


Visual Abstract
Abstract
68Ga-RM2 targets gastrin-releasing peptide receptors (GRPRs), which are overexpressed in prostate cancer (PC). Here, we compared preoperative 68Ga-RM2 PET to postsurgery histopathology in patients with newly diagnosed intermediate- or high-risk PC. Methods: Forty-one men, 64.0 ± 6.7 y old, were prospectively enrolled. PET images were acquired 42–72 min (median ± SD, 52.5 ± 6.5 min) after injection of 118.4–247.9 MBq (median ± SD, 138.0 ± 22.2 MBq) of 68Ga-RM2. PET findings were compared with preoperative multiparametric MRI (mpMRI) (n = 36) and 68Ga-PSMA11 PET (n = 17) and correlated to postprostatectomy whole-mount histopathology (n = 32) and time to biochemical recurrence. Nine participants decided to undergo radiation therapy after study enrollment. Results: All participants had intermediate- (n = 17) or high-risk (n = 24) PC and were scheduled for prostatectomy. Prostate-specific antigen was 8.8 ± 77.4 (range, 2.5–504) and 7.6 ± 5.3 ng/mL (range, 2.5–28.0 ng/mL) when participants who ultimately underwent radiation treatment were excluded. Preoperative 68Ga-RM2 PET identified 70 intraprostatic foci of uptake in 40 of 41 patients. Postprostatectomy histopathology was available in 32 patients in which 68Ga-RM2 PET identified 50 of 54 intraprostatic lesions (detection rate = 93%). 68Ga-RM2 uptake was recorded in 19 nonenlarged pelvic lymph nodes in 6 patients. Pathology confirmed lymph node metastases in 16 lesions, and follow-up imaging confirmed nodal metastases in 2 lesions. 68Ga-PSMA11 and 68Ga-RM2 PET identified 27 and 26 intraprostatic lesions, respectively, and 5 pelvic lymph nodes each in 17 patients. Concordance between 68Ga-RM2 and 68Ga-PSMA11 PET was found in 18 prostatic lesions in 11 patients and 4 lymph nodes in 2 patients. Noncongruent findings were observed in 6 patients (intraprostatic lesions in 4 patients and nodal lesions in 2 patients). Sensitivity and accuracy rates for 68Ga-RM2 and 68Ga-PSMA11 (98% and 89% for 68Ga-RM2 and 95% and 89% for 68Ga-PSMA11) were higher than those for mpMRI (77% and 77%, respectively). Specificity was highest for mpMRI with 75% followed by 68Ga-PSMA11 (67%) and 68Ga-RM2 (65%). Conclusion: 68Ga-RM2 PET accurately detects intermediate- and high-risk primary PC, with a detection rate of 93%. In addition, 68Ga-RM2 PET showed significantly higher specificity and accuracy than mpMRI and a performance similar to 68Ga-PSMA11 PET. These findings need to be confirmed in larger studies to identify which patients will benefit from one or the other or both radiopharmaceuticals.
Prostate cancer (PC) remains the most common noncutaneous cancer in American men and the second highest cause of cancer-related mortality (1). Cancer stage at diagnosis defines subsequent management. Although low-risk PC (Gleason score 6, pretreatment prostate-specific antigen [PSA] < 10 ng/mL, and clinical stage T1–T2a) may be managed with active surveillance, patients with higher grade, clinically significant cancers typically receive treatment. Imaging plays a crucial role in initial staging. Multiparametric MRI (mpMRI) is widely used for initial evaluation. However, mpMRI may miss clinically significant PC in 5%–8% (2) to 35% (3) of cases.
Molecular imaging with PET and CT (PET/CT) or PET/MRI is changing the landscape of PC staging with the development and regulatory approval of new radiopharmaceuticals. The most promising radiopharmaceuticals target prostate-specific membrane antigen (PSMA). PSMA is highly overexpressed in 90%–95% of PC (4–7). However, it is not specific to PC (8,9) and false-positive (FP) findings have been reported (10–13). Thus, there is a continued need for other imaging targets. 68Ga-RM2 is a bombesin receptor antagonist that targets the gastrin-releasing peptide receptor (GRPR) with high affinity (14). GRPR is highly overexpressed in several cancers including breast (15,16), small cell lung cancer (17), gastrointestinal stromal and neuroendocrine tumors (18,19) and in PC (20–24), especially in earlier stages, making it an attractive target for initial staging (20).
