


Abstract
The aim of this study was to investigate the prognostic value of the quantitative assessment of skeletal tumor burden on bone scintigraphy (Bone Scan Index [BSI]) in patients who have advanced metastatic castration-resistant prostate cancer (mCRPC) and are receiving 223RaCl2. We hypothesized that the BSI can serve as a prognostic biomarker of overall survival (OS) and hematologic toxicity and as a tool for response assessment in patients with mCRPC treated with 223RaCl2. Methods: This study was a retrospective investigation of a Danish cohort of mCRPC patients who received 223RaCl2 therapy between March 2014 and October 2015 and for whom baseline bone scintigraphy was available. Bone scintigraphy studies were reviewed and graded according to the extent of disease. Furthermore, an automated BSI (EXINI BoneBSI) was obtained for baseline scintigraphy studies and follow-up scans after 3 cycles as well as at the end of therapy. Clinical outcomes were OS and occurrence of hematologic toxicity of grades 2–5. Associations between the BSI and clinical outcomes were investigated in multivariate regression models including the visual assessment of bone scintigraphy and other relevant covariates. Results: A total of 88 patients were included. The median number of completed 223RaCl2 cycles was 4, and 27 patients (31%) completed 6 cycles. The BSI was significantly associated with OS in the multivariate analysis; the median OS for patients with a BSI of greater than 5 was 8.2 mo, and the median OS for patients with a BSI of less than or equal to 5 was 15.0 mo (hazard ratio, 2.65 [95% confidence interval, 1.5–4.71]; P = 0.001). Likewise, the baseline BSI was prognostic for the occurrence of hematologic toxicity; patients with a BSI of greater than 5 had an odds ratio of 3.02 (95% confidence interval, 1.2–7.8; P = 0.02) for toxicity. The BSI declined during therapy in 44% of the patients who completed 3 cycles of 223RaCl2 (n = 52) and in 84% of the patients after the end of therapy (n = 32). There was no significant association between a change in the BSI during therapy and OS. Conclusion: The BSI is a promising biomarker for prognostication of OS and hematologic toxicity in late-stage mCRPC patients receiving 223RaCl2. Further prospective studies are needed to evaluate the potential of the BSI for response assessment in 223RaCl2 therapy.
Radionuclide therapy with the α-emitting 223RaCl2 prolongs life and time to symptomatic skeletal events in patients with metastatic castration-resistant prostate cancer (mCRPC) and symptomatic bone metastases (1,2). When administered intravenously, 223RaCl2 accumulates in the bone matrix in proportion to the extent of bone remodeling and is thus ideal for targeting the osteosclerotic metastases from prostate cancer (3).
Although 223RaCl2 was approved for mCRPC in 2013, important clinical issues still need to be investigated. In particular, the role of imaging in prognostication and response assessment needs to be investigated further. In mCRPC patients, 99mTc-diphosphonate bone scintigraphy is a cornerstone of treatment monitoring. Although novel imaging modalities based on PET and MRI are clinically available, these modalities have not been validated for monitoring therapy in mCRPC patients (4–7). Consequently, bone scintigraphy is still the imaging modality recommended by the Prostate Cancer Clinical Trials Working Group (PCWG2) for estimating the skeletal response to therapy in mCRPC patients (8).
The bone scintigraphy response to 223RaCl2 therapy and the correlation with clinical outcome have not been well described in the literature. A multicenter study reported scintigraphically stable disease in most patients, but an association with OS or other clinical endpoints was not investigated (9). A typical pattern of the response to 223RaCl2 was described in a small study of 10 patients: a reduction in the size and intensity of already existing lesions was described but was accompanied by the appearance of new foci (10). This “mixed response” would be characterized as progression by the acknowledged response criteria proposed by the PCWG2, although most patients experienced a decrease in alkaline phosphatase (ALP) levels, suggesting that 223RaCl2 was effective despite the imaging response. This discrepancy highlights the need to assess the response in terms of total skeletal tumor burden instead of focusing on the number of lesions.
