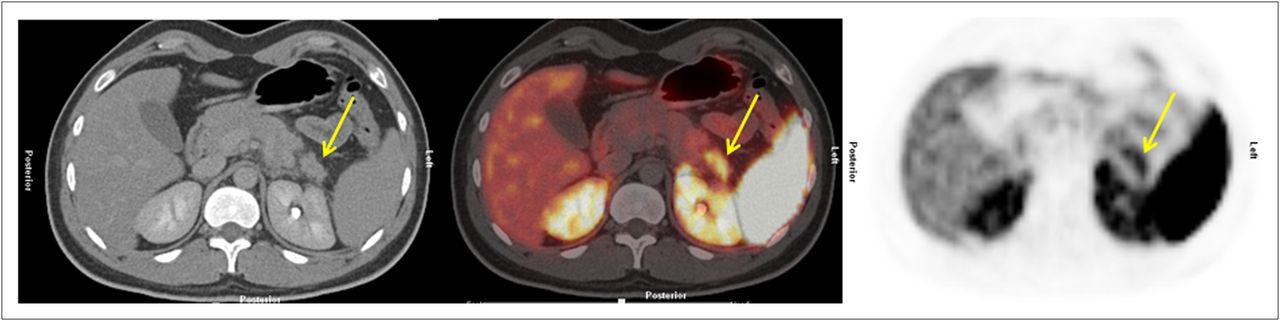
False-positive PET result in 23-y-old man with pancreatic NET suspected because of indeterminate mass in pancreatic tail and enhanced uptake of 68Ga-DOTATATE (arrow). Patient underwent surgical removal of suspected tumor, which was confirmed on histopathologic examination to be chronic pancreatitis with no evidence of NET. Left image is CT, middle image is PET/CT; right image is PET.

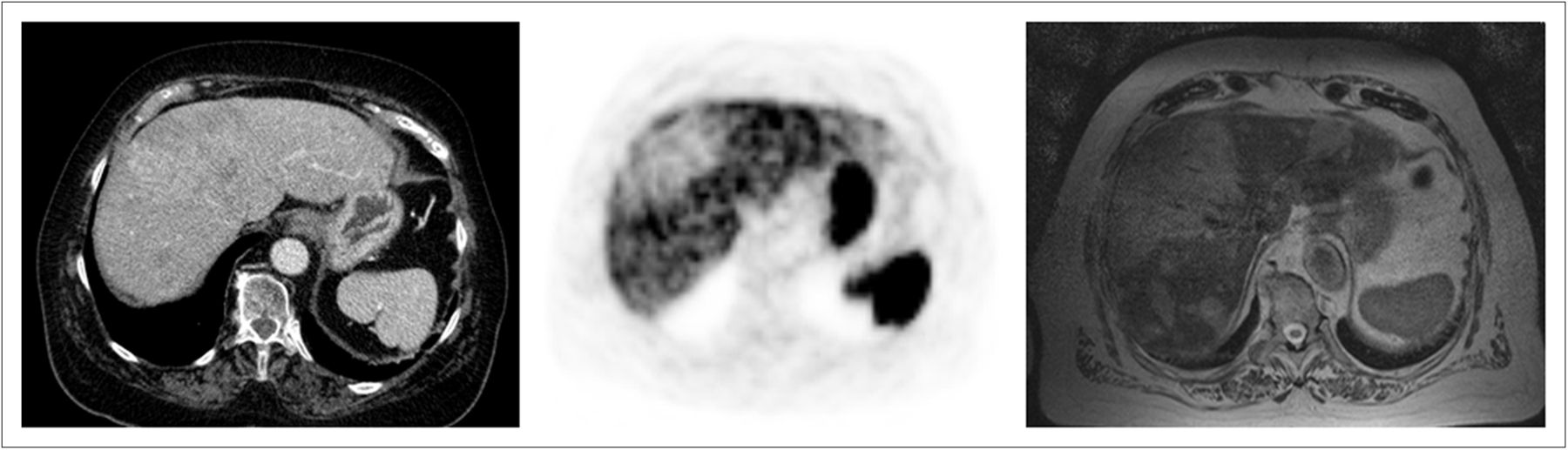
False-negative PET result in 77-y-old woman with Cushing syndrome due to ectopic adrenocorticotropic hormone syndrome. In the 3 phases of CT (left, portal-venous phase), perfusion inhomogeneities led to suspicion of hepatic metastases. On PET (middle), hepatic lesions took up less 68Ga-DOTATATE than did liver parenchyma. Therefore, metastases were judged as non-NET. On MRI (right, T2-weighted), disseminated hepatic metastases were clearly delineated. Histopathologic verification revealed atypical carcinoid with intermediate proliferation rate (Ki-67, 5%) and immunohistochemical expression of adrenocorticotropic hormone.
