


Article Figures & Data
Figures
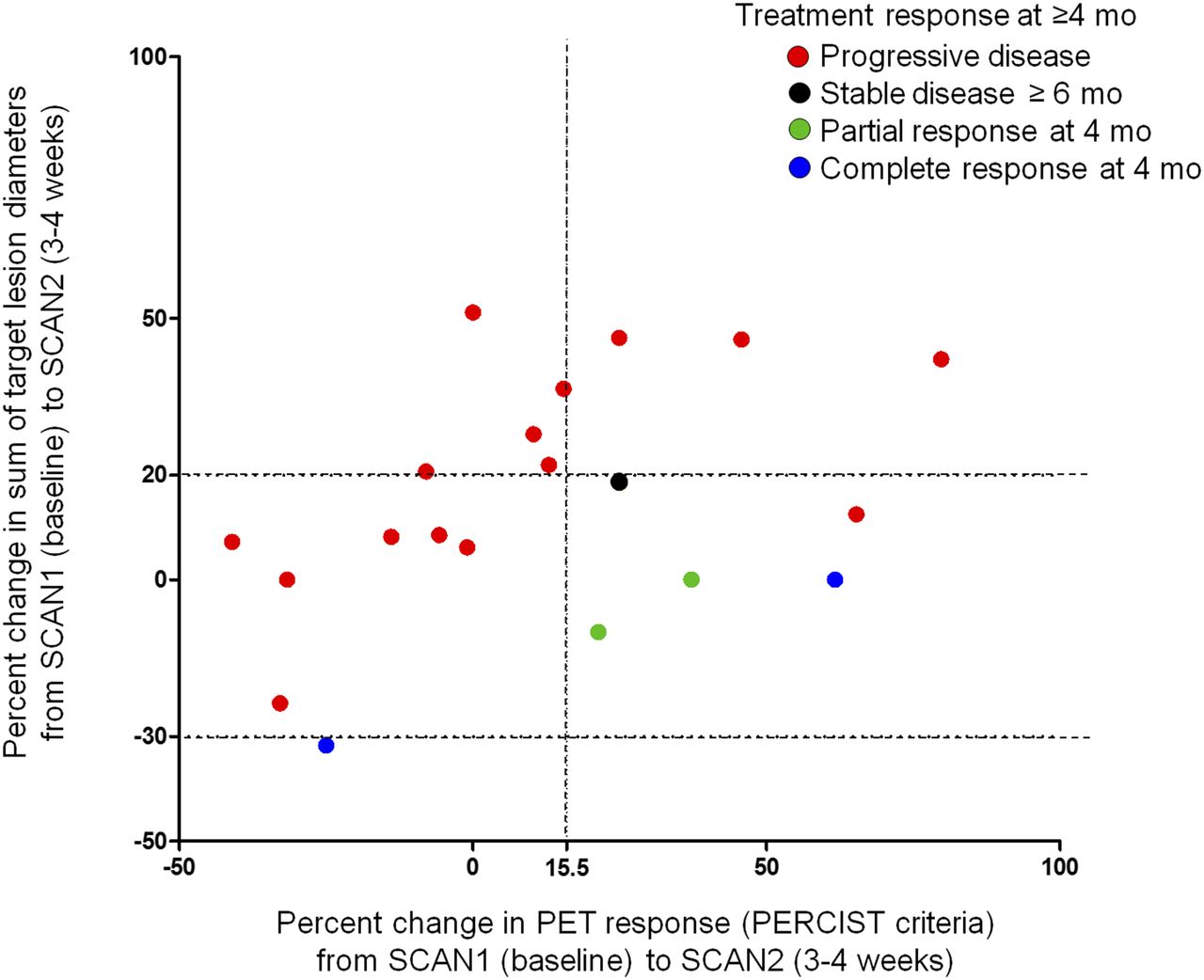
- FIGURE 1.
Scatterplot comparing early CT- and PET-based changes with response to ICI at ≥ 4 mo. Each dot represents a single patient, color coded according to best overall response at ≥ 4 mo. Two horizontal dashed lines on y-axis (+20% and −30%) correspond to thresholds for PD and PR, respectively, using RECIST 1.1, in absence of appearance of new tumor lesions. Vertical dashed line at +15.5% on x-axis represents a threshold associated with eventual response according to criteria proposed in Figure 2.