Quantification of skeletal tumor burden on bone scintigraphy is possible using the software EXINI BoneBSI (EXINI Diagnostics), which calculates the percentage of total skeletal mass affected by metastases as the Bone Scan Index (BSI). The BSI has been found to be prognostic of overall survival (OS) in mCRPC patients in various settings (11,12), including 223RaCl2 therapy, in which the baseline BSI was associated with OS. However, this finding was not validated in a multivariate analysis, and the BSI was not compared with a conventional evaluation of the extent of skeletal disease (13). Quantification of skeletal tumor burden from 18F-fluoride PET/CT has also been demonstrated to be a significant independent predictor of bone marrow failure after 223RaCl2 therapy (14). Likewise, the BSI may be a valuable aid for identifying mCRPC patients with a high risk of hematologic toxicity before the initiation of therapy.
The aims of this study were to investigate the prognostic value of the BSI in patients receiving 223RaCl2 and to compare the BSI results with visual assessments of bone scintigraphy. We hypothesized that the BSI can serve as a prognostic biomarker of OS and hematologic toxicity and as a tool for response assessment in patients with mCRPC treated with 223RaCl2.
MATERIALS AND METHODS
Study Design
The primary objective of this study was to investigate whether the baseline BSI was independently associated with OS and the development of hematologic toxicity during 223RaCl2 therapy through a comparison to visual assessments of bone scintigraphy. The secondary objective was to evaluate the BSI for response assessment in 223RaCl2 therapy.
This study was a retrospective investigation of a Danish cohort of mCRPC patients who received 223RaCl2 therapy between March 2014 and October 2015 at Rigshospitalet, University of Copenhagen, Copenhagen, Denmark. Patients who had bone scintigraphy performed less than or equal to 8 wk before the first 223RaCl2 cycle available for analysis were included in the study. All patients had confirmed mCRPC with symptomatic bone metastases and no visceral metastases or lymph nodes greater than or equal to 3 cm. The clinical criteria for 223RaCl2 therapy were an Eastern Cooperative Oncology Group performance status of less than or equal to 2, a leukocyte count of greater than or equal to 3.0 × 109/L, a thrombocyte count of greater than or equal to 100 × 109/L, and a hemoglobin level of greater than or equal to 6.0 mmol/L (9.7 g/dL). Patients with a baseline hemoglobin level of less than 6.0 mmol/L received a blood transfusion before 223RaCl2. All patients had castration levels of testosterone. No concomitant treatment with chemotherapy, abiraterone, or enzalutamide was administered. Other medications, including denosumab or bisphosphonates, were prescribed at the clinician’s discretion.
The study was approved by the Danish Health Authority (reference number 3-3013-1320/1), and a waiver of informed consent was granted for the retrospective analysis.
223RaCl2 Therapy
Patients received 223RaCl2 at 50 kBq/kg (current recommendation, 55 kBq/kg) intravenously every 4 wk for up to 6 cycles. Dose delays were applied in the presence of hematologic toxicity, gastrointestinal side effects, or other concurrent disease. A dose delay of more than 4 wk led to a discontinuation of therapy. Furthermore, treatment was discontinued early in the case of disease progression, unacceptable adverse events, or declining performance status or by request from the patient.
Imaging and Biochemistry
Routine baseline imaging consisted of planar whole-body bone scintigraphy and CT of the thorax and abdomen. Bone scintigraphy was repeated after 3 cycles and after the end of therapy (EOT). CT or MRI was performed in the case of clinical symptoms of progression. Imaging was performed at local hospitals, and bone scintigraphy studies were subsequently reviewed by 2 experienced nuclear medicine physicians evaluating the extent of disease at baseline as proposed by Soloway et al. (15). Bone scintigraphy studies during therapy and after the EOT were interpreted according to imaging criteria for progression as stated by the PCWG2 (8).
All bone scintigraphy studies available in the Digital Imaging and Communications in Medicine format were additionally analyzed with the commercially available EXINI BoneBSI, version 2. The methodology for calculation of the BSI was previously described (16). The BSI results were assessed visually to ensure correct identification of malignant lesions according to guidelines from the manufacturer. Scintigraphy studies with diffuse metastatic involvement of the skeleton (superscan) were included if the software correctly identified the extent of bone involvement. A change in the BSI was recorded in patients for whom bone scintigraphy was available after 3 cycles of 223RaCl2 or after EOT.