In this study we compared preoperative 68Ga-RM2 PET and mpMRI with histopathology after radical prostatectomy (RP) in patients with newly diagnosed intermediate- or high-risk PC. In a subgroup of patients, comparison with 68Ga-PSMA11 PET was also available.
MATERIALS AND METHODS
Participants
Patients scheduled to undergo RP for newly diagnosed, nontreated, intermediate- or high-risk PC were prospectively enrolled in 2 clinical trials evaluating the performance of 68Ga-RM2 (NCT03113617) and 68Ga-PSMA11 (NCT02678351). This study was approved by the local institutional review board. Written informed consent was obtained from all participants. Presurgical clinical assessments included serum PSA, Gleason score, clinical stage, and risk assessment according to the D’Amico classification (25). Patients were followed up to evaluate time to biochemical recurrence (BCR).
Scanning Protocols
68Ga-RM2 PET
Discovery 690 PET/CT (n = 19), Discovery MI PET/CT (n = 19), or SIGNA PET/MRI (n = 3) scanners (GE Healthcare) were used for 68Ga-RM2 PET. Details of PET/CT and PET/MRI acquisitions were previously described (26,27). The choice of PET/CT or PET/MRI was dictated by the funding available to support the clinical trials. Discovery MI PET/CT and SIGNA PET/MRI use the same silicon photomultiplier–based detectors, and we previously reported their clinical evaluation (28,29).
mpMRI Protocol
The protocol consisted of T2-weighted imaging, diffusion-weighted imaging, and dynamic contrast-enhanced imaging sequences using a 3T scanner (MR750; GE Healthcare). Details of mpMR image acquisition were previously described (31).
Histopathology
Hematoxylin-eosin–stained slides from whole-mount prostate specimens were analyzed according to standard of care. The slides were annotated by a genitourinary pathologist to outline areas of cancer across the entire gland.
Fusion of Histology and PET/MRI
The RAPSODI registration framework was used to align corresponding preoperative axial T2-weighted imaging, whole-mount histopathology, and 68Ga-PSMA11 PET/MRI using rigid, affine, and deformable transformations (32). This registration ensures a slice-to-slice alignment between histology—including ground-truth cancer labels—mpMRI, and PET/MRI. The methodology relies on precise prostate segmentations, automatically generated by a validated deep learning model, and its accuracy was evaluated using a Dice Similarity coefficient (33).
Image Analysis
Two nuclear medicine physicians reviewed and analyzed PET images independently and in a random, masked fashion with the knowledge that participants were scheduled to undergo RP for known PC. Any focal uptake of 68Ga-RM2 or 68Ga-PSMA11 higher than the adjacent background and not associated with physiologic accumulation was deemed suggestive of PC (34,35). The number and location of each lesion and its SUVmax were recorded. A visual comparison was performed between annotated suggestive lesions on PET and cancer-annotated histology slides. A lesion was deemed true-positive when annotations on PET and histopathology matched and considered true-negative when uptake on PET was not above background and when there was no cancer annotation on corresponding histopathology slides.
mpMRI was interpreted as standard of care using PI-RADS criteria version 2 (36). Lesions with a PI-RADS score ≥ 3 were recorded. A PI-RADS score of 3 was considered equivocal, PI-RADS 4 likely, and 5 highly likely for PC.
Statistical Analysis
A logistic regression model was used to determine the predictive value of preoperative biopsy, mpMRI, 68Ga-RM2, and 68Ga-PSMA11 PET for final histopathology and risk prediction. Sensitivity, specificity, and accuracy were stratified to intermediate- and high-risk groups for 68Ga-RM2 and 68Ga-PSMA11. A McNemar test determined difference between 68Ga-RM2 and mpMRI for sensitivity, specificity, and accuracy. A Wilcoxon signed-rank test was performed to determine differences between SUVmax. Concordance correlation was used for 68Ga-RM2 and 68Ga-PSMA11 SUVmax. The degrees of correlation are: > 0.99, almost perfect; 0.95–0.99, substantial; 0.90–0.95, moderate; and < 90, poor agreement. Spearman correlation was used for evaluation of SUVmax and time to BCR. Statistical analyses were performed with Stata (version 16.1; Stata Corp. LLC). Continuous data are presented as median ± SD, with minimum–maximum values. A P value of <0.05 was considered significant except when Bonferroni adjustment was applied for concordance analyses (P value < 0.0025 significant) and risk prediction (P value < 0.017 significant).
