


Abstract
Targeting tumor-expressed receptors using selective molecules for diagnostic, therapeutic, or both diagnostic and therapeutic (theragnostic) purposes is a promising approach in oncologic applications. Such approaches have increased significantly over the past decade. Peptides such as gastrin-releasing peptide receptors targeting radiopharmaceuticals are small molecules with fast blood clearance and urinary excretion. They demonstrate good tissue diffusion, low immunogenicity, and highly selective binding to their target cell-surface receptors. They are also easily produced. Gastrin-releasing peptide receptors, part of the bombesin family, are overexpressed in many tumors, including breast and prostate cancer, and therefore represent an attractive target for future development.
NOTEWORTHY
GRPRs, part of the bombesin family, are overexpressed in many malignancies, including breast and prostate cancer, and therefore represent an attractive target for future development.
Peptides such as GRPR-targeting radiopharmaceuticals are small molecules with fast blood clearance and urinary excretion.
Both diagnostic and therapeutic versions have been developed and are currently in clinical trials.
Cancer remains the number 2 cause of death in the United States, second only to heart disease. It is estimated that approximately 606,880 Americans will die from cancer and 1,806,590 new cancer cases will be diagnosed in the United States in 2020 (1). The receptor-mediated targeting of tumors is an area of investigation under constant development that attempts to identify a biomarker that is overexpressed on the surface of cancer cells and bind its ligand to carriers that allow tumor visualization and treatment. The success of this approach depends on the selectivity of the receptor for certain malignant cells, as well as on its binding specificity to the targeting ligand. Here, we will introduce the bombesin receptor family and focus on the gastrin-releasing peptide receptors (GRPRs), which are overexpressed in various cancers (2–8). A special emphasis will be on prostate and breast cancers, in which GRPR expression has been studied the most.
BOMBESIN
Bombesin is a 14-amino-acid peptide (Pyr-Gln-Arg-Leu-Gly-Asn-Gln-Trp-Ala-Val-Gly-His-Leu-Met-NH2) purified for the first time in 1970 from the skin of 2 European frogs, Bombina and Bombina variegate (9,10). Bombesin had a structural similarity to that of ranatensin, a peptide isolated only few months earlier from the skin of a different frog (11). In 1978, the mammalian counterpart to the amphibian bombesin was isolated from porcine nonantral gastric tissue and called gastrin-releasing polypeptide (GRP) because of its main function, gastric acid stimulation due to the release of gastrin (12). Later on, Minamino et al. identified the mammalian counterpart to the amphibian ranatensin in the porcine spinal cord, and they called it neuromedin-B (13). These 2 mammalian bombesin peptides are highly expressed in the human peripheral tissues and in the central nervous system (14). Three different receptors have been discovered for the mammalian bombesin peptides: BB1 (neuromedin-B receptor), BB2 (GRPR), and BB3 (bombesin receptor subtype 3) (15–18). These are 7-transmembrane-domain, G-protein–coupled receptors. Bombesin receptor subtype 3 is an orphan receptor, which means that at present its natural ligand is unknown, but it has been included in the bombesin receptor family because of its high homology to neuromedin-B receptor and GRPR (19,20). Among them, GRPR has been the most extensively studied.
GRP AND GRPR NORMAL BIODISTRIBUTION AND PHYSIOLOGIC FUNCTION
GRPRs are highly concentrated in the pancreas and expressed at lower levels in the colon, breast, prostate, and some regions of the central nervous system, including hippocampus, hypothalamus, amygdala, and pons (21,22). The first human atlas of the physiologic uptake of a GRPR antagonist radiolabeled with 68Ga has been recently published by our group: the highest uptake was seen in the pancreas, followed by clearance in the urinary system; mild to moderate uptake was seen in the gastrointestinal tract (23).
