


Abstract
A growing body of evidence suggests that gastrin-releasing peptide receptor (GRPR) might be a valuable target in breast cancer. To understand which patients can be potential candidates for GRPR-based imaging or targeted therapy, we screened invasive breast cancers by immunohistochemistry for the presence and intensity of GRPR expression. Methods: We explored a tissue microarray of 1,432 primary breast tumors from patients who underwent surgery between 2000 and 2005 at Institut Bergonié, without prior neoadjuvant treatment. We studied associations between GRPR expression and clinical, pathologic, and biologic parameters. The association between GRPR expression and distant metastasis-free interval was also examined. Results: GRPR overexpression was found in 75.8% of the 1,432 tumors and was most strongly associated with estrogen receptor (ER) positivity (GRPR was high in 83.2% of ER-positive and 12% of ER-negative tumors; P < 0.00001). When molecular subtypes of breast cancer were considered, GRPR was overexpressed in 86.2% of luminal A–like tumors, 70.5% of luminal B–like human epidermal growth factor receptor 2 (HER2)–negative tumors, 82.8% of luminal B–like HER2-positive tumors, 21.3% of HER2-enriched tumors, and 7.8% of triple-negative tumors. Importantly, when breast tumors overexpressed GRPR, high GRPR expression was also found in metastatic lymph nodes in 94.6% of cases. Primary tumors with high GRPR expression were associated with lower risk of distant metastases at follow-up in univariate analysis (Log-rank P = 0.0084) but not in multivariate analysis. Hence, the prognostic impact of GRPR was lost when examined within specific molecular subtypes. Conclusion: Because GRPR is overexpressed in a high percentage of ER-positive tumors, GRPR targeting offers wide perspectives for imaging and treatment in patients with ER-positive breast cancer, using recently developed radiolabeled GRPR ligands.
The overexpression in tumors of receptors for some regulatory peptides offers the possibility of targeting these receptors for imaging or treatment. A well-known example is the targeting of somatostatin receptors in neuroendocrine tumors. PET with radiolabeled somatostatin analogs (e.g.,68Ga-DOTATOC, 68Ga-DOTATATE) is the most exquisite means of imaging these tumors (1), whereas targeted therapy using similar analogs labeled with β-emitting radionuclides (e.g., 90Y-DOTATOC or 177Lu-DOTATATE) offers excellent results in metastatic patients (2). Receptors for other peptides are overexpressed in many tumors, raising hopes for similar achievements (3).
The gastrin-releasing peptide receptor (GRPR) is a G-protein–coupled receptor of the family of bombesin receptors (3–5). GRPR overexpression was found in small cell lung cancer (6) and then in many tumors, including prostate, breast, colon, and pancreatic cancer; head and neck squamous cell tumors; neuroblastomas; and gliomas (4,5).
After early reports on the presence of GRPR in some breast cancer cell lines (7), Halmos et al. studied the binding of the bombesin analog 125I-Tyr4-BN on cell membranes from 100 human breast carcinomas; 33% of the tumors expressed bombesin/GRPR at levels greater than 10 fmol/mg membrane protein and there was a positive correlation between the binding capacity of bombesin and estrogen receptor (ER) levels (8). Using autoradiography, Gugger and Reubi found GRPR to be expressed in 32 of 52 (62%) invasive breast carcinomas. GRPR was also expressed, although heterogeneously, in normal breast tissue (9). Dalm et al. studied frozen sections from 50 breast tumors with autoradiography using the GRPR agonist 111In-AMBA; GRPR was expressed in 96% of specimens (10). In another study, they found that high GRPR messenger mRNA (mRNA) levels were more frequent in samples with positivity for estrogen receptor mRNA ESR1, or progesterone receptor (PR) mRNA, with negativity for ERBB2 status, and in samples with favorable genomic grade (11). These studies show that GRPR is a relevant target in breast cancer, although the rate of GRPR positivity varies from one study to another.
