


Abstract
The purpose of this study was to conduct a phase I trial of 90Y-DOTATOC to determine the dose-toxicity profile in children and young adults with somatostatin receptor–positive tumors. Methods: A 3 × 3 design was used to determine the highest tolerable dose of 90Y-DOTATOC, with administered activities of 1.11, 1.48, and 1.85 GBq/m2/cycle given in 3 cycles at 6-wk intervals. An amino acid infusion was coadministered with the radiopharmaceutical for renal protection. Eligibility criteria included an age of 2–25 y, progressive disease, a positive lesion on 111In-diethylenetriaminepentaacetic acid-D-Phe1-octreotide scanning, a glomerular filtration rate of 80 mL/min/1.73 m2 or more, bone marrow cellularity of 40% or more or stored autologous hematopoietic stem cells, 60% or more on the Lansky Play Scale, and informed consent. Results: Seventeen subjects (age, 2–24 y) received at least 1 dose of 90Y-DOTATOC; diagnoses included neuroblastoma, embryonal and astrocytic brain tumors, paraganglioma, multiple endocrine neoplasia IIB, and neuroendocrine tumors. No dose-limiting toxicities and no individual dose reductions due to renal or hematologic toxicity were noted. No complete responses were observed; 2 subjects experienced partial response, 5 had minor responses, 6 experienced stable disease, 2 had progressive disease, and 2 withdrew. Conclusion: Peptide receptor radionuclide therapy with 90Y-DOTATOC is safe in children and young adults and demonstrated a 12% partial response plus 29% minor response rate in patients with somatostatin receptor–positive tumors. No dose-limiting toxicities were observed. The recommended phase II dosing is 3 cycles of 1.85 GBq/m2/dose of 90Y-DOTATOC coadministered with amino acids.
Somatostatin receptor expression has been demonstrated in several embryonal tumors in children, including in more than 90% of neuroblastoma and medulloblastomas and 35% of Ewing sarcomas (1,2). Similarly, bronchopulmonary, intestinal, and pancreatic neuroendocrine tumors (NETs) are known to express somatostatin receptors both in vitro (3) and in vivo (4). Early observations were made on excised tumor tissue using immunohistochemistry or in vitro receptor-binding studies and have since been shown to correlate closely with in vivo nuclear imaging techniques using 111In-diethylenetriaminepentaacetic acid (DTPA)-D-Phe1-octreotide (OctreoScan; Covidien), which primarily targets somatostatin receptor type 2 (5–7). These advances led to the development of somatostatin analogs labeled with β-emitting radionuclides that can be used for peptide receptor radionuclide therapy (PRRT) of NETs (8). The radiopharmaceuticals most commonly used in PRRT are 90Y-DOTATOC and 177Lu-DOTA0-Tyr3-Thre8-octreotide (9). The present phase I trial in the pediatric patient population used 90Y-DOTATOC. 90Y is a pure β-emitter, with a maximum energy of 2.3 MeV, a maximum range of 12 mm, and a half-life of 64 h. The relatively long range of the β-particle allows for a bystander effect in heterogeneous tumors in which some cells may be somatostatin receptor type 2–negative.
Both neuroblastoma and medulloblastoma are known to be responsive to external-beam and to targeted radiotherapies (10–13); thus, these tumors should be responsive to PRRT as well. On the other hand, NETs are minimally responsive to conventional radiation therapy (14), yet their response to PRRT has been promising, with phase I–II trials in adults demonstrating 25%–30% partial-response (PR) rates (9,15). Early dose-finding clinical trials in adults established the kidneys as the critical organ of toxicity, followed by bone marrow toxicity at high doses (16). Renal failure was observed in subjects who received up to 7.4 GBq/m2 in the absence of kidney protection with infusion of cationic amino acids (17). Current practice in adults now includes infusion of amino acid solution, beginning 30 min before and continuing 90 min after the administration of 90Y-DOTATOC (18). This therapeutic advance, combined with limiting the renal dose to less than 25 Gy, has considerably reduced renal toxicity (18). Severe bone marrow toxicity has also been rare in adults treated with radiolabeled somatostatin analogs (19). With its low-toxicity profile, significant improvement in symptoms and quality of life, and lack of effective alternative therapies, PRRT has been suggested as a possible first-line therapy in adult patients with gastroenteropancreatic NETs (20). Recent data have also demonstrated a significant survival benefit with PRRT in this population, compared with historical controls (21).
