


Abstract
6-18F-fluoro-l-dopa (18F-FDOPA) measured with PET as a biomarker of amino acid uptake has been investigated in brain tumor imaging. The aims of the current study were to determine whether the degree of 18F-FDOPA uptake in brain tumors predicted tumor grade and was associated with tumor proliferative activity in newly diagnosed and recurrent gliomas. Methods: Fifty-nine patients (40 men, 19 women; mean age ± SD, 44.4 ± 12.3 y) with newly diagnosed (n = 22) or recurrent (n = 37) gliomas underwent 18F-FDOPA PET perioperatively. Tumor tissue was obtained by resection or biopsy in all patients. The tumor grade and Ki-67 proliferation index were obtained by standard pathology assays. Tumor 18F-FDOPA uptake was quantified by determining various standardized uptake value (SUV) parameters (mean SUV, maximum SUV [SUVmax], mean values of voxels with top 20% SUVs, and tumor–to–normal-brain tissue ratios) that were then correlated with histopathologic grade and Ki-67 proliferation index. Results: Fifty-nine lesions in 59 patients were analyzed. 18F-FDOPA uptake was significantly higher in high-grade than in low-grade tumors for newly diagnosed tumors (SUVmax, 4.22 ± 1.30 vs. 2.34 ± 1.35, P = 0.005) but not for recurrent tumors that had gone through treatment previously (SUVmax, 3.36 ± 1.26 vs. 2.67 ± 1.18, P = 0.22). An SUVmax threshold of 2.72 differentiated low-grade from high-grade tumors, with a sensitivity and specificity of 85% and 89%, respectively, using receiver-operating-characteristic curve analysis (area under the curve, 0.86). 18F-FDOPA PET uptake correlated significantly with Ki-67 tumor proliferation index in newly diagnosed tumors (r = 0.66, P = 0.001) but not in recurrent tumors (r = 0.14, P = 0.41). Conclusion: 18F-FDOPA uptake is significantly higher in high-grade than in low-grade tumors in newly diagnosed but not recurrent tumors that had been treated previously. A significant correlation between 18F-FDOPA uptake and tumor proliferation in newly diagnosed tumors was observed, whereas this correlation was not identified for recurrent tumors. Thus, 18F-FDOPA PET might serve as a noninvasive marker of tumor grading and might provide a useful surrogate of tumor proliferative activity in newly diagnosed gliomas.
In primary brain gliomas, markers of proliferative potential and tumor grade determined by pathologic examination of tumor tissue specimens have been among the best-established correlates of clinical outcome (1–4). However, gliomas are notoriously heterogeneous. Tumor tissue is often sampled by stereotactic biopsy, which may not be an accurate representation of the true malignant potential of the tumor. This might lead to a misclassification of true tumor grade and, thus, an inaccurate reflection of prognosis (5). Various noninvasive imaging markers have been studied in brain tumors to evaluate their predictive power in determining tumor grade and proliferative potential.
Amino acid analogs (6–12) and proliferation markers such as 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) (13–17) have been studied for brain tumor imaging. Correlations between tumor proliferation by Ki-67 and 18F-FLT uptake have been reported for 18F-FLT (14–16) and 11C-methionine (14,18–20). 18F-labeled amino acid analogs have the advantage of easy clinical application because of the longer half-life of the 18F PET tracer. It has been shown previously that the amino acid analog 6-18F-fluoro-l-dopa (18F-FDOPA) provides excellent visualization of high-grade and low-grade brain tumors (21–26). 18F-FDOPA is brought into tumor cells via amino acid transporters. However, previous studies have provided conflicting data as to whether 18F-FDOPA uptake differs significantly among high- and low-grade gliomas (22,23,26). Furthermore, it is unknown whether tumor 18F-FDOPA uptake correlates with tumor proliferative activity as measured by antibody staining of the Ki-67 antigen of tumor cells.