GRP binds with very high affinity to GRPR, which mediates various physiologic mechanism in the human body: it controls gastrointestinal motility and gastric emptying, inducing smooth muscle contraction (24); it causes the release of endogenous gastrin by activating sensory neurons in the gastric mucosa (25,26); it regulates the release of pancreatic enzymes (27); and it has a role in the immunologic responses (28,29) and in several brain functions such as regulation of circadian rhythm (30,31), memory (32), stress, fear, and anxiety (33–35).
GRP AND GRPR EXPRESSION IN VARIOUS CANCERS
GRP and GRPR expression and mechanisms of action have been widely studied both in vitro and in vivo for many different tumor types. Most of the studies have described GRPR acting as an autocrine growth factor receptor in tumor cells, increasing their ability to proliferate. Another hypothesis is that GRP and GRPR would act as a morphogen factor able to retain the tumor in a better-differentiated state. This has been evaluated in colon cancer in vivo xenograft studies, in which moderately differentiated tumors became better differentiated in mice expressing GRP and GRPR but progressively degenerated into poorly differentiated tumors in GRP- and GRPR-negative mice (36).
GRPR expression is higher in prostate cancer than in normal prostate tissue, but variable expression can be found in benign prostate hyperplasia (6,37,38), and the degree to which this may confound image interpretation, creating false-positive findings, is still under investigation. Several groups evaluated the correlation between GRPR expression and clinical features of prostate cancer such as Gleason score, stage of disease, and prostate-specific antigen (PSA) levels (38–42). The results are not definitive, and prospective trials should be performed to evaluate the relationship between GRPR expression and stage of disease, and in androgen-naïve versus castration-resistant patients, to better select cases in which the use of this molecular target is appropriate.
GRPR overexpression in breast cancer has been extensively demonstrated (7,43–49), particularly in estrogen receptor (ER)–expressing tumors (50–52). A recent study analyzed and compared 68Ga-RM2 (DOTA-4-amino-1-carboxymethyl-piperidine-d-Phe-Gln-Trp-Ala-Val-Gly-His-Sta-Leu-NH2) and 18F-FDG–specific binding in tumoral areas of 14 breast cancer samples using tissue microimaging. Immunohistochemistry for ER, progesterone receptor (PR), Ki-67, human epidermal growth factor receptor type 2, and GRPR was also assessed in all specimens (50). The authors found a significantly higher specific binding of 68Ga-RM2 in the ER- and PR-positive groups than in ER- and PR-negative tumors; 68Ga-RM2 binding was higher in the low–Ki-67 group, whereas no difference was associated with human epidermal growth factor receptor type 2 status. 18F-FDG uptake was lower in ER-positive than in ER-negative cancers; it looked similar in PR groups and higher in the high Ki-67 group, and no differences were associated with human epidermal growth factor receptor type 2 status. 68Ga-RM2 binding was significantly higher in tumors without 18F-FDG uptake. These results suggest that 68Ga-RM2 PET may be complementary to 18F-FDG PET in ER-positive tumors with a low proliferation index.
Mattei et al. analyzed 238 lung cancer specimens, including both small and non–small cell lung cancer, and correlated the immunohistochemistry results with clinical stage, cell type, sex, and survival (53). GRPR expression was more abundant in advanced-stage disease, and a significant correlation was found between higher clinical stage and more intense GRPR expression. The overall GRPR expression between small cell lung cancer and non–small cell lung cancer was similar, but the intensity of the expression was higher in non–small cell lung cancer.
An immunohistochemistry study was performed by Carroll et al. on 50 human colon cancer specimens (54). Both GRP and GRPR were highly expressed in most cancers (62%), whereas no expression was detected in normal adjacent tissues. An interesting finding was that coexpression of the 2 proteins was seen always in well-differentiated tumors regions but was never observed in poorly differentiated tumor areas, suggesting a strong relation between GRP/GRPR expression and tumor differentiation.
A large number of other tumors overexpress GRPR on their cell surface, including head and neck cancer, renal cancer, and intestinal and bronchial carcinoids (43,55); however, aside from breast and prostate cancer, only few clinical studies are currently under way.
