


Abstract
Preclinical models predict that blockade of the coinhibitory molecule cytotoxic T lymphocyte–associated antigen 4 (CTLA4) on lymphocytes results in the release of a cell cycle inhibitory checkpoint, allowing lymphocyte proliferation, tumor targeting, and regression. However, there is a paucity of data demonstrating that lymphocyte proliferation does occur in humans treated with CTLA4-blocking antibodies. Methods: We tested the role of whole-body molecular imaging in patients with advanced melanoma receiving the CTLA4-blocking antibody tremelimumab, allowing the analysis of changes in glucose metabolism using the PET probe 18F-FDG and cell replication with the PET probe 3′-deoxy-3′-18F-fluorothymidine (18F-FLT). Results: PET/CT scans obtained at a median of 2 mo after initial dosing did not demonstrate significant changes in lesion size or 18F-FDG or 18F-FLT uptake when focusing on metastatic lesions. Similarly, there was no difference in 18F-FDG uptake in the non–melanoma-involved spleen. However, there were significant increases in standardized uptake values for 18F-FLT in the spleen using post- and pretremelimumab treatment scans. Conclusion: Molecular imaging with the PET probe 18F-FLT allows mapping and noninvasive imaging of cell proliferation in secondary lymphoid organs after CTLA4 blockade in patients with metastatic melanoma.
The cytotoxic T lymphocyte–associated antigen 4 (CTLA4) is a coinhibitory activation–induced surface receptor on T cells that functions as a major negative regulator of anti–self-immune responses. It provides a dominant negative signaling to T cells on binding to the costimulatory molecules CD80 (B7.1) and CD86 (B7.2) expressed on the surface of antigen-presenting cells (1). Most naïve T cells do not express surface CTLA4 because of its binding to AP50, a subunit of the clathrin adaptor AP-2 protein (2). Once a T cell is activated through its T-cell receptor, downstream T-cell receptor signaling through Src kinases results in tyrosine phosphorylation of CTLA4 and the uncoupling of CTLA4 from AP50, allowing its surface expression, which peaks at 48 h after activation. Cell surface CTLA4 has 100–1,000 times higher affinity for the costimulatory molecules expressed by antigen-presenting cells, thereby efficiently competing with the positive costimulatory receptor CD28 (1). The engagement of CTLA4 by costimulatory molecules results in decreased T-cell receptor signaling, interleukin 2 transcription (3), and cell cycle arrest at the G1 stage, with the final result of inducing T-cell anergy (4,5). A clear example of the critical role of CTLA4 on tolerance is the striking phenotype of CTLA4 knock-out mice, which develop rapid T-cell proliferation and autoimmune infiltration of multiple organs shortly after birth (6,7).
Monoclonal antibodies blocking CTLA4 induce regression of immunogenic tumors in mice (8) and are being pursued as a treatment approach for patients with cancer. Two fully human antibodies with CTLA4-blocking activity—ipilimumab and tremelimumab—are in clinical development (9,10). The emerging clinical data suggest that a subset of patients with metastatic melanoma treated with CTLA4-blocking antibodies, in the range of 5%−15%, achieve durable objective tumor responses. However, clinically relevant toxicities, most often autoimmune or inflammatory, developed in a significant proportion of patients, in the range of 20%−30% (11–13).
There has been a great deal of interest shown in defining the mechanisms by which anti-CTLA4 antibodies induce tumor regressions in humans. Most of the studies have focused on analyzing T-cell activation in peripheral blood. Despite occasional cases of expansion of melanoma-specific T cells (14,15), the bulk of the data suggest that there is no detectable expansion of tumor antigen–specific lymphocytes, in particular when focusing on CD8+ T-cell responses. The most consistent effects in peripheral blood cells after administering anti-CTLA4 antibodies have been limited to marginal increases in the surface expression of nonspecific activation markers predominantly on CD4+ T lymphocytes (16–18). The picture is markedly different when analyzing changes inside tumors. Regressing metastatic lesions in patients that go on to achieve a durable objective tumor response are densely infiltrated by immune cells with a predominance of CD8+ T lymphocytes, whereas progressive lesions are not (19). It is currently unclear where these lymphocytes replicate and how they reach tumor lesions in some but not all patients, especially because there is no evidence of a quantitative increase of any lymphocytic subset in peripheral blood. It is also unclear if the failure of tumor lesions to respond in most patients is due to the lack of pharmacodynamic effects of anti-CTLA4 antibodies, for which in some patients the immune system may be activated in a different way from the patients with an objective response, and how this information may guide dose and schedule of CTLA4-blocking antibody administration.
