


Article Figures & Data
Figures
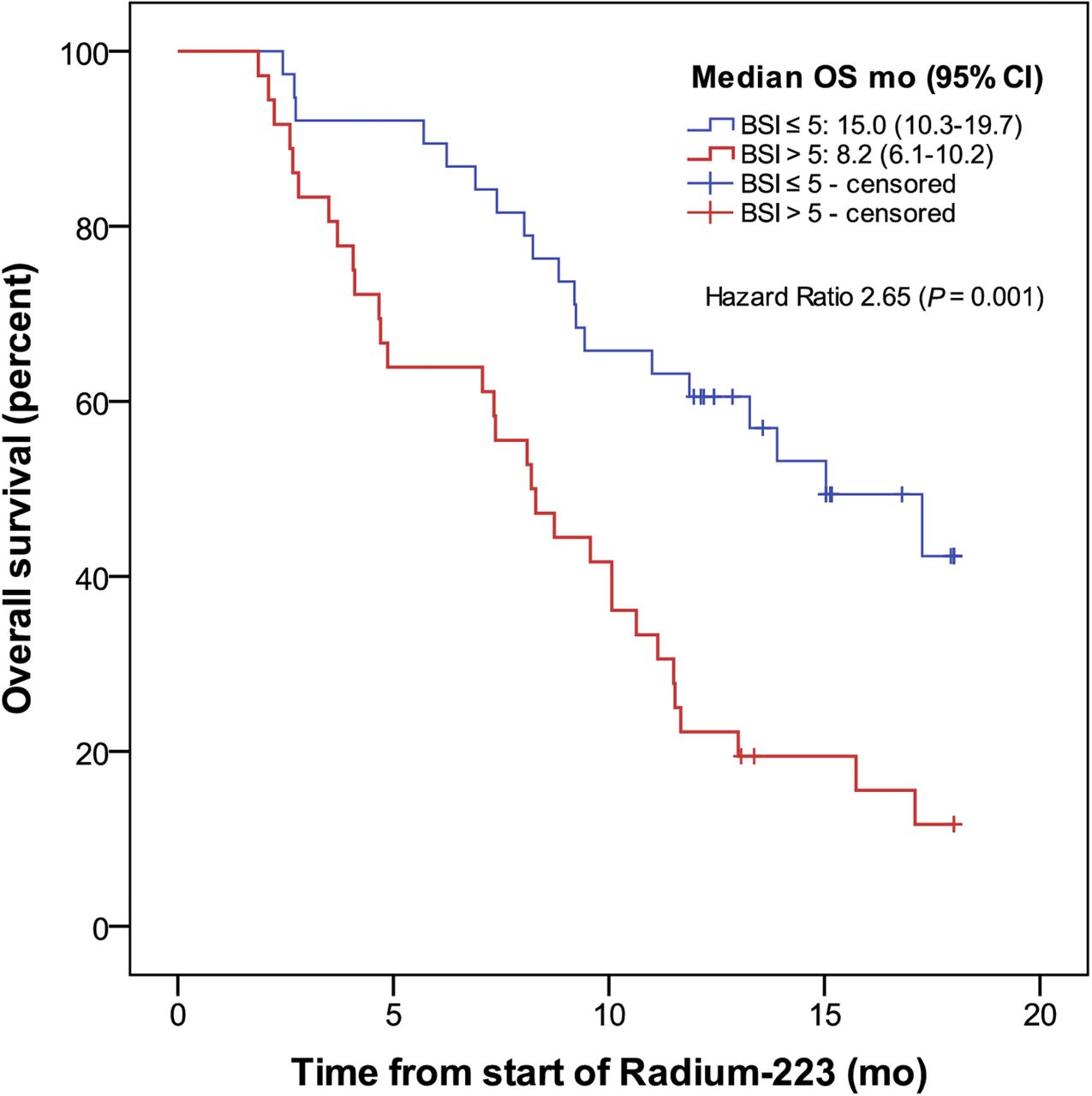
- FIGURE 1.
OS stratified by baseline BSI below or above median (median BSI, 5).