This study was undertaken to test the hypothesis that PRRT would be safe and effective in children and young adults with refractory solid tumors that express somatostatin receptors.
MATERIALS AND METHODS
Design
The 90Y-DOTATOC was administered in 3 cycles, 6 wk apart, starting with 1.11 GBq/m2/cycle in cohort 1 and escalating to 1.48 and then to 1.85 GBq/m2/cycle, using 3 subjects per cohort. Each cohort included at least 3 subjects who received 3 complete cycles of the drug, with no intrapatient dose escalation (22). If 1 of 3 subjects in any cohort developed grade 3 toxicity or above, 3 additional subjects were entered in the cohort; if 2 of 6 subjects in the cohort developed grade 3 toxicity or above, no further subjects were enrolled in that dose cohort, and the dose in the previous cohort was considered as the maximum-tolerable dose. Because this was the first, to our knowledge, use of 90Y-DOTATOC in children, the starting administered activity was based on a requirement of the Food and Drug Administration that the initial dose be limited to less than 50% of the dose used in the phase II trial in adults and that the total estimated dose to the kidneys—including from both 90Y-DOTATOC and any prior direct or scatter doses from external-beam radiotherapy—be limited to 21 Gy for children and 23 Gy for young adults (23). In a subgroup of patients in the third dose cohort, dosimetry studies were performed with 111In-DTPA-D-Phe1-octreotide to measure the renal, hepatic, and bone marrow dose; however, the dosimetry data were not used to adjust the dosage of 90Y-DOTATOC.
Eligibility Criteria
Children and young adults (2–25 y old at the time of first cycle of drug treatment) were eligible to participate if they had pathologically confirmed disease with at least 1 lesion positively imaged with 111In-DTPA-D-Phe1-octreotide that was colocalized with CT or MRI. Eligible patients had progressive disease (PD) that either was not amenable to standard treatment or was recurrent after 2 therapies, with a life expectancy of 2 mo or more but less than 12 mo, and Lansky Play Scale or Karnofsky scores greater than 60%. Additionally, at least 1 target lesion was required that had never been irradiated or had progressed despite radiation and had not been irradiated within 4 wk of the study drug administration. No full brain or spine radiation was allowed within 3 mo, and no surgery or chemotherapy was allowed within 4 wk of the study drug administration. A glomerular filtration rate greater than 80 mL/min/1.73 m2 was required as measured by plasma clearance of 99mTc-DTPA. Hematopoietic status requirements included an absolute neutrophil count greater than 1,000/mm3, a platelet count greater than 100,000/mm3, and a bone marrow cellularity of 40% or more or the availability of 1 × 106 or more CD34-positive hematopoietic stem cells per kilogram. Stem cell availability was required for any subject who had received cranial–spinal irradiation of 12 Gy or more. Adequate cardiac function with a shortening fraction of 30% or more and adequate liver function with bilirubin less than 1.5 times and aspartate aminotransferase and alanine aminotransferase 2.5 or less times the upper limit of normal were also required. All subjects were required to have provided written informed consent for the protocol, which was conducted under Investigational New Drug no. 61,907 and approved by the Institutional Review Board of the University of Iowa.
Exclusion Criteria
Concomitant therapy was not allowed except for somatostatin analogs or bisphosphonates; somatostatin therapy was limited to short-acting subcutaneous doses between cycles, with discontinuation 24 h before each dose of 90Y-DOTATOC. Potential subjects were excluded if they were pregnant or breast-feeding, if they had more than 1 concurrent malignancy, or if they had received external-beam radiation to both kidneys (scatter doses of <0.5 Gy to a single kidney or radiation to <50% of a single kidney was acceptable).