CLINICAL EVALUATION OF GRP AND GRPR IN PROSTATE CANCER
Diagnostic Studies
The use of GRP analogs in prostate cancer patients has increased recently. Various bombesin analogs have been labeled with different radioisotopes (64Cu, 18F, 68Ga). GRPR antagonists replaced agonists because of their more favorable pharmacokinetics; they block the receptor instead of activating it (as agonists do), resulting in no gastrointestinal side effects and increased binding (56,57).
Roivainen et al. reported the first-in-humans study of 68Ga-RM2 (58). Five healthy volunteers were included. The radiopharmaceutical was rapidly excreted via the urinary system and accumulated predominantly in the pancreas; acceptable radiation exposure (effective dose of 7.7 mSv for an injected dose of 150 MBq) was reported, with the urinary bladder wall and the pancreas being the organs with the highest absorbed doses (0.61 and 0.51 mSv/MBq, respectively). Similar results were reported for 2 other radiopharmaceuticals: 68Ga-RM26 (68Ga-1,4,7-triazacyclononane-N,N′,N″-triaceticacid-d-Phe-Gln-Trp-Ala-Val-Gly-His-Sta-Leu-NH2) and 68Ga-NODAGA-MJ9 (68Ga-NODAGA-4-amino-1-carboxymethyl-piperidine-d-Phe-Gln-Trp-Ala-Val-Gly-His-Sta-Leu-NH2) (59,60).
Kahkönen et al. analyzed 11 patients with prostate cancer who underwent 68Ga-RM2 PET/CT before surgery (61). The region-based PET accuracy across all patients was 83%, with a sensitivity and specificity of 89% and 81%, respectively. The authors reported a significantly higher SUVmax in tumor foci than in benign prostate hyperplasia and normal prostate tissue. Similar results were recently reported by Touijer et al. (41). Immunohistochemistry was performed to look for both GRPR and prostate-specific membrane antigen (PSMA) expression, since the latter is currently the target of the most used (but not yet Food and Drug Administration–approved in the United States) radiopharmaceuticals in the evaluation of prostate cancer. Immunohistochemistry showed no correlation between GRPR and PSMA expression, suggesting that they may provide complementary information. Fassbender et al. analyzed 15 patients with biopsy-proven prostate cancer and compared the PET scan performed before surgery with the histopathology results (62). Although 93% of the patients had at least 1 focus of pathologic 68Ga-RM2 uptake, the overall PET accuracy using the region-based visualization was rather low (63% across all patients). No significant correlations were found between region-based SUVmax and histopathology or between whole-prostate SUVmax and postoperative T category or International Society of Urological Pathology score.
Unpublished data from our group indicate a high detection rate of newly diagnosed prostate cancer using 68Ga-RM2 PET in 34 patients who underwent either surgery (n = 27) or radiotherapy (n = 7) after imaging. 68Ga-RM2 PET/CT showed intraprostatic cancer lesions in 33 patients (1 patient had a negative scan), which correlated with pathology in 27 patients who underwent prostatectomy. Increased uptake was identified in 4 pelvic lymph nodes, confirmed by pathology (n = 3) or follow-up imaging (n = 1). An example is shown in Figure 1.
