


Abstract
The purpose of this study was to evaluate 18F-FDG PET/CT scanning as an early predictor of response to immune checkpoint inhibitors (ICIs) in patients with advanced melanoma. Methods: Twenty patients with advanced melanoma receiving ICI prospectively underwent 18F-FDG PET/CT at 3 scan intervals: before treatment initiation (SCAN-1), at days 21–28 (SCAN-2), and at 4 mo (SCAN-3). This study was approved by the institutional review board, and informed consent was received from all patients who were enrolled between April 2012 and December 2013. Tumor response at each posttreatment time point was assessed according to RECIST 1.1, immune-related response criteria, PERCIST (PERCIST 1.0), and European Organization for Research and Treatment of Cancer (EORTC) criteria. Performance characteristics of each metric to predict best overall response (BOR) at ≥ 4 mo were assessed. Results: Twenty evaluable patients were treated with ipilimumab (n = 16), BMS-936559 (n = 3), or nivolumab (n = 1). BOR at ≥ 4 mo included complete response (n = 2), partial response (n = 2), stable disease (n = 1), and progressive disease (n = 15). Response evaluations at SCAN-2 using RECIST 1.1, immune-related response criteria, PERCIST, and EORTC criteria demonstrated accuracies of 75%, 70%, 70%, and 65%, respectively, to predict BOR at ≥ 4 mo. Interestingly, the optimal PERCIST and EORTC threshold values at SCAN-2 to predict BOR were >15.5% and >14.7%, respectively. By combining anatomic and functional imaging data collected at SCAN-2, we developed criteria to predict eventual response to ICI with 100% sensitivity, 93% specificity, and 95% accuracy. Conclusion: Combining functional and anatomic imaging parameters from 18F-FDG PET/CT scans performed early in ICI appears predictive for eventual response in patients with advanced melanoma. These findings require validation in larger cohorts.
Immune checkpoint inhibitors (ICIs) blocking CTLA-4 (e.g., ipilimumab), PD-1 (e.g., nivolumab, pembrolizumab), or PD-L1 (e.g., atezolizumab, avelumab, durvalumab) have demonstrated objective tumor regressions in patients with advanced melanoma and other cancer types. Some drugs and drug combinations (e.g., nivolumab plus ipilimumab) can prolong survival in patients with melanoma (1,2). However, these drugs have mechanisms of action that differ from targeted agents and traditional cytotoxic chemotherapies, making assessment of therapeutic benefit (or lack thereof) in a given patient challenging, especially soon after initiation of therapy. In some cases, tumors assessed using standard CT imaging appear to enlarge before later regressing, likely due to the infiltration and proliferation of lymphocytes and other immune cells. Other tumors remain stable in size for a prolonged time, even after therapy has been stopped (3–6). Indeed, a variety of radiologic responses to ICIs has been described, some of which are linked to therapeutic benefit (7,8). Because traditional RECIST or World Health Organization criteria may be insufficient to characterize outcomes after administration of immune-based antineoplastic drugs, immune-related response criteria (irRC (9)) are increasingly being incorporated into clinical trials of cancer immunotherapies (10,11).
Several studies have investigated the utility of 18F-FDG PET/CT imaging in early detection of response to targeted and chemotherapeutic agents in a variety of tumor types (12–14). Results from these studies and others suggest that functional imaging information obtained from 18F-FDG PET/CT scans may complement data from anatomic imaging studies such as conventional spiral CT scanning and MRI.
Two 18F-FDG PET–based tumor response evaluation criteria commonly used in studies of patients with solid tumors are PERCIST 1.0 and European Organization for Research and Treatment of Cancer (EORTC) 1999 criteria (15,16). Disease response to therapy has been evaluated in multiple studies encompassing a variety of tumor types using these metrics (17–19).
To investigate the utility of 18F-FDG PET/CT as a tool to detect early evidence of response in patients with advanced melanoma receiving immune checkpoint blocking agents, we prospectively performed serial 18F-FDG PET/CT imaging in patients with advanced melanoma undergoing ICI therapy, conducted several analyses to characterize changes in tumor burden and functional parameters, and used these data to develop criteria to predict eventual clinical response to therapy.