Importantly, radiolabeled GRPR antagonists for PET imaging recently offered interesting results in prostate and breast cancer patients (12–14). 68Ga-SB3 showed good targeting in 4 of 6 patients with metastatic breast cancer (13). In another study, 68Ga-RM2 visualized 13 of 18 breast tumors, with high intensity compared with normal breast tissue, and detected metastatic lesions (14). GRPR antagonists have also now been labeled with therapy radionuclides (e.g., 177Lu-RM2, 177Lu-NeoBOMB1) (15,16).
Selection of appropriate candidates for clinical trials aiming at GRPR imaging or therapy requires precise knowledge of which tumors might overexpress the receptors. Using immunohistochemistry (IHC), we aimed at elucidating GRPR expression in the complex landscape of breast cancer.
MATERIALS AND METHODS
Tissue Microarray
Samples from 1,432 invasive breast cancers from patients having received initial surgery at Institut Bergonié between 2000 and 2005 were included in this study. Quadruplicate cores, 0.6 mm in diameter each, of Hollande-fixed tumor samples were used for the construction of the tissue microarray (TMA). No patient had received neoadjuvant hormone therapy or chemotherapy. After surgery, adjuvant radiotherapy or systemic therapy (hormonal, chemotherapy) was offered according to prevailing guidelines; trastuzumab as adjuvant treatment was not used during this period. Clinical follow-up data had been prospectively entered into a database and were available for this study.
All IHC and fluorescence in situ hybridization (FISH) analyses were performed on the TMA. Human epidermal growth factor receptor 2 (HER2) status was determined according to published recommendations (17). Molecular subtypes of breast cancers were derived from IHC markers, based on ER status, PR status, Ki-67–labeling index, and HER2 status, according to St Gallen consensus (18) and Maisonneuve classification (19).
Molecular subtypes were defined as follows: luminal A–like (ER ≥ 1%; HER2 score 0, 1+, or 2+ with no HER2 amplification by FISH analysis and Ki-67 < 14% or Ki-67 ranging from 14% to 19%; and PR ≥ 20%); luminal B–like HER2− (ER ≥ 1%; HER2 score 0, 1+, or 2+ with no HER2 amplification by FISH analysis and Ki-67 ≥ 20% or Ki-67 14% to 19%; and PR < 20%); luminal B–like HER2+ (ER ≥ 1%; HER2 score 3+ or 2+ with HER2 amplification by FISH analysis); HER2-enriched (HER2 score 3+ or 2+ with HER2 amplification by FISH analysis, ER = 0% and PR = 0%); and triple-negative (ER = 0%; PR = 0%; HER2 score 0, 1+, or 2+ with no HER2 amplification by FISH analysis).
As regards androgen receptor (AR), tumors were considered AR+ if 10% or more of the nuclei were stained, independent of intensity.
Characteristics of our series are presented in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
The Ethics committee of Institut Bergonié waived requirement for informed consent for the present retrospective analysis.
GRPR IHC
Rules for G-protein–coupled receptor IHC studies in human tissues were strictly adhered to (20). Briefly, our validation steps of the IHC assay included: Western blotting of breast cancer cell line lysates, immunochemistry of these cell lines fixed and embedded with the same material as that used for construction of TMA, subcellular localization of the immunostaining, and identification of positive and negative tumors within a dedicated TMA and validation of the signal recorded in IHC by Western blotting of corresponding frozen tumors from patient samples. Then, the TMA of 1,432 tumors was analyzed.
For IHC staining on TMA, 4-μm-thick paraffin-embedded tissue sections were mounted on slides. The IHC procedure was conducted using the Ventana Benchmark-ultra automated staining system and according to the manufacturer’s recommendations. Primary antibodies and procedures are detailed in Supplemental Table 2. IHC results for GRPR were assessed under light microscope by a senior pathologist and expressed as an immunoreactive score (IRS) (21) that took into account staining intensity (0 for no staining, 1 for weak staining, 2 for moderate staining, and 3 for strong staining) and the percentage of stained tumor cells (0 for no positive cells, 1 for ≤10% positive cells, 2 for 11%–50% positive cells, 3 for 51%–80% positive cells, and 4 for >80% of positive cells). The final IRS score (staining intensity × percentage of positive cells) thus ranged from 0 to 12. For the purpose of our study, no GRPR expression referred to IRS 0–1, weak GRPR expression referred to IRS 2–3, moderate GRPR expression meant IRS 4–8, and strong GRPR expression meant IRS 9–12.