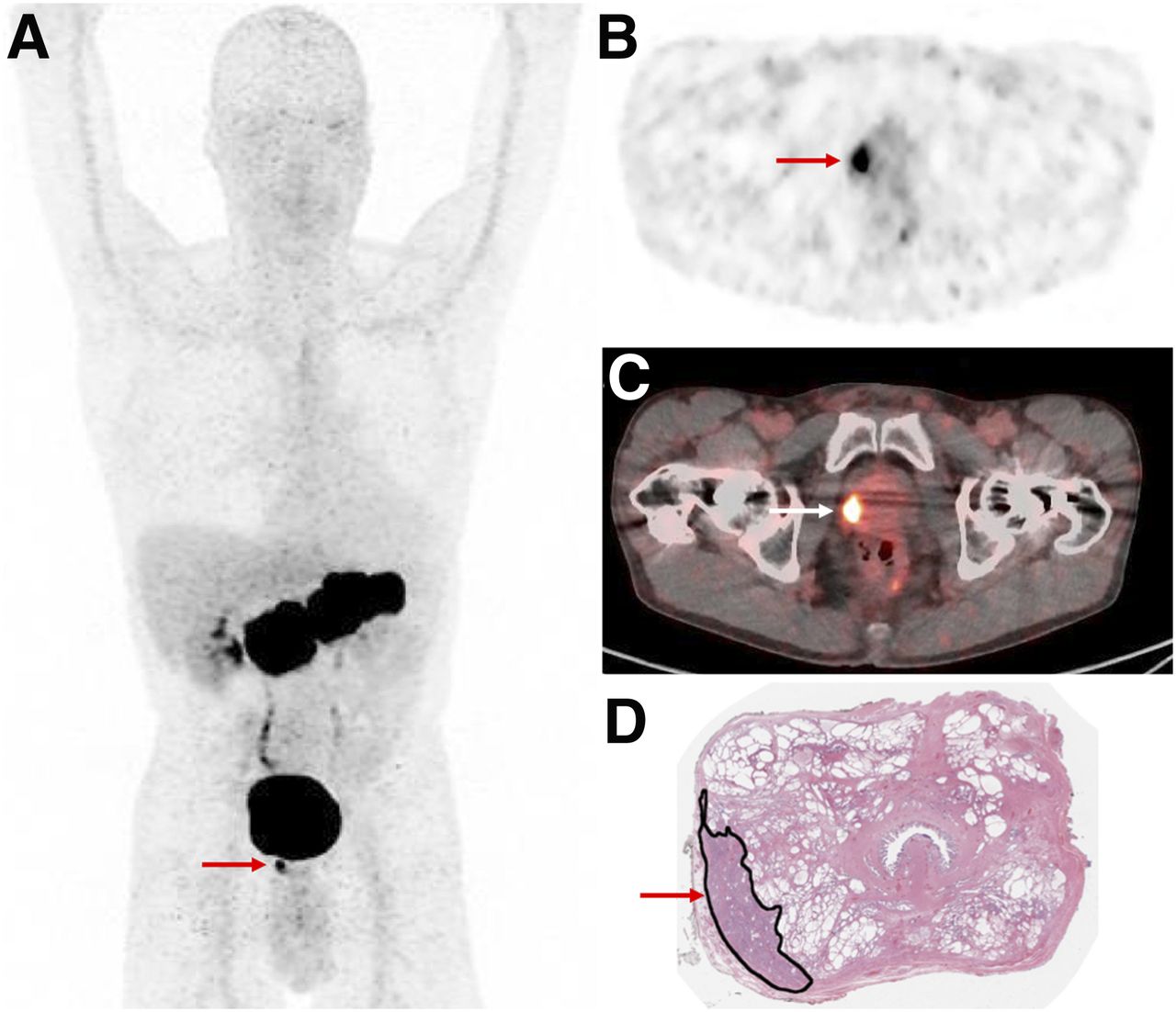
A 64-y-old man with newly diagnosed high-risk prostate cancer (PSA, 6.42 ng/mL). Intense focal 68Ga-RM2 uptake is seen in prostate gland (arrows) on maximum-intensity-projection (A), axial PET (B), and PET/CT (C) images, correlating with location of cancer marked in black ink on postprostatectomy histopathology slide (D).