Baseline laboratory tests consisted of prostate-specific antigen (PSA), total ALP, lactate dehydrogenase (LDH), and hemoglobin levels and leukocyte and thrombocyte counts. The hematologic parameters (ALP and LDH) were evaluated before each administration of 223RaCl2, and the PSA level was evaluated after the third and sixth cycles.
Outcomes
The primary clinical outcome was OS, defined as the time from the first 223RaCl2 cycle to death from any cause. The secondary outcome was the occurrence of hematologic toxicity, defined as leukopenia or thrombocytopenia of grades 2–5 (according to Common Terminology Criteria for Adverse Events, version 4.03 (17)) occurring within 90 d of the preceding 223RaCl2 administration. Because grade 1 or 2 anemia is common in mCRPC patients (because of hypogonadism, previous chemotherapy, and a chronic disease state), only cases of grade 3–5 anemia were included in the logistic regression model if they coincided with leukopenia or thrombocytopenia of grade 2 or higher. This step was done in an attempt to distinguish between toxicity from therapy and bone marrow suppression due to advanced disease. Recovery from hematologic toxicity was recorded as normalization of the given parameter within 180 d from the nadir.
The follow-up period from the first administration of 223RaCl2 was up to 18 mo or the date of death.
Statistical Analysis
The clinical characteristics of the patients were summarized using descriptive statistics. The prognostic value of the BSI was compared with clinical covariates associated with OS and hematologic toxicity in published studies. Correlations among BSI, the extent of disease, and clinical covariates were estimated using the Kendall τ. Associations between independent variables and OS were examined using univariate Cox regression analyses followed by multivariate Cox regression with stepwise backward elimination. The assumption of proportional hazards was examined using a log-minus-log plot for categoric variables and Schoenfeld residuals for continuous variables. The potential effects of influential observations were examined using deviance residuals, and nonlinearity was examined by plotting Martingale residuals. A Kaplan–Meier plot and the log-rank test were used to evaluate differences in median OS according to the baseline BSI.
Associations between clinical variables and hematologic toxicity were determined using univariate binary logistic regression analysis followed by a multivariate binary logistic regression model with stepwise backward elimination; variables with a P value of less than 0.2 were retained in the model. A test for linearity was performed with the Box–Tidwell transformation test.
Because the study was considered exploratory, no corrections for multiple comparisons were performed. Cases with missing data were excluded listwise.
All statistical analyses were performed using IBM SPSS Statistics, version 22 (IBM Corp.).
RESULTS
In the relevant time period, 91 consecutive patients received 223RaCl2 therapy at Rigshospitalet, University of Copenhagen. Baseline bone scintigraphy was available for 88 patients, who were included in the study (Table 1). The BSI result for 1 patient with a superscan was excluded because the diffuse metastatic involvement could not be automatically detected, resulting in a very low BSI. Patients received a total of 349 doses of 223RaCl2. The median number of cycles per patient was 4, and all 6 cycles were completed in 27 patients (31%). Reasons for early discontinuation of therapy were progression (n = 25 [28%]), hematologic toxicity (n = 21 [24%]), declining performance status (n = 10 [11%]), gastrointestinal side effects (n = 2 [2%]), and request from the patient (n = 2 [2%]). Furthermore, 1 patient discontinued therapy because of the sudden development of blindness during 223RaCl2; this development was subsequently interpreted as cancer-associated retinopathy and not related to therapy (18). A significant correlation between the baseline BSI and ALP was found (Kendall τ, 0.566; P < 0.001), whereas the BSI was only moderately correlated with visual assessment of the extent of disease (Kendall τ, 0.443; P < 0.001).
