


Visual Abstract
Abstract
Prostate-specific membrane antigen (PSMA) PET offers an accuracy superior to other imaging modalities in initial staging of prostate cancer and is more likely to affect management. We examined the prognostic value of 68Ga-PSMA-11 uptake in the primary lesion and presence of metastatic disease on PET in newly diagnosed prostate cancer patients before initial therapy. Methods: In a prospective study from April 2016 to December 2020, 68Ga-PSMA-11 PET/MRI was performed in men with a new diagnosis of intermediate- or high-grade prostate cancer who were candidates for prostatectomy. Patients were followed up after initial therapy for up to 5 y. We examined the Kendall correlation between PET (intense uptake in the primary lesion and presence of metastatic disease) and clinical and pathologic findings (grade group, extraprostatic extension, nodal involvement) relevant for risk stratification, and examined the relationship between PET findings and outcome using Kaplan–Meier analysis. Results: Seventy-three men (age, 64.0 ± 6.3 y) were imaged. Seventy-two had focal uptake in the prostate, and in 20 (27%) PSMA-avid metastatic disease was identified. Uptake correlated with grade group and prostate-specific antigen (PSA). Presence of PSMA metastasis correlated with grade group and pathologic nodal stage. PSMA PET had higher per-patient positivity than nodal dissection in patients with only 5–15 nodes removed (8/41 vs. 3/41) but lower positivity if more than 15 nodes were removed (13/21 vs. 10/21). High uptake in the primary lesion (SUVmax > 12.5, P = 0.008) and presence of PSMA metastasis (P = 0.013) were associated with biochemical failure, and corresponding hazard ratios for recurrence within 2 y (4.93 and 3.95, respectively) were similar to or higher than other clinicopathologic prognostic factors. Conclusion: 68Ga-PSMA-11 PET can risk-stratify patients with intermediate- or high-grade prostate cancer before prostatectomy based on degree of uptake in the prostate and presence of metastatic disease.
- oncology: GU
- PET
- PET/MRI
- prostate cancer
- biochemical recurrence
- prostate-specific membrane
- antigen
- prostatectomy
Patients diagnosed with localized prostate adenocarcinoma have generally prolonged natural history, although some patients experience rapid progression after initial curative intent prostatectomy or radiation therapy. Initial risk stratification affects treatment decisions and subsequent management of prostate cancer patients. Risk stratification is primarily based on clinical tumor stage, histologic grade group, and the prostate-specific antigen (PSA) level (1), although incorporating molecular markers is increasingly being considered (2). Imaging is indicated in all men with unfavorable intermediate-, high-, or very-high-risk disease (3,4). The presence of nodal or distant metastatic disease on cross-sectional imaging or bone scintigraphy affects management and prognosis. Prostate-specific membrane antigen (PSMA) PET/CT or PET/MRI has significantly better sensitivity and higher diagnostic yield for detection of metastatic disease (5,6). Unfortunately, the outcome data on patients with metastasis that is occult on anatomic imaging and bone scintigraphy are sparse. Extrapolation of data from prostatectomy and pelvic nodal dissection suggests that prognosis of patients with nodal metastasis could be variable (7). After prostatectomy, even in node-positive patients, 75% achieve complete biochemical response and are at low risk for recurrence and caner specific mortality (8). There is a need for prognostic models to identify patients at risk for persistent or recurrent disease based on PET versus others who do not benefit from overtreatment.
We and others have examined the clinical utility of pretherapy vertex to mid-thigh 68Ga-PSMA-11 PET as a part of PET/MRI in newly diagnosed prostate cancer patients and correlation with histopathology (9–11). We now examine the association between PET findings and outcomes/biochemical recurrence after initial therapy.
MATERIALS AND METHODS
Patient Population
The study protocol was approved by the Stanford University Institutional Review Board, and all subjects signed a written informed consent form. Patients with newly diagnosed intermediate- or high-risk prostate cancer (PSA ≥ 10 ng/mL, cT2b or greater, or Gleason score ≥ 7) who were scheduled for radical prostatectomy were enrolled from April 2016 until December 2020 (NCT02678351). The protocol has been described previously (11). Exclusion criteria were androgen deprivation therapy, neoadjuvant chemotherapy, or radiation therapy before the planned prostatectomy.