68Ga-RM2 was evaluated more extensively at biochemical recurrence of prostate cancer. Our group published preliminary results from 32 prostate cancer patients who underwent 68Ga-RM2 PET/MRI at biochemical recurrence with negative conventional imaging (63). 68Ga-RM2 PET and MRI identified recurrent disease in 23 and 11 of these patients, respectively. PET was positive for all 11 patients with MRI pathologic findings. Our unpublished data from 114 participants enrolled to date indicate the following trend of 68Ga-RM2 PET positivity: 31.8% for a PSA level of less than 0.5 ng/dL (n = 22), 60% for a PSA level of 0.5–1.0 ng/dL (n = 15), 64.7% for a PSA level of 1.0–2.0 ng/dL (n = 17), 81.8% for a PSA level of 2.0–5.0 ng/dL (n = 22), and 87.2% for a PSA level of more than 5.0 ng/dL (n = 38) (64). An example is shown in Figure 2. Another study compared 68Ga-RM2 with 18F-fluoroethylcholine PET/CT in patients with biochemically recurrent PC (65). The authors retrospectively analyzed 16 men with biochemical relapse and negative or inconclusive 18F-fluoroethylcholine PET/CT results. Overall, 68Ga-RM2 PET/CT showed abnormal uptake in 10 of 16 patients (63%): for 2 patients with inconclusive results on 18F-fluoroethylcholine PET/CT, 68Ga-RM2 showed additional lymph nodes in the pelvis and multiple bone lesions. However, because the median PSA at the time of 18F-fluoroethylcholine PET/CT was lower than that at the time of 68Ga-RM2 PET/CT (2.4 vs. 5.5 ng/mL, respectively), further investigation in larger prospective clinical trials is needed to confirm these data.

A 72-y-old man with BCR prostate cancer (PSA, 0.72 ng/mL). (A, B, and D) Intense 68Ga-RM2 uptake is seen in right prostate bed (arrows) on early maximum-intensity-projection (A), axial PET (B), and PET/MR (D) images. (C) Corresponding axial T1-weighted MR image is also shown.
68Ga was used to label other GRPR-targeting peptides. The DOTA-conjugated GRPR antagonist SB3 (DOTA-paminomethylaniline-diglycolic acid-d-Phe-Gln-Trp-Ala-Val-Gly-His-Leu-NHEt) was tested on 17 patients with breast or prostate cancer (66). All patients had disseminated disease, and many had previous treatments, including hormonal therapies; a positive scan was registered in about 50% of cases. Data suggest that GRPR expression declines in advanced androgen-independent stages of prostate cancer, especially in osseous metastases (6,38). An optimized version, 68Ga-NeoBOMB1, was developed by replacement of the C-terminal Leu13-Met14-NH2 dipeptide of SB3 with Sta13-Leu14-NH2 (67). At 30 min after injection, more than 90% of 67Ga-NeoBOMB1 and 80% of 177Lu-NeoBOMB1 were found still intact in peripheral mouse blood, a characteristic that was pointed out by the authors as it makes an argument for use as theragnostic agents.
68Ga-RM26 is another GRPR antagonist with high affinity to GRP (59). The first-in-humans study included 28 patients with prostate cancer (17 newly diagnosed and 11 after therapy). 68Ga-RM26 PET/CT was positive in 15 of 17 patients at the initial diagnosis of PC (88.2%) and in 11 of 11 with biochemical recurrence. Twenty-two patients also underwent 68Ga-bombesin PET/CT, a GRPR agonist radiopharmaceutical. 68Ga-RM26 detected more primary tumors, lymph nodes, and bone metastases than did 68Ga-bombesin, further confirming the improved performance of antagonists over agonists.