The aims of this study were, therefore, 3-fold: first, to determine whether the degree of 18F-FDOPA uptake correlated with World Health Organization (WHO) histopathologic tumor grade by pathologic verification; second, to examine whether 18F-FDOPA tumor uptake and tumor cell proliferation as determined by Ki-67 index were correlated; and third, to compare these characteristics among newly diagnosed and recurrent tumors.
MATERIALS AND METHODS
Patients
The study population consisted of 17 prospectively and 42 retrospectively enrolled patients with malignant brain tumors (Table 1). There were 40 men and 19 women, with a mean age of 44 ± 12 y, ranging from 23 to 71 y. Twenty-two patients had newly diagnosed tumors and 37 patients presented with recurrent tumors who had received treatment previously. Among these 37 patients, all had gone through surgical resection. In addition to surgery, 32 patients had received chemotherapy or radiation (86%), whereas 27 patients had undergone radiation only (73%). The median time from completion of radiation to the PET scan was 51 wk. The time between 18F-FDOPA PET and histologic diagnosis averaged 4.8 ± 4.2 wk (4.0 ± 4.6 wk for newly diagnosed and 5.3 ± 3.9 wk for recurrent tumors).
Patient Characteristics
All prospectively enrolled patients provided written informed consent for participating in this study, which was approved by the University of California, Los Angeles, Office for Protection of Research Subjects. The consent requirements were waived by that office for the retrospectively enrolled patients who had undergone clinical 18F-FDOPA PET or PET/CT scans.
PET
PET was performed on a dedicated system (ECAT HR or HR+; Siemens) (27,28) for 49 patients, and 10 patients were imaged with a dual-detector PET/CT system (Biograph Duo; Siemens). The dedicated PET systems are equipped with bismuth germinate crystal detectors, and the PET/CT system consists of lutetium oxyorthosilicate crystal detectors and a dual-detector helical CT scanner. Our phantom study showed that differences in activity in the volumes of interest between the scanners were not significantly different from differences measured in volumes of interest within a scanner (mean difference of 2.5% in each case).
Patients were asked to fast for at least 4 h before image acquisition. 18F-FDOPA was synthesized according to a previously reported procedure (29,30) and was injected intravenously at a dose of 1.1–6.6 MBq/kg.
For dedicated PET, data were acquired in 3-dimensional mode. Attenuation correction was calculated as reported previously (31). For PET/CT, a CT scan (120 kV, 80 mAs, 1-s tube rotation, 3-mm slice collimation) was acquired first. The CT data were used for attenuation correction as reported previously (32). For both PET and PET/CT scans, the emission scan was started 10 min after tracer injection. Images were acquired for 30 min in 3-dimensional mode. Image data acquired between 10 and 30 min were summed to obtain a 20-min static image. This time window was based on our previous experience that the highest tracer uptake in the tumor generally occurs between 10 and 30 min after 18F-FDOPA injection (23). PET images were reconstructed using iterative techniques with ordered-subset expectation maximization consisting of 6 iterations with 8 subsets (33). A gaussian filter with a full width at half maximum of 4 mm was applied.
Image Analysis
Images were first inspected visually. Then the axial PET image slice displaying the maximum tumor 18F-FDOPA uptake was selected. The activity counts from the 2 adjacent axial slices (1 plane above and 1 below the chosen slice) were summed to improve count statistics.
Tumor regions of interest (ROIs) were defined on summed images in 2 ways. First, a standardized 10-mm circular region was placed over the area with the peak activity. This first ROI was used to derive maximum standardized uptake value (SUVmax) and mean standardized uptake value. To minimize operator dependence, an additional ROI was derived by an 80% peak-voxel-intensity isocontouring approach. This method provided the mean values of voxels with the top 20% SUVs. A normal reference brain region was defined by drawing an ROI involving the entire contralateral hemisphere at the level of the centrum semiovale to derive tumor-to-background ratios. The radiotracer concentration in the ROIs was normalized to the injected dose per kilogram of patient's body weight to derive the SUVs.