PET/MR Imaging Protocol
68Ga-PSMA-11 was prepared as described previously (11,12). The mean ± SD administered dosage was 160.8 ± 31.1 MBq (range, 91.4–236.4 MBq). After an uptake time of 50.0 ± 8.9 min (range, 40–108 min), patients were imaged from mid-thighs to vertex using a time-of-flight simultaneous PET/MR scanner (SIGNA; GE Healthcare) in 3-dimensional mode for 4 min per bed position in 5–9 beds. Delayed pelvic PET/MRI including prostate multiparametric MRI (mpMRI) was obtained after voiding, at 70.5 ± 13.4 min (range, 43–108 min) after the initial scan. A 2-point Dixon 3-dimensional T1-weighted spoiled gradient-echo MR sequence was acquired using the volume coil for MR-attenuation correction.
Image Analysis
PET images acquired before October 2017 (33 patients) were independently reviewed in correlation with MRI by 2 nuclear medicine physicians with 13 and 5 y of experience (11). Subsequent studies were reviewed by one of the original nuclear physicians (with more than 13 y of experience) using MIM (version 7; MIM Software Inc.). PET findings were communicated with the referring surgeon and the information was used as a part of clinical decision making. SUVs normalized based on body weight were measured for prostate lesions and physiologic activity in liver, spleen, right parotid gland, and mediastinal blood pool separately by a radiologist/nuclear medicine physician (with 10 y of experience). For prostate lesions, SUVmax and SUVpeak were recoded for initial images, and SUVmax was recorded for delayed images. Physiologic activity was recorded using SUVmean per Prostate Cancer Molecular Imaging Standardized Evaluation recommendations (13). Lesion PSMA index was calculated using SUVpeak comparison with blood pool and liver activity (14).
Outcome Analysis
Biochemical persistence and recurrence were assessed via review of all available electronic medical records (including PSA results and clinical notes). Biochemical failure was defined as PSA ≥ 0.4 ng/mL after prostatectomy or persistent PSA that was followed by adjuvant therapy. Recurrence was defined as a rise in PSA at least 6 wk after radical prostatectomy with or without adjuvant therapy measuring ≥ 0.2 ng/mL that was subsequently confirmed by a follow-up measurement (15) or any rise in PSA that was treated with salvage therapy.
Statistical Analysis
Analysis was performed using MATLAB (R2021B) Statistics and Machine Learning toolbox (The MathWorks). A multistep analysis was performed. PET findings were dichotomized (low vs. high uptake in the primary lesion, presence of metastatic disease). We next examined the correlation between PET findings and clinical and pathologic parameters in prostate cancer risk stratification. Finally, we examined the relationship between PET findings and outcomes.
There is no a priori threshold for dichotomizing uptake in prostate although uptake higher than twice activity in normal liver parenchyma has been suggested for metastatic lesions (13,14). To explore a basis for thresholding of the primary prostate lesion (or the dominant lesion if more than one lesion were present), we used histogram and cluster analysis. The Shapiro–Wilk test was used to examine normality of SUVmax distribution. We subsequently used cluster analysis of the SUVmax based on L1-norm (k-medians) with k = 2. The resulting categories (low vs. high uptake) were stable for SUVmax < 12.5 (n = 40) or SUVmax > 20 (n = 13), but classification was variable for SUVmax between 12.5 and 20 (i.e., k-median results depended on initial state, n = 20). We used an SUV of 12.5 as the cutoff threshold for future analysis, which is close to twice average normal liver activity (11.88 g/mL) in our patients, and more evenly divided the patients into low- and high-uptake groups compared with a higher cutoff value.
We also explored reliability of physiologic uptake that can define an internal reference per subject (16). Coefficient of variation was used to examine the variability of physiologic uptake. Person correlation coefficient was used to estimate the contribution of factors that systematically affect physiologic uptake in different organs to the overall variability of physiologic uptake.
Metastatic disease on 68Ga-PSMA-11 PET/MRI was categorized as absent versus present (regardless of number of metastases). For clinical parameters, conventional categories were used (PSA level: <10, 10–20, >20; clinical tumor stage: T1–2a, T2b/c, ≥T3; grade group: 2, 3, ≥4) (17).
