


Abstract
The annual incidence of primary intracranial tumors is 7 to 19 cases per 100,000 people. The general approach to the treatment of brain neoplasms is surgical resection of solitary lesions or limited disease, followed by radiation therapy with or without chemotherapy. Multiple metastatic lesions are usually treated with whole-brain radiation. Radiation injury occurs in 5% to 37% of cases and can be difficult to differentiate from residual or recurrent malignancy by MRI. PET has been used to differentiate radiation injury from malignancy on the basis of differences in glucose uptake. Recent studies have reported the sensitivity and specificity of PET to be 81% to 86% and 40% to 94%, respectively. This article reviews the classification of primary brain tumors, the histologic changes associated with radiation injury, and the diagnostic and prognostic information provided by PET.
The annual incidence of primary intracranial tumors is 7 to 19 cases per 100,000 people (1,2). The incidence is 3.1 cases per 100,000 people at 0–4 y of age. The incidence decreases between 15 and 24 y and then increases steadily to a peak of 18 to 19 per 100,000 between 65 and 79 y. Primary central nervous system (CNS) neoplasms are the third leading cause of death between 15 and 35 y and the second leading neoplastic disease in children under 15 y (1). The World Health Organization (WHO) classification that relies on cellular origin is outlined in Table 1. Tumors of neuroepithelial origin are the most common, followed by tumors of meningeal, hematopoietic, and nerve sheath origin. In adults, most neuroepithelial tumors are from glial cells; common glial cells types are astrocytes, oligodendrocytes, ependymocytes, and subependymocytes. Tumors originating from the glia are collectively known as gliomas. Gliomas constitute over 90% of primary brain tumors in persons older than 20 y (3,4).
WHO Classification of Primary Intracranial Tumors
There have been numerous attempts to classify astrocytomas, and there are several incongruous systems in use today, which sometimes contribute to the lack of clarity regarding which grade of tumor is being discussed (Table 2). Low- and high-grade astrocytoma refers to grades 1–2 and grades 3–4, respectively, of the Kernohan, Mayo, or WHO systems. The Mayo/St. Anne classification is based on nuclear atypia, mitoses, necrosis, and endothelial proliferation. Daumas-Duport et al. (5) and Black (6) reported a better reproducibility and correlation with survival using the Mayo/St. Anne system than its predecessors. The WHO grading system was introduced in 1979 in an attempt to provide a grading system that was based on morphology for all types of glioma (2,4). The system includes pilocytic astrocytoma, which is a posterior fossa tumor that occurs in children and has a better prognosis than astrocytoma in adults.
Classification of Astrocytomas
Neoplasms of ependymal origin are classified as ependymoma (WHO grade 2) and anaplastic ependymoma (WHO grade 3). Oligodendroglial neoplasms are classified as oligodendroglioma and anaplastic oligodendroglioma (WHO grades 2 and 3, respectively). Ependymomas and oligodendrogliomas rarely progress into highly malignant tumors with features of glioblastoma multiforme (i.e., high cellularity, necrosis, and endothelial proliferation) and are classified as WHO grade 4. Other primary brain tumors include neuroblastoma, retinoblastoma, lymphoma, and meningioma (4).
Brain metastases are up to 10 times more common than primary brain tumors and occur in 20% to 40% of patients with cancer. There are 170,000 new cases of brain metastases in the United States per year (7).
TREATMENT
The general approach for treating brain neoplasms is surgical resection of solitary lesions or limited disease, followed by radiation therapy with or without chemotherapy. Multiple metastatic lesions are usually treated with whole-brain radiation. Solitary primary and metastatic tumors may be treated with local field radiotherapy or stereotactic radiosurgery. The usual local field radiation dose for metastases is up to 40 Gy, for astrocytoma up to 50 Gy, and for glioblastoma multiform (GBM) up to 60 Gy. The dose is fractionated over 4 to 6 wk. Tumor response to treatment is proportionate to the dose in this range. Stereotactic radiosurgery is being used increasingly as an alternative to conventional radiotherapy or surgery. Radiosurgery uses a highly collimated beam of radiation that delivers a high dose to a lesion over a brief period of time (3,7,8).