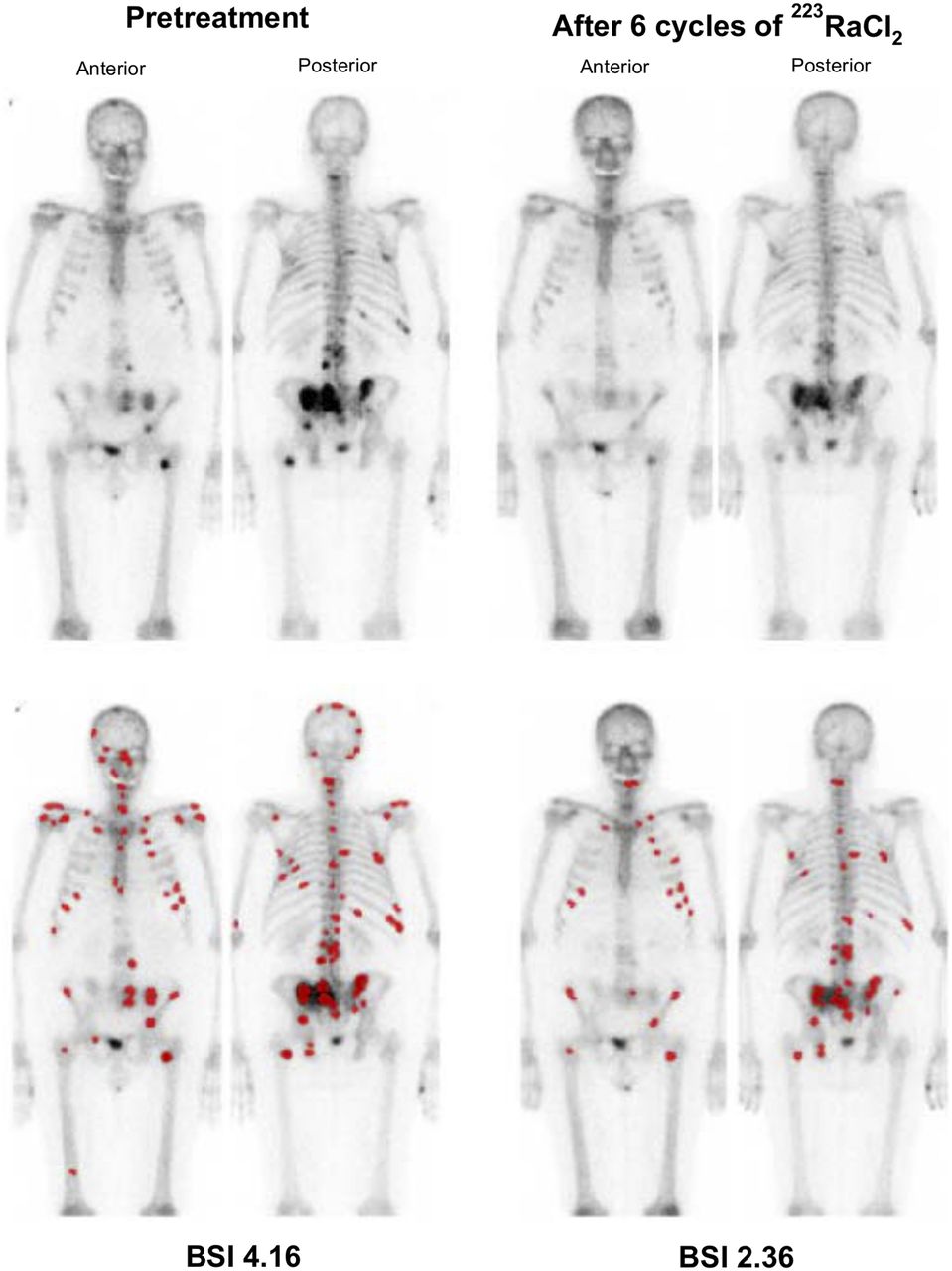
- FIGURE 2.
Example of BSI analysis at baseline and after 6 cycles of 223RaCl2. Lesions detected and interpreted as malignant by software are highlighted in red (bottom row).