Statistical Analysis
For association with other parameters, GRPR data were dichotomized into 2 groups: low GRPR (absent/weak GRPR expression) and high GRPR (moderate/strong GRPR expression). We studied associations between GRPR expression and the various parameters displayed in Supplemental Table 1. Differences between categorized variables were assessed with the χ2 test or Fischer exact test. All P values were 2-sided, and a P value of less than 0.05 was considered statistically significant. Factors that are predictive of high GRPR expression (moderate/strong) were investigated by univariate and multivariate analysis using a logistic regression. Odds ratios and their 95% confidence intervals (95% CIs) were reported.
The median follow-up was calculated by the reverse Kaplan–Meier method. Probabilities of overall survival (OS) and distant metastasis-free interval (DMFI) were calculated with the Kaplan–Meier method. The log-rank test was used for comparison between GRPR groups. For OS, all causes of death were considered as events. For DMFI, all distant metastatic events were considered and patients with no metastases were censored at the date of last news. Multivariate analyses for DMFI were calculated with a Cox model. Variables significant at the 0.05 level in the univariate analysis were introduced in the multivariate model, which used a stepwise descending maximum likelihood method. Hazard ratios (HRs) and their 95% CIs were reported. For validity of the Cox model, proportionality was tested with the residuals test. For lymph node status, patients who did not receive lymph node dissection (Nx) were kept in the prognostic model as a separate category.
Statistical analyses were performed using the SAS software (version 9.3; SAS Institute, Inc.).
Lymph Node Metastases (Ancillary Study)
In addition to our investigation of the TMA of primary tumors, we studied 37 lymph node metastases from 37 patients (1 lymph node per patient) whose primary breast tumors were positive for GRPR. This ancillary study aimed at verifying that GRPR expression is maintained in metastatic tissue.
RESULTS
Validation Steps for GRPR IHC
Analysis of various human breast cancer cell lines (MCF-7, ZR75.1, SKBR3, MB-453, MDA-MB-468, and T47-D) revealed a good correlation between GRPR signal recorded with Western blot and that seen with immunocytochemistry (Supplemental Table 3). Western blots showed a single band at the expected GRPR molecular weight (Supplemental Fig. 1).
Analysis of tumoral tissue from 34 patients showed good correlation of GRPR signals at IHC on Holland-fixed paraffin-embedded material and on Western blot analyses of corresponding fresh frozen tissue (Supplemental Fig. 1B).
GRPR Expression in 1,432 Breast Cancers and Its Association with Pathologic and Biologic Parameters
GRPR exhibited a predominantly intracytoplasmic expression in tumor cells and with concomitant immunoreactivity of the cell membrane. This distribution fits the established criteria on IHC for G-protein–coupled receptors (20). Tumor-associated stromal tissue showed either no or weak expression of GRPR.
Among 1,432 invasive breast cancers, GRPR expression was absent in 145 (10.1%) tumors (IRS score = 0 or 1), weak in 202 (14.1%) tumors (IRS score = 2 or 3), moderate in 512 (35.8%) tumors (IRS score = 4–8), and strong in 573 (40.0%) tumors (IRS score = 9–12). Representative IHC samples are shown in Figure 1.