Histopathology and Immunohistochemistry
All excised tumors were graded using the WHO grading system (malignancy scale) for central nervous system tumors (34), and all were stained for Ki-67 expression. The available tissue was formalin-fixed and paraffin-embedded. These tissue blocks were recut, and serial sections of 3–4 μm were immunohistochemically labeled with the polyclonal antibody that labels the Ki-67 antigen. The immunohistochemistry was performed according to standard protocol (35). The number of Ki-67–positive cells among the total number of resting cells (Ki-67 labeling index) was determined. Ki-67 labeling index was determined through computerized morphometry as previously described (36). Only nuclei of tumor cells staining definitely brownish were considered positive. The percentage of nuclei stained with Ki-67 antibody per total number of nuclei in the biopsy was defined as proliferative activity.
Statistical Analysis
Receiver operating characteristic curves were used to define optimum cutoff values for the prediction of histopathologic grade. Correlations between various 18F-FDOPA uptake parameters and tumor proliferation (Ki-67 labeling index) were sought using linear regression analysis. Comparisons between groups were done using the Mann–Whitney U test. Statistical analysis was performed using SPSS software (version 16.0; SPSS Inc.) for Windows (Microsoft), and P values less than 0.05 were considered statistically significant.
RESULTS
Histopathology
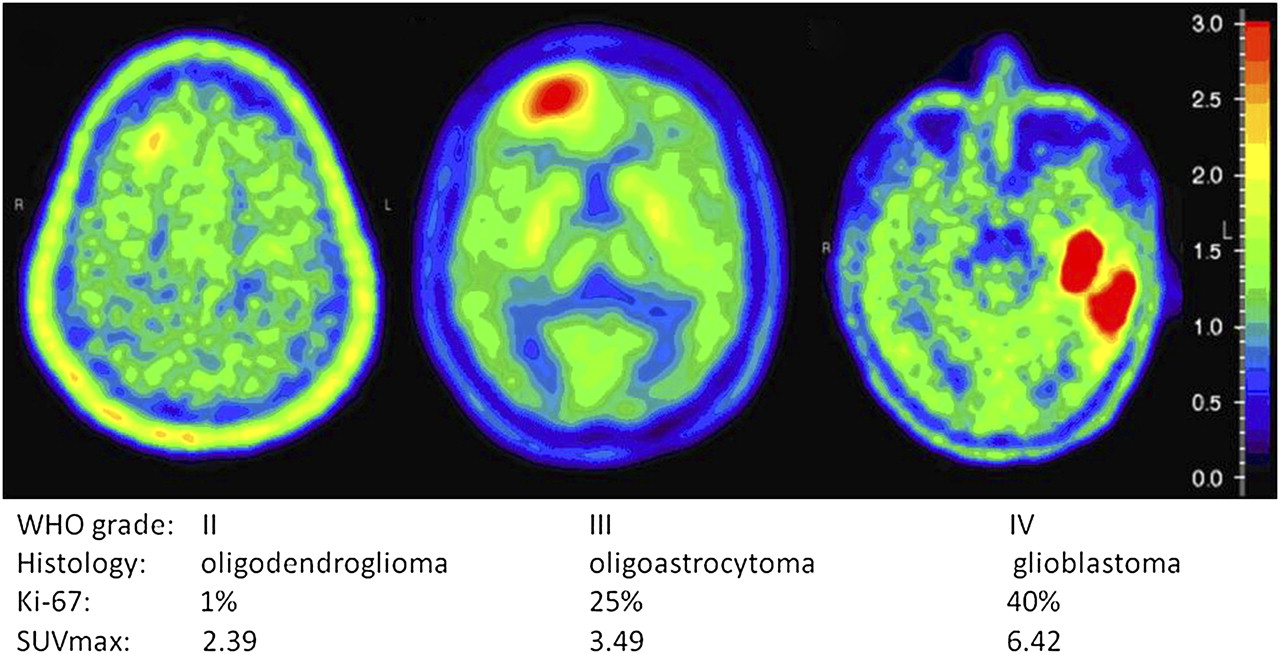
The distribution of tumor types and grades is listed in Table 1. In brief, of the 59 lesions, 25 (42%) were classified as glioblastoma, 12 (20%) as astrocytoma, 11 (19%) as oligodendroglioma, 9 (15%) as oligoastrocytoma, and 2 (3%) as gliosarcoma. Thirteen of 59 lesions (22%) were classified as grade II, 19 (32%) as grade III, and 27 (46%) as grade IV (Fig. 1). No grade I lesions were identified in this patient population. The Ki-67 antibody staining index ranged from 1% to 90% in the 59 samples (mean ± SD, 22.2 ± 20.6), with 17.3% ± 15.9% in patients with newly diagnosed tumors and 25.2% ± 22.6% in recurrent brain tumors (P = 0.20). When stratified by tumor grades, the Ki-67 labeling index averaged 3.92 ± 2.36 in grade II, 17.68 ± 9.06 in grade III, and 34.26 ± 23.50 in grade IV lesions (P < 0.0001).