RADIATION INJURY
Radiation injury to the brain is the major dose-limiting complication of radiotherapy. The term “radiation necrosis” is commonly used to describe radiation injury, but it is inaccurate because the pathology of radiation injury is not limited to necrosis (9,10). The incidence of radiation injury depends on the total dose and the rate of delivery (fractionation). Very young children are more susceptible than adults. Edema, vasculopathy, infection, and chemotherapy potentiate radiation injury. Some chemotherapy agents, such as nitrosurea, procarbazine, and vinca alkaloids, are directly neurotoxic. Other agents, such as adriamycin and methotrexate, potentiate radiation effects.
Radiation injury can be divided into acute, early-delayed, and late-delayed stages (Table 3). Late-delayed radiation injury (LDRI) occurs 4 mo to 10 y after radiation. Seventy percent of cases occur in the first 2 y. The primary mechanism of LDRI is vascular endothelial injury or direct damage to oligodendroglia (10). The white matter is affected more than gray matter. The incidence of LDRI is 5% to 37% and increases with higher radiation doses (8,11). Symptoms of recurrent tumor and LDRI are similar. Both conditions can cause progressive deterioration and death. Treatment of LDRI ranges from conservative measures to control intracranial pressure to surgical excision of the edematous mass (1,2,7).
Clinical, Radiologic, and Pathologic Findings in Brain Radiation Injury
RADIOGRAPHIC EVALUATION
The typical appearance of brain tumors as well as LDRI is a contrast-enhancing mass, surrounded by edema and mass effect. Contrast enhancement with Gd diethylenetriamine pentaacetic acid (DTPA) on MRI or with iodine on CT depends on the disruption of the brain–blood barrier (BBB) by tumor or radiation. Steroid treatment can increase the integrity of the BBB and decrease the amount of contrast enhancement (12). There have not been any studies evaluating the sensitivity and specificity of CT and MRI for recurrent tumor, but there is general agreement in the literature that CT and MRI cannot reliably distinguish recurrent brain tumor from LDRI (13–16). The limitations of CT and MRI prompted us to search for more accurate noninvasive tests.
PET
Background
LDRI and a recurrent tumor have different rates of glucose metabolism. Areas of radiation injury have lower glucose metabolism than normal brain tissue because they are less cellular (17). Glucose metabolism can be measured by the uptake of 2-[18F] FDG. FDG is actively transported across the BBB into the cell, where it is phosphorylated by glucose hexokinase. FDG-6-phosphate is trapped in the cell because it is not susceptible to the G-6-phosphate dehydrogenase reaction, which is the next step in the glycolytic cycle. The amount of intracellular FDG is proportionate to the rate of glucose transport and intracellular phosphorylation. Malignant cells generally have high rates of aerobic glucose metabolism, although the metabolic rate of low-grade gliomas and some metastases may be less than normal cortex. FDG PET may be less sensitive in differentiating recurrence from radiation injury in these tumors. A few low-grade tumors, such as pilocytic astrocytoma (a posterior fossa tumor that usually occurs in children) and pituitary adenoma, may have high FDG uptake and are an exception. Janus et al. (18) suggested that a higher malignant grade may be associated with an increase in anaerobic metabolism and a false-negative scan. A reversible decrease in metabolic activity in viable tumors in the immediate postradiation period could also decrease glucose metabolism (12,19,20). In a controlled study on chemotherapy effects, researchers reported that all the false-negative scans occurred in patients who received accelerated fractionated radiotherapy (higher average dose in less time than the rest of the patients) (18). False-positive scans may be caused by radiation injury, which activates repair mechanisms that can increase aerobic glucose metabolism (18). Normal healing processes during the immediate postsurgical period (up to 3 mo) have also caused false-positive scans (12). The optimal timing of an FDG PET scan in the postradiation period has not been determined. Other nonmalignant causes of elevated glucose uptake are seizure foci and abscesses (12,21).