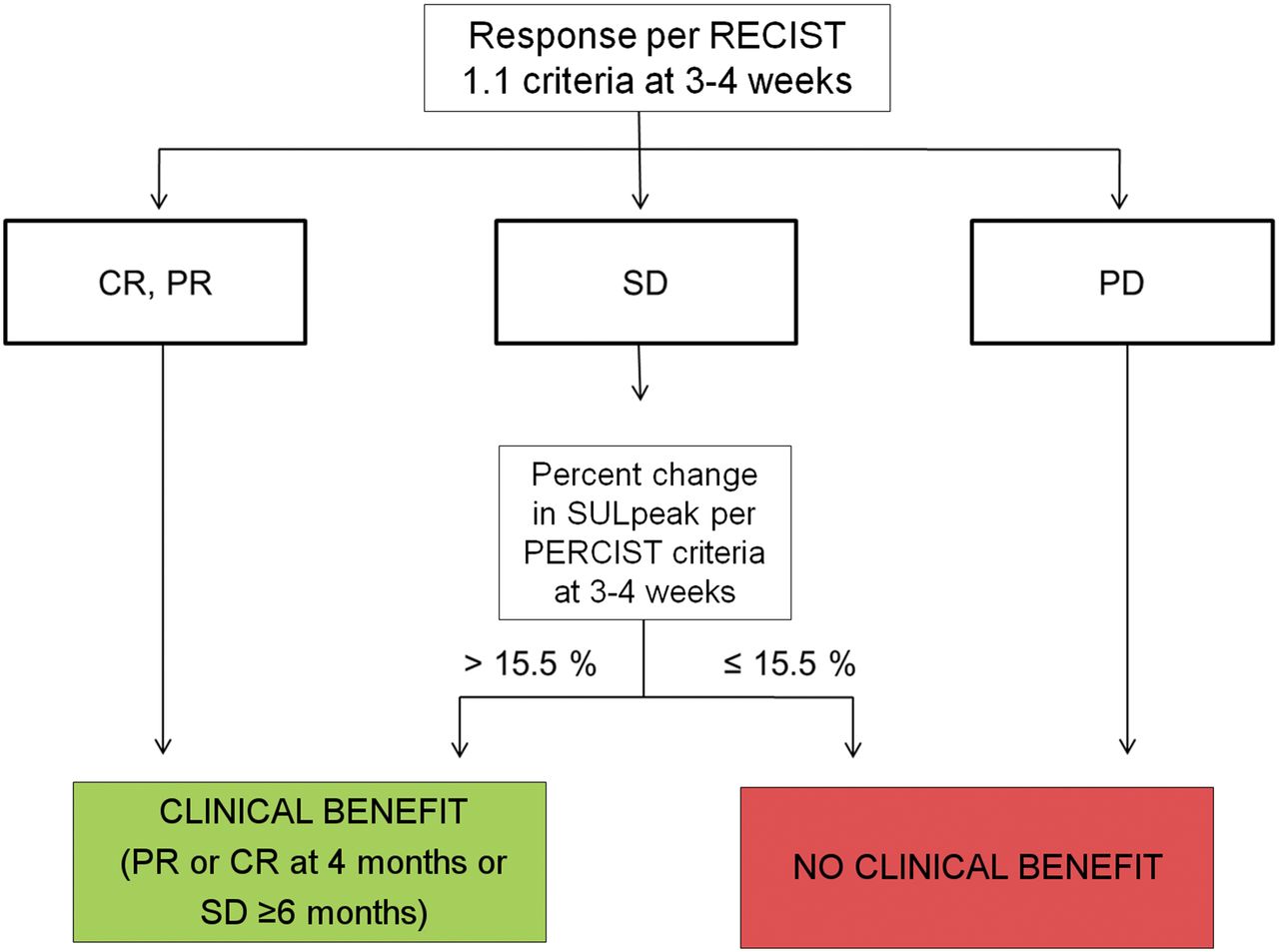
- FIGURE 2.