Given these controversies, we reasoned that PET-based whole-body molecular imaging would allow the determination of changes induced by treatment with anti-CTLA4 antibodies, thereby providing information on the sites of immune cell activation and as a pharmacodynamic readout without invasive sampling. Given the known effects of CTLA4 blockade on T-cell activation and cell cycle progression derived from elegant studies in preclinical models (3–5,20), we used 2 PET tracers that provide a noninvasive readout of these events. The widely used PET tracer 18F-FDG, a glucose analog, provides information on metabolic changes on immune cell activation, because activated lymphocytes increase their glucose use, leading to increased accumulation of 18F-FDG at sites of inflammation (21). The less widely used PET tracer 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) provides a readout of nucleoside transporter and thymidine kinase 1 activity that is correlated with cell proliferation (22). Our results demonstrate that 18F-FLT PET allows the visualization of how cells in the spleen, the largest secondary lymphoid organ, proliferate on treatment with the anti-CTLA4 antibody tremelimumab in patients with metastatic melanoma, regardless of demonstrating an objective and durable tumor response after CTLA4 blockade.
MATERIALS AND METHODS
Description of Clinical Trial
Twelve patients treated at UCLA within an investigator-initiated research protocol (UCLA Institutional Review Board no. 06-06-093, Investigational New Drug no. 100453, Trial Registration no. NCT00471887) that administered the anti-CTLA4-blocking antibody tremelimumab (Pfizer) consented to be enrolled in a study cohort with pre- and postdosing research PET scans. All patients received tremelimumab as a single agent administered at 15 mg/kg every 3 mo. Objective clinical responses were recorded as the best overall response on therapy following a slight modification of the Response Evaluation Criteria in Solid Tumors (RECIST) (23). Response assessment was based on diagnostic CT scans obtained at 3-mo intervals throughout the study and compared with the baseline diagnostic CT scans. The RECIST modification was defined prospectively in the protocol and allowed the measurement of target disease lesions in the skin and subcutaneous lesions not detected using imaging examinations but evaluable by physical examination and adequately recorded using a camera with a measuring tape or ruler. There was no minimum size limit to define these lesions as measurable. Adverse events attributed to tremelimumab by the study investigators were graded according to the National Cancer Institute common toxicity criteria, version 2.0 (24).
Performance of Research PET Scans
The performance of research PET/CT with both 18F-FDG and 18F-FLT was approved by the local Medical Radiation Safety Committee and for 18F-FLT by the Radioactive Drug Research Committee of the Food and Drug Administration. Patients were imaged with 18F-FDG and 18F-FLT both before and after the initiation of therapy. The time interval between the 2 scans was at least 24 h (>12 physical half-lives). Thus, cross contamination of data from radioactivity from the first to the second scan was ruled out. The follow-up research PET/CT scans were planned between study days 30 and 60, but given practical considerations of PET tracer availability and patient scheduling, the study protocol allowed up to 1 mo variation from this period for the follow-up scans. For research PET/CT scans, a low-dose whole-body non–contrast-enhanced CT scan was acquired first and used for lesion localization and attenuation correction (25). The following parameters were used: 130 kVp, 120 mA, 1-s tube rotation, 4-mm slice collimation, and bed speed of 8 mm/s (i.e., a pitch of 2).
PET/CT studies were performed using either a Siemens Biograph Duo or a Siemens Biograph 64 with a 64-detector helical CT system (both from Siemens AG). PET images were acquired 45–60 min after the intravenous injection of 18F-FDG given at 7.77 MBq/kg (0.21 mCi/kg) following the standard clinical protocol, accepting dose deviations of ±10%. Administered 18F-FLT doses were always within 10% of 196.1 MBq (5.3 mCi) as stipulated by the UCLA Medical Radiation Safety Committee and the Radioactive Drug Research Committee. Scans were obtained with the patient in the arms-up position. PET duration was dependent on patient weight (26). Baseline and follow-up PET/CT studies were analyzed quantitatively by measuring the maximal standardized uptake values (SUVmax) of all visualized cancer lesions and nonaffected lymphoid organs. The single maximum pixel value within the 1 slice with the highest radioactivity concentration was detected (SUVmax). In addition, mean organ SUV (SUVmean) was recorded for the spleen. The mean tracer uptake of the entire organ volume was defined in addition to the maximum organ tracer uptake, to avoid data contamination due to heterogeneous tracer uptake within the spleen. Two correction approaches were used. First, the organ borders were manually delineated on consecutive axial slices of the baseline and follow-up CT images. Then, the mean and maximum tracer uptake within this volume of interest were defined using a Mirada workstation (REVEALMVS; CTI Mirada Solutions). Treatment responses were prospectively defined as being significant if 18F-FDG or 18F-FLT SUV decreased by 25% or more (27).
Tremelimumab
Tremelimumab (compound code CP-675,206) is a fully human IgG2 monoclonal antibody with high binding affinity for human CTLA4 and a plasma half-life of 22.1 d (10,28). It was supplied by Pfizer Inc. as a liquid solution in vials containing 50 mg at 5 mg/mL. Vials were mixed in sodium chloride 0.9%, and the amount of antibody to be administered was calculated. The dose of 15 mg/kg is known to result in plasma levels of tremelimumab beyond 30 μg/mL for 2–3 mo in humans (28), which correlates with the in vitro concentrations required to have a biologic effect of CTLA4 blockade (10).
Statistical Analysis
The pre- and posttreatment SUVmax and SUVmean were analyzed using a 2-sided Student paired t test (GraphPad Software, Inc.). For all statistical analysis, the P value was set at less than 0.05.