Kidney, Liver, and Bone Marrow Dosimetry
Individual kidney, liver, and bone marrow dosimetric analyses were performed for 8 administrations of 90Y-DOTATOC in 5 subjects in cohort 3, each of whom received 1.85 GBq/m2 per cycle. 111In-DTPA-D-Phe1-octreotide (222 MBq/1.73 m2) was administered concurrently with 90Y-DOTATOC and used as a surrogate for individual kidney and liver dosimetry. 111In-DTPA-D-Phe1-octreotide SPECT/CT images of the abdomen—along with a 1.85-MBq 111In standard in a 30-mL plastic bottle included in the field—were obtained at 4–6, 20–28, and 44–52 h after injection. All imaging studies were acquired on a low-power dual-detector SPECT/CT system with 25-mm-thick NaI(Tl) crystals (Hawkeye; GE Healthcare). Multiple energy windows were set to capture the 172- and 247-keV γ-rays of 111In as well as a window from 300 to 500 keV for the 90Y bremsstrahlung radiation, with an additional scatter window for SPECT studies. Regions of interests were drawn about the kidneys and liver in the coronal views. The kidney and liver masses were determined from the coregistered SPECT/CT images. The cumulative activity in the kidneys and liver was determined from the multiple 111In-DTPA-D-Phe1-octreotide SPECT/CT scans obtained over 48 h. The MIRD scheme (OLINDA software) was used to calculate the renal and liver dose from the accumulated activity (24). To compare the blood clearance of 111In-DTPA-D-Phe1-octreotide and 90Y-DOTATOC, blood samples were also obtained before administration of the radiopharmaceuticals and at 5 min, 4–6 h, 20–28 h, and 44–52 h after administration and counted for 111In and 90Y activity. The cross talk between the counts acquired in the 111In and 90Y energy windows was measured by counting individual standards for the 2 radionuclides. Each standard was counted in both energy windows to determine the cross-talk ratios. For the blood samples, the 90Y bremsstrahlung window was set well above the 111In energies so that the cross-talk ratio from 111In to 90Y was essentially 0. The cross-talk ratio from the 90Y bremsstrahlung into the 111In energy window was 0.695. Thus, the counts in the 111In energy window were corrected by subtracting 0.695 multiplied by the counts in the 90Y window. The calculated blood doses were used as a surrogate for the bone marrow dose.
Drug Administration
To reduce the renal radiation dose, an amino acid solution containing 0.713 mg of arginine and 0.735 mg of lysine per 100 mL (Aminosyn II, 7%; Abbott Laboratories) was infused with each administration of 90Y-DOTATOC. The amino acid solution was infused over 4 h at a dose of 8.3 mL/kg/h, beginning 30 min before infusion of the 90Y-DOTATOC. For nausea, subjects were preadministered ondansetron or lorazepam 30 min before the start of the amino acid infusion. 90Y-DOTATOC was infused over 15 min, beginning 30 min after the initiation of the infusion of amino acid solution. 90Y-DOTATOC was provided by Novartis Pharmaceuticals, Inc., and Molecular Insight Pharmaceuticals, Inc., in patient-specific vials.
Response and Toxicity Assessment
CT or MR images and 111In-DTPA-D-Phe1-octreotide scans were obtained before each cycle and 6–8 wk after the last cycle of therapy. Pediatric Oncology Group criteria were used for response assessment (25). Complete response (CR) is defined as no measureable disease; PR as a 50% or more decrease in longest multiplied by widest perpendicular diameter of target lesions with no increase in any lesions and no new lesions; minor response (MR) as a 25%–50% decrease in target lesions with no increase in any lesion and no new lesions; and stable disease as a less than 25% increase or decrease in any target lesion and no new lesions. An increase greater than 25% in any measureable lesion or the presence of any new lesion was considered PD. Response was based on intent to treat for all subjects who received at least 1 dose of 90Y-DOTATOC. Toxicity was graded using the Common Toxicity Criteria of the National Cancer Institute, version 3.0. The final toxicity assessment was obtained 6–8 wk after the last cycle of 90Y-DOTATOC. Clinical long-term follow-up data were obtained by contacting the referring physicians and included follow-up imaging results and relevant serum biomarkers.
RESULTS
Patient Characteristics
Characteristics of subjects are shown in Table 1 (17 subjects; 5 women and 12 men; age range, 2–24 y). NETs were the most common malignancy (7/17 subjects who participated in the trial). Other diagnoses included neuroblastoma (2), paraganglioma (3), and 1 each of multiple endocrine neoplasia IIB, medulloblastoma, anaplastic astrocytoma, pinealoblastoma, and choroid plexus carcinoma.