Patients whose CT scans performed 3–4 wk into therapy demonstrate an objective response (PR or CR by RECIST 1.1) are predicted to maintain a response at 4 mo. Similarly, PD detected at that same interval predicts continued disease progression at 4 mo. In patients with stable disease by RECIST 1.1 at 3–4 wk, an increase > 15.5% in SULpeak of hottest lesion by PET is associated with eventual clinical benefit (PR or CR at 4 mo or stable disease ≥ 6 mo). Sensitivity, specificity, and accuracy of algorithm to predict response at 4 mo were 100%, 93.3%, and 95.0%, respectively. CR = complete response; PD = progressive disease; PR = partial response; SD = stable disease; SULpeak = average SUV corrected by lean body mass within a 1-cm3 spheric volume of interest.
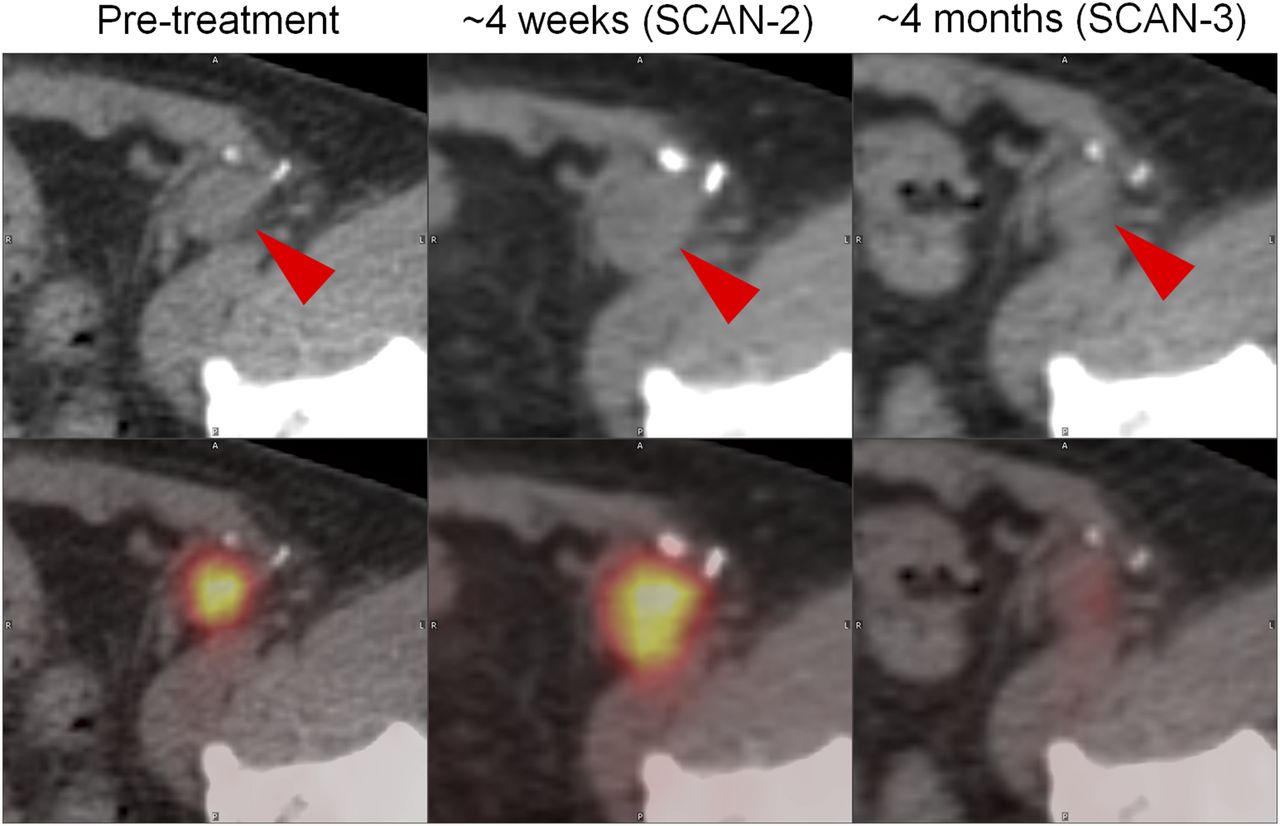
- FIGURE 3.
