


Article Figures & Data
Figures
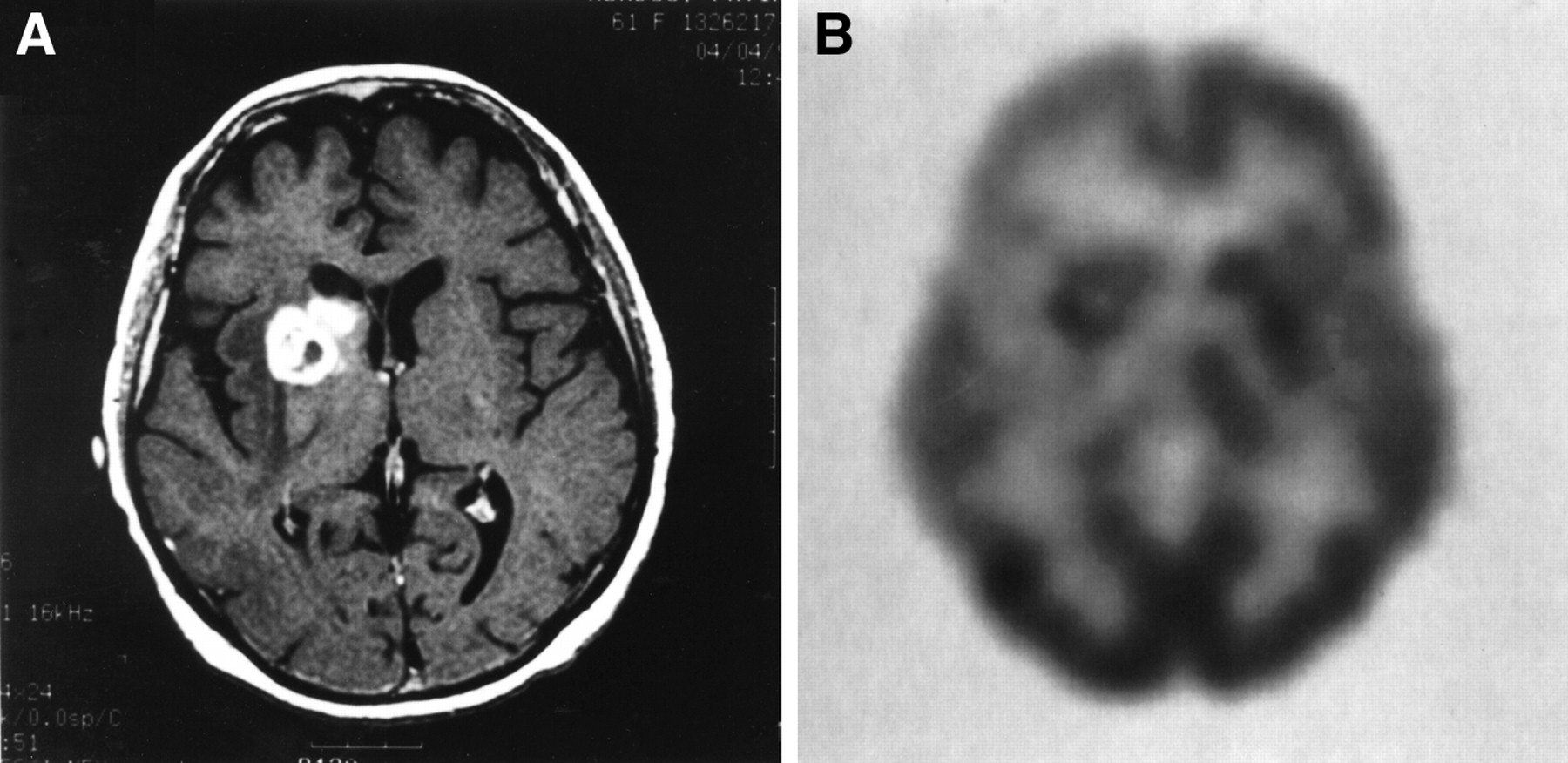
- FIGURE 1.
Sixty-y-old woman with stage IV ovarian cancer (diagnosed Sept. 1993) treated with surgery and chemotherapy until April 1994. (A) GdDTPA T1-weighted (Tr = 766, TE = 13) MRI scan (performed April 4, 1997) showing ring-enhancing lesions with central low signal in the right parietal cortex, the white matter of the right frontal lobe, and the right caudate head and anterior portion of the internal capsule. (B) PET scan (performed April 2, 1997) shows 2 right parietal cortical hypermetabolic lesions, hypometabolism in right frontoparietal area, and 2 areas of annular hypermetabolism with central hypometabolism: in the right frontal white matter and adjacent to the right caudate. In 1995, patient developed ataxia and right-sided hearing problems. MRI showed 2 right parietal metastases. Patient was treated with whole-brain radiation (30 Gy in 10 fractions) and dexamethasone and then with stereotactic radiosurgery (18 Gy to right parietal lesions). She developed seizures 8 mo later; MRI showed enlargement of 2 right parietal lesions. On April 4, 1997, she had stereotactic removal of the superficial lesions that were hypermetabolic on PET. Deeper lesions could not be removed because of location. Patient was lost to follow up after this procedure.