18F-FDOPA uptake in gliomas.
18F-FDOPA Uptake and Tumor Grade
Correlation coefficients between tumor grade or Ki-67 and the different standardized uptake value (SUV) indices were nearly identical. Therefore, we elected to focus on reporting SUVmax, the most frequently used SUV parameter in the oncologic PET literature.
SUVmax averaged 2.44 ± 1.26 in grade II, 3.34 ± 1.02 in grade III, and 3.78 ± 1.48 in grade IV tumors (grade II vs. III, P = 0.009; grade II vs. IV, P = 0.004; Table 2). No significant differences in 18F-FDOPA SUVmax were noted among grade III and IV tumors (P = 0.42).
18F-FDOPA Uptake in Various Tumors
When stratified into newly diagnosed and recurrent tumors, significant correlations between SUVmax and tumor grades were seen in newly diagnosed tumors but not recurrent tumors (Table 2; Fig. 2). In newly diagnosed tumors, SUVmax averaged 2.34 ± 1.35 in grade II, 3.38 ± 0.93 in grade III, and 5.19 ± 0.93 in grade IV tumors (grade II vs. III, P = 0.044; grade II vs. IV, P = 0.007; grade III vs. IV, P = 0.010). In recurrent tumors, SUVmax averaged 2.67 ± 1.18 in grade II, 3.33 ± 1.10 in grade III, and 3.38 ± 1.37 in grade IV tumors (grade II vs. III, P = 0.38; grade II vs. IV, P = 0.23; grade III vs. IV, P = 0.78).

18F-FDOPA uptake and tumor grade in newly diagnosed and previously treated tumors combined (A), in newly diagnosed tumors (B), and in previously treated tumors (C).
For clinical purposes and risk assessment, brain tumors are frequently stratified into high-grade and low-grade variants. Using this approach, significant differences between high-grade tumors and low-grade tumors were seen in newly diagnosed tumors but not recurrent tumors (P = 0.005 in newly diagnosed and P = 0.22 in recurrent tumors [Table 2]). Receiver-operating-characteristic curve analysis was used to identify the best 18F-FDOPA SUVmax threshold between low- and high-grade tumors. For newly diagnosed tumors, an SUVmax threshold of 2.72 was the best discriminator for differentiating between high- and low-grade tumors (sensitivity and specificity of 85% and 89%, respectively; area under the curve, 0.86).
18F-FDOPA Uptake and Tumor Proliferation
The correlations between the Ki-67 index and all SUV parameters were tested (Table 3). Most were significantly but only weakly correlated with the Ki-67 index (for SUVmax, r = 0.29, P = 0.027; Fig. 3A). The Ki-67 index and 18F-FDOPA SUVmax in newly diagnosed tumors (n = 22; r = 0.66, P = 0.001; Fig. 3B) were significantly correlated. In contrast, no significant correlation was found between Ki-67 index and SUVmax in recurrent tumors (n = 37; r = 0.14, P = 0.41; Fig. 3C).