RESULTS
Patient Characteristics, Response, and Toxicity
Twelve patients with advanced melanoma were enrolled in a clinical trial administering the human anti-CTLA4 antibody tremelimumab and consented to also undergo 18F-FDG and 18F-FLT PET scans before and after the study drug administration. Two of these patients did not undergo the planned postdosing scans because of withdrawal of consent on early disease progression. Table 1 describes the 10 remaining patients (2 women, 8 men; age range, 27–81 y), who underwent at least 1 posttreatment PET scan, including 1 patient who did not undergo the posttreatment 18F-FDG PET scan and another patient who did not undergo the posttreatment 18F-FLT PET scan. Six patients had M1c metastatic melanoma (visceral metastasis or high lactate dehydrogenase), 2 had lung metastasis but no other visceral organ metastasis (M1b), and 2 had in-transit melanoma (stage IIIc). These 2 patients with stage IIIc had an objective tumor response, resulting in ongoing tumor regressions. We recorded treatment-related toxicities during the first 3 mo of therapy, because all postdosing scans were obtained within this period. There were 3 patients with toxicities beyond grade 1 attributed to the study drug; 2 of the toxicities were in patients without a response and 1 was in a patient with a response (Table 1). None of these patients received corticosteroids, or any other form of immune suppressive therapy, before the posttreatment PET scans were obtained.
Patient Characteristics and Timing of PET Scans
PET Scan Performance
Posttreatment 18F-FLT scans were acquired at a median of 61 d (range, 43–98 d) and posttreatment 18F-FDG scans at a median of 57 d (range, 36–99 d) from treatment. Because of the limited availability of 18F-FLT and difficulty in patient scheduling, 1 patient (GA 33) underwent the posttreatment scans 9 d beyond the initially planned period (Table 1). This patient traveled far and the postdosing 18F-FLT PET could not be performed until the day before the patient returned for the second administration of tremelimumab.
Evaluation of CT Scans for Tumor Sizes
The postdosing 18F-FDG PET/CT studies were compared with the baseline scans, and the size of all detectable lesions representing measurable metastatic melanoma was recorded. Among the 2 patients who went on to achieve an objective and durable response to therapy, both qualified as having stable disease by RECIST at this early time point, with minimum fluctuations in the sum of maximum diameters. Among the other 8 patients, all of whom went onto have clear disease progression at 3 mo or later on the basis of standard restaging CT scans, only 3 had evidence of disease progression by RECIST at this time point. Among the 5 remaining patients, 1 qualified for a partial response with a 64% regression in the sum of diameters of 2 lymph node metastasis, and 3 other patients had decreases in tumor sizes (24%, 17%, and 12% decrease in the sum of maximum diameters), which did not qualify for a partial response. We pooled all the individual tumor size data and compared the lesion size before and after the administration of tremelimumab using a paired t test that demonstrated a lack of significant change in tumor sizes at this early time point (Supplemental Fig. 1A; supplemental materials are available online only at http://jnm.snmjournals.org).
Evaluation of 18F-FDG and 18F-FLT Scans at Tumor Sites
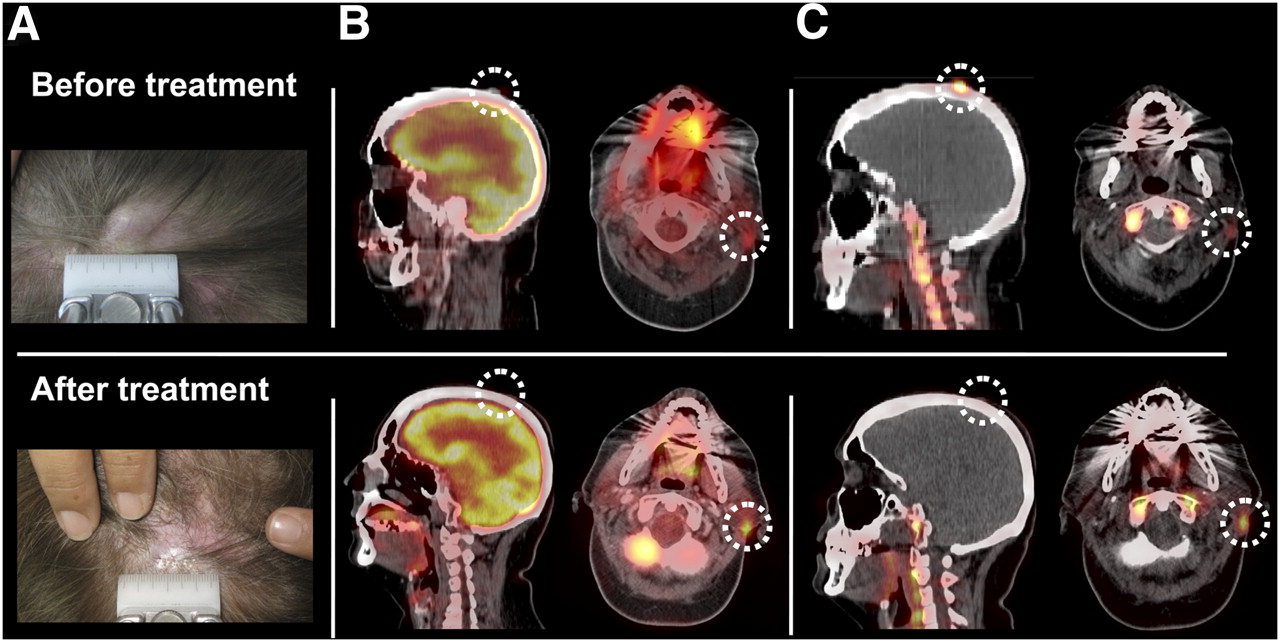