Baseline Characteristics of 88 Patients
Baseline Prognostic Factors for OS
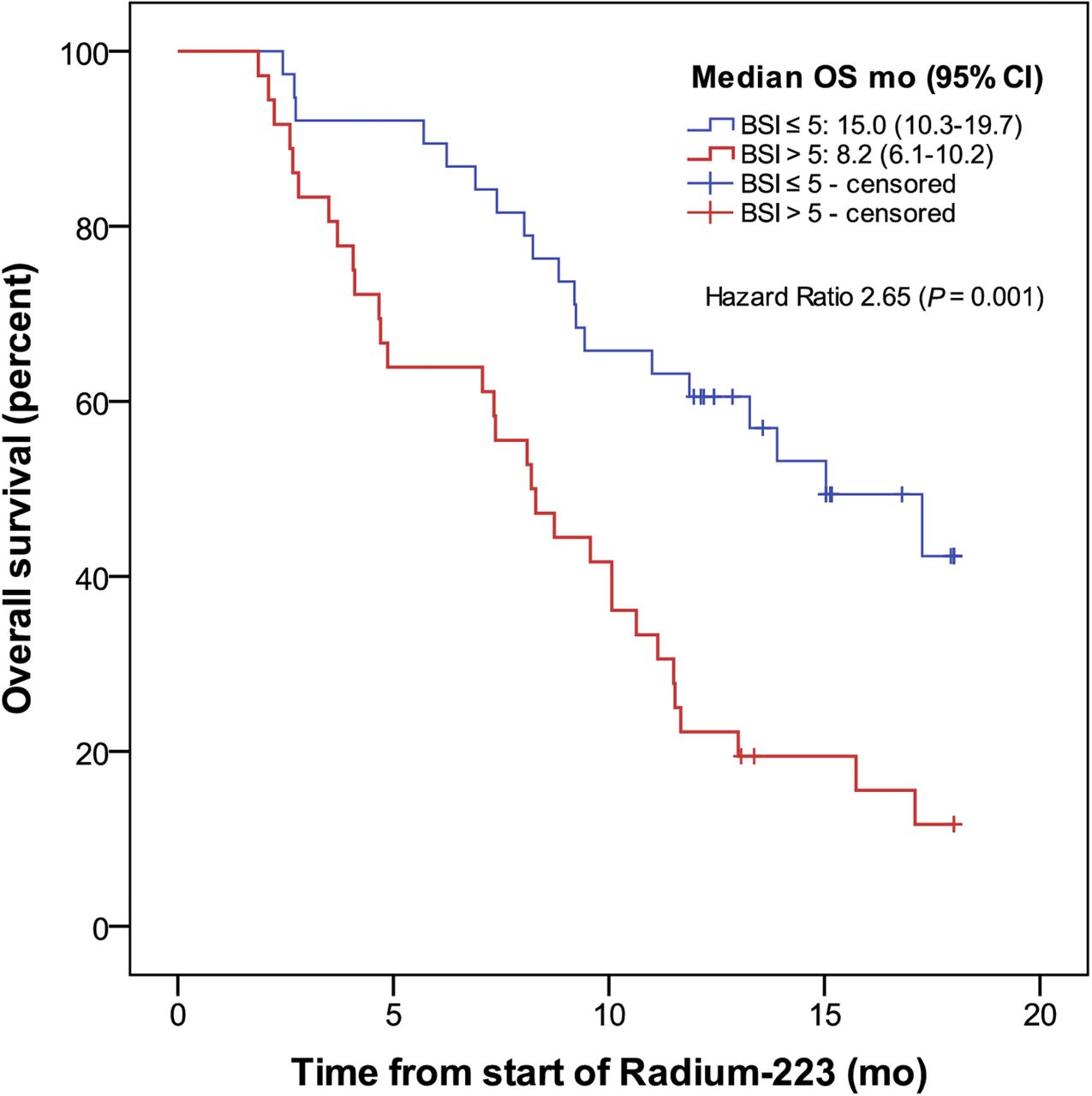
The median OS for the cohort was 10.1 mo (95% confidence interval [CI], 7.9–12.2), and 59 deaths were reported. The results of Cox regression analyses regarding associations between baseline variables and OS are shown in Table 2. Only the BSI and LDH were found to be significant predictors of OS in the multivariate analysis. Stratifying patients according to the median baseline BSI (>5 vs. ≤5) revealed significantly shorter OS for patients with a high BSI (Fig. 1).
Univariate and Multivariate Cox Proportional Hazards Regression Model of Predictors of OS

OS stratified by baseline BSI below or above median (median BSI, 5).