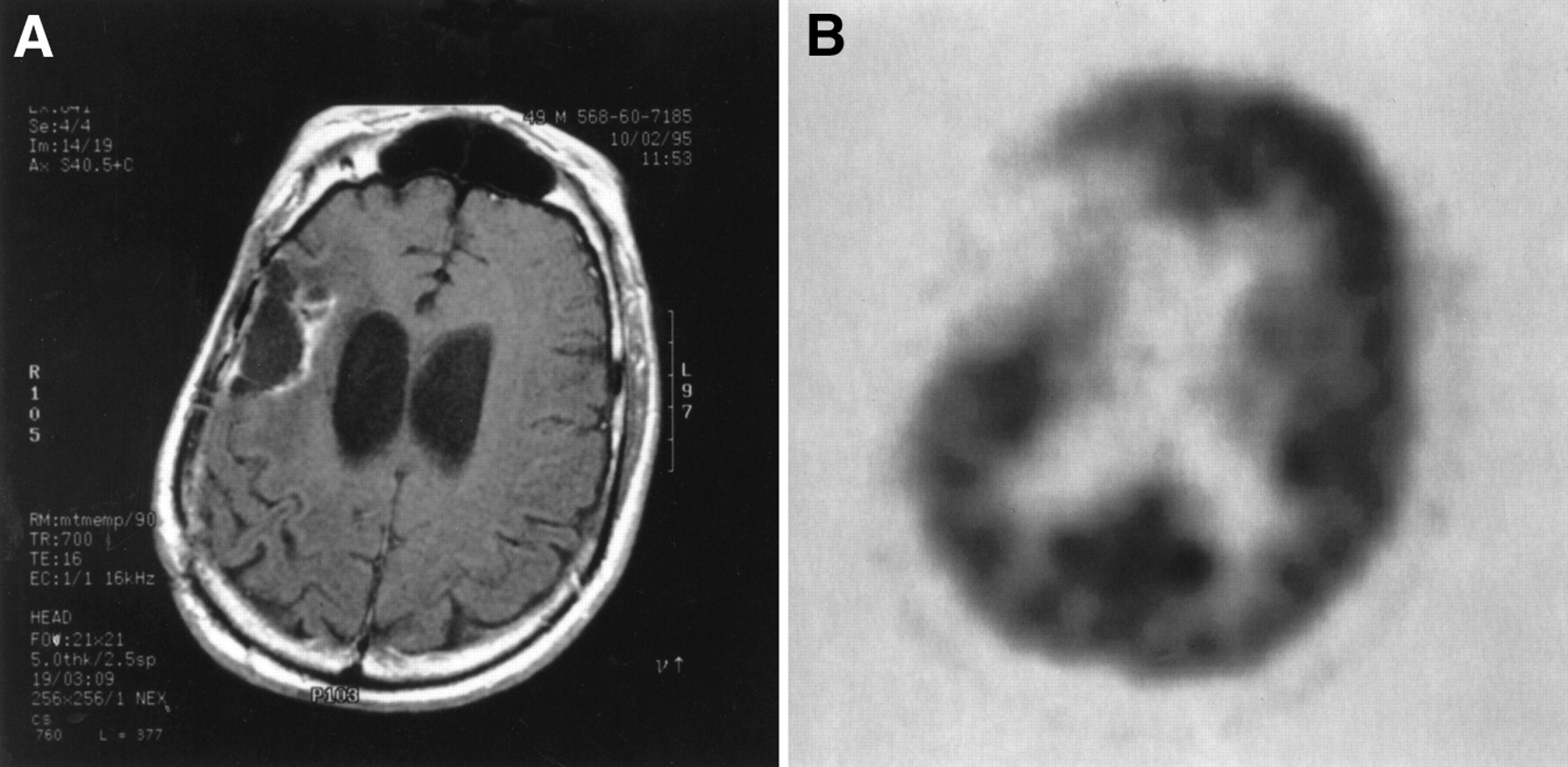
- FIGURE 2.
MR and PET scans of 50-y-old man, with a history of grade 2 right frontal oligodendroglioma, who presented with headaches and memory loss. (A) GdDTPA T1-weighted (Tr = 700, TE = 16) MR scan of 50-y-old man, showing an area of low signal in the right parietal lobe with predominantly peripheral contrast enhancement, edema, and focal areas of hemorrhage, which indicated the possibility of tumor or DLRI. (B) PET scan of patient's brain, showing hypometabolic right frontoparietal area consistent with changes after surgery and radiation. No hypermetabolic foci to suggest recurrent tumor. Tumor was resected on September 8, 1993, and treated with radiation therapy to the frontal and parietal lobes (total dose between September 29 and November 9, 1993 = 56 Gy). Patient continued to have mild cognitive deficits and psychosis. In 1995, patient developed new neurologic deficits and dementia worsened. MR showed progression of edema and enhancement in the right parietal lobe, next to the resection site. PET scan in November 1995 was negative for abnormal hypermetabolic foci; a second craniotomy was performed December 1995, and right frontoparietal cystic lesion without evidence of malignancy on a frozen section was removed. Histologic examination showed mixed astrocytoma and oligodendroglioma without mitotic activity, and with areas of focal necrosis. Patient died in February 1996.