MATERIALS AND METHODS
Study Design
This study was approved by the Johns Hopkins University and University of Wisconsin–Madison Institutional Review Boards in accordance with an assurance filed with and approved by the Department of Health and Human Services Subjects (ClinicalTrials.gov no. NCT01666353). Per institutional review board requirements, study data were anonymized during data collection and analysis. Twenty adult patients who were scheduled to initiate ICI therapy as their first or later systemic treatment for metastatic or unresectable melanoma at the Johns Hopkins Sidney Kimmel Comprehensive Cancer Center provided written informed consent to participate in this prospective study between April 2012 and December 2013. Subjects were required to have at least 1 lesion, >10 mm, that could be accurately measured in at least 1 dimension with spiral CT scanning. Patients were treated with ipilimumab at 3 mg/kg intravenously every 3 wk for a maximum of 4 doses (anti–CTLA-4; n = 16); BMS-936559 at 0.1–1 mg/kg intravenously every 2 wk until complete response, disease progression, or dose-limiting toxicity (anti–PD-L1; n = 3; ClinicalTrials.gov no. NCT00729664 (20)); or nivolumab at 3 mg/kg every 2 wk (anti–PD-1; n = 1; ClinicalTrials.gov no. NCT01621490 (21)). 18F-FDG PET/CT imaging was performed within 4 wk before therapy (SCAN-1) was initiated, again between days 21 and 28 on therapy (SCAN-2), and at approximately 4 mo after treatment initiation (SCAN-3). Patients were observed until death or initiation of subsequent therapy for disease progression. Of note, because of the investigational nature of SCAN-2, data from that scan were not used to guide patient management decisions. Evaluable patients were required to have received at least 2 doses of ICI therapy and have undergone SCAN-1, SCAN-2, and at least 1 additional evaluation (radiographic or clinical) thereafter. Because of the poor performance of PET/CT imaging to detect brain metastases, intracranial lesions were not included in disease assessments.
Imaging
18F-FDG PET/CT images were acquired on a Discovery DRX PET/CT scanner (GE Healthcare). 18F-FDG PET/CT scanning was performed according to the Uniform Protocols for Imaging in Clinical Trials Protocol for 18F-FDG PET/CT Imaging in Oncology Clinical Trials (22). Low-dose CT images were acquired for tissue attenuation correction and anatomic correlation. Patients were injected with 370 ± 37 MBq (10 ± 1 mCi) of 18F-FDG and scanned supine, starting from the midthigh and through the vertex of skull, followed by a separate scan from the upper thigh through bilateral feet. Patients fasted for 4–6 h immediately before injection of 18F-FDG.
Response Evaluation
18F-FDG PET/CT images were reviewed and analyzed using MIRADA XD3 software (MIRADA Medical) by 2 nuclear medicine specialists with convened consensus review of PET and CT response evaluation. CT-based responses, assessed by study investigators, were characterized according to RECIST 1.1 (23) and irRC (9). 18F-FDG PET–based responses were evaluated using PERCIST 1.0 (24,25) and EORTC 1999 criteria (16). Response criteria used in this study are summarized in Table 1. Because EORTC 1999 criteria do not include a prespecified number of target lesions, we considered all 18F-FDG–avid lesions at SCAN-1 as target lesions. The sum of the SUVmax of all 18F-FDG–avid metastatic lesions was measured for the EORTC 1999 criteria. An 18F-FDG–avid lesion was defined as focal, abnormally increased 18F-FDG uptake versus background with a corresponding anatomic lesion seen on CT scan, suggestive of metastasis.
Summary of Treatment Response Criteria
CT-based antitumor responses based on changes observed from SCAN-1 to SCAN-2 and SCAN-1 to SCAN-3 were classified as complete response, partial response, stable disease, or progressive disease (PD). 18F-FDG PET–based responses were classified as complete metabolic response, partial metabolic response, stable metabolic disease, or progressive metabolic disease. Percentage change in lesion dimensions (CT) or 18F-FDG avidity (PET) from SCAN-1 to SCAN-2 were calculated using the following formula: [(SCAN-2 – SCAN-1)/SCAN-1) × 100]. The same formula was adapted for SCAN-1 to SCAN-3 calculations subtracting the SCAN-1 result from the SCAN-3 result. During and after the study period, patients were followed per standard-of-care imaging and clinical follow-up to assess best overall response (BOR) to ICI therapy. The duration of observation for each patient is included in Table 2. Radiographic changes observed at SCAN-2 were analyzed for their capacity to predict eventual clinical benefit, which we defined as CR or PR at 4 mo or stable disease lasting at least 6 mo. Confirmatory scans for PR and CR seen at SCAN-3 were not required.
Response Assessments, Excluding Brain Lesions, in 20 Patients with Metastatic Melanoma Receiving ICI Therapies
Outcomes Analysis
Intercriteria agreements at SCAN-2 and SCAN-3 were assessed using κ-coefficients (26). The positive and negative predictive values of outcomes at SCAN-2 for clinical benefit were assessed for all 4 criteria. Receiver-operating-characteristic (ROC) analysis was used to assess the predictive value of continuous measurements and to find the optimal cutoff of measurements to predict clinical benefit. The Pearson correlation coefficient (r) was used for correlation analysis. Finally, a combined functional–anatomic approach was developed and evaluated to enhance the predictive value of the 18F-FDG PET and CT measurements at SCAN-2 for clinical benefit. Statistical analyses were performed using MedCalc software version 10.1 (version 10.1; MedCalc Software).