Diagnostic Accuracy and Patient Subgroups
The diagnostic accuracy for the 3 predefined patient subgroups was within the same range (Fig. 4). Seventy patients had a suspected NET because of the presence of clinical symptoms such as diarrhea or flushing. Of these, 21 (30%) had a proven NET. In this subgroup, 68Ga-DOTATATE PET/CT thus showed a sensitivity of 86% (18/21 patients) and a specificity of 90% (44/49 patients).

In patients with suspected NET, accuracy of 68Ga-DOTATATE PET/CT findings stratified according to clinical symptoms (n = 70), elevated levels of tumor markers (n = 49), and tumor suggestive of NET (n = 53). C = clinical symptoms; NPV = negative predictive value; PPV = positive predictive value; TM = elevated levels of tumor markers; UT = indeterminate tumor.
Of the 49 patients with elevated tumor markers (43 with increased CgA or 13 with increased neuron-specific enolase), 16 (40%) had histologically proven NET. In this patient group, 68Ga-DOTATATE PET/CT thus showed a sensitivity of 81% (13/16 patients) and a specificity of 88% (29/33 patients). Of the 43 patients with elevated CgA levels, 12 (29%) had histologically proven NET. CgA levels were significantly higher in patients with a positive PET scan result (1,841 vs. 342 ng/mL; P < 0.05) and patients with verified NET (2,214 vs. 524 ng/mL; P < 0.05). However, using receiver-operating-characteristic curve analyses, we could not establish satisfactory CgA (area under the curve, 0.59 and 0.52) or neuron-specific enolase (area under the curve, 0.55 and 0.50) thresholds indicative of NET or a positive PET/CT result.
In 53 patients, an indeterminate tumor suggestive of NET had been found by previous imaging examinations, most often with CT or ultrasound. In most cases, these suspected tumors were in the pancreas (Fig. 5) or the liver or presented as an abdominal mass (Table 1). Of this group, 22 (42%) had a proven tumor of neuroendocrine differentiation, such that 68Ga-DOTATATE PET/CT had a sensitivity of 81% (18/22 patients) and specificity of 84% (26/31 patients). Of the remaining 31 of 53 patients with initially suspected NET, the final diagnoses were pancreatic cancer (n = 3), hepatocellular cancer (n = 3), metastasis of renal carcinoma (n = 1), gastrointestinal stromal tumor (n = 1), and a gynecologic tumor (most probably ovarian carcinoma; n = 1). This left 22 patients in whom no malignancy was detected. The final diagnosis was verified by histopathology in 29 of the 53 patients with suspected NET.

A 28-y-old woman with multiple endocrine neoplasia type 1 and unclear lesion on endosonography (without hypervascularization) in pancreatic head. Tumor markers (including glucagon and blood glucose levels) were within normal levels. Focus of intense uptake of 68Ga-DOTATATE (left, PET; right, fused PET/CT) in pancreatic head without morphologic abnormalities on CT (middle) was present. Histopathologic examination proved evidence of G1 glucagonoma smaller than 10 mm.
One child (age, 21 mo) who had experienced recurrent life-threatening episodes of hypertension and vomiting with the suspicion of a hormone-secreting tumor was examined with 50 MBq of 68Ga-DOTATATE. Previous MRI examinations of the thorax, abdomen, and cranium; multiple ultrasound examinations; radiography examinations of the abdomen and thorax; and metaiodobenzylguanidine scintigraphy, including SPECT/CT, revealed no evidence of pathologic findings, thus ruling out pheochromocytoma. In this situation with multiple hospitalizations requiring intensive care and without evidence of an underlying tumor, the pediatricians referred the child for a 68Ga-DOTATATE PET/CT scan, which did not depict a hormone-secreting tumor. During follow-up, the diagnosis of a defective hypothalamic or pituitary regulatory circuit was made and additional epilepsy appeared, such that the scan result was rated truly negative.