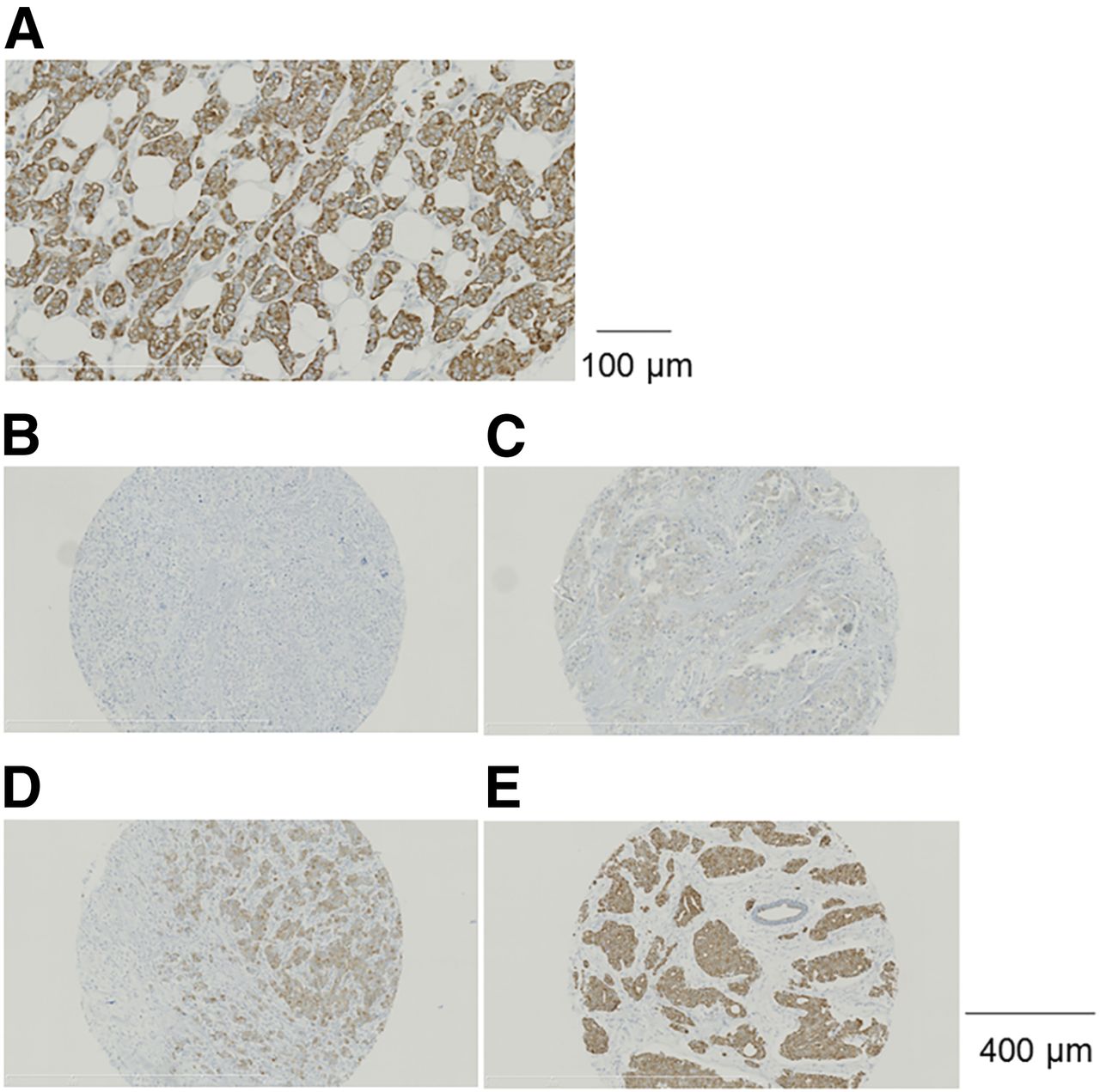
(A) Membrane and cytoplasmic localization of GRPR immunostaining in a breast cancer specimen (magnification, ×20). (B–E) Representative samples of breast cancer specimens showing the 4 categories of GRPR immunostaining results: no GRPR expression (IRS score 0 or 1) (B), weak GRPR expression (IRS score 2 or 3) (C), moderate GRPR expression (IRS score 4–8) (D), and strong GRPR expression (IRS score 9–12) (E) (magnification, ×10).
When results were dichotomized into 2 groups to study associations with other parameters, 347 tumors (24.2%) were GRPR-low (absent/weak) and 1,085 tumors (75.8%) were GRPR-high (moderate/strong).