Kendall τ was used to assess correlation between PET findings and clinical and pathologic parameters. A cutoff value of P < 0.05 was used for significance. The Kruskal–Wallis H test was used to examine whether a similar number of nodes were sampled during pelvic dissection between various groups.
Survival Analysis
The relationship between PET findings and outcomes was analyzed using Kaplan–Meier survival plots and log-rank test using MatSurv (https://github.com/aebergl/MatSurv) (18).
RESULTS
Patient Characteristics and Pathologic Findings
Seventy-five men were enrolled in this study (Fig. 1). One patient was excluded because of equipment failure. No imaging could be done in one patient, and PET/MRI was terminated early (after acquisition of pelvis and lower abdomen) in another patient because of claustrophobia. The data for prostate lesions and regional lymph nodes include 73 patients (Tables 1 and 2). The data for distant metastasis and physiologic uptake include 72 patients.

Study diagram.
Clinical Characteristics of Patients Included in Study (n = 73)
Gleason Score and Clinical Stage of Patients Included in Study
Sixty-five patients underwent prostatectomy 12.4 ± 15.4 d (median, 7 d; range, 1–95 d) after PET. In all cases, clinically significant prostate cancer was confirmed. On average, 14.83 ± 10.84 lymph nodes (median, 13; range, 0–54) from 64 patients were submitted for pathologic examination. The Gleason grade group after prostatectomy correlated with grade group based on initial biopsy (Kendall τ = 0.42, P = 0.0002), and was unchanged, revised up, or revised down after prostatectomy in 32, 26, and 5 patients, respectively (Table 3.
Initial Biopsy Versus Prostatectomy
In 72 of 73 patients, follow-up data were available (34.4 ± 15.49 mo after PET; median, 35.91 mo; range, 4.86–60.7 mo). Persistent disease (based on PSA failure) was documented in 10 patients after prostatectomy and 4 after other treatments. Biochemical recurrence (after initial complete response) was documented in 14 patients after prostatectomy and in 6 patients after prostatectomy and adjuvant therapy.
PET Findings
Except for 1 patient, focal uptake was identified within the prostate gland. In 7 patients (including a patient with negative PET results) MI showed more lesions, and in 26 patients PET showed more lesions. For the remaining patients, a PET-positive lesion was congruent with mpMRI in 36 patients and incongruent in 1 (Table 4). In 20 patients (27.4%), PET showed focal uptake outside the prostate consistent with metastatic disease in 66 lesions (3.3 ± 4.6 sites per patient; median, 1; range, 1–19) (Table 5).
Laterality of PSMA-Avid Lesion Versus PIRADS 4 or 5 Lesions on Prostate mpMRI
Positivity Versus Number of Lymph Nodes Removed During Pelvic Nodal Dissection
Metastatic Disease on PET Versus Pelvic Dissection
Of 16 patients with pathologically proven N1 disease, 9 had PSMA metastasis (56% per patient sensitivity). There were 9 patients for whom nodal dissection did not reveal metastasis (pN0) but who had PSMA metastasis. The extent of a pelvic lymph node dissection confounds the probability of positive lymph nodes. Patients with PSMA metastasis and negative pelvic dissection had on average less than half of the number of lymph nodes sampled compared with patients for whom both PET and pelvic dissection showed metastatic disease, or only pelvic dissection showed metastatic disease (11.7 ± 5.2 vs. 24.4 ± 13.1 and 27.3 ± 15.7, respectively, P = 0.012, Kruskal–Wallis test). The per-patient 68Ga-PSMA-11 PET/MRI positivity rate was 2.5 times higher than pelvic nodal dissection when 5–15 nodes were surgically sampled (Table 5).
Degree of 68Ga-PSMA-11 Uptake
For prostate lesions (dominant lesion if multiple lesions are present), the SUVmax was 14.53 ± 10.42 (median, 10.64; range, 3.61–50.12 g/mL) and the SUVpeak was 9.18 ± 7.21 (median, 6.69; range, 2.13–40.24 g/mL). Figure 2A depicts the histogram of SUVmax of the dominant prostate lesion in our dataset. The distribution is asymmetric and nongaussian (P < 0.001, Shapiro–Wilk test). A cutoff value of 12.5 (∼55th percentile) was used for subsequent analysis as the threshold for high uptake. Uptake on initial PET and delayed pelvic PET was highly correlated (r = 0.968, Fig. 2B) and followed a similar distribution, with the equivalent delayed SUV cutoff of 13.5.