Tables
Classification Neuroepithelial Cranial and spinal nerves Meninges Lymphomas and hematopoietic tissue Germ cell Cysts and tumor-like lesions Astrocytoma Oligodendroglioma Ependymoma Mixed choroid plexus Uncertain neuronal Pineal Embryonal Schwannoma Neurofibroma MPNST Meningioma (all variants) Anaplastic meningioma Benign mesenchymal Malignant mesenchymal Primary melanocytic Uncertain Malignant lymphoma Plasmacytoma Granulocytic sarcoma Others Germinoma Embryonal carcinoma Yolk sac Choriocarcinoma Teratoma Mixed germ cell Rathke cleft Epidermoid Dermoid Colloid Enterogenous neuroglial Granular cell Hypothalamic Hamartoma Plasma cell Granuloma MPNST, malignant peripheral nerve sheath tumor.
Kernohan (1940) Mayo/St. Anne (1981/1988) WHO grade (1979/1993) WHO designation Histopathology Grade 1 Excluded I Pilocytic astrocytoma Bipolar, piloid cells, Rosenthal fibers, eosinophilic granular bodies Grade 1 Grades 1 and 2 II Low-grade astrocytoma Neoplastic fibrillary or gemistocytic astrocytes; nuclear atypia Grade 2 Grade 3 III Anaplastic astrocytoma Neoplastic fibrillary or gemistocytic astrocytes; nuclear atypia mitotic activity Grade 3 Grade 4 Grade 4 IV Glioblastoma multiforme Cellular anaplasia, nuclear atypia, mitoses, vascular proliferation, necrosis Table modified from Kleihues (3) and Tatter (6).
Stage (time to onset) Symptoms MRI/CT PET Pathology Acute (hours to weeks) Related to mass effect and ensuing increased ICP (headache, vomiting, altered consciousness) Edema; enhancing tumor mass Hypometabolism Edema; demyelinating plaques; gray–white junction fibrin exudate; hemorrhageic coagulation necrosis and vascular proliferation Early delayed (weeks to 4 mo) Mixed 1 and 3 White matter cyst formation Hypometabolism Mixed 1 and 3 Late delayed (4 mo to years) Focal neurologic deficits depending on the size and location of the lesion Cortical atrophy Diffuse periventricular edema Expansile enhancing mass with focal hyperintensity on T2 and proton density images Hypometabolism Fibrinoid necrosis of the medium and small arteries with vascular proliferation; swollen gyri; hemorrhagic coagulation necrosis of the gray matter; white matter affected more than gray; axonal swelling, multifocal demyelination, hyalinization, and reactive gliosis Chronic Stable focal neurologic deficits as well as global effects causing personality changes and dementia Vascular dystrophic calcification with cystic changes; cortical atrophy; telangioectasia Hypometabolism Reactive gliosis; subcortical cyst formation; vasculitis, arteritis, enhanced atherosclerosis, and vascular dystrophic calcification with cystic changes Study n Pathology Sensitivity Specificity PPV NPV Patronas et al. (25) 5 Low-grade glioma 100 100 Doyle et al. (26) 9 High-grade glioma 100 100 Di Chiro et al. (17) 95 Glioma + metastases 100 100 Valk et al. (24) 38 Glioma 81 88 79 89 Janus et al. (18) 20 Glioma 83 63 77 71 Davis et al. (12) 35 Glioma, lymphoma metastases 83 No data Kahn et al. (28) 19 Glioma (n = 17), other (n = 2) 81 40 Kim et al. (27) 33 Glioma + metastases 80 94 92 85 Ricci et al. (21) 31 Glioma 86 56 80 46 PPV, positive predictive values; NPV, negative predictive values.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Rewiring of cortical glucose metabolism fuels human brain cancer growth
- Positron emission tomography and perfusion weighted imaging in the detection of brain tumors recurrence: A meta-analysis
- PET/MRI in Pediatric Neuroimaging: Primer for Clinical Practice
- Although Non-diagnostic Between Necrosis and Recurrence, FDG PET/CT Assists Management of Brain Tumours After Radiosurgery
- Multimodality Assessment of Brain Tumors and Tumor Recurrence
- Perfusion CT Imaging of Brain Tumors: An Overview
- Permeability Estimates in Histopathology-Proved Treatment-Induced Necrosis Using Perfusion CT: Can These Add to Other Perfusion Parameters in Differentiating from Recurrent/Progressive Tumors?
- An Experimental Study of Acute Radiation-Induced Cognitive Dysfunction in a Young Rat Model
- MR Spectroscopy in Radiation Injury
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- Clinical Applications of PET in Brain Tumors
- Uptake of 18F-Fluorocholine, 18F-FET, and 18F-FDG in C6 Gliomas and Correlation with 131I-SIP(L19), a Marker of Angiogenesis
- PET and SPECT for Detection of Tumor Progression in Irradiated Low-Grade Astrocytoma: A Receiver-Operating-Characteristic Analysis