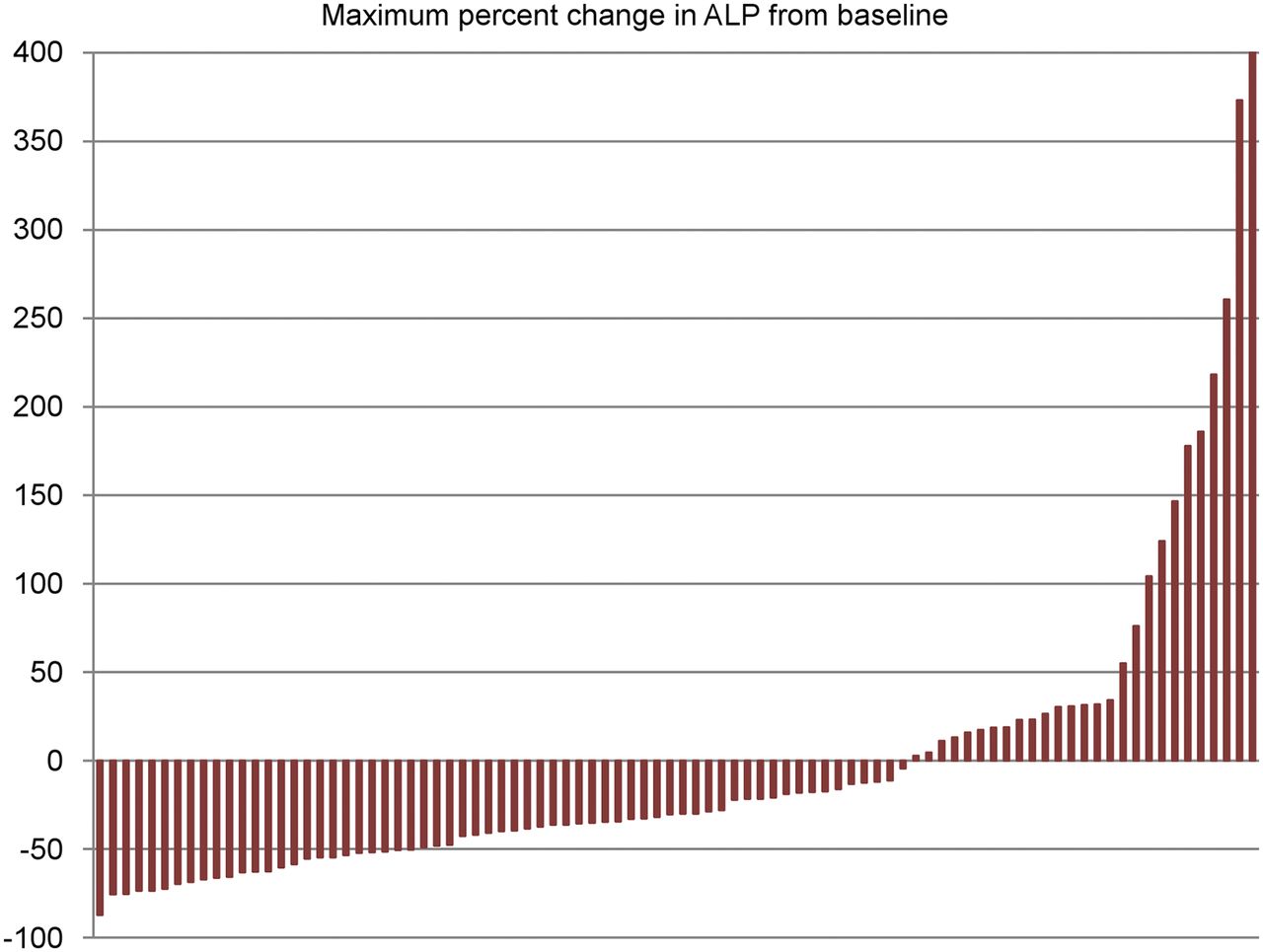
- FIGURE 3.
Maximum percentage of change in ALP during 223RaCl2 therapy (n = 87).
- FIGURE 4.
Maximum percentage of change in LDH during 223RaCl2 therapy (n = 86).
- FIGURE 5.
Maximum percentage of change in PSA during 223RaCl2 therapy (n = 75).




Tables
Characteristic Value* Age (y) 71 (51–89)† Time from diagnosis of mCRPC to 223Ra (mo) 23 (0–87)† ECOG performance status score 0 17 (19.3) 1 68 (77.3) 2 3 (3.4) Extent of skeletal disease <6 metastases 6 (6.8) 6–20 metastases 16 (18.2) >20 metastases 56 (63.6) Superscan‡ 10 (11.4) BSI§ 4.96 (0.1–35.4)† Enlarged lymph nodes at baseline 23 (26.1) Previous use of cabazitaxel 45 (51.1) Previous use of docetaxel 74 (84.1) Previous lines of mCRPC therapy∥ 0 4 (4.5) 1 13 (14.8) 2 21 (23.9) 3 40 (45.5) 4 10 (11.4) Biochemical values Total ALP, U/L 152 (26–1,950)† PSA, μg/L 212 (3–3,441)† LDH, U/L 241 (138–2,330)† Hemoglobin, mmol/L 7.3 (5.1–9.1)† Leukocytes, 109/L 6.6 (3.3–13.0)† Thrombocytes, 109/L 254 (102–558)† ↵* Values are reported as numbers of patients, with percentages in parentheses, unless otherwise indicated.
↵† Reported as median, with range in parentheses.
↵‡ Bone scintigraphy with diffuse skeletal uptake of tracer but without visible renal or background activity.
↵§ n = 87.