Pre- and posttremelimumab tumor SUVs did not differ significantly for 18F-FDG or 18F-FLT by paired t test analysis (Supplemental Figs. 1B and 1C, and scan image examples in Supplemental Fig. 2). The 2 lesions with the highest starting SUVmax for 18F-FDG decreased significantly according to the prospective criteria for SUVmax changes defined in the protocol. Both decreases were in patients who had disease progression to therapy at the 3-mo restaging diagnostic CT scans, demonstrated by the appearance of several new metastases. These included a large subclavicular mass in patient GA 24, which had decreased in size by 12% by CT scan criteria and decreased in 18F-FDG SUVmax by 31%, and a large lung mass in patient GA 23, which had increased in size by 27% by CT criteria and decreased in 18F-FDG PET SUVmax by 25%. The largest decrease in SUVmax for 18F-FLT was a completely regressed scalp lesion in patient GA 33. However, an auricular lesion in this same patient increased in 18F-FLT SUVmax by 184% at the same time point (Fig. 1).

18F-FDG and 18F-FLT PET/CT scans in patient with metastatic melanoma with objective tumor response to tremelimumab. Images are from patient GA 33, who had complete response to tremelimumab. Initial sites of disease were 3 scalp skin metastases, 1 of them 1.5 cm in size by physical examination, and enlarged right neck lymph node. (A) Pictures of largest scalp metastasis. (B) Fused 18F-FDG PET/CT scans. (C) Fused 18F-FLT PET/CT scans. Top row are pretreatment images, and bottom row are posttremelimumab images.
Evaluation of 18F-FDG and 18F-FLT Scans in Spleen
A major goal of this research was to determine whether PET scans would be able to detect metabolic changes induced by treatment with tremelimumab in secondary lymphoid organs. Therefore, we quantified changes in SUV in the spleen, which is the largest lymphoid organ in humans. For the spleen measurements, we recorded both the SUVmean and the change in SUV for the pixel with the highest tracer concentration (SUVmax). Overall, maximum splenic uptake of 18F-FDG at baseline was low, with most SUVmax in the range of 2–4, which was lower than the SUVmax of melanoma metastasis. There was no significant change between SUVs for 18F-FDG before and after treatment, quantifying either the SUVmean or SUVmax splenic organ uptake (Figs. 2A and 2B). Spleen SUVs for 18F-FLT were equally low at baseline, but there was a statistically significant increase after the administration of tremelimumab for both spleen SUVmean (Fig. 2C) and spleen SUVmax (Fig. 2D). In 5 patients, this increase was beyond the SUV change prospectively defined as a positive change, with increases of between 31% and 91% in the spleen SUVmean (see examples from patients GA 24 and GA 33, Fig. 3). In 4 other patients, changes in spleen SUVmean were in the range of −1.5% to 11%. One patient had a concordant decrease in SUVs, both when measured as SUVmax (−7%) and when measured as SUVmean (−1%). This is the patient presented in Supplemental Figure 2 with a bulky metastatic melanoma who had previously received several rounds of cytotoxic therapy. This patient had rapid disease progression. Interestingly, patient GA 29, who went on to a durable complete response to therapy, had marginal changes in 18F-FLT uptake, with a decrease of −1.5% when measured as SUVmax and a 3.9% increase in SUVmean. Two of the patients with grade 2 or 3 toxicities during the first 3 mo of therapy also clustered in this group, with lower 18F-FLT changes.