RESULTS
Patient Characteristics
Twenty subjects were enrolled in the trial. Their mean age was 59.2 y (range, 42–72 y). Seven were women. Eleven patients had previously received systemic therapy for advanced melanoma, including nilotinib, high-dose interleukin-2, and temozolomide. One patient who received ipilimumab on the present trial had previously received nivolumab. All 20 enrolled subjects with metastatic melanoma were evaluable for response to therapy with ICIs. Sixteen patients received ipilimumab (anti–CTLA-4) as a standard-of-care therapy in the first- or later line setting. Three patients received BMS-936559 (anti–PD-L1) on a clinical trial in the second-line setting. One patient received nivolumab (anti–PD-1) on a clinical trial in the first-line setting.
Treatment Response
Tumor responses were measured by PET/CT according to 4 different criteria systems, after 3–4 wk of treatment (SCAN-2) and at about 4 mo (SCAN-3) (Table 2). The best overall responses for each patient, including information from standard-of-care radiographic imaging performed in addition to SCAN-2 and SCAN-3, are included in Table 2.
Five subjects classified as having derived clinical benefit from ICI therapy included 2 patients with CR at 4 mo, 2 patients with PR at 4 mo, and 1 patient with stable disease lasting 9 mo. The 5 subjects had been treated with ipilimumab. The remaining 15 patients experienced stable disease lasting less than 6 mo, or PD. No patient with an early assessment categorized as PD by RECIST 1.1 later experienced an objective response to therapy.
Of note, baseline scans for patient 11 demonstrated a 1.1-cm retroperitoneal lymph node, proven by fine-needle aspirate to be metastatic melanoma. Although the patient met study entry criteria (at least 1 lesion, >10 mm, that could be accurately measured in at least 1 dimension with spiral CT scanning), the tumor did not qualify as measurable by RECIST 1.1 (≥1.5-cm short diameter). However, because the lesion was proven to be tumor by biopsy, and because we were able to measure it at baseline and after administration of therapy, we included this patient in our study.
Comparisons of Response Evaluations at SCAN-2 and SCAN-3
Comparisons of tumor response measurement criteria at SCAN-2, performed 21–28 d after ICI was initiated, demonstrated excellent degrees of intercriteria agreement. κ-coefficient values were calculated within the same imaging modality: RECIST 1.1 versus irRC (CT-based), 0.9; PERCIST versus EORTC (PET-based), 0.886. Comparisons between different modalities demonstrated lesser degrees of agreement, with κ-values between 0.48 and 0.7. At SCAN-3, performed 4 mo after ICI was initiated, all pairs of response criteria showed good to excellent correlation (κ-value range, 0.66–0.88), except irRC versus PERCIST (κ = 0.53) (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
Findings on Early PET/CT Associated with Eventual Clinical Outcomes
At SCAN-2, of the 4 metrics assessed, RECIST 1.1 demonstrated the highest predictive value for BOR at ≥ 4 mo (accuracy, 75%; Table 3). ROC analysis revealed that percentage change from SCAN-1 to SCAN-2 using RECIST 1.1, irRC, PERCIST, and EORTC criteria were predictive for BOR at ≥ 4 mo as follows: area under the curve, 0.853, 0.827, 0.680, and 0.600, respectively (Supplemental Table 2).