RESULTS
Forty-one men (age, 64.0 ± 6.7 y [range, 50–78 y]) scheduled to undergo RP for PC were prospectively enrolled. Seventeen (41.5%) participants had intermediate-risk and 24 (58.5%) had high-risk PC. PSA was 8.8 ± 77.4 ng/mL (range, 2.5–504 ng/mL) and 7.6 ± 5.3 ng/mL (range 2.5–28.0 ng/mL) when participants who received radiation therapy (RT) were excluded. PSA was undetectable 3 mo after RP in all but 3 patients. In 1 patient, preoperative biopsy was not available and PC was diagnosed by imaging and PSA. All participants (n = 41) were imaged with 68Ga-RM2 PET, 36 of 41 underwent additional mpMRI, and 17 of 41 underwent 68Ga-PSMA11 PET. Of these 41 patients, 32 underwent RP and 9 opted for RT after enrollment in the protocol and completion of the scan. Patient characteristics are shown in Table 1.
Patients’ Characteristics (n = 41)
68Ga-RM2 PET
68Ga-RM2 PET identified 70 intraprostatic foci in 40 of 41 and focal uptake in 19 nonenlarged pelvic lymph nodes in 6 of 41 patients. One participant had a negative 68Ga-RM2 PET scan result.
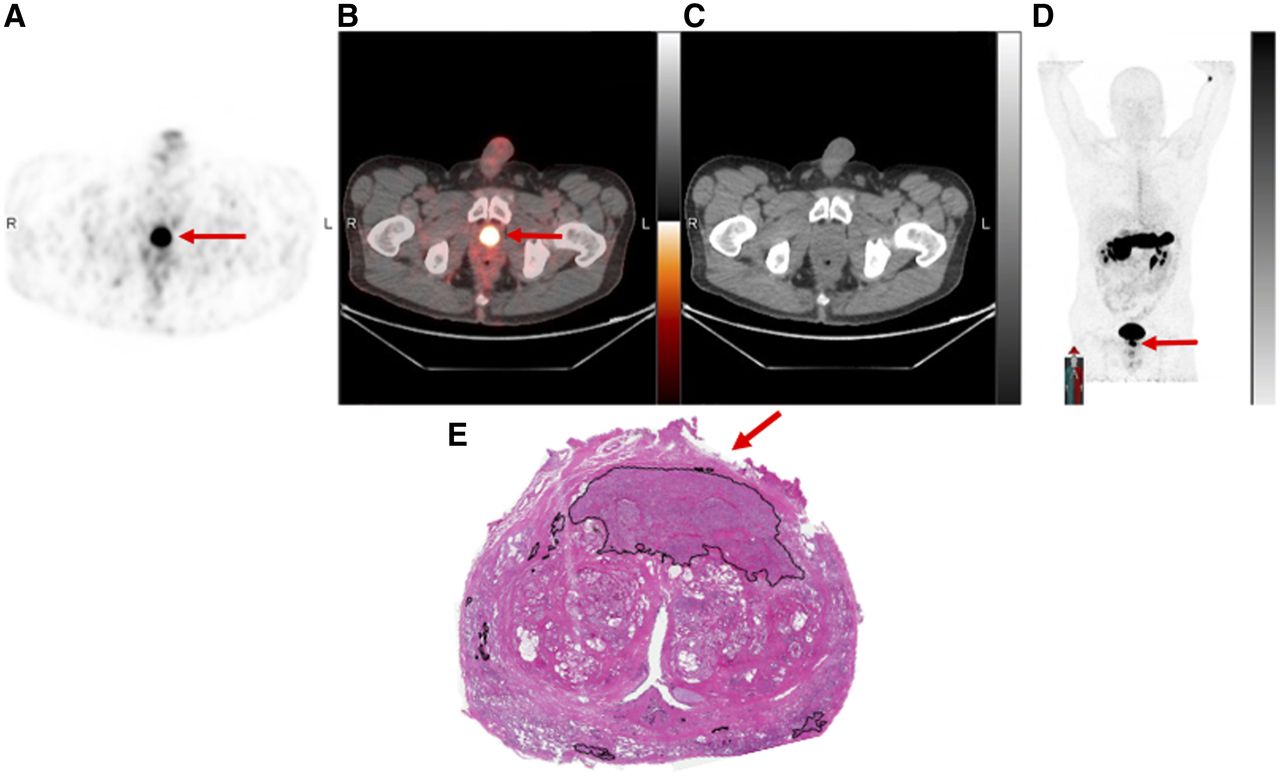
In the 32 patients who underwent RP, 68Ga-RM2 identified 54 intraprostatic foci, with 50 of 54 (92.6%) confirmed by histology (example shown in Fig. 1). Four lesions in 4 patients were false-negative (FN). A total of 527 lymph nodes were removed, of which 26 of 527 proved to be metastases in 8 participants. 68Ga-RM2 PET identified 19 lymph nodes in 6 patients, of which 16 were verified by pathology. The 3 unverified positive lymph nodes were seen in the 3 patients whose PSA did not decrease after RP, suggesting TP for metastases. Two lesions were subsequently confirmed by standard-of-care 18F-fluciclovine PET after RP.