Changes in Bone Scintigraphy, BSI, and Blood-Based Biomarkers
Bone scintigraphy studies were available after 3 cycles of therapy in 52 patients and after the EOT in 32 patients. Because of early discontinuation of therapy, the EOT imaging was performed after 5 cycles of 223RaCl2 in 4 patients and after 4 cycles in 1 patient. The response to therapy (BSI and number of lesions) is shown in Table 3, and an example of bone scintigraphy and the BSI during 223RaCl2 therapy is shown in Figure 2. The correlation between the response indicated by the BSI and PCWG2 criteria was moderate (Kendall τ, 0.49; P = 0.001) from the baseline to the EOT, whereas there was no significant correlation for the imaging results from the baseline to the third cycle of 223RaCl2. There was no association between OS and changes in the BSI measured as absolute difference or percentage of change and categorized as increased (change in BSI, >0) or stable/decreased (change in BSI, ≤0). The bone scintigraphy response evaluated according to PCWG2 from the baseline to the EOT was significantly associated with OS. The median OS for patients who progressed according to PCWG2 during therapy (n = 20 [63%]) was 11.9 mo (95% CI, 8.0–15.7), whereas the median OS was not reached for patients with stable disease (n = 12 [38%]; hazard ratio, 5.82; 95% CI, 1.31–25.9; P = 0.02).
Imaging Response After 223RaCl2 Therapy
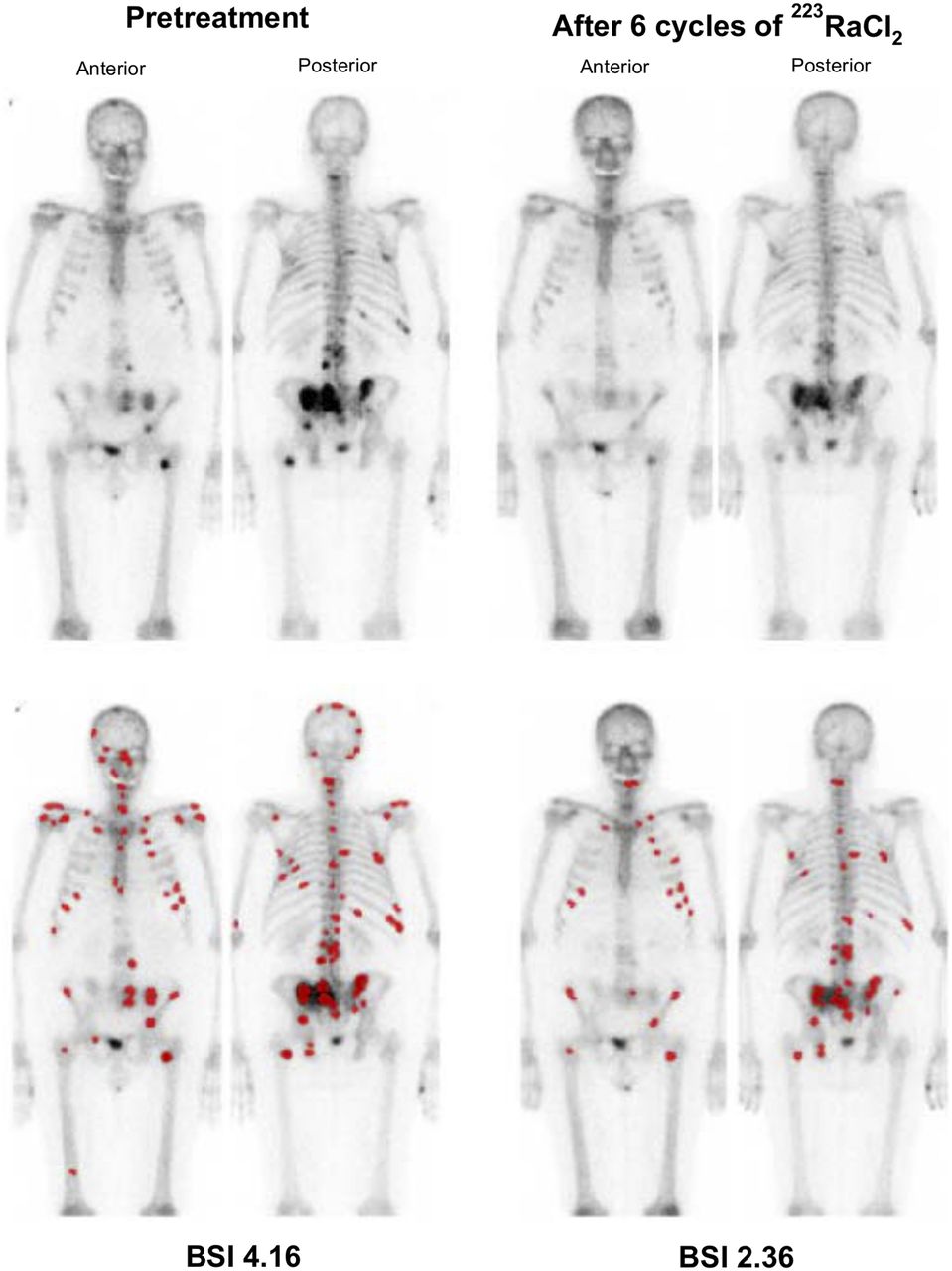
Example of BSI analysis at baseline and after 6 cycles of 223RaCl2. Lesions detected and interpreted as malignant by software are highlighted in red (bottom row).