Characteristics and Treatment Response of Subjects Treated with 90Y-DOTATOC
Toxicity
Grade 1 or 2 nausea and vomiting was observed in 12 of 17 subjects during amino acid infusion. These symptoms resolved within 30 min of completion of the infusion. Grade 4 hyponatremia requiring intravenous electrolyte resuscitation was observed in 1 patient; 6 additional episodes of mild hyponatremia and 8 cases of hypokalemia self-corrected within 24 h. Two patients developed grade 2 neutropenia, and 1 patient developed grade 2 thrombocytopenia. A grade 1 decrease in glomerular filtration rate was observed in 2 patients. Carcinoid syndrome developed in 2 patients with metastatic NETs within 96 h of 90Y-DOTATOC. Both improved within 24 h after restarting octreotide, with 1 patient requiring hospital admission for the administration of intravenous fluids and octreotide. One death due to tumor progression occurred within 30 d of drug treatment. The maximum-tolerated dose was not reached in this study because no grade 3 renal or bone marrow toxicity was observed at any dose level.
Tumor Response
The overall response rate based on intent to treat was PR in 2 of 17 subjects (12%), MR in 5 of 17 subjects (29%), stable disease in 6 of 17 subjects (35%), and PD in 2 of 17 (12%). Two subjects withdrew. The Lansky Play Scale rating or Karnofsky score increased in 8 patients (47%) and remained stable in 4 patients (24%). The treatment response and follow-up of each subject is presented in Table 1. Seven patients died of their disease 0–23 mo after therapy; 8 patients are alive with disease, and 2 patients have no evidence of disease after a median follow-up of 39 mo (45 ± 24 mo). The 2 subjects with no evidence of disease had PR and MR to therapy and both underwent surgery after 90Y-DOTATOC therapy. One child had removal of the primary pancreatic tumor and 2 surgeries to remove liver metastases, and the second child had a liver transplant. Hormonal response was observed in 5of 6 patients with NETs, who had follow-up of secretory hormones or peptides available (Table 2). Tumor response of 3 patients with astrocytoma, gastrinoma, and bronchial carcinoid, respectively, are presented in Figures 1–3.