64Cu- and 18F-labeled GRPR antagonists were also evaluated in small cohorts of prostate cancer patients. 64Cu-CB-TE2A-AR06 (64Cu-4,11-bis(carboxymethyl)-1,4,8,11-tetraazabicyclo(6.6.2)hexadecane)-PEG4-d-Phe-Gln-Trp-Ala-Val-Gly-His-Sta-LeuNH2) was assessed in 4 patients with newly diagnosed prostate cancer (68); favorable tumor uptake and image contrast were reported for the radiotracer. The longer half-life of 64Cu will allow for dosimetry applications before therapy using a GRPR antagonist. 18F-BAY 864367 (3-cyano-4-18F-fluorobenzoyl-Ala(SO3H)-Ala(SO3H)-Ava-Gln-Trp-Ala-Val-N-MeGly-His-Sta-Leu-NH2) was used in a first-in-humans study evaluating 10 patients with primary prostate cancer (n = 5) or recurrent disease (n = 5) (69). 18F-BAY 864367 PET/CT was compared with 18F-fluorocholine PET/CT and with histopathology when available. Among patients with primary prostate cancer 18F-BAY 864367 PET/CT detected 3 of 5 lesions; for the 2 negative scans, both 18F-fluorocholine PET/CT and histopathology confirmed the prostate lesions. Only 2 recurrent-disease lesions were detected by 18F-BAY 864367, whereas 18F-fluorocholine PET/CT identified suggestive lesions in all 5 patients.
Theragnostic Studies
The first-in-humans dosimetry study of a 177Lu-labeled GRPR antagonist was published by Kurth et al. (70). Four patients with metastatic castration-resistant prostate cancer received a mean dose of 4.48 GBq of 177Lu-RM2. The most intense physiologic uptake was seen in the pancreas, as expected from diagnostic studies (mean absorbed dose, 4.5 ± 1.6 Gy), but not so high as to prevent further administrations (71). For the bone marrow, the reported absorbed dose of 177Lu-RM2 was low and similar to what was previously described for PSMA ligand therapies (72,73), whereas for the kidneys the 177Lu-RM2 mean absorbed dose was lower than that for 177Lu-PSMA-617 (72) or 177Lu-DOTATATE (74). Bone metastases had the highest uptake, followed by lymph nodes and soft-tissue lesions. This study confirmed a high interpatient variability in terms of tumor uptake, a characteristic that had already been described (62) and implies that differences in tumor biology affect GRPR expression. Although these preliminary results are encouraging, further evaluations are needed.
Radiopharmaceuticals targeting GRPR are promising tracers for prostate cancer evaluation, showing a high detection rate for local and locoregional disease; they are accurate for the assessment of metastatic foci as well, although further evaluation is needed to understand the relation between GRPR expression and advanced hormone-resistant prostatic tumors. Compared with PSMA, whose high sensitivity and specificity in prostate cancer patients have been widely demonstrated (75–83), GRPR could play an important complementary role for PSMA-negative cancer and for tumors characterized by a heterogeneity of receptors expressed on their cell surface.
CLINICAL EVALUATION OF GRP AND GRPR IN BREAST CANCER
Although only a few pilot translational studies evaluating GRPR expression in breast cancer patients have been published so far, preliminary results seem to confirm what in vitro data already suggested: GRPR expression is strongly present in ER-positive tumors; furthermore, when the primary tumor is GRPR-positive, the lymph node metastases also show GRPR overexpression (51,52,66).
Stoykow et al. evaluated the performance of 68Ga-RM2 PET/CT in 15 patients with newly diagnosed breast cancer (84). Eighteen breast cancer lesions were known from core-needle biopsy (3 patients had bilateral lesions). 68Ga-RM2 PET/CT clearly detected 13 of these 18 lesions; the 5 PET false-negative results were tumors with an uptake level not distinguishable from normal breast tissue. However, in these cases, metastatic axillary lymph nodes were identified. All cancers seen on PET showed positivity for ER and PR expression; among the 5 cancers not detected by PET, only 1 was ER-positive, with an immunohistochemical ER expression of 30%. In the multivariate analysis, ER status was the primary predictor of 68Ga-RM2 uptake.