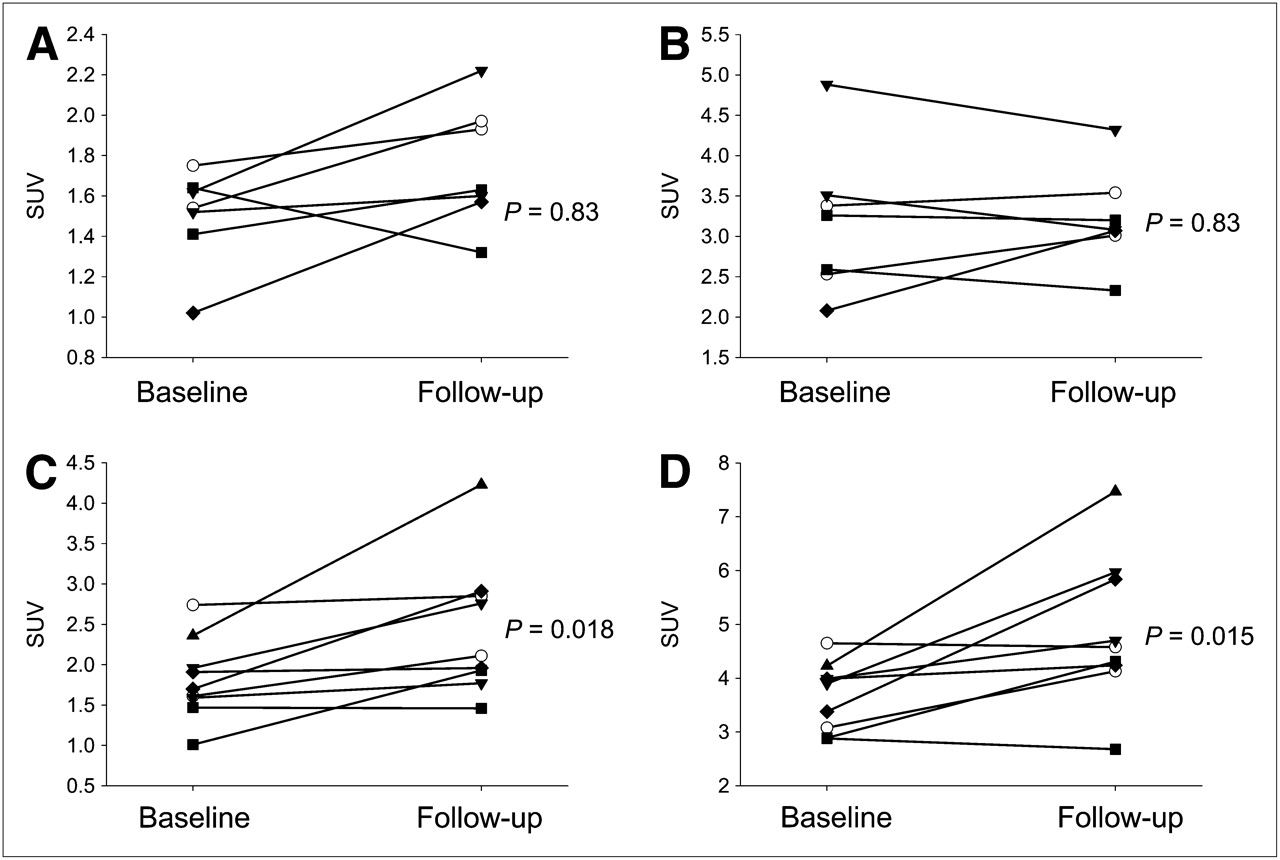
Analysis of SUV for 18F-FDG and 18F-FLT PET scans in spleen. (A and B) Changes in SUV for 18F-FDG in spleen by PET scans, as SUVmean (A) or SUVmax (B). (C and D) Changes in SUV for 18F-FLT in spleen by PET scans, as SUVmean (C) or SUVmax (D). In all plots, open symbols represent values from 2 patients with objective response, and filled symbols represent values from patients