A 50-y-old patient with intermediate-risk PC and PSA of 5.27 ng/mL. 68Ga-RM2 PET/CT (A, axial PET, fused PET/CT, CT, and maximum-intensity-projection images, respectively) shows focal uptake in left mid gland (red arrows) correlating to Gleason 4 + 3 prostate cancer (black arrow) on histology (B).
The SUVmax of histologically verified intraprostatic lesions was statistically significantly higher than that of verified lymph node metastases (P = 0.04) and benign prostatic uptake (P < 0.001). 68Ga-RM2 uptake in lymph node metastases was also significantly higher than that in benign nodes (P < 0.001). SUVmax findings are summarized in Table 2.
SUVmax of 68Ga-RM2 in Verified Intraprostatic Lesions and Lymph Node Metastases Compared with Benign Prostate and Lymph Node Uptake
mpMRI
mpMRI identified lesions in 36 of 41 participants: 43 PI-RADS ≥ 4 lesions (vs. 64 on corresponding 68Ga-RM2) in 33, and 6 PI-RADS 3 lesions (vs. 5 on corresponding 68Ga-RM2) in 3 patients. In the 30 participants who underwent RP, mpMRI detected 42 intraprostatic lesions with 38 confirmed by histopathology (vs. 50 seen and 48 verified lesions on corresponding 68Ga-RM2). One suggestive pelvic lymph node was seen and verified as PC metastasis on mpMRI (vs. 18 seen and 16 verified pelvic lymph nodes on corresponding 68Ga-RM2 PET). Four lesions were FP on histopathology, and 10 lesions were FN. Table 3 summarizes detection rates of the 3 modalities.
Lesion Detection Rates with Histopathologic Confirmation Among modalities
68Ga-PSMA11 and 68Ga-RM2 PET
In 17 participants, 68Ga-RM2 and 68Ga-PSMA11 PET identified 27 and 26 intraprostatic lesions, respectively, and 5 positive pelvic lymph nodes each. Concordance was seen in 18 intraprostatic lesions (example shown in Fig. 2) and 3 lymph nodes. Histopathology was available in 13 patients and confirmed 18 of 19 and 17 of 18 intraprostatic lesions and 4 of 5 and 3 of 5 lymph node metastases for 68Ga-RM2 and 68Ga-PSMA11, respectively. On a per-lesion analysis, 68Ga-RM2 had 1 FP and 2 FN intraprostatic lesions, whereas 68Ga-PSMA11 had 1 FP and 3 FN. Six patients had incongruent uptake (examples shown in Supplemental Figs. 1 and 2; supplemental materials are available at http://jnm.snmjournals.org): cancer was present in 5 of 6 lesions on 68Ga-RM2 versus 3 of 4 on 68Ga-PSMA11.

A 65-y-old man, presenting with PSA of 9.5 ng/mL and Gleason 3 + 4 lesion on presurgery biopsy. 68Ga-PSMA11 PET/MRI (A) and 68Ga-RM2 PET/CT (B) axial PET, fused PET/CT, CT, and maximum-intensity-projection images, respectively, show concordant focal uptake in left anterior apex of prostate (arrows), correlating to Gleason 3 + 3 on histology (C, arrow).