PET/CT images demonstrating representative changes in melanoma inguinal lymph node metastasis (red arrowheads) at 4 wk and 4 mo after initiation of ipilimumab. At about 4 wk (SCAN-2), sum of target lesion diameters assessed by CT scan (top) increased by 18.6% (stable disease by RECIST 1.1). During that same interval, PET imaging revealed 25.1% increase in SULpeak (average SUV corrected by lean body mass within a 1-cm3 spheric volume of interest) (PERCIST). Imaging at approximately 4 mo revealed a marked improvement in 18F-FDG avidity of inguinal lymph node metastasis. Similar pattern was observed in this patient’s other sites of disease, including hepatic, nodal, and soft-tissue metastases. Patient’s metastases outside of brain remained stable for 51 wk.


Tables
CT-based criteria PET-based criteria Response RECIST 1.1 irRC PERCIST 1.0 EORTC Complete response Disappearance of all TLs and NLs; all LNs < 10 mm short axis Resolution of all lesions (whether measurable or not) and no new lesions Complete metabolic response Complete resolution of 18F-FDG uptake within measurable TL and disappearance of all other lesions to BBP levels Complete resolution of 18F-FDG uptake within TV so that it is indistinguishable from surrounding NT Partial response ≥30% decrease in SoDs of TLs; NLs may persist but not unequivocally progress Decrease in TB ≥ 50%, measured as SoPs of 2 largest perpendicular diameters of all ILs, relative to BL Partial metabolic response >30% RD and >0.8 AD in SULpeak of HL Reduction of 15%–25% in tumor SUV after 1 CoT and >25% after more than 1 CoT Stable disease Neither sufficient TR nor TG to qualify for PR or PD Not meeting criteria for irCR or irPR, in absence of irPD Stable metabolic disease Not meeting criteria for CMR, PMR, or PMD Increase in tumor SUV of <25% or decrease of <15% and no visible increase in extent of 18F-FDG TU (20% in LD) Progressive disease ≥20% increase in sum of diameters of TLs or unequivocal progression of NL or appearance of new lesion Increase in TB ≥ 25% relative to nadir, measured as SoPs of 2 largest perpendicular diameters of all ILs Progressive metabolic disease >30% RI and >0.8 AI in SULpeak of HL or unequivocal progression of 18F-FDG–avid NL or appearance of new 18F-FDG–avid lesion Increase from BL in tumor SUV of >25% within tumor region, visible increase in extent of 18F-FDG TU (20% in LD), or appearance of new 18F-FDG uptake in MLs TL = target lesion; NL = nontarget lesion; LN = lymph node; BBP = background blood-pool; TV = tumor volume; NT = normal tissue; SoDs = sum of diameters; TB = tumor burden; SoPs = sum of the products; IL = index lesion; BL = baseline; RD = relative decrease; AD = absolute decrease; SULpeak = average SUV corrected by lean body mass within a 1-cm3 spheric volume of interest; HL = hottest lesion; CoT = cycle of therapy; TR = tumor regression; TG = tumor growth; PR = partial response; PD = progressive disease; irCR = immune-related complete response; irPR = immune-related partial response; irPD = immune-related progressive disease; CMR = complete metabolic response; PMR = partial metabolic response; PMD = progressive metabolic disease; TU = tumor uptake; LD = longest dimension; RI = relative increase; AI = absolute increase; ML = metastatic lesion; SUV = for EORTC we used SUVmax (maximum voxel value of SUV).