Procedure
FDG (74–370 MBq depending on age and weight) was injected in a room with low ambient light and noise. Patients were asked to rest quietly with their eyes closed. An emission scan of the head was acquired 30–60 min after injection of FDG. Emission data were corrected for signal attenuation using a transmission scan, or an empiric uniform correction method in place of the transmission scan. The empiric method technique does not account for areas of nonwater attenuation, such as the sinuses, but is not susceptible to error from misregistration of emission and transmission data that is caused by patient movement. This method allows relative, but not absolute, quantitative measurement of regional glucose metabolism. Absolute quantification of regional cerebral glucose metabolism (rCMRGlu) requires tracer kinetic modeling and serial arterial blood sampling (22,23,24). Qualitative scan evaluation may be superior to quantitative analysis because accurate regions of interests may be difficult to define, and rCMGlu of small, highly hypermetabolic foci within a larger, moderately hypermetabolic tumor may be underestimated by averaging over the entire tumor (24). Interpretation of PET is based on detection of abnormal hypometabolic or hypermetabolic foci compared with the surrounding tissue or the contralateral equivalent area (21). Availability of MRI or CT for anatomic correlation is important. Co-registration of PET with MRI or CT on a single computer may improve diagnostic accuracy of PET for lesions located in the cortex or at the border between the cortex and white matter. Improved localization is particularly important in the regions that are anatomically distorted by surgery or radiation therapy.
Diagnostic Value
Studies conducted prior to 1990 (17,24–26) reported very high accuracy of FDG PET (Table 4). Patronas et al. (25) and Doyle at al. (26) studied very small samples, had limited correlation with pathology, and may have had patient selection bias. Di Chiro et al. (17) had the largest sample, with pathologic confirmation of PET diagnosis in all cases, although the timing of tissue confirmation of PET results was not discussed. Di Chiro et al. reported 100% sensitivity and specificity of PET in the diagnosis of radiation necrosis and recurrent tumor; however, 2 of the cases classified as true negative had mixed tumor and necrosis. In the study by Valk et al. (24), the results showed that the sensitivity and specificity of PET were 88% and 81%, respectively, on the basis of clinical course (24). Studies performed after 1990 also have shown that the sensitivity of FDG PET for identifying recurrent tumor is greater than 80%, but the reported specificity ranges from 40% to 94% (12,18,21, 27,28). Ricci et al. (21) reported that the number of false-positive cases decreased when contralateral gray matter was used for comparison with the lesion instead of contralateral white matter. Some of the false-positive results in this study could have been from post-test bias because patients with negative PET were less likely to have a tissue diagnosis. Another study with a high rate of false-positive results had significant design limitations that included lack of pathologic correlation in most cases, up to an 18-mo lag between PET and the tissue diagnosis, and poor interrater reliability (28). Inflammatory activity may be a cause of FDG uptake in late-delayed radiation injury (LDRI). Fischman et al. reported a case of FDG avid radiation necrosis after radiotherapy of meningioma (20).
Accuracy of PET in Differentiation of Radiation Injury from Tumor Recurrence
We reviewed 72 consecutive cases referred to us by the Palo Alto Veterans Affairs PET Center (Palo Alto, CA) from January 1995 through March 1999, with a request to differentiate recurrent tumor from DLRI as a cause of new clinical symptoms or increase in size or enhancement characteristics of a known brain abnormality. Eleven of 72 patients had a brain lesion tissue diagnosis by biopsy or surgery within 60 d after the PET scan. PET scans were true positive in 8 patients, false negative in 2 patients, and equivocal in 1 patient (sensitivity, 82%; Figures 1 and 2). One of the false-negative cases was a patient with a low-grade glioma, and the other patient had a well-differentiated adenocarcinoma of unknown primary origin.