68Ga-PSMA11 SUVmax of verified PC was significantly higher than that of lymph node metastases (P = 0.002). No statistically significant differences were noted when comparing SUVmax for 68Ga-RM2 with 68Ga-PSMA11 for intraprostatic cancers (P = 0.43) or lymph node metastases (P = 0.25). 68Ga-RM2 and 68Ga-PSMA11 were poorly correlated between the left and right prostate. Table 4 summarizes 68Ga-RM2 and 68Ga-PSMA11 findings.
Correlation of 68Ga-RM2 and 68Ga-PSMA11 PET in 17 Patients and Comparison to Histopathologic Outcome in 13 Patients
Sensitivity, Specificity, and Accuracy
All 3 modalities—68Ga-RM2, 68Ga-PSMA11 PET, and mpMRI—were significant predictors for PC (P ≤ 0.0025). For intraprostatic lesions, both 68Ga-RM2 and 68Ga-PSMA11 had higher sensitivity and accuracy rates than mpMRI, whereas specificity was highest for mpMRI (Supplemental Table 1). For intraprostatic and lymph node lesions, specificity increased for both radiopharmaceuticals, whereas sensitivity decreased for 68Ga-PSMA11 (Supplemental Table 2). Significantly higher sensitivity (P = 0.01) and accuracy (P < 0.01) were seen for 68Ga-RM2 PET than for mpMRI.
Sensitivity, specificity, and accuracy for 68Ga-RM2 were slightly higher for the high-risk than for the intermediate-risk group. For 68Ga-PSMA11, the opposite was found (Supplemental Table 3).
For the relationship and predictive value of PSA (grouped into <5, 5–10, 10.1–15, and ≥15 ng/mL), PI-RADS (3, ≥4), and SUVmax for histopathologic outcome, the only significance found was a higher SUVmax of 68Ga-RM2 in PSA ≥5 versus PSA <5 (P < 0.0025, Fig. 3).

Boxplot of 68Ga-RM2 SUVmax stratified to PSA < 5 ng/mL and ≥ 5 ng/mL. Patients with PSA ≥ 5 ng/mL had a statistically significantly higher SUVmax (P = 0.0025).
Follow-up
Six patients were lost in follow-up. After RP, patients (n = 26) were followed for 28.6 ± 11.7 mo (range, 7.0–47.3 mo). PSA remained undetectable in 15 patients, whereas 11 developed BCR 17.7 ± 10.8 mo (range, 2.8–32.0 mo) after RP. 68Ga-RM2 SUVmax of intraprostatic lesions and time to BCR were negatively correlated (r = −0.34), meaning the lower the SUVmax, the longer the time to BCR. The correlation of PSA and time to BCR was also negatively correlated (r = −0.25), indicating the lower the PSA, the longer the time to BCR.
DISCUSSION
In this study, we prospectively compared GRPR-targeting 68Ga-RM2 PET with whole-mount histopathology after RP in patients with newly diagnosed PC. Sensitivity and accuracy were high for 68Ga-RM2 at 98% and 89%, respectively, and were comparable to those for 68Ga-PSMA11 and superior to those for mpMRI. However, a specificity of 65% was lower than that for mpMRI. These results were comparable to previously reported sensitivity, specificity, and accuracy rates of 89%, 81%, and 83% for prostatic lesions and sensitivity of 70% for lymph node metastases for 68Ga-RM2 PET/CT in a smaller cohort of 14 men with primary PC and 3 with BCR (37).
68Ga-RM2 and 68Ga-PSMA11 both showed high detection rates for primary PC and lymph node metastases but were poorly correlated. A recently published study compared 68Ga-RM2 and 68Ga-PSMA11 PET/MRI in staging of 19 men with biopsy-proven high-risk PC, with histopathology available in 12 patients. Although the detection rate of 95% for the primary tumor is similar that in to our study, the positivity rates for lymph nodes were lower (37% for 68Ga-PSMA11, 21% for 68Ga-RM2). Apart from a negative 68Ga-RM2 finding in 1 participant, concordant uptake was seen between 68Ga-RM2 and 68Ga-PSMA11 (38). The incongruent uptake pattern in our cohort might be due to our more heterogeneous groups of intermediate- and high-risk PC. However, the difference in expression pattern of PSMA and GRPR is consistent with our previous findings in BCR PC (30,39) and is supported by immunohistochemistry showing that GRPR and PSMA expression are not correlated (40). Fassbender et al. found in a voxel-based approach that 68Ga-RM2 and 68Ga-PSMA11 in 8 patients with primary PC showed similar averaged SUVmean; however, on a per-patient basis, they found a different intensity, revealing again a different expression pattern of GRPR and PSMA (41).