- TABLE 2
Response Assessments, Excluding Brain Lesions, in 20 Patients with Metastatic Melanoma Receiving ICI Therapies
Response at SCAN-2 (21–28 d) Response at SCAN-3 (∼4 mo) Patient no. Treatment RECIST 1.1 irRC PERCIST EORTC RECIST 1.1 irRC PERCIST EORTC Best overall response at ≥ 4 mo (RECIST 1.1) Duration of observation(wk)* Best overall response before SCAN-3 (RECIST 1.1)† 1 Ipilimumab PD PD PMD PMD PD PD PMD PMD PD 10 — 2 Ipilimumab SD PD SMD SMD SD SD PMR PMR SD > 6 mo 51 — 3 Ipilimumab PD PD PMD PMD PD PD PMD PMD PD 15 — 4 Ipilimumab PD PD PMD PMD PD PD PMD PMD PD 15 — 5 Ipilimumab PD PD PMD PMD PD PD PMD PMD PD 18 — 6 BMS-936559 SD SD PMR PMR PD PD PMD PMD PD 23 uSD at 6 wk, PD at 12 wk 7 BMS-936559 SD SD SMD SMD PD PD PMD PMD PD 18 — 8 BMS-936559 PD PD PMD PMD PD PD PMD PMD PD 18 uSD at 6 wk, PD at 12 wk 9 Ipilimumab PD PD PMD PMD PD PD PMD PMD PD 16 — 10 Ipilimumab SD SD PMD PMD PD PD PMD PMD PD 17 — 11 Ipilimumab SD SD PMD PMD CR CR PMR PMR CR 184 — 12 Ipilimumab SD SD PMR PMR PD PD SMD SMD PD 17 — 13 Ipilimumab PD PD PMD PMD PD PD PMD PMD PD 16 — 14 Ipilimumab SD SD SMD PMD PR PR PMR PMR PR 28 — 15 Ipilimumab PD PD PMD PMD PD PD PMD PMD PD 19 — 16 Ipilimumab SD SD PMD PMD PR SD PMD SMD PR 40 — 17 Ipilimumab PR PR SMD PMR CR CR PMR PMR CR 31 — 18 Nivolumab SD SD PMR SMD PD SD PMD PMD PD 23 SD at 8 and 15 wk 19 Ipilimumab PD PD PMD PMD PD PD PMD PMD PD 17 — 20 Ipilimumab PD PD PMD PMD PD SD PMD PMD PD 16 — ↵* Duration of observation is calculated from time of first administration of ICI therapy on this trial. Patients who received ipilimumab were treated with maximum of 4 doses and observed thereafter. Patients who received anti–PD-1/PD-L1 continued to receive therapy until disease progression.
↵† Standard of care on-treatment radiographic assessments performed between SCAN-2 and SCAN-3 for 3 patients demonstrated transient disease stability. Their responses are characterized in last column.
PD = progressive disease; PMD = progressive metabolic disease; SD = stable disease; SMD = stable metabolic disease; PMR = partial metabolic response; PR = partial response; u = unconfirmed, seen only on 1 set of scans; CR = complete response.
Responses based on 4 criteria in 20 patients with metastatic melanoma after receiving ipilimumab (anti–CTLA-4), nivolumab (anti–PD-1), or BMS-936559 (anti–PD-L1). 18F-FDG PET/CT imaging was performed before therapy (SCAN-1), again between days 21 and 28 (SCAN-2), and at approximately 4 mo posttreatment initiation (SCAN-3).
- TABLE 3
Performance of 4 Radiologic Evaluation Criteria Applied to Early (3–4 Week) PET/CT Scans in Predicting Best Overall Response (RECIST 1.1) to ICI Therapy at ≥ 4 Months
Response evaluation criteria Sensitivity (%) Specificity (%) PPV (%) NPV (%) Accuracy (%) RECIST1.1 100.0 (48.0–100.0) 66.7 (38.4–88.1) 50.0 (18.9–81.1) 100.0 (69.0–100.0) 75.0 irRC 80.0 (28.8–96.7) 66.7 (38.4–88.1) 44.4 (14.0–78.6) 90.9 (58.7–98.5) 70.0 PERCIST 60.0 (15.4–93.5) 73.3 (44.9–92.0) 42.9 (10.4–81.2) 84.6 (54.5–97.6) 70.0 EORTC 40.0 (6.5–84.6) 73.3 (44.9–92.0) 33.3 (5.3–77.3) 78.6 (49.2–95.1) 65.0 PPV = positive predictive value; NPV = negative predictive value.
Data in parentheses are 95% confidence intervals.