Performance of 4 Radiologic Evaluation Criteria Applied to Early (3–4 Week) PET/CT Scans in Predicting Best Overall Response (RECIST 1.1) to ICI Therapy at ≥ 4 Months
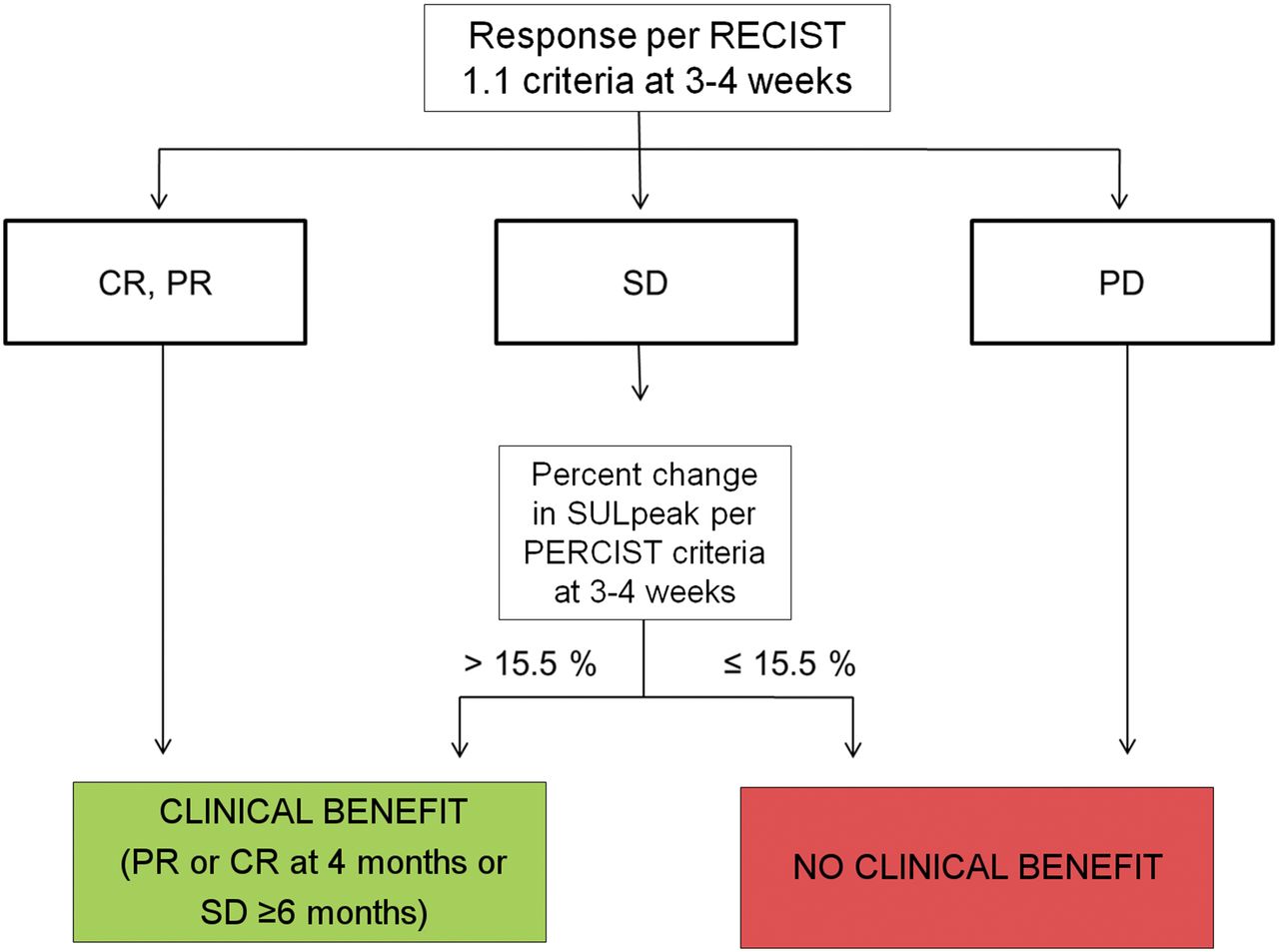
On the basis of the percentage change from SCAN-1 to SCAN-2 of target lesion dimensions (CT) or 18F-FDG uptake (PET), we derived the predictive values of these measurements based on optimal threshold values, calculated using ROC analysis, to forecast outcomes at 4 mo (Table 4). Percentage change per RECIST 1.1 had the highest predictive value, with an accuracy of 85%. Intriguingly, optimal PERCIST and EORTC threshold values predictive of BOR were >15.5% and >14.7%, respectively, indicating that increased 18F-FDG tumor uptake at SCAN-2 may correlate with eventual clinical benefit. Incorporating optimal thresholds using RECIST-based and PERCIST-based changes at SCAN-2, visualized on a 2-dimensional plot (Fig. 1), we retrospectively developed criteria for early of prediction eventual response (PET/CT criteria for Early Prediction of Response to ICI Therapy, incorporating RECIST-based and PERCIST-based changes seen 3–4 wk into treatment) (Fig. 2). Patients whose CT scans demonstrated an objective response by RECIST 1.1 at SCAN-2 maintained a response at 4 mo. Similarly, PD by RECIST 1.1 at SCAN-2 was associated with disease progression at 4 mo. However, in patients with stable disease at SCAN-2, an increase > 15.5% in SULpeak (average SUV corrected by lean body mass within a 1-cm3 spheric volume of interest) of the hottest lesion was associated with eventual clinical benefit, providing a potentially informative indicator based on dual criteria. A case study is provided in Figure 3. The sensitivity, specificity, and accuracy of the proposed criteria to predict response by RECIST 1.1 at 4 mo were 100%, 93.3%, and 95.0%, respectively (Table 4). The predictive capacities of 4 different methods of measurement of changes in tumor burden from SCAN-1 to SCAN-2 to predict eventual response are provided in Supplemental Table 3.