Associations between GRPR expression (high vs. low) and various pathologic and biologic parameters are summarized in Table 1. GRPR-high was more frequent in tumors from women older than 40 y (77.1% vs. 54.1%; P < 0.00001) and in tumors less than 20 mm (79.1% vs. 69%; P = 0.00003), whereas no difference was observed between invasive ductal carcinomas and invasive lobular carcinomas (74.6% vs. 80.7%; P = 0.09). GRPR-high was more frequent in SBR (Scarff–Bloom–Richardson) grades I/II than in grade-III tumors (85.3% vs. 51.4%; P < 0.00001) and in tumors with Ki-67 < 20% than in tumors with Ki-67 ≥ 20% (83% vs. 50.2%; P < 0.00001). GRPR-high was slightly more frequent in tumors from patients without nodal involvement (76.7% vs. 71.2%; P = 0.03). There was a striking difference in the rate of GRPR-high between ER-positive and ER-negative tumors (83.2% vs. 12%; P < 0.00001) (Table 1). GRPR-high was also more frequent in PR-positive tumors (84.1% vs. 39.1%; P < 0.00001) and in AR-positive tumors (81.5% vs. 37%; P < 0.00001). GRPR was high in 77.2% of HER2-negative and in 63% of HER2-positive tumors (P = 0.0001).
Distribution of Low and High GRPR Expression Within Different Categories of Breast Cancers
Table 2 shows results of univariate and multivariate analyses of factors predictive for high GRPR expression. In multivariate analysis, ER positivity was the most important predictor (odds ratio, 11.998; 95% CI, 5.980–24.075; P < 0.0001).
Univariate and Multivariate Analysis of Predictors of High GRPR Expression
GRPR Expression in ER-Positive Tumors
High GRPR expression in ER-positive tumors makes this group of particular interest as regards GRPR targeting for imaging or therapy. Among the 1,282 ER-positive tumors, GRPR was highly expressed in 83.2% of tumors overall, with only small variations between different categories (Table 3). GRPR-high is somewhat more frequent in women older than 40 y (83.9% vs. 70.8%; P = 0.006), in tumors less than 20 mm (85.1% vs. 79.2%; P = 0.009), in tumors with lower SBR grade (I and II vs. III, 86.8% vs.70.4%; P < 0.00001) or with Ki-67 less than 20% (86.7% vs. 70%; P < 0.00001), in PR-positive tumors (84.1% vs. 74.1%; P = 0.006), and in AR-positive tumors (84.5% vs. 67%; P = 0.00002). There was no influence of HER2 status, histologic subtype (invasive ductal carcinoma vs. invasive lobular carcinoma), or nodal status (N+ vs. N0) (Table 3).
Distribution of Low and High GRPR Expression Within Different Categories of ER-Positive Tumors
There was no linearity between the percentage of ER-positive cells and the probability of GRPR overexpression (Pearson linear correlation coefficient = 0.403). However, the 19 tumors with only 1%–9% ER-positive cells had lower rates of GRPR overexpression (55.6% vs. 83.6%; P = 0.005).
GRPR Expression in ER-Negative Tumors
When ER-negative tumors were considered together (n = 150), high GRPR expression was found in only 12%. GRPR-high was more frequent in HER2-positive tumors (21.3% vs. 7.8%; P = 0.018) or in AR-positive tumors (19.3% vs. 7.5%; P = 0.03). No other associations were found (Supplemental Table 4).
GRPR Expression in Different Molecular Subtypes of Breast Cancer
GRPR-high was found in 86.2% of luminal A–like tumors, in 70.5% of luminal B–like HER2-negative tumors, and in 82.8% of luminal B–like HER2-positive tumors. Among ER-negative subtypes, only 21.3% of HER2-enriched cases and 7.8% of triple-negative breast cancer cases were GRPR-high (Table 4).
Distribution of Low and High GRPR Expression Within Different Molecular Subtype of Breast Cancers
GRPR Expression and Outcomes
Median follow-up was 122 mo. Distant metastases occurred in 153 patients. There were 198 deaths overall.
Figure 2 shows Kaplan–Meier curves for OS and DMFI according to GRPR status. There was no difference in OS (Log-rank P = 0.1056). Less distant metastases occurred in the GRPR-high group (Log-rank P = 0.0084). Ten-year DMFI was 89.9% in the GRPR-high group and 85.1% in the GRPR-low group.