Baseline and Best Posttherapy Secretory Hormone/Peptide Levels for NETs
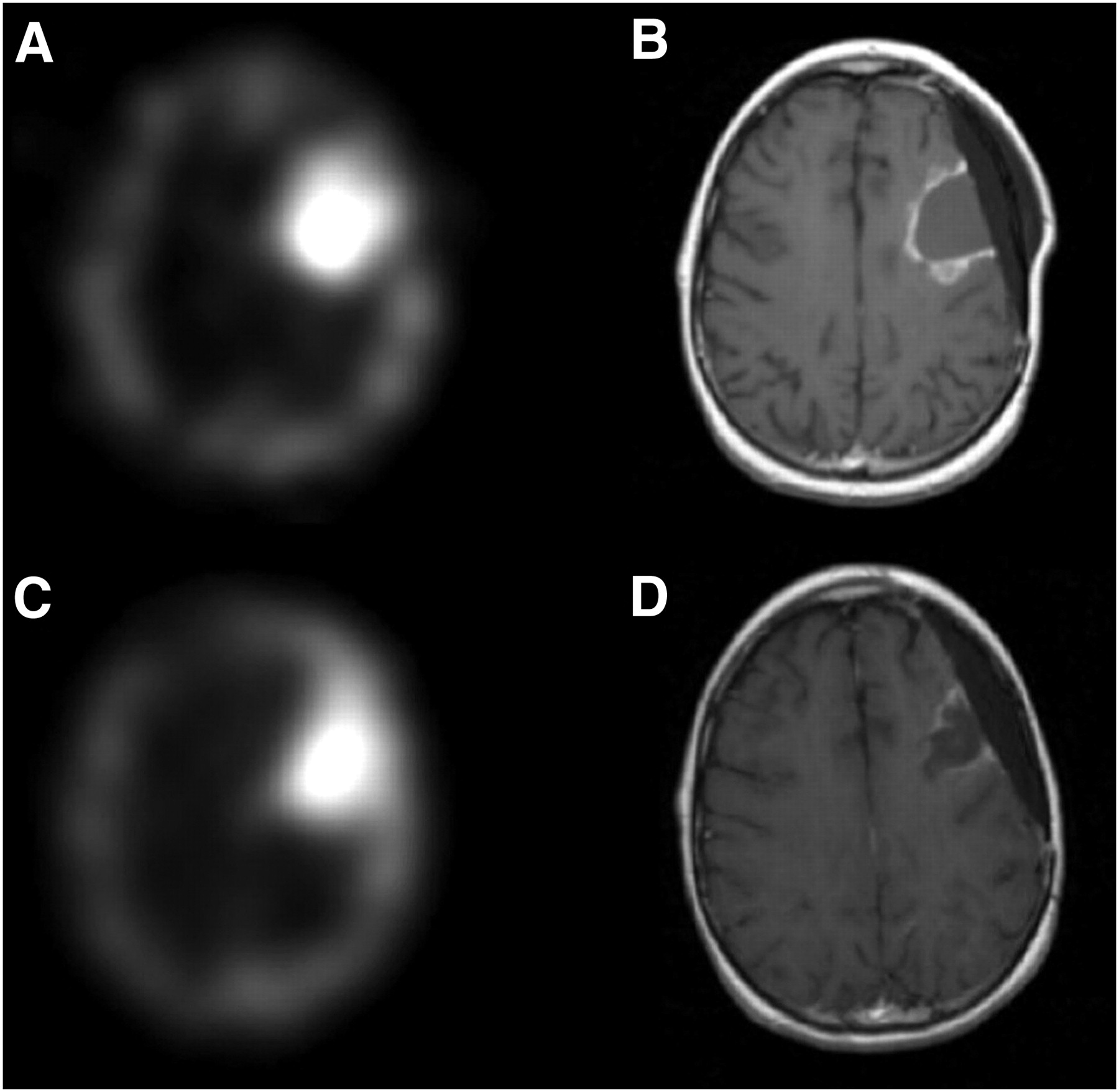
Baseline and posttherapy imaging of subject 3 with anaplastic astrocytoma. This subject had surgery and chemotherapy, followed by cranial–spinal radiation as initial treatment of disease, with further chemotherapy after recurrence. Baseline 111In-DTPA-D-Phe1-octreotide image (A) shows intense uptake in left parietal tumor seen on MR image (B). Posttherapy images show decrease in uptake (C) with partial response on MR imaging with reduction of tumor size and decrease in enhancement around the lesion (D). This patient was able to return to school and participate in sports for 2 y after therapy but ultimately experienced tumor recurrence and died of disease 23 mo after last dose of 90Y-DOTATOC.

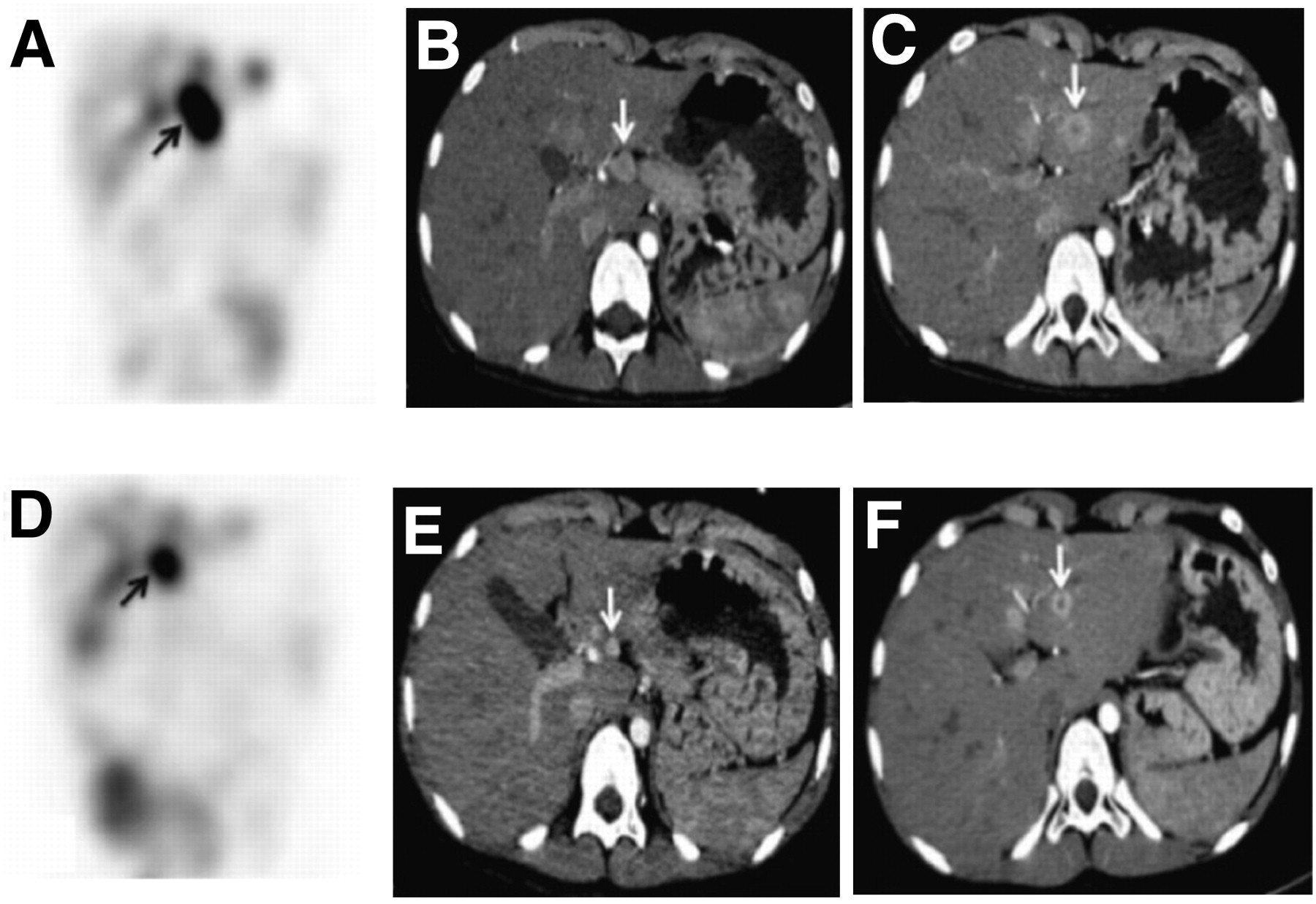
Baseline (A–C) and posttherapy (D–F) coronal 111In-DTPA-D-Phe1-octreotide and CT images of subject 5 with pancreatic gastrinoma and extensive liver metastases. Pancreatic primary tumor (B; arrow) and adjacent liver lesion (C; arrow) show intense uptake of 111In-DTPA-D-Phe1-octreotide (A; arrow). This patient was treated for gastric ulcers until liver metastases were observed on CT scan. After treatment with 90Y-DOTATOC, there was significant decrease in tumor burden on 111In-DTPA-D-Phe1-octreotide image (D) and PR in target lesions on CT scan (E and F; arrows). Serum gastrin levels decreased from 5,440 to 824 pg/mL. Pancreatic tumor was subsequently resected along with partial hepatectomy. Subsequent increase in gastrin level coincided with regrowth of liver lesion at resection margin. Second surgery was performed to extricate this lesion and achieve clear margins; this subject remains free of disease, maintained on octreotide, 68 mo after 90Y-DOTATOC.