- TABLE 4
Performance Characteristics of 5 Methods of Early Tumor Response Evaluation in Predicting Response (RECIST 1.1) to ICI Therapy at 4 Months
Method no. Tumor response evaluation method description SCAN-1 to SCAN-2 optimal percentage change cutoff Sensitivity (%) Specificity (%) PPV (%) NPV (%) Accuracy (%) 1 Change in sum of RECIST 1.1–based target lesion diameters ≤0 80.0 (28.8–96.7) 86.7 (59.5–98.0) 66.7 (22.7–94.7) 92.9 (66.1–98.8) 85.0 2 Change in sum of the products of the 2 largest perpendicular diameters of irRC-based index lesions ≤ −14.7 60.0 (15.4–93.5) 93.3 (68.0–98.9) 75.0 (20.3–95.9) 87.5 (61.6–98.1) 85.0 3 Change in SULpeak of the hottest lesion >15.5 80.0 (28.8–96.7) 73.3 (44.9–92.0) 50.0 (16.0–84.0) 91.7 (61.5–98.6) 75.0 4 Change in sum of SUVmax of all 18F-FDG–avid metastatic lesions >14.7 80.0 (28.8–96.7) 66.7 (38.4–88.1) 44.4 (14.0–78.6) 90.9 (58.7–98.5) 70.0 Methods 1 and 3, above, combined (PECRIT) 100.0 (48.0–100) 93.3 (68.0–98.9) 83.3 (36.1–97.2) 100.0 (76.7–100.0) 95.0 PPV = positive predictive value; NPV = negative predictive value; method 1 = change in sum of target lesion diameters, selected based on RECIST 1.1; method 2 = change in sum of the products of the 2 largest perpendicular diameters of index lesions, selected based on irRC criteria; method 3 = change in peak SUV, normalized by lean body mass, of the hottest lesion (SULpeak) seen on PET scan (PERCIST 1.0); method 4 = change in the SUVmax of all 18F-FDG–avid metastatic lesions; PECRIT = PET/CT Criteria for early prediction of Response to Immune checkpoint inhibitor Therapy.
Changes in tumor burden seen on PET/CT scans from baseline (SCAN-1) to 3–4 wk (SCAN-2) were calculated using 4 methods, each based on standard response criteria. Optimal cutoff percentage changes to predict response to ICI therapy based on RECIST 1.1 at 4 mo were determined from ROC analysis. Data in parentheses are 95% confidence intervals.
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Approaches to Imaging Immune Activation Using PET
- Imaging endpoints for clinical trial use: a RECIST perspective
- Dynamic Tumor-Specific MHC-II Immuno-PET Predicts the Efficacy of Checkpoint Inhibitor Immunotherapy in Melanoma
- CD8-Targeted PET Imaging of Tumor-Infiltrating T Cells in Patients with Cancer: A Phase I First-in-Humans Study of 89Zr-Df-IAB22M2C, a Radiolabeled Anti-CD8 Minibody
- Efficacy and safety of neoadjuvant sintilimab, oxaliplatin and capecitabine in patients with locally advanced, resectable gastric or gastroesophageal junction adenocarcinoma: early results of a phase 2 study
- Response Evaluation and Survival Prediction After PD-1 Immunotherapy in Patients with Non-Small Cell Lung Cancer: Comparison of Assessment Methods
- Multimodal Molecular Imaging Detects Early Responses to Immune Checkpoint Blockade
- Mars Shot for Nuclear Medicine, Molecular Imaging, and Molecularly Targeted Radiopharmaceutical Therapy
- Radiomics, Tumor Volume, and Blood Biomarkers for Early Prediction of Pseudoprogression in Patients with Metastatic Melanoma Treated with Immune Checkpoint Inhibition
- Is there a link between very early changes of primary and secondary lymphoid organs in 18F-FDG-PET/MRI and treatment response to checkpoint inhibitor therapy?
- Immune Checkpoint Imaging in Oncology: A Game Changer Toward Personalized Immunotherapy?
- Comparison Between 18F-FDG PET-Based and CT-Based Criteria in Non-Small Cell Lung Cancer Patients Treated with Nivolumab
- Imaging the Cancer Immune Environment and Its Response to Pharmacologic Intervention, Part 1: The Role of 18F-FDG PET/CT
- Preclinical PERCIST and 25% of SUVmax Threshold: Precision Imaging of Response to Therapy in Co-clinical 18F-FDG PET Imaging of Triple-Negative Breast Cancer Patient-Derived Tumor Xenografts
- Detecting Early Response to Immune Checkpoint Blockade by Multimodal Molecular Imaging
- Predictive value of integrated 18F-FDG PET/MRI in the early response to nivolumab in patients with previously treated non-small cell lung cancer
- 18F-FDG PET/CT for Monitoring of Ipilimumab Therapy in Patients with Metastatic Melanoma
- The Immunoimaging Toolbox