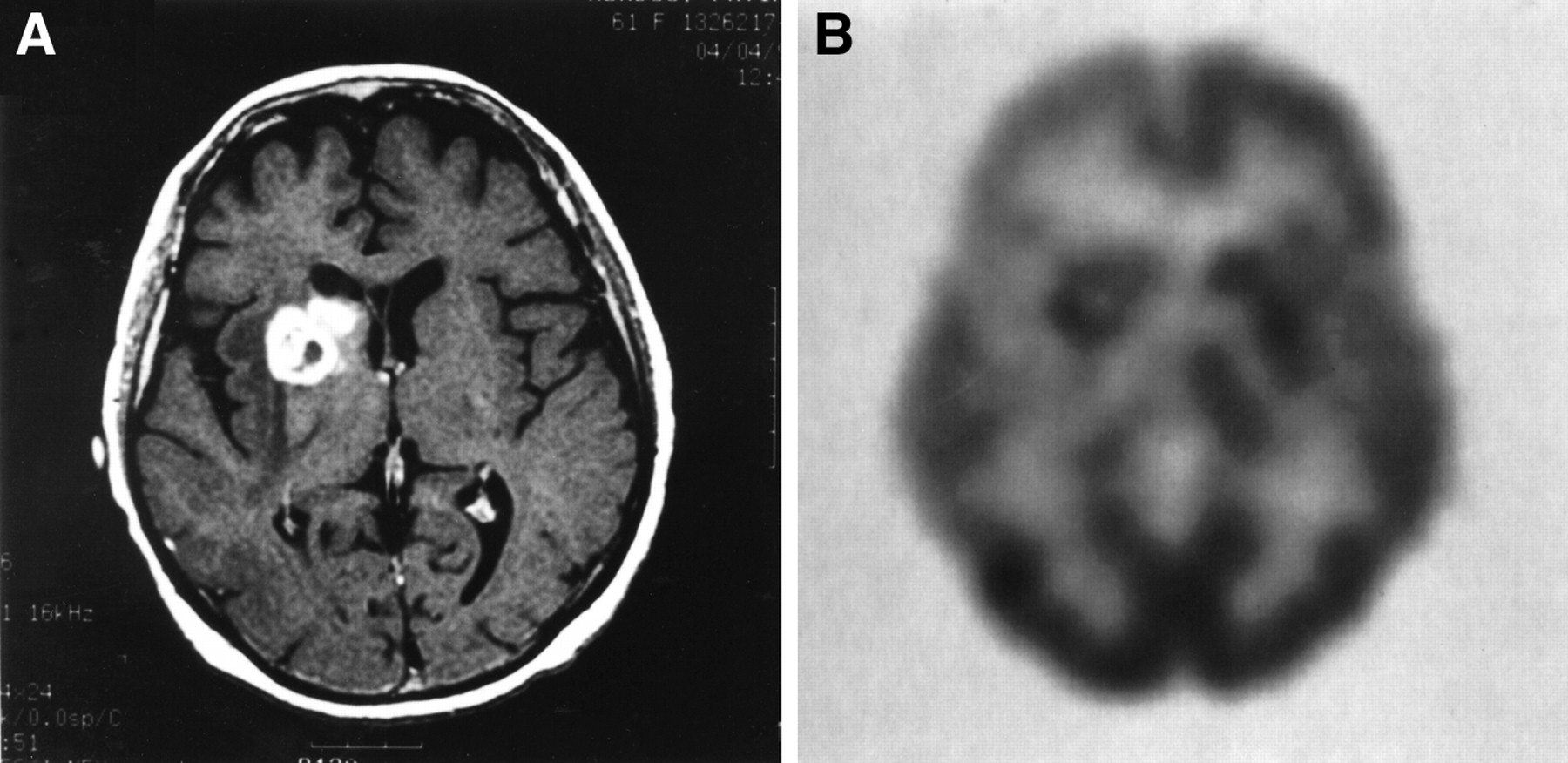
Sixty-y-old woman with stage IV ovarian cancer (diagnosed Sept. 1993) treated with surgery and chemotherapy until April 1994. (A) GdDTPA T1-weighted (Tr = 766, TE = 13) MRI scan (performed April 4, 1997) showing ring-enhancing lesions with central low signal in the right parietal cortex, the white matter of the right frontal lobe, and the right caudate head and anterior portion of the internal capsule. (B) PET scan (performed April 2, 1997) shows 2 right parietal cortical hypermetabolic lesions, hypometabolism in right frontoparietal area, and 2 areas of annular hypermetabolism with central hypometabolism: in the right frontal white matter and adjacent to the right caudate. In 1995, patient developed ataxia and right-sided hearing problems. MRI showed 2 right parietal metastases. Patient was treated with whole-brain radiation (30 Gy in 10 fractions) and dexamethasone and then with stereotactic radiosurgery (18 Gy to right parietal lesions). She developed seizures 8 mo later; MRI showed enlargement of 2 right parietal lesions. On April 4, 1997, she had stereotactic removal of the superficial lesions that were hypermetabolic on PET. Deeper lesions could not be removed because of location. Patient was lost to follow up after this procedure.