Performance Characteristics of 5 Methods of Early Tumor Response Evaluation in Predicting Response (RECIST 1.1) to ICI Therapy at 4 Months
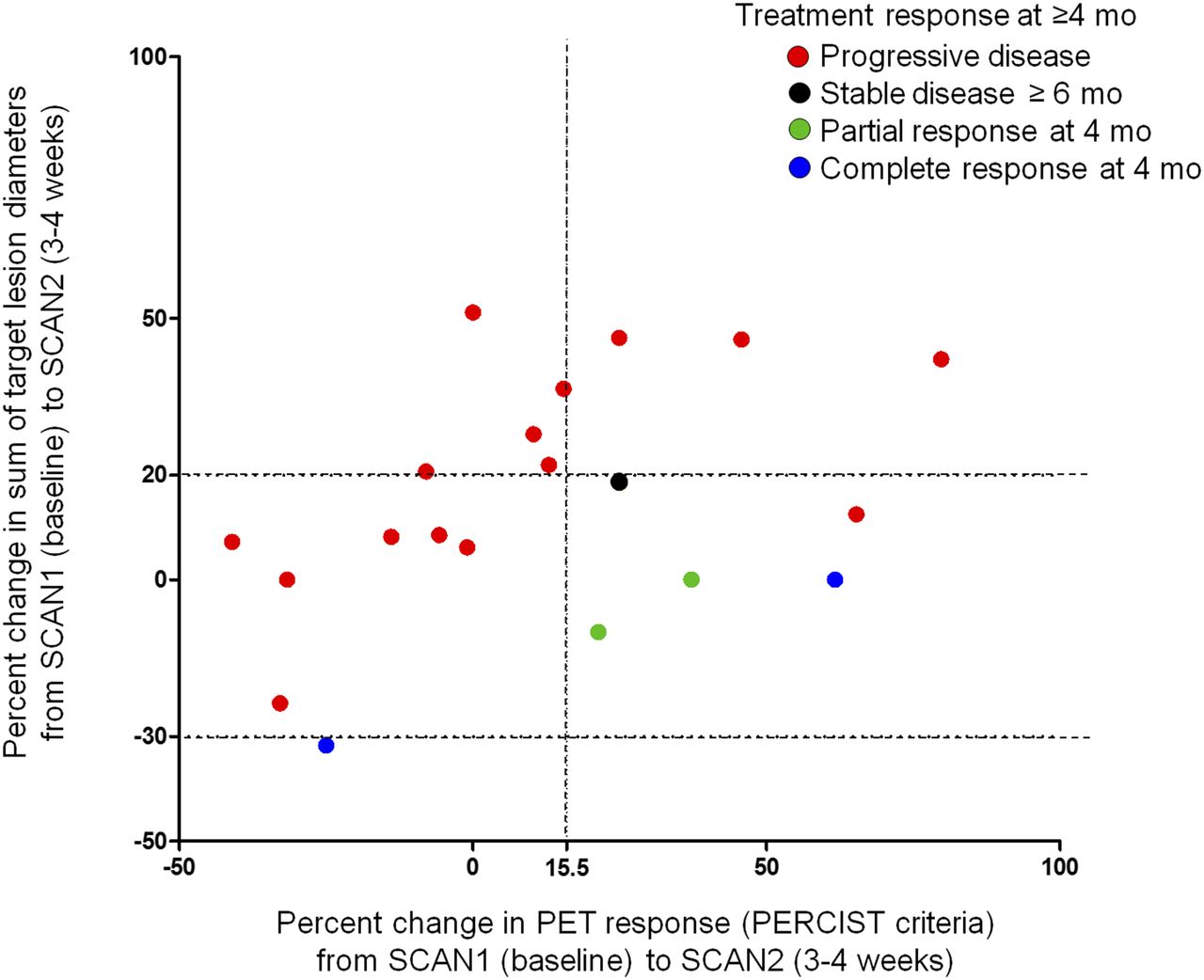
Scatterplot comparing early CT- and PET-based changes with response to ICI at ≥ 4 mo. Each dot represents a single patient, color coded according to best overall response at ≥ 4 mo. Two horizontal dashed lines on y-axis (+20% and −30%) correspond to thresholds for PD and PR, respectively, using RECIST 1.1, in absence of appearance of new tumor lesions. Vertical dashed line at +15.5% on x-axis represents a threshold associated with eventual response according to criteria proposed in Figure 2.