Baseline (A–E) and posttherapy (F–J) coronal 111In-DTPA-D-Phe1-octreotide and CT images of patient with liver metastases from poorly differentiated bronchial carcinoid (subject 14). Because of extensive liver disease at time of initial diagnosis, primary bronchial carcinoid had not been removed. Baseline 111In-DTPA-D-Phe1-octreotide images show multiple hepatic metastases (A and B), left lung lesion, and thoracic spine metastasis (D; arrows), with corresponding liver (C) and lung lesions seen on CT scan (E; arrow). Standard 111In activity (S) is seen on pretherapy 111In-DTPA-D-Phe1-octreotide image. Corresponding posttherapy images (F–J) show improvement in liver lesions and thoracic spine and lung lesions on 111In-DTPA-D-Phe1-octreotide image, although this only qualified for MR based on assessment of target lesions on CT scan. Serum chromogranin level in this patient dropped from 69,404 to 11,160 ng/mL, followed by resection of primary lung lesion and stabilization of disease for 19 mo.
Kidney, Liver, and Bone Marrow Dosimetry
The average blood concentration of 111In-DTPA-D-Phe1-octreotide and 90Y-DOTATOC normalized to the amount of administered activity for all 8 studies is depicted in Figure 4. The blood clearance for the 2 tracers was similar, with 111In-DTPA-D-Phe1-octreotide clearing slightly faster from the blood than 90Y-DOTATOC. The bone marrow dose inferred from blood activity ranged between 0.07 and 0.19 mGy/MBq (mean ± SD, 0.12 ± 0.03 mGy/MBq), and the range of renal radiation dose was between 1.1 and 3.8 mGy/MBq (mean ± SD, 2.29 ± 0.95 mGy/MBq). The radiation dose to the liver was between 0.4 and 2.8 mGy/MBq, with higher doses observed in patients with diffuse liver metastases. Patients with diffuse liver metastases tended to have lower renal doses (Table 3).