DISCUSSION
In this first, to our knowledge, report of the diagnostic utility of 68Ga-DOTATATE PET/CT in a patient population with suspected NET, the examination proved to have a sensitivity and positive predictive value of 81%. Only one third of the patients included in the study group proved to have a NET; 68Ga-DOTATATE PET/CT was able to rule out a diagnosis of NET with a specificity and negative predictive value of 90%. These values are notably higher than those reported for octreotide (OctreoScan; Covidien). In a study including 29 patients with suspected pancreatic NET, octreotide had a sensitivity of 54% and a specificity of 81% (16). In another study of 20 patients with the clinical suspicion of gastrinoma or insulinoma, octreotide was of high value in the detection of gastrinomas (sensitivity, 86%) but had a limited sensitivity (14%) in insulinomas (17). Furthermore, in a series of patients with Zollinger–Ellison syndrome, octreotide was more sensitive than conventional imaging methods but missed one third of all surgically confirmed gastrinomas (18). The present encouraging results with 68Ga-DOTATATE PET/CT, if independently confirmed, support its use in the management of patients with NET suspected on the basis of conventional imaging and clinical tests. It is well known that the several 68Ga-labeled somatostatin analogs used for the diagnosis of NETs have different affinities for the SSTRs. However, in studies evaluating the sensitivities and uptake values of 68Ga-DOTATATE versus 68Ga-DOTATOC and of 68Ga-DOTATATE versus 68Ga-DOTANOC, no differences in diagnostic accuracy were found (19,20).
In general, the clinical presentation of NET patients is frequently vague, and the differential diagnoses include a considerable number of other diseases. Furthermore, the diagnosis of NET is challenging per se because of the heterogeneity and the frequent small size of this tumor entity. Up to 14% of all NET cases are incidentally diagnosed postmortem (21), underlining the difficulty in localizing these tumors in vivo. Therefore, it is crucial to have a more reliable imaging method for the initial diagnosis of NET than is afforded by structural imaging methods.
The extent of binding and uptake of SSTR ligands to NET cells strongly depends on their degree of differentiation. Higher-grade NETs and neuroendocrine carcinomas tend to have absent or low SSTR expression, thus leading to a risk of negative PET results. Nonetheless, we encountered in this study only a single NET case with low tracer uptake, which proved to be liver metastases of an atypical carcinoid tumor of intermediate grade (Fig. 4). Patients with high-grade NETs and neuroendocrine carcinomas frequently present with symptoms related to mass effects, as distinct from the endocrine symptoms characteristic of low-grade NET. This may explain the absence of cases of undifferentiated NET that were negative on 68Ga-DOTATATE PET/CT. On the other hand, false-positive findings can sometimes arise from inflammatory changes. Because macrophages also express SSTR subtype 2, inflammation leads to an increased uptake of 68Ga-DOTATATE (22), in turn leading to the use of 68Ga-DOTATATE PET/CT for the investigation of vulnerable coronary plaques (23). In our single patient with inflammatory changes whose 68Ga-DOTATATE PET/CT result was initially suspected of showing pancreatic NET, the result was false-positive (Fig. 2). However, NETs generally present with much higher 68Ga-DOTATATE uptake than that seen in simple inflammatory changes (24).
In clinical routine, CT scans of the thorax and the abdomen are initially performed in patients with suspected NET. Previous studies comparing the diagnostic accuracies of SSTR PET and CT have consistently reported higher specificity of PET. Comparably high sensitivity for CT could be achieved only when multiple contrast medium phases, including the arterial, portal-venous, and venous phases, were imaged (25,26). Furthermore, SSTR PET had a higher sensitivity than any single CT phase in those reports. Another study in patients with known NET reported a higher accuracy for SSTR PET than for CT using late arterial and portal-venous phase (27). Notably, multiphase CT is not usually performed in patients with suspected NET, because the localization of the tumor is unknown. In any case, the sensitivity and specificity of whole-body portal-venous–phase CT alone are inherently lower than those of SSTR PET (11,28). A study by Putzer et al. reports that PET was more sensitive in the diagnosis of bone metastases from NETs than was either CT or bone scintigraphy (29). Two further studies demonstrated that the diagnostic accuracy of SSTR PET was higher than that of CT and MRI in patients mostly with known NET; PET results led to a change of clinical management in 38%–60% of the patients examined (26,30). Thus, the high positive and negative predictive values found in the present 68Ga-DOTATATE PET/CT study of patients with suspected NET are in line with previous findings in various cohorts of known NET patients.