Linear Regression Results of Various SUV Indices and Ki-67 Index
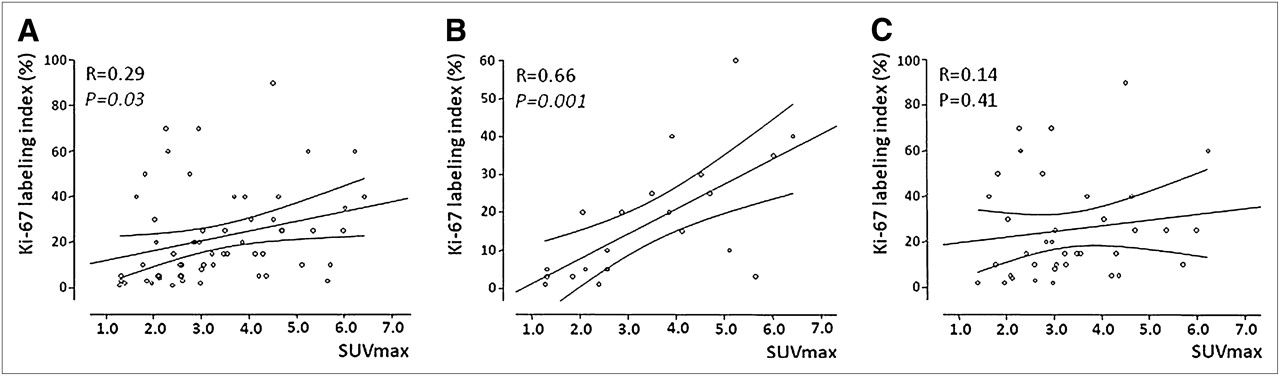
Correlation between 18F-FDOPA uptake and Ki-67 index in newly diagnosed and previously treated tumors combined (A), in newly diagnosed tumors (B), and in previously treated tumors (C).
18F-FDOPA SUVmax and Ki-67 index correlated in astrocytomas (n = 27; r = 0.51, P = 0.0007) but not in nonastrocytomas (n = 32; r = 0.09, P = 0.64). The correlation in astrocytomas was, again, significant only in newly diagnosed tumors (n = 12; r = 0.76, P = 0.004), not in recurrent tumors (n = 15; r = 0.39, P = 0.15).
DISCUSSION
In the current study, we analyzed differences in 18F-FDOPA SUVs among grade II, III, and IV lesions (no grade I lesions were identified) in both newly diagnosed and recurrent gliomas. In addition, we explored whether the degree of 18F-FDOPA uptake could provide information about tumor proliferative activity.
The current study demonstrated that in newly diagnosed tumors, an 18F-FDOPA SUVmax of 2.72 discriminated between low- and high-grade tumors, with a sensitivity and specificity of 85% and 89%, respectively. Furthermore, 18F-FDOPA uptake correlated significantly with the tumor cell proliferation by Ki-67 proliferation index.
Importantly, however, 18F-FDOPA tumor uptake failed to provide reasonable predictions about tumor grade and proliferation in recurrent tumors that had undergone treatments. Thus, our study is consistent with previously published data. The studies that failed to show a correlation of 18F-FDOPA uptake with tumor grade were performed in patient populations with mostly recurrent tumors, 13 of 19 (22) and 71 of 81, respectively (23), and another study that revealed differences between tumor grade and PET uptake used kinetic data in a group of 9 newly diagnosed tumors (26). Furthermore, previously reported studies that showed correlation between Ki-67 and tumor uptake of the amino acid tracer 11C-methionine were performed in patients with newly diagnosed brain tumors (14,18–20).