↵∥ Recorded mCRPC therapies included docetaxel, cabazitaxel, enzalutamide, and abiraterone.
ECOG = Eastern Cooperative Oncology Group.
- TABLE 2
Univariate and Multivariate Cox Proportional Hazards Regression Model of Predictors of OS
Univariate analysis Multivariate analysis Baseline variable Hazard ratio 95% CI P Hazard ratio 95% CI P BSI (per 1-unit increase) 1.052 1.02–1.09 0.003 1.042 1.003–1.083 0.035 Extent of skeletal disease 6–20 metastases (vs. <6) 1.092 0.36–3.31 0.876 >20 metastases (vs. <6) 1.427 0.56–3.64 0.457 Superscan (vs. <6) 2.35 0.78–7.09 0.130 Lymph node metastases* (yes vs. no) 1.26 0.71–2.25 0.432 Opioid use (yes vs. no) 1.562 0.87–2.82 0.139 PSA (μg/L) (per 10-unit increase) 1.01 1.00–1.02 <0.001 ALP (U/L) (per 10-unit increase) 1.001 1.00–1.01 0.058 LDH (U/L) (per 10-unit increase) 1.021 1.01–1.03 <0.001 1.018 1.01–1.03 <0.001 ↵* Defined as enlarged lymph nodes (>3 cm) visualized on baseline CT of thorax and abdomen.
Toxicity Frequency† Discontinuation of therapy due to toxicity‡ Recovery from toxicity§ Anemia All grades 83 (94) Grade 2 32 (36) 0 0 Grade 3 12 (14) 3 (25) 1 (8) Grade 4 1 (1) 0 0 Grade 5 0 0 Leukopenia All grades 37 (42) Grade 2 20 (23) 2 (10) 16 (80) Grade 3 5 (6) 4 (80) 2 (40) Grade 4 3 (3) 2 (67) 1 (33) Grade 5 1 (1) 1 (100) Thrombocytopenia All grades 40 (46) Grade 2 5 (6) 3 (60) 0 Grade 3 10 (11) 9 (90) 0 Grade 4 6 (7) 6 (100) 0 Grade 5 1 (1) 1 (100) ↵* Most severe grade of toxicity occurring within 90 d of preceding 223RaCl2 administration was recorded.
↵† Reported as numbers of patients, with percentages in parentheses.
↵‡ Early discontinuation of therapy (<6 cycles) registered as being due to hematologic toxicity. Reported as numbers of patients with toxicity, with percentages in parentheses. Percentages were calculated from total frequency of given grade of toxicity.
↵§ Defined as normalization of hematologic value (to grade 0) within 180 d from nadir. Reported as numbers of patients with toxicity, with percentages in parentheses. Percentages were calculated from total frequency of given grade of toxicity.
- TABLE 5
Univariate and Multivariate Logistic Regression Analyses for Predictors of Hematologic Toxicity of Grades 2–5
Univariate analysis Multivariate analysis Baseline variable Odds ratio 95% CI P Odds ratio 95% CI P BSI (per 1-unit increase) 1.147 1.04–1.26 0.005 1.112 1.00–1.23 0.044 Extent of skeletal disease 6–20 metastases (vs. <6) 3.000 0.28–32.21 0.364 >20 metastases (vs. <6) 4.032 0.442–36.78 0.216 Superscan (vs. <6) 20.0 1.42–282.45 0.027 Previous chemotherapy* (yes vs. no) 0.967 0.29–3.15 0.956 PSA (μg/L) (per 10-unit increase) 1.013 1.00–1.023 0.018 Hemoglobin (mmol/L) (per 1-unit decrease) 2.595 1.56–4.31 <0.001 1.888 1.012–3.53 0.043 Leukocytes (109/L) (per 1-unit decrease) 1.299 1.06–1.59 0.013 1.372 1.05–1.79 0.019 Thrombocytes (109/L) (per 1-unit decrease) 1.003 0.99–1.01 0.249 * Previous chemotherapy for mCRPC was defined as docetaxel or cabazitaxel.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Translation of Targeted {alpha}-Therapy: An Evolution or a Revolution?
- Clinical Translation of Targeted {alpha}-Therapy: An Evolution or a Revolution?
- The Prognostic Value of Quantitative Bone SPECT/CT Before 223Ra Treatment in Metastatic Castration-Resistant Prostate Cancer
- Assessing Radiographic Response to 223Ra with an Automated Bone Scan Index in Metastatic Castration-Resistant Prostate Cancer Patients
- Validation of the Semiautomatic Quantification of 18F-Fluoride PET/CT Whole-Body Skeletal Tumor Burden