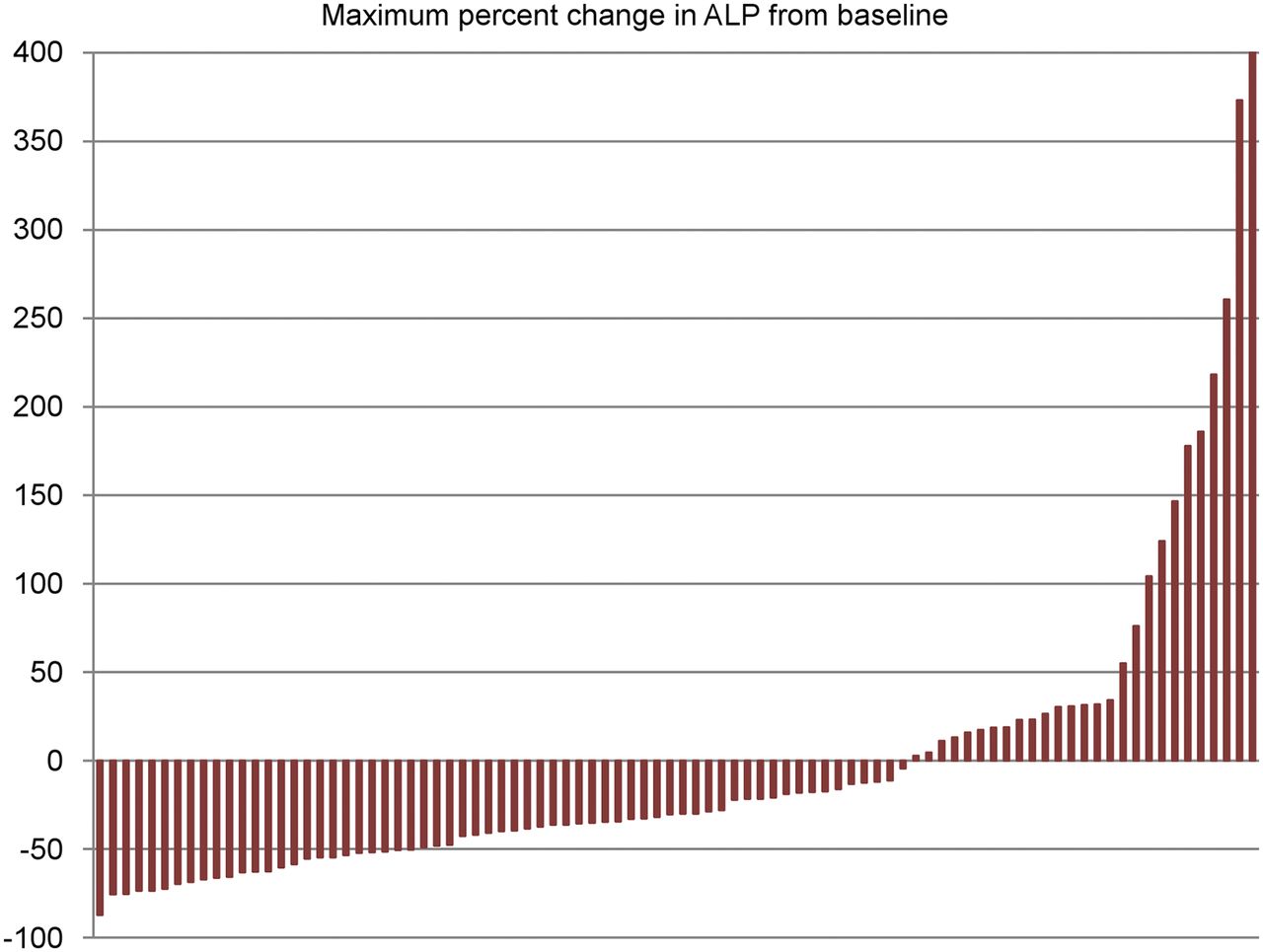
Changes in ALP, LDH, and PSA are shown in Figures 3, 4, and 5, respectively. Of 75 patients for whom data were available, only 12 patients (16%) experienced a decrease in the PSA level during therapy. There was no significant association between OS and changes in ALP, LDH, or PSA.