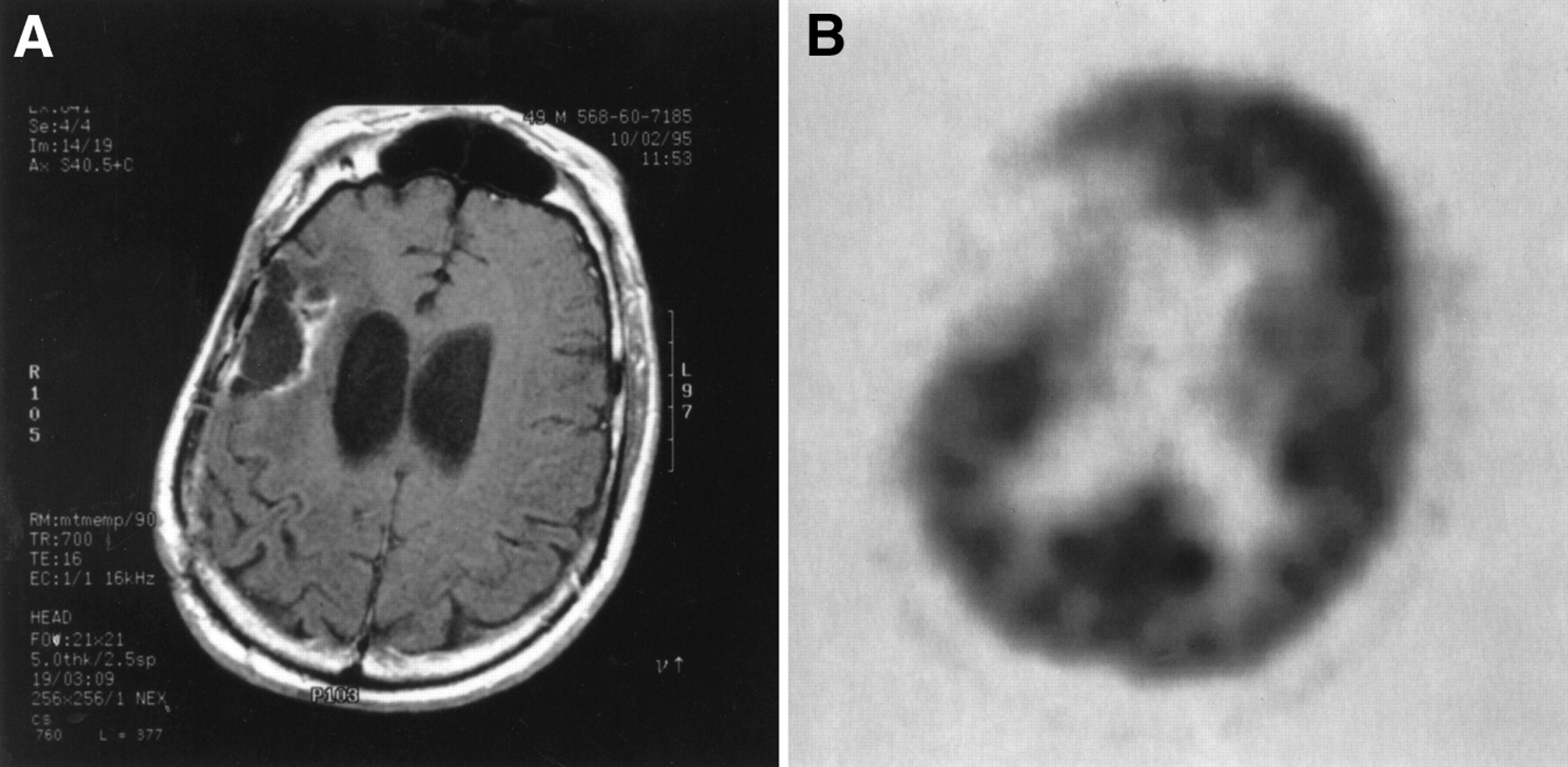
MR and PET scans of 50-y-old man, with a history of grade 2 right frontal oligodendroglioma, who presented with headaches and memory loss. (A) GdDTPA T1-weighted (Tr = 700, TE = 16) MR scan of 50-y-old man, showing an area of low signal in the right parietal lobe with predominantly peripheral contrast enhancement, edema, and focal areas of hemorrhage, which indicated the possibility of tumor or DLRI. (B) PET scan of patient's brain, showing hypometabolic right frontoparietal area consistent with changes after surgery and radiation. No hypermetabolic foci to suggest recurrent tumor. Tumor was resected on September 8, 1993, and treated with radiation therapy to the frontal and parietal lobes (total dose between September 29 and November 9, 1993 = 56 Gy). Patient continued to have mild cognitive deficits and psychosis. In 1995, patient developed new neurologic deficits and dementia worsened. MR showed progression of edema and enhancement in the right parietal lobe, next to the resection site. PET scan in November 1995 was negative for abnormal hypermetabolic foci; a second craniotomy was performed December 1995, and right frontoparietal cystic lesion without evidence of malignancy on a frozen section was removed. Histologic examination showed mixed astrocytoma and oligodendroglioma without mitotic activity, and with areas of focal necrosis. Patient died in February 1996.