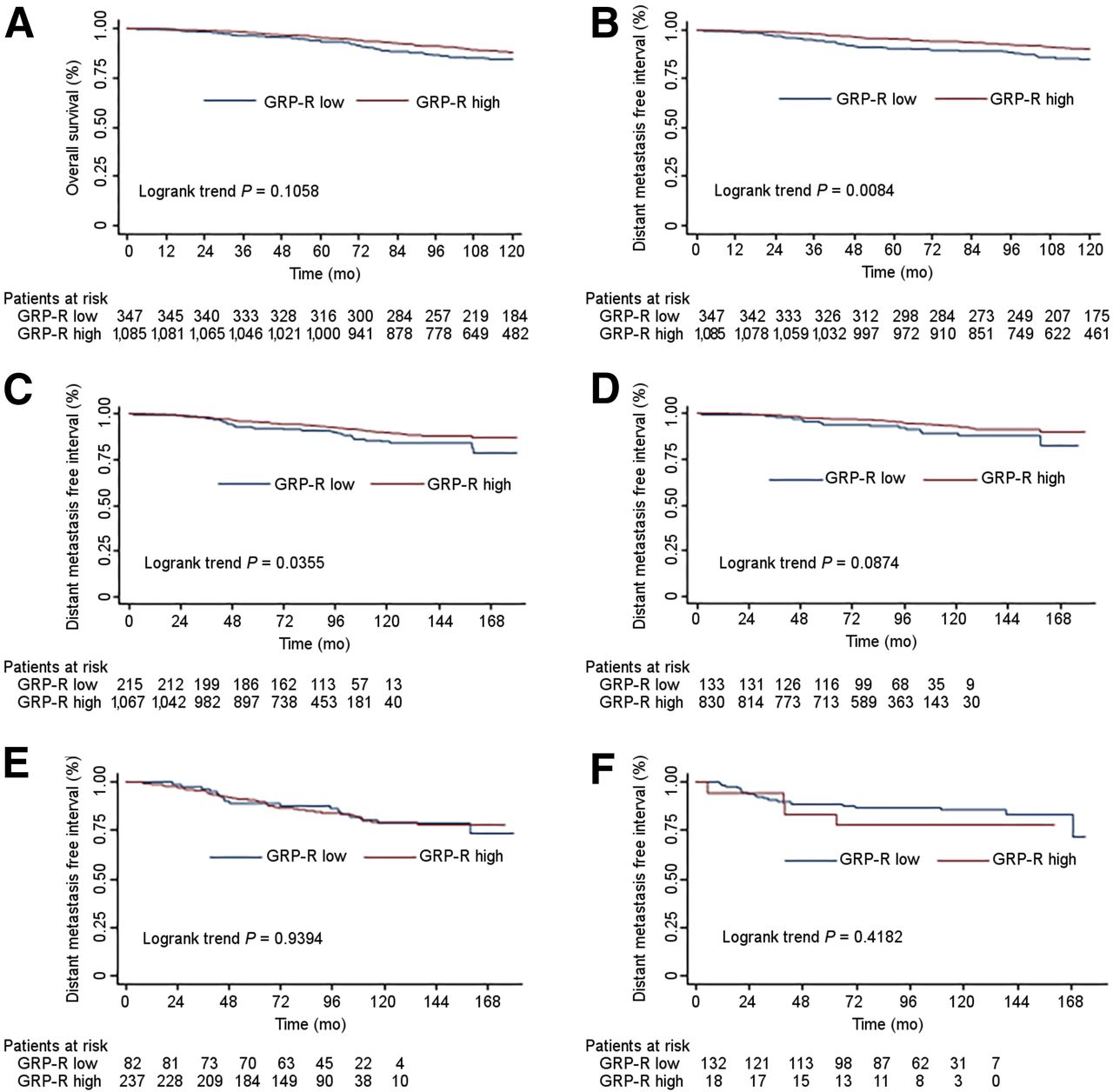
(A) Association of GRPR expression in primary tumors with OS in 1,432 patients. (B) DMFI in 1,432 patients according to GRPR expression in primary breast tumor. (C) DMFI in ER-positive tumors as a function of GRPR expression. (D) DMFI in luminal-A tumors as a function of GRPR expression. (E) DMFI in luminal-B tumors as a function of GRPR expression. (F) Distant MFI in ER-negative tumors as a function of GRPR expression.