without objective response at formal restaging studies. P values reflect paired t test analysis.
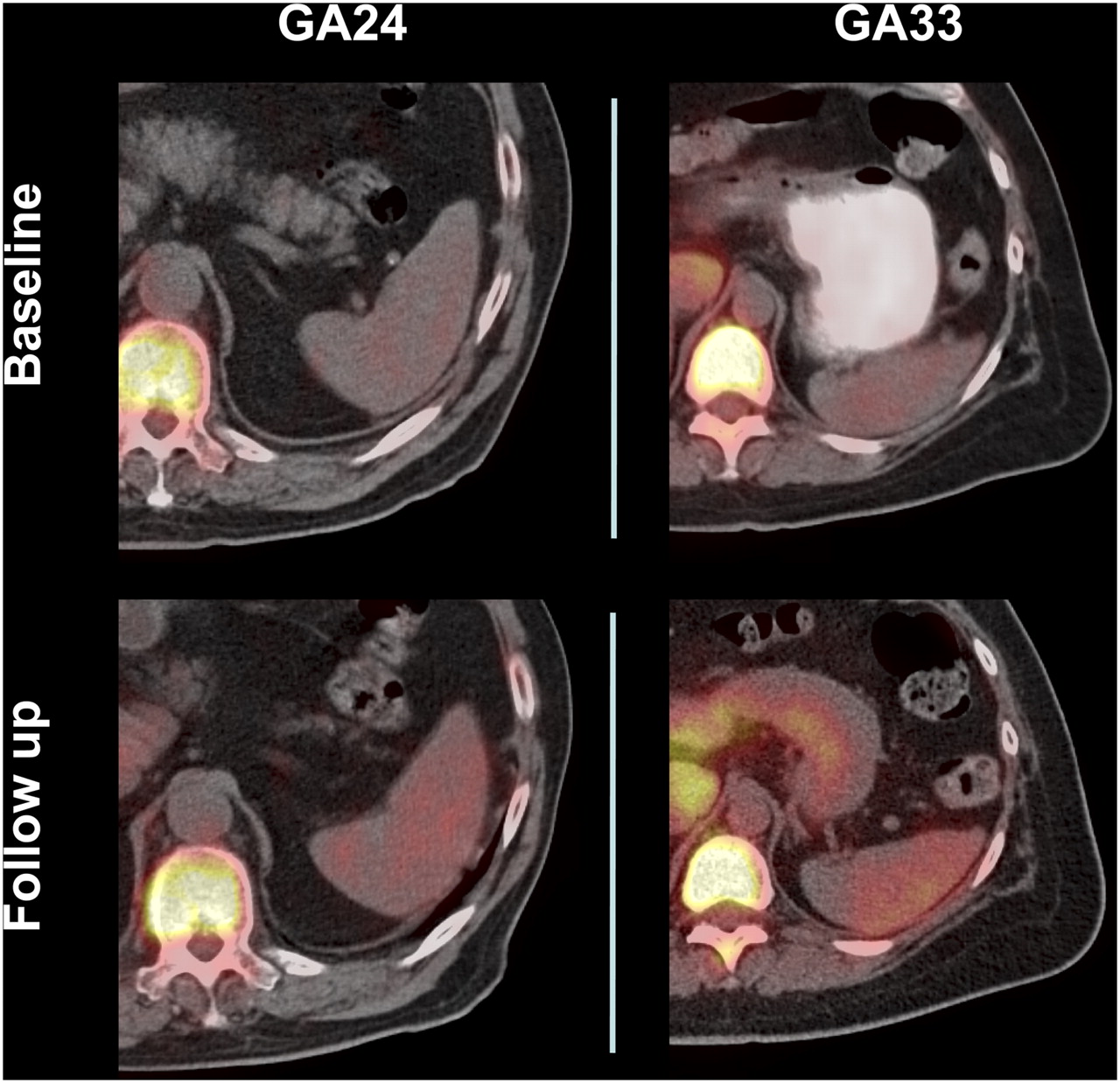
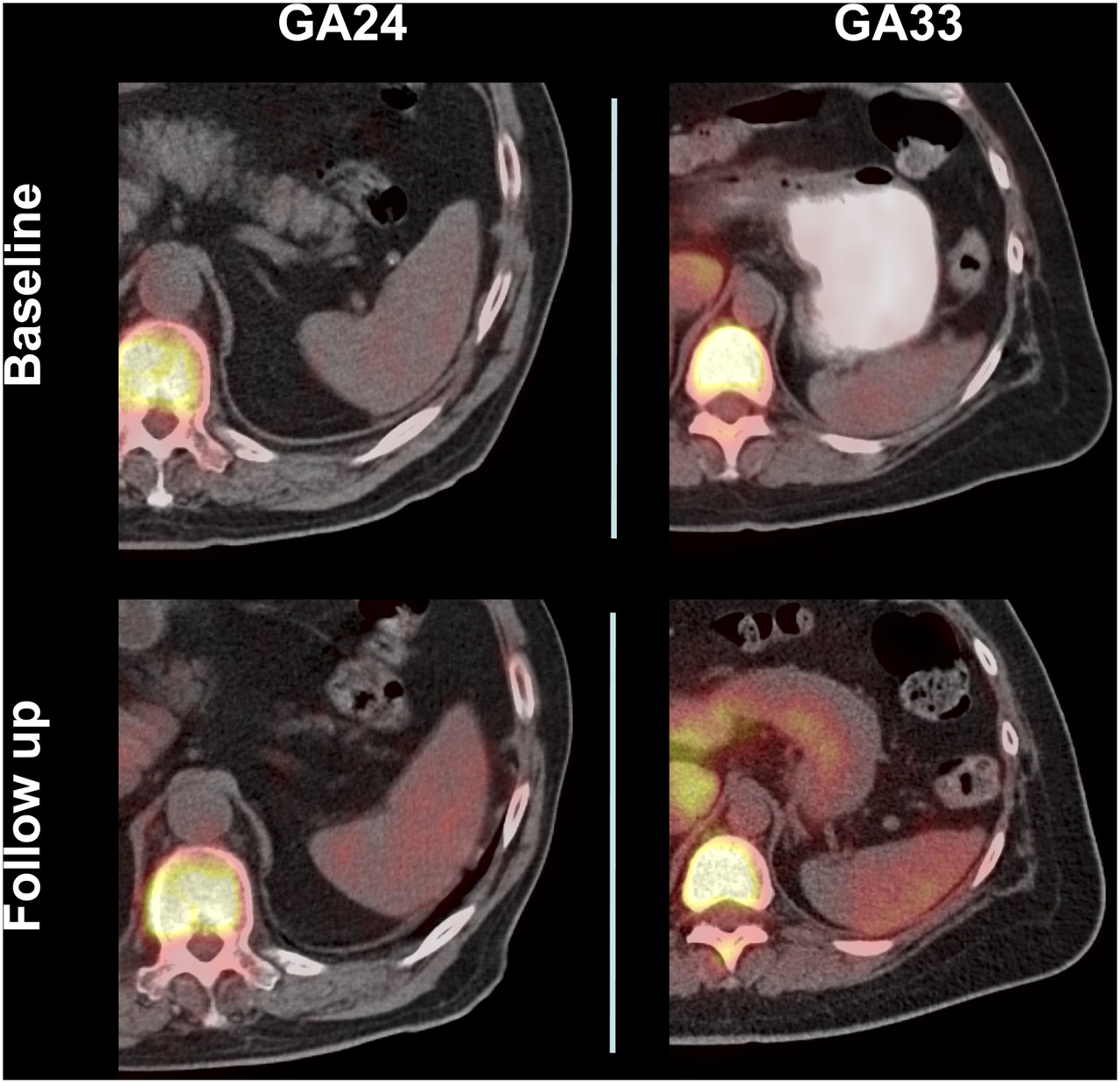
Representative 18F-FLT PET images of cell proliferation in spleen. Fused CT and 18F-FLT PET scans are from patient GA 24, who had disease progression (left column), and patient GA 33, who had durable disease regression (right column).