We found no correlation between 68Ga-RM2 uptake and Gleason score or tumor volume, but a positive correlation between PSA and 68Ga-RM2 SUVmax. SUVmax was also negatively correlated to time to BCR. This negative correlation is supported by previous findings in patients with BCR PC showing a positive correlation between 68Ga-RM2 positivity and PSA and PSA velocity and, conversely, a negative correlation of SUVmax and PSA with time to BCR indicating that the higher 68Ga-RM2 SUVmax and PSA, the shorter the time to BCR (27). However, there is controversy (24) as to whether GRPR density is related to a better prognosis of PC (20,21) or found in high-risk tumors as our results indicate. Larger studies with a longer follow-up are needed to understand these possible correlations.
The need now is to understand if and how these radiopharmaceuticals may provide complementary and useful information in patients with PC at various stages and risks. Given the high tumor heterogeneity in PC, and that neither 68Ga-RM2 nor 68Ga-PSMA11 are 100% sensitive or specific and hence attributing to FP and FN lesions, a bispecific tracer that targets GRPR and PSMA simultaneously may present a promising imaging option (42).
Limitations of this study include the relatively small number of patients, especially of participants undergoing both 68Ga-RM2 and 68Ga-PSMA11 PET, and the different imaging modalities used, that is, different PET/CT scanners and PET/MRI. In addition, not all participants had histopathology data available because some elected to undergo RT. Correlating lymph node positivity to histopathology is a challenge because not all lymph nodes seen on PET were resected. PET data were analyzed by readers who were aware that participants were scheduled to undergo RP for known PC, whereas readers for mpMRI were unaware that participants were scheduled for RP as mpMRI was part of clinical care for PC diagnosis.
CONCLUSION
68Ga-RM2 PET accurately detects intermediate- and high-risk primary PC with a significantly higher specificity and accuracy than mpMRI and a performance similar to 68Ga-PSMA11 PET. The poor correlation between 68Ga-RM2 and 68Ga-PSMA11 underline the different expression patterns of GRPR and PSMA and the complex tumor biology of PC. Larger prospective studies are needed to identify which patients will benefit from one, the other, or both radiopharmaceuticals.
DISCLOSURE
The study was partially supported by GE Healthcare. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 68Ga-RM2 PET a useful tool in the initial staging of PC?
PERTINENT FINDINGS: Forty-one patients with newly diagnosed PC underwent 68Ga-RM2 PET; a subgroup also underwent mpMRI (n = 36) and 68Ga-PSMA11 PET (n = 17). 68Ga-RM2 PET showed high sensitivity, accuracy, and detection rates of 98%, 89%, and 93%, respectively. Specificity at 65% was lower than that of mpMRI (75%). Poor correlation to 68Ga-PSMA11 indicates the different expression patterns of GRPR and PSMA in PC.
IMPLICATIONS FOR PATIENT CARE: 68Ga-RM2 PET accurately detected intermediate- and high-risk primary PC with a significantly higher sensitivity and accuracy than that mpMRI and a performance similar to that of 68Ga-PSMA11 PET. Larger prospective studies are needed to identify which patients will benefit from one, the other, or both radiopharmaceuticals.
Footnotes
Published online May. 12, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 2, 2022.
- Revision received May 10, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Additive Value of [68Ga]Ga-RM26 PET/CT to [68Ga]Ga-PSMA-617 PET/CT in Detecting Pelvic Lymph Node Metastasis in Prostate Cancer: A Prospective, Single-Center, Phase II Study
- A Pilot Study of 68Ga-PSMA11 and 68Ga-RM2 PET/MRI for Biopsy Guidance in Patients with Suspected Prostate Cancer
- A Pilot Study of 68Ga-PSMA11 and 68Ga-RM2 PET/MRI for Evaluation of Prostate Cancer Response to High-Intensity Focused Ultrasound Therapy
- Comparison of 68Ga-PSMA-617 PET/CT and 68Ga-RM2 PET/CT in Patients with Localized Prostate Cancer Who Are Candidates for Radical Prostatectomy: A Prospective, Single-Arm, Single-Center, Phase II Study