Uptake in primary prostate cancer versus physiologic uptake. (A) Histogram of SUVmax of primary lesion on initial PET. (B) Correlation between early and delayed SUVmax. (C) Average uptake in blood pool, liver, spleen, and right parotid gland (error bars indicate SD). *Lesion uptake (using SUVmax) is also plotted for comparison (white bar). (D) Poor within-subject correlation between liver and spleen uptake.
The average uptake in liver, spleen, blood pool, and parotid gland were 5.94 ± 1.53, 9.33 ± 3.11, 1.26 ± 0.24, and 16.08 ± 3.94 g/mL, respectively (corresponding to interpatient coefficients of variation of 0.26, 0.34, 0.19, and 0.25, respectively; Fig. 2C). SUVmax or SUVpeak of the prostate lesion did not correlate with physiologic uptake in the liver, spleen, blood pool, or parotid gland (r < 0.12 for all tests). Correlation between physiologic uptake in various organs was weak, with the highest between liver and spleen (r = 0.224, P = 0.058; Fig. 2D).
Relationship Between PET Findings and Clinicopathologic Risk Factors
Uptake in the primary lesion and presence of PSMA metastasis correlated with several clinical and pathologic factors as detailed in Table 6. The notable exception was a nonsignificant correlation between clinical or pathologic T stage (extraprostatic extension) and PET findings (in contrast to the study of Lima et al. (19)). High uptake in the primary lesion correlated more with preprostatectomy PSA level and D’Amico risk category whereas PSMA metastasis correlated more with grade group and nodal involvement.
Cross-Tabulation of the Relationship Between PET Findings and Clinical or Pathologic Risk Factors in Prostate Cancer
Relationship Between PET Findings and Outcome
High uptake (SUVmax > 12.5) and presence of PSMA metastasis were associated with biochemical failure or rapid recurrence within 2 y after prostatectomy. In contrast, patients with low uptake in the primary lesion who did not have evidence of metastatic disease on PET had low likelihood of experiencing recurrence within the follow-up period (Fig. 3). The outcomes were worse in patients with high uptake in the primary lesion and PSMA metastasis (Fig. 4). Results were similar when the analysis included all patients rather than only patients who underwent prostatectomy (P = 0.008 for uptake in primary, P = 0.0135 for PSMA metastasis, and P = 0.001 for the combination of the two). Alternative measures of uptake using body surface area and lean body mass also showed significant differences in survival (P < 0.05) between high and low uptake when a comparable cutoff threshold (about 55 percentile of corresponding population values) was used. Neither SUVpeak nor lesion index (14) (defined based on SUVpeak) reached statistical significance.

Kaplan–Meier Analysis for disease free survival after prostatectomy according to uptake of primary lesion (A) (SUVmax on initial PET), and presence of metastatic disease on PET (B). Censored events are marked with a tick.

Kaplan–Meier Analysis for disease-free survival after prostatectomy as a function of uptake in primary cancer and presence of metastatic disease. Patient with both high uptake in primary cancer and metastatic disease on PET had worse survival than patient who had no or only 1 risk factor. *Exclusive disjunction.