Patients whose CT scans performed 3–4 wk into therapy demonstrate an objective response (PR or CR by RECIST 1.1) are predicted to maintain a response at 4 mo. Similarly, PD detected at that same interval predicts continued disease progression at 4 mo. In patients with stable disease by RECIST 1.1 at 3–4 wk, an increase > 15.5% in SULpeak of hottest lesion by PET is associated with eventual clinical benefit (PR or CR at 4 mo or stable disease ≥ 6 mo). Sensitivity, specificity, and accuracy of algorithm to predict response at 4 mo were 100%, 93.3%, and 95.0%, respectively. CR = complete response; PD = progressive disease; PR = partial response; SD = stable disease; SULpeak = average SUV corrected by lean body mass within a 1-cm3 spheric volume of interest.

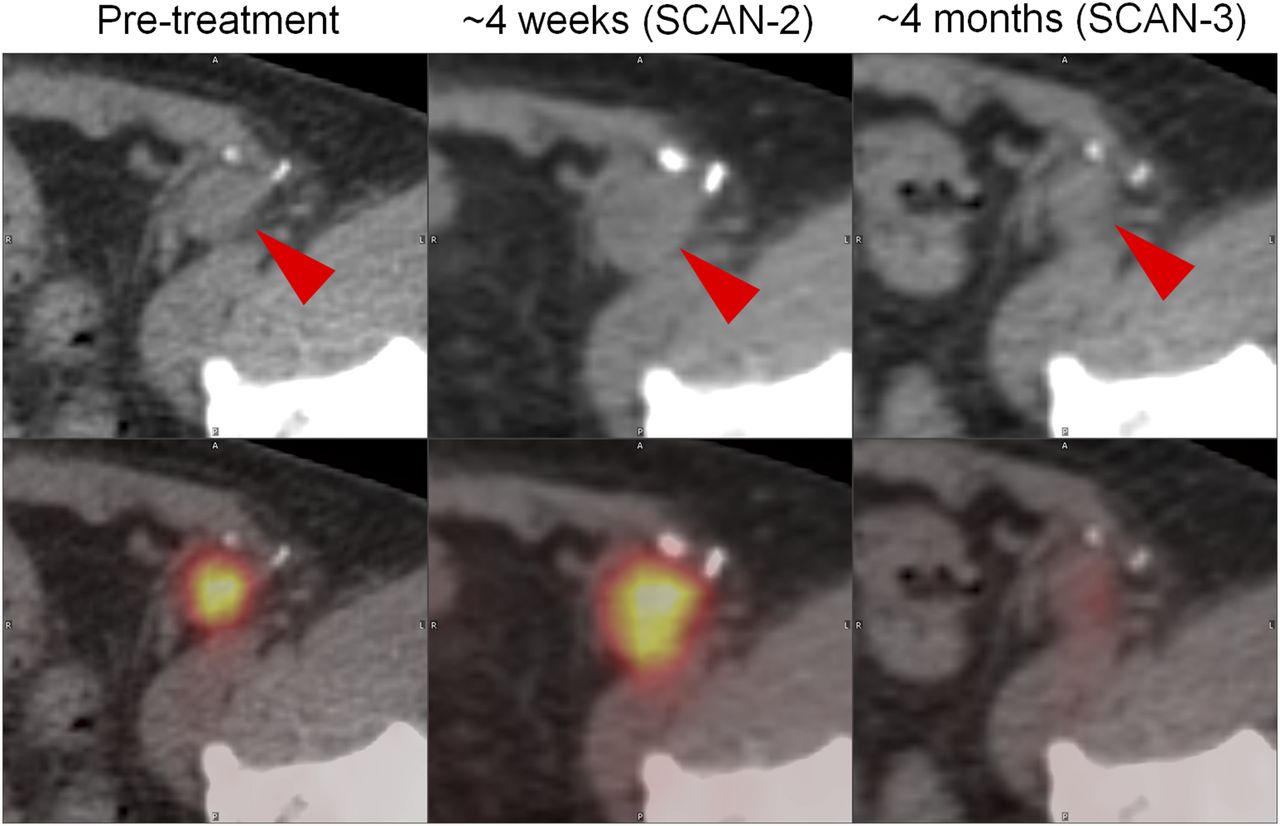
PET/CT images demonstrating representative changes in melanoma inguinal lymph node metastasis (red arrowheads) at 4 wk and 4 mo after initiation of ipilimumab. At about 4 wk (SCAN-2), sum of target lesion diameters assessed by CT scan (top) increased by 18.6% (stable disease by RECIST 1.1). During that same interval, PET imaging revealed 25.1% increase in SULpeak (average SUV corrected by lean body mass within a 1-cm3 spheric volume of interest) (PERCIST). Imaging at approximately 4 mo revealed a marked improvement in 18F-FDG avidity of inguinal lymph node metastasis. Similar pattern was observed in this patient’s other sites of disease, including hepatic, nodal, and soft-tissue metastases. Patient’s metastases outside of brain remained stable for 51 wk.