The patients included in the present study had NET suspected on the basis of a variety of symptoms. Most experienced typical but ambiguous neuroendocrine symptoms such as diarrhea or flushing. In this subgroup, the diagnostic accuracy of 68Ga-DOTATATE PET/CT was comparable to that seen in the entire patient cohort. Furthermore, no relevant differences in accuracy were found between the subgroups presenting with elevated tumor markers or imaging-based suspicion of NET. In all of the present suspected NET cases, the PET findings contributed to the patient management decisions by virtue of the localization or exclusion of a present NET (although this issue was indeed not a focus of the present study). However, it is well known from previously published studies that knowledge of the primary tumor site and the extent of metastatic spread markedly influences both the therapeutic strategy and the prognosis of the patient (31).
This study has several limitations, mainly arising from the heterogeneous nature of NETs and their generally slow rate of growth. Despite a mean follow-up of 107 wk, we cannot rule out that patients with 68Ga-DOTATATE PET/CT results judged as negative in the present study may yet develop a detectable NET, perhaps because of the growth of a tumor initially too small for detection. Indeed, 3 of 7 false-negative findings could be attributed to small NET size. We included patients consecutively, such that potential selection bias affecting the results of our study cannot be excluded. However, about one third of our patient cohort had histologically verified NET, a rate that in our experience reflects clinical routine.
CONCLUSION
In patients with NET suspected on the basis of clinical symptoms, elevated levels of tumor markers, or indeterminate tumor masses suggestive of NET, 68Ga-DOTATATE PET/CT proved to have high accuracy. Our findings support its use in clinical routine diagnostics and substantiate the need for larger prospective trials with this agent.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
A substantial part of this work originated from the doctoral thesis of Ramona Cindea-Drimus. We thank Dr. Paul Cumming for critical revisions of the manuscript. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 14, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 15, 2011.
- Accepted for publication June 5, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Primary neuroendocrine tumour of the extrahepatic biliary duct
- Dual Somatostatin Receptor/18F-FDG PET/CT Imaging in Patients with Well-Differentiated, Grade 2 and 3 Gastroenteropancreatic Neuroendocrine Tumors
- Quantitative 3D Assessment of 68Ga-DOTATOC PET/MRI with Diffusion-Weighted Imaging to Assess Imaging Markers for Gastroenteropancreatic Neuroendocrine Tumors: Preliminary Results
- Evaluating the Role of Theranostics in Grade 3 Neuroendocrine Neoplasms
- Pleuropulmonary tuberculosis with spinal lesions due to metastatic malignancy differentiated definitively on imaging
- The Impact of Somatostatin Receptor-Directed PET/CT on the Management of Patients with Neuroendocrine Tumor: A Systematic Review and Meta-Analysis
- 68Ga-DOTATATE PET/CT Interobserver Agreement for Neuroendocrine Tumor Assessment: Results of a Prospective Study on 50 Patients
- Comparison of the Impact of 68Ga-DOTATATE and 18F-FDG PET/CT on Clinical Management in Patients with Neuroendocrine Tumors
- 68Ga-DOTATATE Compared with 111In-DTPA-Octreotide and Conventional Imaging for Pulmonary and Gastroenteropancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis
- The Impact of 68Ga-DOTATATE PET/CT Imaging on Management of Patients with Neuroendocrine Tumors: Experience from a National Referral Center in the United Kingdom
- Superiority of [68Ga]-DOTATATE PET/CT to Other Functional Imaging Modalities in the Localization of SDHB-Associated Metastatic Pheochromocytoma and Paraganglioma
- 64Cu-DOTATATE PET for Neuroendocrine Tumors: A Prospective Head-to-Head Comparison with 111In-DTPA-Octreotide in 112 Patients
- Can Complementary 68Ga-DOTATATE and 18F-FDG PET/CT Establish the Missing Link Between Histopathology and Therapeutic Approach in Gastroenteropancreatic Neuroendocrine Tumors?
- GEP-NETS update: Functional localisation and scintigraphy in neuroendocrine tumours of the gastrointestinal tract and pancreas (GEP-NETs)
- Promises of Cyclotron-Produced 44Sc as a Diagnostic Match for Trivalent {beta}--Emitters: In Vitro and In Vivo Study of a 44Sc-DOTA-Folate Conjugate
- Interrogating Tumor Metabolism and Tumor Microenvironments Using Molecular Positron Emission Tomography Imaging. Theranostic Approaches to Improve Therapeutics