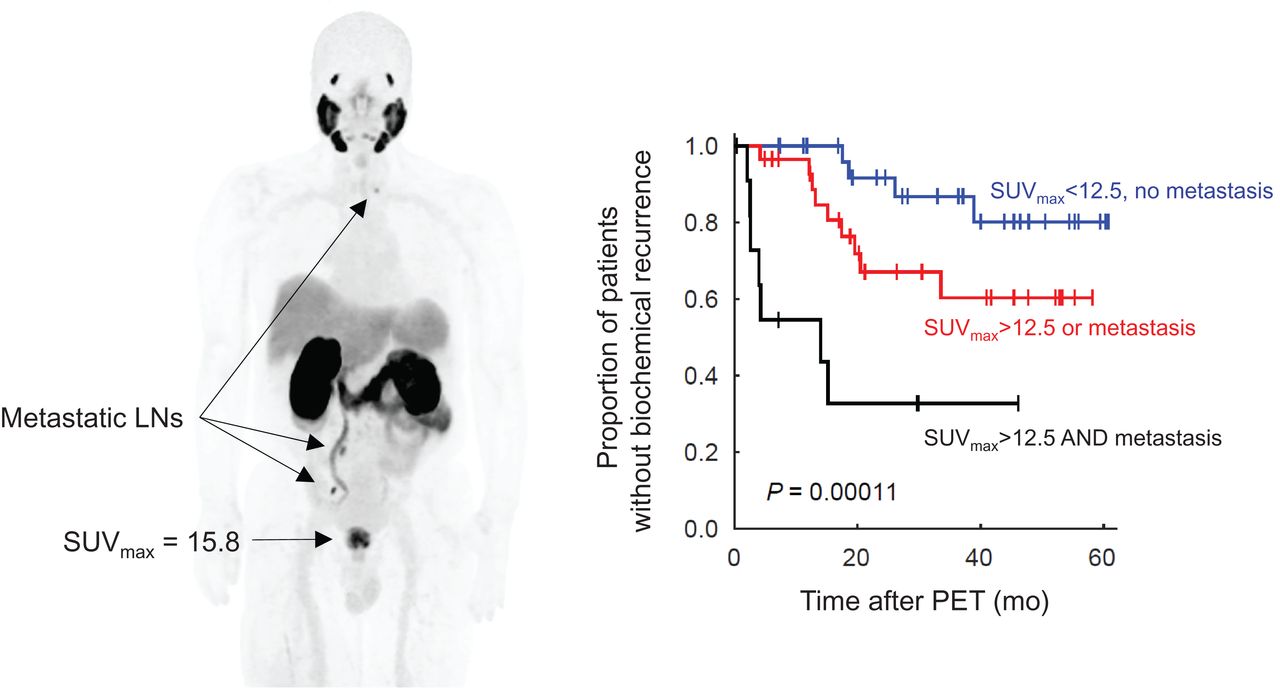
PET findings correlated with the duration of biochemical response after initial therapy (including adjuvant therapy) (Fig. 5). The hazard ratio for PET compared with clinicopathologic factors for biochemical recurrence within the first 24 mo are depicted in Table 7. High uptake in the primary cancer and presence of PSMA-avid metastasis were associated with higher hazard ratios for early recurrence compared with clinicopathologic factors, although our sample is too small to allow for statistical comparison and testing independence. Kaplan–Meier survival analysis showed worse outcome for patients with bilateral disease in the prostate (based on either PET or MRI) or if PET and MRI results were incongruent (P = 0.125, not significant).

Proportion of patients without biochemical progression after initial treatment with or without adjuvant radiation therapy over time according to uptake of primary prostate lesion (A), presence of metastatic disease on PET (B), or combination of them (C). *Exclusive disjunction.
Prognostic Factors for Biochemical Recurrence Within 24 Months After Initial Response
DISCUSSION
In patients with newly diagnosed intermediate- or high-risk prostate cancer who were candidates for radical prostatectomy, 68Ga-PSMA-11 PET/MRI findings were closely linked with clinical and pathologic risk factors. High 68Ga-PSMA-11 uptake in the primary lesion and presence of PSMA-avid metastatic disease were negatively associated with response to initial therapy and duration of biochemical response. Our findings add to the evidence of the utility of PSMA PET in the initial workup of prostate cancer and correlation between PSMA expression and tumor behavior (20).
Dedicated prostate MRI was performed in the same session in conjunction with PET and helped identify prostate lesions (particularly lesions with very low uptake). Uptake and conspicuity increase on delayed PET. Nonetheless, most lesions were readily visible on the initial PET, including lesions that were identified only on PET or lesions with indeterminate appearance on mpMRI that were not prospectively called. Although survival analysis did not use MRI findings, scanner hardware, attenuation correction methodology, and postprocessing affect image quality and SUV measurements, which should be considered before applying our results to data from PET/CT or other PET/MRI systems.