Maximum percentage of change in ALP during 223RaCl2 therapy (n = 87).

Maximum percentage of change in LDH during 223RaCl2 therapy (n = 86).

Maximum percentage of change in PSA during 223RaCl2 therapy (n = 75).
Baseline Prognostic Factors for Hematologic Toxicity
Before the first cycle of 223RaCl2, 73 patients (83%) had hemoglobin levels under the lower limit of normal (<8.2 mmol/L; ≈13.2 g/dL), 1 patient (1%) had leukocyte counts under the lower limit of normal (<3.5 × 109/L), and 7 patients (8%) had thrombocyte counts under the lower limit of normal (<150 × 109/L). The frequency and severity of hematologic toxicity during and after 223RaCl2 therapy are shown in Table 4. Two cases of grade 5 toxicity were reported: 1 patient died because of leukopenic infection (died 13 d after preceding 223RaCl2 therapy), and 1 patient died because of thrombocytopenia and intracranial hemorrhage (died 80 d after preceding 223RaCl2 therapy). Both leukopenia and thrombocytopenia frequently resulted in the early discontinuation of therapy. Despite the discontinuation of therapy, no patient who developed thrombocytopenia of greater than or equal to grade 2 recovered from toxicity.
Frequency and Severity of Hematologic Toxicity*
The baseline BSI, hemoglobin level, and leukocyte count were associated with hematologic toxicity in a multivariate logistic regression model (Table 5). Stratifying patients according to the median baseline BSI (>5 vs. ≤5) resulted in an odds ratio of 3.02 (95% CI, 1.2–7.8; P = 0.02) for toxicity of grades 2–5 in patients with a baseline BSI of greater than 5.
Univariate and Multivariate Logistic Regression Analyses for Predictors of Hematologic Toxicity of Grades 2–5
DISCUSSION
Quantitative approaches and computer-aided diagnostics are gaining popularity in many fields of nuclear medicine and radiology. Obvious potential advantages include lower interobserver variation, higher reproducibility and, possibly, better accuracy. The automated BSI for the assessment of skeletal tumor burden in patients with prostate cancer is an example of such a diagnostic tool. The BSI has been proven to be valuable for prognostication, prediction, and response assessment in prostate cancer patients (11,19–21).
In this nationwide study, we found that the baseline BSI was a prognostic biomarker of OS and the development of hematologic toxicity in mCRPC patients receiving 223RaCl2 therapy. The extent of disease graded by counting lesions did not show a significant independent association with clinical outcome. This finding is in accordance with the results of quantification of skeletal tumor burden by 18F-fluoride PET, which performed better than visual grading for the prognostication of OS and bone marrow failure (14,22). Likewise, a small study of 14 patients with a high BSI reported short median survival after 223RaCl2 therapy (23). However, that study did not include a direct comparison to patients with a low BSI or a multivariate analysis to investigate other prognostic factors.