Cross-Study Comparison and Study Design Considerations
Cross-study comparison was difficult because of the differences in study designs and tumor types included. There was no uniformity among studies in the important variables of chemotherapy, radiation therapy dose, time interval between PET and tissue diagnosis, and qualitative methods of scan interpretation. Some of these variables were not described in detail in some of the articles. All studies were subject to post-test bias because the decision for reoperation or stereotactic biopsy was influenced by PET. The validity of using the clinical course as a confirmation of tumor recurrence or LDRI in all or some patients is also questionable, because LDRI may have a clinical course that is indistinguishable from tumor recurrence. From the available data, we could not derive a single numerical value for the accuracy of PET in differentiating recurrent tumor from LDRI.
Prognostic Value
Di Chiro and Fulham (19) challenged the role of pathologic diagnosis as the best predictor of prognosis. They suggested that tumor biologic behavior and patient prognosis may be better predicted by tumor metabolic activity rather than histologic grade. Pathologic diagnosis is limited by the tendency of gliomas to progress to more malignant histologic types over time. Biopsy material is difficult to interpret because gliomas are not homogenous and could contain areas of necrosis and cells of variable degree of malignancy or even type (2). Ericson et al. (see Table 5) prospectively studied the survival of 31 patients with suspected recurrent brain metastases after stereotactic radiation (29). Fourteen patients had hypermetabolic foci at the tumor site, and 17 patients had hypometabolic foci. The hypometabolic group had a median survival of 19.9 mo (40% increase) versus 12.3 mo in the hypermetabolic group. Barker et al. (30) studied a cohort of 55 previously treated patients with suspected recurrent high-grade glioma (73% grade 4; 22% grade 3). They reported a median survival time of 10 mo for patients with FDG uptake equal to or greater than the adjacent cortex and 20 mo for those with FDG uptake less than the adjacent cortex (30). DiChiro and Fulham also questioned the role of pathologic diagnosis as a gold standard for FDG PET. They argued that the presence of morphologically intact tumor cells in a tissue sample did not indicate tumor recurrence, because the cells may be unable to proliferate after treatment (19). Valk et al. also presented evidence to support this argument (9,24): 19 patients had pathologic examination within 4 mo of PET. Nine of the 18 patients had PET evidence of tumor, whereas the other 9 patients showed radiation injury. The clinical course correlated better with PET than pathology. All patients in our small series also had some tumor cells, regardless of PET or MRI findings or the clinical course. The 2 patients with a false-negative FDG PET result survived 6 mo and 26 mo. Patients whose scans were true positive survived from 2 mo to more than 21 mo (5 of 9 patients were alive at the time of this writing). Most studies support the predictive value of FDG PET in suspected recurrent brain tumor. Prospective studies that excluded brain metastases from primary brain tumors confirmed earlier observations of DiChiro and Fulham (19) and Patronas et al. (25) of significantly longer survival in patients with a negative PET scan (29,30).
Median Survival with Negative or Positive FDG PET
Impact on Management
The impact of a test on clinical management does not rest only on the scientific merit or even cost effectiveness. Availability and physician education are also important. The impact of a test may grow with increased physician awareness. At this time, the literature on the impact of PET in the clinical management of patients with brain tumor is limited, and the conclusions of the available studies are variable. In the largest review available to date, Deshmukh et al. (32) reviewed the effect of FDG PET on subsequent management in 89 patients with treated primary brain tumors. In 59% of cases, PET results contributed to a decision by the physician to withhold treatment and in 31%, PET results contributed to a decision to initiate new therapy or surgery. In a study by Janus et al. (18), treatment decisions were affected by PET in 24 of 50 patients. The high rate of agreement between GdDTPA MRI and FDG PET has been interpreted by some authors as an indication of limited added value of FDG PET (12,33).