The lack of correlation of 18F-FDOPA uptake to tumor grade or proliferation index cannot be explained by a longer time between PET and histopathologic assessments, because this interval did not differ significantly between newly diagnosed (5.3 ± 3.9 wk) and recurrent tumors (4.0 ± 4.6 wk). We suspect that in recurrent tumors, blood–brain barrier breakdown contributes to the degree of 18F-FDOPA uptake in addition to amino acid transport as described before (37,38). In our patient population of 37 patients with recurrent tumors, 32 had received chemotherapy or radiation before the PET study (86%). As recurrent tumors may have a wide range of blood–brain barrier breakdown, depending on previous treatments, it is not surprising that the correlation between 18F-FDOPA PET uptake and tumor grade is better in those newly diagnosed tumors that have not gone through previous treatment.
The application of full kinetic modeling in 18F-FDOPA PET studies of gliomas has been demonstrated to provide extra parameters to distinguish high- from low-grade recurrent tumors (26). Significant differences between high- and low-grade tumors were found for 18F-FDOPA transport, influx rate, uptake (SUV), and distribution volume. Dynamic evaluation of O-(2-18F-fluoroethyl)-l-tyrosine PET comprising absolute changes in peak SUV from frame to frame multiplied by the duration of the respective time frame has shown high diagnostic power in tumor grading in untreated and recurrent tumors (11,39). O-(2-18F-fluoroethyl)-l-tyrosine PET also has the advantage over 18F-FDOPA in that there is absence of uptake in the striatum.
It has been reported that tumor cells may upregulate amino acid transporter under adverse conditions (40). Our data further support 18F-FDOPA as an amino acid analog in imaging gliomas because its uptake is predictive of tumor grade and proliferation potential. Thus, our study would predict that, in newly diagnosed gliomas, 18F-FDOPA PET uptake may have significant prognostic value. Further study will demonstrate the value of 18F-FDOPA PET uptake. The prognostic value of 18F-FDOPA PET in recurrent tumors needs further study as well.
CONCLUSION
18F-FDOPA PET of previously untreated gliomas provides potentially useful noninvasive predictions about tumor grade and proliferative activity. 18F-FDOPA PET in previously treated gliomas does not provide information similar to that from untreated tumors. The prognostic value of 18F-FDOPA PET awaits further study.
Footnotes
Guest Editor: Wolf-Dieter Heiss, Max-Planck-Institut für Neurologische Forshung
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication April 29, 2010.
- Accepted for publication June 29, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FDOPA PET for the Noninvasive Prediction of Glioma Molecular Parameters: A Radiomics Study
- O-(2-(18F)fluoroethyl)-L-tyrosine PET for the differentiation of tumour recurrence from late pseudoprogression in glioblastoma
- Effects of L-DOPA Pretreatment on the Kinetics, Migration and Carbon Ion Radiation Response of T98G Cells
- The Role of PET [18F]FDOPA in Evaluating Low-grade Glioma
- Comparison of the Amino Acid Tracers 18F-FET and 18F-DOPA in High-Grade Glioma Patients
- Clinical Impact of Amino Acid PET in Gliomas
- Treatment Response Evaluation Using 18F-FDOPA PET in Patients with Recurrent Malignant Glioma on Bevacizumab Therapy
- Dynamic 18F-FET PET in Newly Diagnosed Astrocytic Low-Grade Glioma Identifies High-Risk Patients
- Radiolabeled Amino Acids for Oncologic Imaging
- Correlation of MRI-Derived Apparent Diffusion Coefficients in Newly Diagnosed Gliomas with [18F]-Fluoro-L-Dopa PET: What Are We Really Measuring with Minimum ADC?
- Analysis of the Growth Dynamics of Angiogenesis-Dependent and -Independent Experimental Glioblastomas by Multimodal Small-Animal PET and MRI
- Impact of 3,4-Dihydroxy-6-18F-Fluoro-L-Phenylalanine PET/CT on Managing Patients with Brain Tumors: The Referring Physician's Perspective
- Multimodality Assessment of Brain Tumors and Tumor Recurrence