DISCUSSION
As the use of immune checkpoint blockade agents increases, so too does the challenge of assessing their antitumor efficacy in patients whose posttherapy CT scans may demonstrate unconventional or delayed patterns of response. Although a midtreatment tumor biopsy might provide useful information about the viability of tumor cells and the activity of the immune response within a lesion, biopsy is not always possible because tumors may be inaccessible or multiple. Additionally, biopsies of a single lesion may not accurately capture patients experiencing a mixed response (concomitant regression/progression of individual metastases). Thus, early, whole-body noninvasive indicators of drug efficacy could help to better predict which patients might respond to therapy and guide clinicians in adjusting treatment regimens as appropriate.
Even in patients in whom conventional CT scanning performed at traditional intervals (every 2–3 mo) turns out to be an accurate gauge of therapeutic response, there may still be benefits to early identification of patients not predicted to respond. Early discontinuation of ICI could mitigate the risk for immune-related adverse events, reduce the cost of the therapy, and allow for initiation of a different treatment approach.
Here, we prospectively evaluated the utility of a baseline and follow-up 18F-FDG PET/CT scan, performed early in the course of ICI, as a predictor of BOR at ≥ 4 mo. Because human melanomas consistently have high glucose metabolism, 18F-FDG PET/CT imaging is particularly well suited for detecting these tumors, some of which are difficult to identify by standard CT scans (27,28). PET imaging, performed as early as 7 d after initiation of radioimmunotherapy, has been shown to be predictive of outcomes in patients with lymphoma (29). However, glucose metabolism is sensitive but not specific for neoplastic growth, because other processes such as inflammation involve glucose utilization. Indeed, 18F-FDG PET/CT has been used to detect and monitor treatment efficacy in various inflammatory/infectious processes such as osteomyelitis, prosthesis infection, fever of unknown origin, and sarcoidosis (30).
Consequently, we were not surprised to observe that patients with stable anatomic disease and modest to markedly increased 18F-FDG uptake at SCAN-2 tended to demonstrate eventual tumor regression. Our findings suggest an early inflammatory response at the site of tumor brought about by ICI. These observations are consistent with gene expression profiling analyses demonstrating a correlation between an immunologically active tumor microenvironment and an antitumor response to ipilimumab (31). A similar biology has emerged in the PD-1 literature, in which immune activation reflected by PD-L1 expression in the presence of immune cell infiltrates in pretreatment tumor biopsies correlates with tumor regression (1).
Our observations also support a potential mechanism for pseudoprogression, in which apparent tumor growth on conventional CT scans may reflect an increased density of activated inflammatory cells within the tumor microenvironment. Similar findings were reported by Ribas et al., who demonstrated lymphoid cell activation after the administration of tremelimumab, a CTLA-4 antagonist (32).
Sachpekidis et al. performed a study similar to ours, which investigated the predictive value of 18F-FDG PET/CT performed after 2 cycles (∼6 wk) of ipilimumab in predicting final response to therapy (33). Response classifications were based on EORTC 1999 criteria, which mainly incorporate changes in tumor metabolic activity rather than changes in tumor dimensions. The 2 patients in that study who demonstrated a partial metabolic response at the end of treatment were metabolically classified as having progressive metabolic disease on early PET/CT. Thus, the authors concluded that those 2 patients were incorrectly classified based on early PET/CT. The results of our study suggest that a combination of changes in lesional dimensions along with changes in 18F-FDG uptake may provide a more accurate predictor of eventual response.
Intercriteria agreements between RECIST 1.1, PERCIST, and EORTC were good to excellent at SCAN-3, performed 4 mo after ICI was initiated, which is in accordance with a previous report using cytotoxic chemotherapy (19). However, interestingly, intercriteria agreement between the PET and CT modalities was not good in the early course of ICI therapy. This disagreement should be caused by the paradoxically increased 18F-FDG uptake in the responding tumor in the early course of ICI therapy. Thus, we could incorporate the different response information from PET and CT to propose an early response criteria (PET/CT criteria for Early Prediction of Response to ICI Therapy).
Other potential methods for prediction of ICI therapy response include measurement of circulating tumor DNA in plasma. Small trials have shown that circulating tumor DNA level changes can mirror radiologic changes in tumor burden and may predict eventual response to ICI (34,35). These emerging technologies, which require only serial blood sampling and laboratory analysis, may compare favorably with PET/CT in terms of feasibility and accessibility among an increasing population of patients undergoing therapy with ICI.