Another group studied breast cancer patients using 68Ga-RM26 PET/CT (85), which detected 29 tumors of 34 confirmed by histopathology. The 5 PET-negative tumors had un uptake that was lower than or equal to uptake by normal breast tissue. PET positivity correlated with ER status: 26 of 28 ER-positive primary cancers were also PET-positive. Histopathology confirmed the presence of lymph node metastases in 18 patients; PET was positive in lymph nodes for 15 of them. 68Ga-RM26 PET/CT missed metastases in 3 lymph nodes that were 1 mm in size. The SUVmax was significantly higher in ER-positive tumors than in ER-negative tumors and positively correlated with the expression level of GRPR. Uptake level was associated with menstrual cycle in both normal breast tissue and cancer (SUVmax was significantly higher during the secretory phase than in either the nonsecretory phase or the postmenopause phase); 4 of 5 PET-negative scans were performed on women during their secretory phase. The sensitivity, specificity, and accuracy of 68Ga-RM26 PET/CT increased either when ER-negative tumors were not considered or when patients who underwent the scan during their secretory phase were removed from the analysis.
An example from our own experience with 68Ga-RM2 PET/MRI in ER-positive breast cancer is shown in Figure 3. Supplemental Tables 1 and 2 summarize the clinical studies in prostate and breast cancer (supplemental materials are available at http://jnm.snmjournals.org).
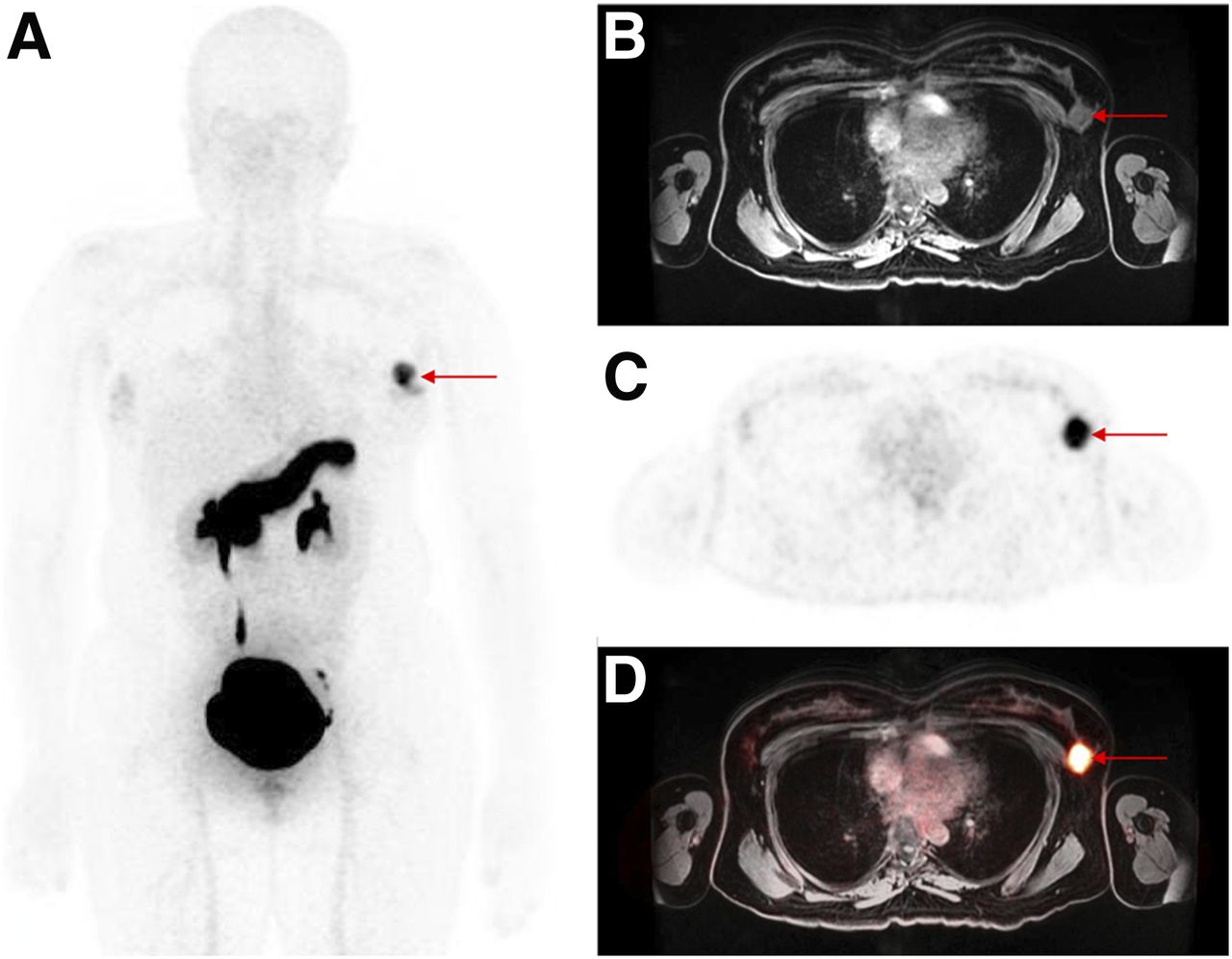
A 36-y-old woman with newly diagnosed ER-positive breast cancer. Intense 68Ga-RM2 uptake is seen in left breast (arrows) on maximum-intensity-projection (A), axial T1-weighted MR (B), axial PET (C), and PET/MR (D) images.
FUTURE DIRECTIONS
One area of development is to explore and understand the variability in GRPR expression in prostate cancer tumors in order to select the optimal imaging and therapy strategy for each patient. For tumors expressing GRPR, the detection rates for both the primary lesions and metastases are high. The well-known concept of intratumor heterogeneity (i.e., types of receptors expressed, receptor expression level, grade of malignancy, resistance to therapy) led to the development of bivalent prostate cancer–targeting peptides with the ability to target 2 receptors. In particular, heterodimers targeting both PSMA and GRPR have been evaluated (86,87). In addition, strategies to decrease physiologic uptake in the pancreas and to increase tumor uptake are being evaluated by various groups.