DISCUSSION
These studies were undertaken to explore how the anti-CTLA4 antibody tremelimumab affects the host immune system and tumors using noninvasive molecular imaging. Our data suggest that the evaluation of CT scans by size criteria and 18F-FDG and 18F-FLT PET scans focusing on the SUVmax of metastatic melanoma lesions within 3 mo of initial dosing with tremelimumab were unreliable in predicting later treatment responses and patient outcome. However, an analysis focusing on spleen images in 18F-FLT PET scans allowed the detection of an effect of tremelimumab on splenic cell proliferation in humans consistent with the anticipated pharmacodynamic effect of CTLA4-blocking monoclonal antibodies. It has long been demonstrated in preclinical models that ligation of CTLA4 by B7 costimulatory molecules prevents T-cell cycle progression at the G1 to S transition (4,5), which is particularly evident in CD4 cells on secondary antigen exposure. Therefore, we had anticipated that blocking this negative signaling would release the CTLA4 checkpoint on cell cycle in lymphocytes, resulting in increased 18F-FLT uptake in lymphoid organs such as the spleen.
However, release of the CTLA4 checkpoint on T-cell proliferation with the administration of monoclonal antibodies to patients with cancer had been difficult to demonstrate in prior studies based on the analyzing of immune cells ex vivo. Overall, quantitative immune monitoring assays failed to detect expansions of antigen-specific T cells, either to tumor or to infectious disease antigens (16,18), although T-cell expansions to melanoma antigens can be detected in occasional patients (14,15). On the contrary, biopsies of regressing tumor lesions demonstrate that CD8 and CD4 T-cell proliferation is likely to have occurred, because regressing lesions after therapeutic CTLA4 blockade have dense intratumoral infiltrates by these 2 cell subsets; no such infiltrates were noted in biopsies of progressing tumors (19). These tumor biopsy data had suggested that the release of the CTLA4 proliferative checkpoint may happen only in patients who go on to have a durable objective response after the administration of tremelimumab. T-cell proliferation may occur inside tumors or at distant lymphoid organs (lymph nodes and spleen), leading to accumulation in tumors. However, because anti-CTLA4 antibodies are a mode of nonspecific immunotherapy, we could not rule out the alternative possibility that T-cell proliferation would occur in all patients at a site different from the tumor or the peripheral blood but that only patients who go on to have an objective response to therapy would accumulate these cells inside tumors. To study these 2 possibilities, we reasoned that whole-body molecular imaging in humans receiving therapeutic doses of the anti-CTLA4 antibody tremelimumab would allow the study of cell cycle progression of lymphocytes in their natural environment and better define how the immune system of patients with metastatic melanoma responds to therapy with CTLA4-blocking monoclonal antibodies.
In the current experience, most posttreatment scans were obtained between 1 and 2 mo after the initial dose of tremelimumab, a time that may be too early to detect objective responses to immunotherapy. In fact, in a prior study with tremelimumab the median time to first detection of a tumor response by CT scans was 5 mo (13). The main goal of the PET scans in the current study was not to detect tumor responses but to be a potential readout for immune activation, the desired pharmacodynamic effect of tremelimumab. Therefore, we were not surprised that CT size criteria were not able to differentiate between the 2 patients who went on to have a complete, durable response the 8 patients with disease progression. The posttreatment scans were obtained later than planned (3 mo) in 1 of the 2 patients who went on to have an objective response to therapy (GA 33) because of patient scheduling issues. By physical examination and CT size criteria, there was evidence of a complete regression of scalp metastasis, but a neck node appeared enlarged at that time point. The neck node lesion had a marked increase in both 18F-FDG and 18F-FLT uptake at the postdosing examination. The next restaging scans performed at 6 mo after initiating therapy demonstrated that the neck node had completely regressed. No biopsy was done at the peak of 18F-FDG and 18F-FLT uptake, so we cannot assess if the increase in PET tracer uptake at 3 mo was mainly due to melanoma or an inflammatory response, a common event in regressing lesions analyzed by tumor biopsies (19). In 2 other patients, there was a decrease in 18F-FDG and 18F-FLT uptake in large tumor lesions at the research PET scans, but both patients went on to have evidence of disease progression at the 3-mo diagnostic CT scans following RECIST criteria, both with the appearance of new metastatic sites. These findings demonstrate partial necrosis of large tumor lesions that overgrew their blood supply, as opposed to isolated and temporary responses to tremelimumab.