Our study is limited by a relatively small sample size, a lack of intravenous contrast agent in many of the CT scans, and a predominance of anti-CTLA-4–directed therapy. Additionally, brain MRI was not routinely performed as a part of our investigation, and because PET/CT imaging is not well-suited for detecting melanoma brain metastases, patients may have had undetected brain metastases during the study period. However, these preliminary findings suggest that PET/CT scans obtained early in the course of ICI therapy, particularly ipilimumab, appear predictive for eventual response in patients with advanced melanoma.
CONCLUSION
Combining functional and anatomic parameters obtained from PET/CT scans performed early in the course of ICI therapy may predict eventual response in patients with advanced melanoma. Increased 18F-FDG uptake in the early course of ICI therapy may be associated with immune activation and favorable outcome. Given the rapidly increasing use of ICI for patients with a variety of malignancies, further prospective study is warranted to assess our proposed tumor assessment criteria in larger cohorts of patients with various cancer types, treated with other checkpoint inhibitors, both as monotherapy and in combination.
DISCLOSURE
This study was supported by a research grant from the Melanoma Research Alliance (Richard L. Wahl and Suzanne L. Topalian) and by The National Institutes of Health grants P30 CA006973 and 5U01CA140204. Evan J. Lipson received a research grant from Genentech and is a consultant for Bristol-Myers Squibb, EMD Serono, Merck, and Novartis. Drew M. Pardoll received a research grant from Bristol-Myers Squibb and is a consultant for Merck. Suzanne L. Topalian received a research grant from Bristol-Meyers Squibb and is a consultant for ImaginAb. Richard L. Wahl is a consultant for Nihon Medi Physics. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Akimosa Jeffrey-Kwanisai and Jeffrey Leal for study support. This study was presented in part at the 2015 Melanoma Research Alliance Scientific Retreat and at the 2013 and 2015 Radiological Society of North America (RSNA) Scientific Assembly and Annual Meetings.
Footnotes
↵* Contributed equally to this work.
Published online Mar. 30, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 23, 2016.
- Accepted for publication March 13, 2017.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Approaches to Imaging Immune Activation Using PET
- Imaging endpoints for clinical trial use: a RECIST perspective
- Dynamic Tumor-Specific MHC-II Immuno-PET Predicts the Efficacy of Checkpoint Inhibitor Immunotherapy in Melanoma
- CD8-Targeted PET Imaging of Tumor-Infiltrating T Cells in Patients with Cancer: A Phase I First-in-Humans Study of 89Zr-Df-IAB22M2C, a Radiolabeled Anti-CD8 Minibody
- Efficacy and safety of neoadjuvant sintilimab, oxaliplatin and capecitabine in patients with locally advanced, resectable gastric or gastroesophageal junction adenocarcinoma: early results of a phase 2 study
- Response Evaluation and Survival Prediction After PD-1 Immunotherapy in Patients with Non-Small Cell Lung Cancer: Comparison of Assessment Methods
- Multimodal Molecular Imaging Detects Early Responses to Immune Checkpoint Blockade
- Mars Shot for Nuclear Medicine, Molecular Imaging, and Molecularly Targeted Radiopharmaceutical Therapy
- Radiomics, Tumor Volume, and Blood Biomarkers for Early Prediction of Pseudoprogression in Patients with Metastatic Melanoma Treated with Immune Checkpoint Inhibition
- Is there a link between very early changes of primary and secondary lymphoid organs in 18F-FDG-PET/MRI and treatment response to checkpoint inhibitor therapy?
- Immune Checkpoint Imaging in Oncology: A Game Changer Toward Personalized Immunotherapy?
- Comparison Between 18F-FDG PET-Based and CT-Based Criteria in Non-Small Cell Lung Cancer Patients Treated with Nivolumab
- Imaging the Cancer Immune Environment and Its Response to Pharmacologic Intervention, Part 1: The Role of 18F-FDG PET/CT
- Preclinical PERCIST and 25% of SUVmax Threshold: Precision Imaging of Response to Therapy in Co-clinical 18F-FDG PET Imaging of Triple-Negative Breast Cancer Patient-Derived Tumor Xenografts
- Detecting Early Response to Immune Checkpoint Blockade by Multimodal Molecular Imaging
- Predictive value of integrated 18F-FDG PET/MRI in the early response to nivolumab in patients with previously treated non-small cell lung cancer
- 18F-FDG PET/CT for Monitoring of Ipilimumab Therapy in Patients with Metastatic Melanoma
- The Immunoimaging Toolbox