Calculated Kidney, Liver, and Bone Marrow Radiation Doses for 8 Administrations of 90Y-DOTATOC

Mean blood concentration of 111In-DTPA-D-Phe1-octreotide and 90Y-DOTATOC normalized to amount of administered activity for 8 studies in 5 patients.
DISCUSSION
To our knowledge, this is the first clinical trial of PRRT in children. 90Y-DOTATOC as used in this trial had a low-toxicity profile, with no serious adverse events attributed to the radiopharmaceutical. The kidneys are the dose-limiting organs with 90Y-DOTATOC; however, the renal toxicity in this patient group was minimal, with a mild decrease in glomerular filtration rate observed in 2 of 17 patients. Chronic radiation nephropathy may, however, occur up to 5 y after radiation therapy, and a previous report found slow deterioration of renal function, with an annual median decline of 7.3% in creatinine clearance after targeted peptide radiotherapy in adult patients (26). Therefore, long-term follow-up of renal toxicity is necessary after 90Y-DOTATOC treatment.
The most common toxicity associated with 90Y-DOTATOC therapy was nausea and vomiting during the 4-h infusion of amino acids, which are used for renal radioprotection. The occurrence of nausea with amino acid infusion appears to be related to the osmolarity and infusion rate of amino acids (27). The commercially available Aminosyn II 7% solution used in this study contains a multitude of amino acids in addition to arginine and lysine, the key cationic amino acids required for renal protection. Aminosyn II 7% is, therefore, not the ideal amino acid solution for PRTT and is associated with a higher incidence of nausea and vomiting than a solution containing only arginine and lysine (27). The nausea in our patients typically subsided immediately after the infusion of Aminosyn II 7% was completed.
Hematopoietic toxicity due to 90Y-DOTATOC therapy was minimal, with 2 subjects who had previous chemotherapy experiencing transient grade I or II thrombocytopenia. Although preservation of hematopoietic stem cells was required in several subjects because of previous cranial–spinal irradiation or a bone marrow cellularity of less than 40% at the beginning of therapy, stem cell rescue was not needed in any subjects. The lack of a need for stem cell rescue in the patients in our study correlates with the findings of another study, in which 2%–15% of adult patients who received 15.48 GBq or more of 90Y-DOTATOC experienced severe bone marrow toxicity (19). Two subjects experienced carcinoid crisis 48–96 h after 90Y-DOTATOC infusion, likely secondary to tumor cell kill and release of tumor cell contents such as serotonin, neuropeptides, or catecholamines. Both subjects who experienced a carcinoid crisis had the most severe episodes after the first cycle, and both had measureable cell kill when imaged before the second cycle.
Improved quality of life during treatment is a major advantage of this therapy. The minimal toxicity of 90Y-DOTATOC translated into subjects being able to resume normal activity in the 6-wk intervals between cycles. The lack of γ-emission of 90Y permits treatment without the need for strict patient isolation, allowing contact of children with parents and the care team throughout the delivery of therapy (8,28). Although the guidelines of the Nuclear Regulatory Commission allow this treatment to be performed on an outpatient basis in the United States, some patients may need to be observed for up to 24 h, depending on the severity of the initial adverse events. Convenience for subjects, families, and hospital personnel is an attractive feature of 90Y-DOTATOC, compared with external-beam radiation therapy or 131I-metaiodobenzylguanidine.
The 12% PR and 29% MR rates to 90Y-DOTATOC are promising for a phase I trial in children. The highest response rate was observed in NETs. NETs are extremely rare in children and young adults (29); however, most of these tumors are metastatic at diagnosis and are resistant to most chemotherapeutic agents because of their slower proliferation rate. Among 7 patients with metastatic NETs, 5 patients showed a PR or MR to therapy based on anatomic imaging. CT- or MRI-based response assessment may, however, underestimate clinical response in NETs, particularly after therapy with radiolabeled peptides, which is associated with prolonged antitumoral activity and development of residual masses of fibrotic and necrotic tissue (30,31). A combination of anatomic imaging, functional somatostatin receptor imaging, and secretory hormone or peptide levels is likely a better measure of clinical response to PRRT in this patient population. Like NETs, paraganglioma is also a slow-growing malignancy until it becomes metastatic. All 3 subjects with paraganglioma in this trial had bone metastases, and all experienced symptomatic relief of bone pain after therapy, with persistent stable disease on imaging studies. Symptomatic improvement was also noted in a subject with neuroblastoma metastatic to bone, consistent with our observations for NETs in adults, 66% of whom experienced improvement in clinical symptoms after treatment with 90Y-DOTATOC (32).