Alternative and Emerging Diagnostic Modalities
Other modalities that may have a potential role in the differential diagnosis of recurrent brain tumor versus radiation injury are magnetic resonance spectroscopy (MRS); blood-volume imaging with echo-planar magnetic resonance; PET, using radiolabeled pyrimidine nucleosides (11C thymidine) or amino acids (11C-tyrosine and 11C methionine); and 201Tl or 123I-α-methyl-l-tyrosine (IMT) SPECT (2,34–37). Amino acids and IMT uptake are markers of cellular proliferation. Pyrimidine nucleoside uptake is related to mitotic activity (38–40). Physiology of 201Tl uptake may be related not only to disruption of the BBB but also to active transport of this potassium analog (28). Changes in choline, creatine, and n-acetyl aspartate ratios on MRS can also serve as an indicator of tumor proliferation (38). Case reports and small studies of patients showing potential advantages over FDG PET in sensitivity, cost effectiveness, or additional information have been published for those modalities (16,28,40–43). Combining information derived from FDG PET with other modalities could improve the accuracy of FDG PET. At this time, experience with other modalities is still limited.
All studies reviewed here used dedicated PET cameras. Coincidence FDG imaging with gamma cameras for differentiation of brain tumor recurrence from radiation injury has not been evaluated (44).
CONCLUSION
FDG PET is useful in differentiating LDRI from recurrent high-grade glioma. The sensitivity of PET is 80%–90% and the specificity is 50%–90%. Tissue diagnosis may not be the gold standard for evaluation of the accuracy of FDG PET. Methods of analysis assuming absence of an external standard could be used to test the specificity and sensitivity of PET in the future (45,46). Causes of false-negative PET results include recent radiation therapy, low histologic grade, and small tumor volume. FDG PET may be false positive in nonmalignant inflammatory processes and subclinical seizure activity. The question of hypermetabolic foci of radiation injury as a cause of false-positive scans requires further investigation. Other issues requiring further study are the optimal timing of FDG PET after radiation and chemotherapy and the accuracy of FDG PET in tumors other than high-grade gliomas. FDG PET is also a valuable predictor of survival in high-grade recurrent glioma. Additional applications of FDG PET in the management of recurrent brain tumors are the selection of the best biopsy site in case of multiple lesions and determination of active tumor margins for local radiation therapy planning. GdDTPA MRI is an established modality that should be complementary to FDG PET in evaluation of patients with brain tumors. In the future, combining FDG PET and another imaging modality on the basis of different physiologic mechanisms (e.g., MRS, Tl201 or IMT SPECT, PET with radiolabeled amino acids, and nucleosides) could improve diagnostic accuracy.
Footnotes
Received May 24, 2000; revision accepted Jul. 13, 2000.
For correspondence or reprints contact: George M. Segall, MD, Nuclear Medicine Service 115, VA Palo Alto Health Care System, 3801 Miranda Ave., Palo Alto, CA 94304.
*NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org) UNTIL MAY 2001.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Rewiring of cortical glucose metabolism fuels human brain cancer growth
- Positron emission tomography and perfusion weighted imaging in the detection of brain tumors recurrence: A meta-analysis
- PET/MRI in Pediatric Neuroimaging: Primer for Clinical Practice
- Although Non-diagnostic Between Necrosis and Recurrence, FDG PET/CT Assists Management of Brain Tumours After Radiosurgery
- Multimodality Assessment of Brain Tumors and Tumor Recurrence
- Perfusion CT Imaging of Brain Tumors: An Overview
- Permeability Estimates in Histopathology-Proved Treatment-Induced Necrosis Using Perfusion CT: Can These Add to Other Perfusion Parameters in Differentiating from Recurrent/Progressive Tumors?
- An Experimental Study of Acute Radiation-Induced Cognitive Dysfunction in a Young Rat Model
- MR Spectroscopy in Radiation Injury
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- Clinical Applications of PET in Brain Tumors
- Uptake of 18F-Fluorocholine, 18F-FET, and 18F-FDG in C6 Gliomas and Correlation with 131I-SIP(L19), a Marker of Angiogenesis
- PET and SPECT for Detection of Tumor Progression in Irradiated Low-Grade Astrocytoma: A Receiver-Operating-Characteristic Analysis