A PSMA PET sensitivity of 56% for nodal involvement here is in line with that of other studies (21,22). Therefore, the absence of PSMA metastasis does not indicate that a pelvic nodal dissection is not required (23). Several patients had nodal involvement on PET that was not confirmed pathologically. PSMA PET has high specificity (23–26), so we suspected undersampling, corroborated by our analysis. Accurate surgical staging requires extensive lymphadenectomy, which increases surgical morbidity. The positivity rate of PET in our study was 2.5 times higher than limited pelvic dissection (sampling up to 15 lymph nodes), and only slightly lower than extensive pelvic nodal dissection (52% vs. 62%). Therefore, PSMA PET could be supplementary to surgical pathology in staging patients undergoing nodal dissection, particularly if for any reason extensive nodal dissection is not performed. Our survival analysis also suggests that despite limited sensitivity, the prognostic value of PSMA PET (in terms of hazard ratio of biochemical recurrence) can be comparable to pathologic nodal staging given variable prognosis of pN1 disease (7).
PSMA expression and histologic tumor grade are linked (27) and PSMA plays a complex role in tumor progression (28), which is consistent with our finding of slower progression in patients with low uptake in the primary tumor. Low PSMA expression could reduce the sensitivity of PET for metastatic disease but might have little impact on the overall prognostic value of PSMA PET if cancers with low PSMA expression would have low probabilities for metastatic spread in the first place. 68Ga-PSMA-11 uptake and grade group were correlated in our data (Table 6), which partially explains better prognosis in patients with low uptake in the prostate. Nonetheless, for every grade group, we noticed that those with an SUVmax < 12.5 tended to have longer recurrence-free survivals. Larger studies could shed light into the value of incorporating PSMA uptake in prognostic models of prostate cancer in addition to histologic grade. This question could be particularly relevant in patients who decide not to undergo prostatectomy because in nearly half our patients, the grade group based on initial biopsy changed after prostatectomy.
To simplify our analysis, we categorized uptake to low versus high. Variations on how this was done (e.g., normalizing based on lean body mass instead of weight) did not affect our results, although using SUVpeak (which could underestimate uptake in small lesions) did have an impact on the results. Uptake categorization and Kaplan–Meier analysis was reproducible on repeated PET/MRI of the pelvis performed after voiding, suggesting that SUVmax was a sufficiently robust measure in our study (29). Dichotomizing a continuous variable is, however, associated with certain issues such as loss of information (30), and further studies may be needed to confirm the relationship between SUV and duration of biochemical response.
A limitation of our study is that we did not examine how PET findings affected management. Heterogeneity in initial treatment strategies in prostate cancer can confound survival analysis. A few patients elected not to undergo prostatectomy and pursed other treatments after PET. Exclusion of these patients did not change the survival analysis results. As the role of PSMA PET in initial evaluation of patients with prostate cancer evolves, our results point to opportunities for optimizing treatment strategies in patients with high uptake in the primary lesion or with metastatic disease on PET.
CONCLUSION
PSMA PET in initial evaluation of patients with intermediate- and high-risk prostate cancer correlates with the probability of biochemical failure or recurrence at least as well as clinical and pathologic factors. Patients with low uptake in prostate lesions and no evidence of metastatic disease on PET are unlikely to have recurrence within the first 2 y after initial treatment. Patients with high uptake in prostate cancer and metastatic disease are at risk for early recurrence and may require frequent surveillance and aggressive treatments.
DISCLOSURE
This study was partially supported by GE Healthcare. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 68Ga-PSMA-11 PET useful in the assessment of risk for failure after prostatectomy or early biochemical recurrence?
PERTINENT FINDINGS: High 68Ga-PSMA-11 uptake in primary prostate cancer and the presence of PSMA-avid metastatic disease on PET are significant adverse prognostic factors after initial therapy.
IMPLICATION FOR PATIENT CARE: 68Ga-PSMA-11 PET has higher positivity rate than limited pelvic lymphadenectomy for metastatic disease and identifies patients who could benefit from additional treatment or frequent surveillance.
ACKNOWLEDGMENTS
We thank Simon John Christoph Soerensen and Tie Liang for comments and suggestions on earlier versions of the manuscript.
Footnotes
Published online May. 5, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 18, 2022.
- Revision received April 22, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.