Contrary to our expectations, when comparing patients without diarrhea with the 2 patients who had grade 2 or 3 diarrhea (a common toxicity with CTLA4-blocking antibodies) during the first 3 mo after dosing, we did not detect differences in 18F-FDG or 18F-FLT uptake in the gastrointestinal tract. Our data suggest that the ability of these scans to detect inflammatory responses due to tremelimumab may be limited, despite a well-documented case of increased 18F-FDG in the large bowel in a patient who underwent PET/CT at the time of having major colitis after tremelimumab administration (29). It is likely that the timing of scans related to the initiation of symptoms may result in different uptake of PET tracers. We also attempted to analyze SUV changes for these 2 PET tracers in tumor-draining lymph nodes. However, this approach proved to be challenging because it is difficult to correctly assess the nodes draining systemic metastatic deposits and because their size and PET tracer uptake were deemed too low and variable to provide interpretable results. The major finding of the current work is the clear evidence of the release of the cell cycle checkpoint in spleen cells with the administration of the anti-CTLA4 antibody tremelimumab using 18F-FLT PET scans. Given the sensitivity of PET scans, this effect was evident in the largest secondary lymphoid organ, the spleen. We cannot rule out that a similar effect may be happening in tumor-draining or other lymph nodes, which are usually less than 1 cm in diameter and below the sensitivity of clinical PET scans. The increased uptake of 18F-FLT in spleen was equally evident in patients with or without an objective response to therapy or with clinically significant autoimmune or inflammatory toxicities.
CONCLUSION
The frequent increase in 18F-FLT uptake in the spleen after CTLA4 blockade with tremelimumab suggests that this agent has a similar pharmacodynamic effect on lymphoid cell activation in most patients. However, 2 of 9 patients had decreases in 18F-FLT SUVs in the spleen, which may reflect a variable responsiveness to this antibody in a subset of patients. Tremelimumab at 15 mg/kg administered every 3 mo releases the CTLA4 cell cycle checkpoint in most patients as evidenced by the increased uptake of 18F-FLT, a PET tracer that allows the noninvasive imaging of immune cell replication, in the spleen after dosing.
Acknowledgments
We thank Narsis Attar for assistance in data analysis and John A. Glaspy for patient referrals. The clinical trial conduct and the performance of PET/CT scans were supported by clinical research funds from Pfizer Inc. A portion of the study was supported by the National Institutes of Health award P50 CA086306, the California Institute for Regenerative Medicine New Faculty Award 2-00902-1, and the Jonsson Cancer Center Foundation.
Footnotes
-
Guest Editor: Steve Larson, Memorial Sloan-Kettering Cancer Center
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 20, 2009.
- Accepted for publication December 3, 2009.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging cellular immunotherapies and immune cell biomarkers: from preclinical studies to patients
- MRI techniques for immunotherapy monitoring
- 18F-FLT PET/CT as a Prognostic Imaging Biomarker of Disease-Specific Survival in Patients with Primary Soft-Tissue Sarcoma
- STING-driven interferon signaling triggers metabolic alterations in pancreas cancer cells visualized by [18F]FLT PET imaging
- Predictive value of 3'-deoxy-3'-18F-fluorothymidine PET in the early response to anti-programmed death-1 therapy in patients with advanced non-small cell lung cancer
- Imaging of T-cell Responses in the Context of Cancer Immunotherapy
- Imaging the Cancer Immune Environment and Its Response to Pharmacologic Intervention, Part 2: The Role of Novel PET Agents
- FLT PET/CT imaging of metastatic prostate cancer patients treated with pTVG-HP DNA vaccine and pembrolizumab
- The Immunoimaging Toolbox
- Immune Modulation Therapy and Imaging: Workshop Report
- Prediction of Response to Immune Checkpoint Inhibitor Therapy Using Early-Time-Point 18F-FDG PET/CT Imaging in Patients with Advanced Melanoma
- Immuno-PET of Murine T Cell Reconstitution Postadoptive Stem Cell Transplantation Using Anti-CD4 and Anti-CD8 Cys-Diabodies
- Immune Checkpoint Blockade in Cancer Therapy
- CTLA4 Blockade Broadens the Peripheral T-Cell Receptor Repertoire
- Engineered antibody fragments for immuno-PET imaging of endogenous CD8+ T cells in vivo
- PET imaging to non-invasively study immune activation leading to antitumor responses with a 4-1BB agonistic antibody
- PET Imaging of Proliferation with Pyrimidines
- CTLA4 Blockade Induces Frequent Tumor Infiltration by Activated Lymphocytes Regardless of Clinical Responses in Humans