Among the 1,282 ER-positive cases (Fig. 2C), there also was less distant metastases in the GRPR-high group (log-rank P = 0.0355). However, when examined within molecular subgroups, there was no association between GRPR expression and DMFI (luminal-A, P = 0.0874; luminal-B, P = 0.9394) (Figs. 2D and 2E). Also, in a multivariate analysis of factors associated with DMFI in ER-positive cases, only tumor size (>2 cm, HR = 2.2), tumor grade (grade II vs. grade I HR = 3.0; grade III vs. grade I HR = 2.6) and positive node status (HR = 2.2) were significant prognostic factors (Supplemental Table 5).
In ER-negative tumors, there was no association between GRPR expression and DMFI (P = 0.42) (Fig. 2F).
GRPR Expression in Lymph Node Metastases from Patients with GRPR-Positive Breast Tumor (Ancillary Study)
Among the 37 studied lymph nodes metastases, GRPR was absent in 1 (2.7%), weak in 1 (2.7%), moderate in 23 (62.2%), and strong in 12 (32.4%). When results were dichotomized, as performed for primary tumors, 2 (5.4%) lymph nodes metastases were GRPR-low and 35 (94.6%) were GRPR-high. Staining distribution was mostly homogeneous.
DISCUSSION
The overexpression of GRPR in breast cancer raises hopes for imaging (13,14), for radioligand therapy (3,15,16,22), or for selective delivery of chemotherapy or nanoparticles with diverse designs (23). Comprehending the full potential of GRPR targeting requires precise knowledge of which tumors might overexpress the receptors.
In the present study of 1,432 breast cancers, there was a striking association between GRPR expression and ER status. GRPR overexpression at IHC was found in 83.2% of ER-positive tumors and in only 12% of ER-negative tumors (P < 0.00001) (Table 1). These results agree with earlier findings (8,10,11). To further understand associations with GRPR, we performed a multivariate analysis taking into account multiple clinicopathologic and biologic parameters. ER positivity was the most important predictor of high-GRPR expression (OR: ∼12; P < 0.0001) (Table 2).
Within the ER-positive subgroup, there were only small variations in GRPR overexpression (according to tumor size, SBR grade, Ki-67 index, PR status, or AR status); the probability of GRPR overexpression would exceed 70% in most subsets (Table 3). Trials to assess the correlation between GRPR expression on IHC and uptake on GRPR PET imaging will be useful. As regards tumors with only 1%–9% ER-positive cells, representing about 1.5% of ER-positive tumors, GRPR overexpression was found in only 55.6% of cases. In GRPR imaging trials, this subgroup may need to be analyzed separately. When considering molecular subtypes of ER-positive breast cancer, GRPR overexpression was somewhat more frequent in luminal A–like tumors (86.2%) than luminal B–like HER2-negative tumors (70.5%) and luminal B–like HER2-positive tumors (82.8%). Given the association between GRPR overexpression and ER positivity, we are currently investigating with IHC the impact of hormonal neoadjuvant therapy on GRPR expression.
The prognostic value of GRPR probability results from its association with ER status. Its prognostic impact is lost when examined within specific molecular subgroups (Fig. 2) or in multivariate analysis (Supplemental Table 5).
An important finding is that GRPR expression is conserved in nodal metastases. We examined lymph nodes from 37 patients with GRPR-positive breast tumors. In 35 cases (94.6%), lymph nodes metastases were GRPR-high. Staining was mostly homogeneous. These results confirm previous findings from Gugger and Reubi (9) and recent genomic data on GRPR mRNA expression in lymph nodes and distant lesions from Dalm et al. (24).
Pilot studies of imaging with radiolabeled GRPR antagonists are quite encouraging (13,14). 68Ga-SB3 showed good targeting in 4 of 6 unselected patients with metastatic breast cancer (13). In another study, 68Ga-RM2 visualized 13 of 18 primary tumors and identified metastatic sites (internal mammary nodes, bone lesions). When only ER-positive tumors were considered, 68Ga-RM2 PET identified 13 of 14 tumors (14). These results suggest a potential role for GRPR PET imaging that might be complementary to that of 18F-FDG in ER-positive breast cancer patients, because 18F-FDG uptake can be limited in low-grade tumors and in lobular carcinoma (25–27). 16α-18F-fluoro-17β-estradiol is a useful tracer because it allows the assessment of ER expression and prediction of the outcome of hormonal treatment (28). The use of GRPR imaging to monitor endocrine therapy also deserves investigation (29).