A considerable limitation of the present study was the advanced disease stage of the study cohort (high skeletal tumor burden and long duration of mCRPC), which may limit the general applicability of our results. The advanced disease stage of the patients was a result of the current Danish Health Authority guidelines for mCRPC therapy. These guidelines recommend docetaxel, enzalutamide, or abiraterone as the first line of therapy, but the line of therapy for which 223RaCl2 should be given is not specified. Consequently, 223RaCl2 is often the fourth or fifth line of therapy for mCRPC patients in Denmark.
The advanced extent of disease of the study population could have been the reason for the high incidence of hematologic toxicity relative to that in the existing literature (14,24–26). In particular, thrombocytopenia was frequent and was associated with a complete lack of recovery within 6 mo despite the discontinuation of 223RaCl2. In contrast to published studies, we did not find prior use of chemotherapy to be a predictor of hematologic toxicity—perhaps because most of our patients had received chemotherapy, leaving a very small group of patients who had not received chemotherapy for comparison.
These data further underline the need for alternative methods of risk stratification for patients with late-stage disease. In these patients, careful selection of therapy is particularly important, as hematologic side effects may have detrimental consequences. On the basis of our results, the magnitude of the BSI as well as baseline hematologic parameters should be considered before patients are deemed eligible for 223RaCl2 therapy.
Another important aspect of optimizing 223RaCl2 therapy is improvement of methods for response assessment. Bone scintigraphy is widely used for this purpose but has the well-known limitation of the flare phenomenon, which can lead to an increased number of visible lesions after the initiation of therapy despite a clinical response. Therefore, the response cannot be evaluated at the initial scintigraphy after a new therapy is commenced but must be confirmed on a later scan. At present, the fact that 223RaCl2 is approved for only 6 cycles of therapy (with a duration of approximately 24 wk) emphasizes the need for an early response marker. We hypothesized that the BSI could serve as such an early response biomarker, as total skeletal disease conceivably could decrease early during therapy, although the number of lesions might increase. Approximately 45% of our patients who completed at least 3 cycles of 223RaCl2 experienced a decrease in the BSI, but we did not find any significant association between a change in the BSI and OS. A plausible explanation is that the bone flare phenomenon obstructs the interpretation of early BSI changes during therapy, as is the case for visual interpretation. Thus, the BSI does not seem to have the potential to serve as an appropriate measure of an early response in 223RaCl2 therapy.
After the EOT, there was some discrepancy between the response indicated by the BSI and the conventional response assessment (lesion counting). We found a significant association between the bone scintigraphy response (according to PCWG2) and OS, although this finding was based on a small number of observations, whereas no association between the BSI response and OS was detected. These results conflict with recent reports of the BSI as a response marker in mCRPC settings (20,21). The discrepancy could be a result of the extensive skeletal involvement of our cohort; in such a setting, BSI measurement might not perform adequately in detecting changes. The analytic validation study of EXINI BoneBSI included a phantom study of a BSI of up to 13, but the performance of the software in patients with a higher BSI has not been reported (16).
CONCLUSION
Baseline skeletal tumor burden quantified as the automated BSI is a promising prognostic biomarker of OS in patients who have late-stage mCRPC and are receiving 223RaCl2 therapy. Furthermore, a high BSI is a significant risk factor for the development of hematologic toxicity, which occurred frequently in our population. Whether the results are applicable in patients with less extensive disease needs to be investigated further. Additionally, studies are needed to evaluate the potential of the BSI for response assessment in patients with advanced disease in comparison to the validated criteria from PCWG2.
DISCLOSURE
Peter Meidahl Petersen is an Advisory Board Member at Bayer Healthcare. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 1, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 5, 2017.
- Accepted for publication August 10, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Translation of Targeted {alpha}-Therapy: An Evolution or a Revolution?
- Clinical Translation of Targeted {alpha}-Therapy: An Evolution or a Revolution?
- The Prognostic Value of Quantitative Bone SPECT/CT Before 223Ra Treatment in Metastatic Castration-Resistant Prostate Cancer
- Assessing Radiographic Response to 223Ra with an Automated Bone Scan Index in Metastatic Castration-Resistant Prostate Cancer Patients
- Validation of the Semiautomatic Quantification of 18F-Fluoride PET/CT Whole-Body Skeletal Tumor Burden