Another avenue for future use of GRPR antagonists is novel indications both in prostate cancer (biopsy guidance, evaluation or response to targeted local therapy) and in other cancers such as gastrointestinal and gynecologic malignancies. Although PSMA imaging and therapy are gaining significant traction at various stages of prostate cancer, GRPR antagonists are likely to play a complementary role. An example of 68Ga-RM2 and 68Ga-PSMA11 PET in the same patient showing 2 different primary prostate cancer lesions is presented in Figure 4.

A 54-y-old man with newly diagnosed intermediate-risk prostate cancer (PSA, 5.09 ng/mL). Focal 68Ga-RM2 uptake is seen in right prostate gland (arrow) on axial fused PET/CT and PET images (top row), whereas focal 68Ga-PSMA11 uptake is seen in left prostate gland (arrow) on axial PET/MR and PET images (bottom row). Both were prostate cancer on postprostatectomy histopathology.
Lastly, it seems clear that GRPR expression in breast cancer cells strongly correlates with ER-positive tumors. This correlation opens opportunities to expand the use of GRPR antagonists not only for diagnostic purposes but also for therapeutic purposes in this patient population.
CONCLUSION
Cancer imaging and therapy using peptide-based radiopharmaceuticals have ushered in a new era for nuclear medicine. Radiolabeled bombesin analogs are promising theragnostic agents for GRPR-expressing tumors, being able to detect primary tumors and metastatic lesions with high sensitivity and specificity. Larger prospective clinical trials are needed to improve understanding of the relation between the GRPR expression and biologic behavior of different cancer cells, in order to better select patients who will benefit from their use.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 14, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.
- 4.
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.
- 17.
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.
- 40.
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- Received for publication December 16, 2019.
- Accepted for publication February 6, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}