In light of the presented results, we are planning GRPR imaging trials in ER-positive breast cancer patients. We will examine sensitivity in staging patients who have either locally advanced disease or de novo diagnosis of metastatic breast cancer. Comparison will be made with 18F-FDG. We are also planning to study the role of GRPR imaging in assessing response to hormonal treatment in the neoadjuvant setting and in metastatic disease in comparison with 16α-18F-fluoro-17β-estradiol.
The specific advantage of GRPR imaging over other tracers for breast cancer is that it offers unique perspectives for targeted radionuclide therapy. When metastases show high uptake on PET imaging with 68Ga-labeled GRPR ligands, this means that the same ligands labeled with β-emitters (e.g., 177Lu, 90Y, 161Tb) might be envisaged for targeted therapy (22). Pharmacologic side effects encountered with agonist analogs of GRPR (abdominal cramps, emesis) (30) are avoided when using antagonists (15). Some 177Lu-labeled GRPR antagonists have been tested in preclinical studies, with excellent tumor targeting, and are expected to enter clinical trials (15,16). These preclinical data point to the pancreas as the dose-limiting organ regarding the density of GRPR expression. Importantly, the pharmacokinetics of 177Lu-RM2 show much faster clearance from the pancreas than tumors (15). It has also been shown with 177Lu-NeoBOMB1 that the tumor-to-pancreas uptake ratios can be highly improved by careful selection of the amount of injected peptide (16). Thus, GRPR-targeted therapy using radiolabeled antagonists opens new perspectives in ER-positive patients with distant metastases who failed prior therapies.
One limitation to our study on breast cancer TMA is that we could not assess GRPR in nonneoplastic breast tissue compartments. Recent results of PET/CT imaging with the GRPR antagonist 68Ga-RM2 showed only low to moderate uptake in normal breast (14).
CONCLUSION
Our findings on a large tumor bank of primary operable breast cancer show that GRPR is overexpressed in 83% of ER-positive tumors. When the primary tumor had high GRPR expression, this overexpression was also found in lymph node metastases in 94.6% of cases. Clinical trials in ER-positive breast cancer will assess the value of GRPR targeting for imaging or therapy, a promising avenue.
DISCLOSURE
This work was funded by the French Investment for the Future program within LabEx TRAIL ANR-10-LABX-57. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Colette Riès, Lionnelle Belanga, and Catherine Savona-Baron for their precious assistance.
Footnotes
Published online Mar. 9, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 6, 2016.
- Accepted for publication February 17, 2017.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Vision for Gastrin-Releasing Peptide Receptor Targeting for Imaging and Therapy: Perspective from Academia and Industry
- Diagnostic Potential of 68Ga-NeoB PET/CT with Estrogen Receptor- and Progesterone Receptor-Positive Breast Cancer Undergoing Staging or Restaging for Metastatic Disease
- Gastrin-Releasing Peptide Receptor Imaging and Therapy in the Era of Personalized Medicine
- Preclinical Investigation of [212Pb]Pb-DOTAM-GRPR1 for Peptide Receptor Radionuclide Therapy in a Prostate Tumor Model
- Comparison of 68Ga-PSMA-617 PET/CT and 68Ga-RM2 PET/CT in Patients with Localized Prostate Cancer Who Are Candidates for Radical Prostatectomy: A Prospective, Single-Arm, Single-Center, Phase II Study
- Substitution of L-Tryptophan by {alpha}-Methyl-L-Tryptophan in 177Lu-RM2 Results in 177Lu-AMTG, a High-Affinity Gastrin-Releasing Peptide Receptor Ligand with Improved In Vivo Stability
- A Radiotracer for Molecular Imaging and Therapy of Gastrin-Releasing Peptide Receptor-Positive Prostate Cancer
- Imaging the Distribution of Gastrin-Releasing Peptide Receptors in Cancer
- Somatostatin Antagonists for Radioligand Therapy of Nonendocrine Tumors