The peptide used for the pretherapy dosimetry should be ideally the same as the therapeutic radiopeptide used because differences in receptor binding and kinetics may change the dosimetry estimates. 111In- or 86Y-labeled DOTATOC would be preferable to 111In-DTPA-D-Phe1-octreotide for the calculation of 90Y-DOTATOC dosimetry. The selection of 111In-DTPA-D-Phe1-octreotide in this study was made simply because of its commercial availability in the United States. Previous dosimetry studies have reported that the renal uptake of 111In-DTPA-D-Phe1-octreotide and 111In-DOTATOC was comparable, although liver uptake was higher with 111In-DTPA-D-Phe1-octreotide (33). Helisch et al. noted that 111In-DTPA-D-Phe1-octreotide would be a practical second-line alternative if the gold standard imaging with 86Y-DOTATOC PET is not available (34). The blood-clearance rates and residence time for 90Y-DOTATOC and 111In-DTPA-D-Phe1-octreotide were also similar in our patients. The marrow dose estimates of 0.12 ± 0.03 mGy/MBq in our study are about a factor of 2 higher than those reported in other studies (34,35). One reason for this higher estimate is that we took a conservative approach to the calculation and assumed that after the 48-h measurement, clearance was the same as the 90Y physical half-life. The other possible explanation is that all subjects had a low body mass index and that tends to increase the radiation dose because of a smaller dilution effect. The renal dosimetry data obtained in 5 patients showed significant interpatient variability, with kidney radiation doses ranging from 1.1 to 3.8 mGy/MBq, which is comparable to previously reported data in adults (36). These findings indicate that the maximum-tolerable dose of 90Y-DOTATOC therapy is highly variable among patients, and individualized dose administration rather than fixed doses may be preferable to reduce toxicity and improve treatment efficacy. In fact, the estimated renal dose based on dosimetry exceeded significantly the recommended upper limit of 21–23 Gy in 1 patient, who received 1.85 GBq/m2/cycle (subject 17). Our findings also show potential significant intrapatient variability, so that repeated dosimetry may be necessary before each cycle of treatment if the administered dose will be based on the maximum-tolerable dose.
CONCLUSION
PRRT with 90Y-DOTATOC demonstrated a favorable safety profile in this phase I study in children and young adults with refractory solid tumors that express somatostatin receptors. No dose-limiting toxicities were observed. Renal radiation exposure remains the dose-limiting factor and, although no compromise in kidney function has been observed in any subjects, the recommended phase II dose of 90Y-DOTATOC is 1.85 GBq/m2/dose coadministered with amino acids in 3 cycles, 6 wk apart, for a cumulative dose of 5.55 GBq/m2. Together, PR, MR, and stable disease constituted a 76% overall positive response rate to 90Y-DOTATOC, warranting a phase II trial.
Acknowledgments
We thank James Ponto for the preparation of the radiopharmaceutical, John Bricker for technical support, and the nursing team at the Clinical Research Center at the University of Iowa Hospitals and Clinics. This study was funded by the National Cancer Institute (R21 CA91578), the Food and Drug Administration (R01FD002595), Eastern Star, University of Iowa Holden Comprehensive Cancer Center, and University of Iowa Dance Marathon. This study was previously presented at the North American Neuroendocrine Tumor Society Neuroendocrine Tumor Symposium, October 2–3, 2009, Charlotte, North Carolina.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication February 25, 2010.
- Accepted for publication June 25, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- NANETS/SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy
- Radiopeptide Imaging and Therapy in the United States
- Novel SDHD Gene Mutation (H102R) in a Patient With Metastatic Cervical Paraganglioma Effectively Treated by Peptide Receptor Radionuclide Therapy
- 177Lu-DOTATATE Molecular Radiotherapy for Childhood Neuroblastoma