


Abstract
The activation of the renin–angiotensin–aldosterone system prevents the uptake of norepinephrine in the myocardium. However, the additive effects of combined spironolactone and candesartan on cardiac sympathetic nerve activity (CSNA) have not been determined. We investigated the effects of the angiotensin-receptor blocker candesartan alone and in combination with spironolactone on CSNA in patients with congestive heart failure (CHF). Methods: Fifty patients with CHF (left ventricular ejection fraction [LVEF] < 45%) were randomly assigned to candesartan plus spironolactone (group A; n = 25) or to candesartan alone (group B; n = 25). All patients were also treated with a loop diuretic. The delayed percent denervation, delayed heart-to-mediastinum count (H/M) ratio, and washout rate (WR) were determined from 123I-metaiodobenzylguanidine (MIBG) scintigraphy, and plasma brain natriuretic peptide (BNP) concentration was measured before and 6 mo after treatment. The LV end-diastolic volume (LVEDV), LV end-systolic volume (LVESV), and LVEF were also determined by echocardiography. Results: After 6 mo, all of these parameters were improved in both groups. However, the degree of change in the percent denervation was −14 ± 12 in group A and −7 ± 10 in group B (P < 0.05); the change in the H/M ratio was 0.19 ± 0.18 in group A and 0.08 ± 0.14 in group B (P < 0.05), the change in WR was −12% ± 8% in group A and −5% ± 13% in group B (P < 0.05), and the change in plasma BNP was −100 ± 83 pg/mL in group A and −43 ± 97 pg/mL in group B (P < 0.05). The degree of change in LVEDV, LVESV, and LVEF in group A tended to be better than that in group B, but these changes were not statistically significant. Moreover, there were significant correlations between changes in the 123I-MIBG scintigraphic findings and changes in the LVEDV (% denervation, r = 0.692, P < 0.001; H/M ratio, r = −0.437, P < 0.05; and WR, r = 0.505, P < 0.01) or the LVESV (% denervation, r = 0.663, P < 0.001; H/M ratio, r = −0.438, P < 0.05; and WR, r = 0.532, P < 0.01) in group A. In contrast, there was no relationship between these parameters in group B. Conclusion: These findings indicate that the combination of spironolactone and candesartan may be more beneficial for CSNA and LV performance than candesartan alone in patients with CHF.
One of the most important physiologic systems involved in the development and progression of congestive heart failure (CHF) is the renin–angiotensin–aldosterone system (RAAS). Aldosterone independently promotes potassium and magnesium loss, sodium retention, ventricular arrhythmias in humans, and, as shown in animal models, cardiac and vascular fibrosis as well as vascular necrosis (1,2). These effects are mediated by the action of aldosterone on mineralocorticoid receptors in the kidney, brain, heart, and vasculature (3). The angiotensin-receptor blocker (ARB) candesartan targets the renin–angiotensin elements of RAAS, and this agent improves the quality of life and decreases the mortality and morbidity in patients with CHF (4). However, despite ARB treatment, there is still production of aldosterone, a phenomenon known as aldosterone escape or aldosterone breakthrough (1).
Cardiac imaging with 123I-metaiodobenzylguanidine (MIBG), an analog of norepinephrine, is a useful tool for detecting abnormalities of the myocardial adrenergic nervous system in patients with CHF (5,6). Furthermore, cardiac sympathetic nerve activity (CSNA) evaluated by 123I-MIBG scintigraphy has useful prognostic value in patients with CHF (6,7). Many studies have suggested that treatment of heart failure in patients with CHF can improve CSNA, as evaluated by cardiac 123I-MIBG scintigraphy (8–19). However, the additive effects of combined spironolactone and candesartan on CSNA have not been determined. Accordingly, this study was performed to determine whether the combination of spironolactone and candesartan can improve CSNA compared with candesartan alone in patients with CHF.
MATERIALS AND METHODS
Study Population
The study included 50 patients with heart failure (left ventricular ejection fraction [LVEF] < 45% and New York Heart Association [NYHA] functional class III or IV), who were admitted to our institution and whose symptoms had improved to NYHA functional class II or III within 1 mo with standard therapy for CHF. Patients with severe heart failure requiring mechanical support (intraaortic balloon pumping, LV assist device, cardiac resynchronization therapy, or implantable cardioverter-defibrillator) or patients requiring heart transplantation were excluded. Patients with unstable angina pectoris, renal failure, liver dysfunction, cardiogenic shock, or hypotension defined as a systolic blood pressure < 90 mm Hg were also excluded. The study was approved by the ethics review board of Cardiovascular Hospital of Central Japan, and written informed consent was obtained from all patients.
Study Protocol
In the acute phase, all patients were treated with standard therapy for heart failure, including intravenously administered vasodilators and diuretics. All patients also received oral angiotensin-converting enzyme (ACE) inhibitor and loop diuretic (furosemide). When the patient was compensated with oral medications alone for at least 2 wk, 50 patients were randomly assigned (double-blind, 1:1 ratio) to either candesartan plus spironolactone (group A; n = 25) or candesartan alone (group B; n = 25) instead of an ACE inhibitor. Candesartan was started at a dose of 2–4 mg/d in all patients, and the dose was gradually increased to a maximum of 8–12 mg/d. In group A, spironolactone was also started at a dose of 25 mg/d at the same time. In this study, the β-blocker carvedilol was not started for all CHF patients. In both group A and group B, carvediol was added to the study medications in the patients who needed to stabilize the symptoms of heart failure. This agent was finally administered to 36 of 50 patients (group A, n = 17 [68%]; group B, n = 19 [76%]). Carvedilol was started at a dose of 1.25–2.5 mg/d in these patients, and the dose was gradually increased to a maximum of 10–20 mg/d. Examinations were performed before and after candesartan and spironolactone treatment for a mean of 6 mo in all CHF patients.
Echocardiography
Echocardiography was performed using standard methods in a blinded manner: 2 experienced, independent echocardiographers who had no knowledge about the study performed all measurements. The LV end-diastolic volume (LVEDV), LV end-systolic volume (LVESV), and LVEF were calculated using the modified method of Simpson (20).
123I-MIBG Imaging
The 123I-MIBG imaging method has been described previously (21–23). 123I-MIBG was obtained from a commercial source (FUJIFILM RI Pharma Co. Ltd.). Patients were injected 123I-MIBG (111 MBq) intravenously while in the supine position. At 15 min and at 4 h after the injection, static data were acquired in the anterior view with a single-head γ-camera (Millennium MPR; GE Healthcare) equipped with a low-energy, general-purpose, parallel-hole collimator. Static images on a 128 × 128 matrix were collected for 5 min with a 20% window centered on 159 keV, corresponding to the 123I photopeak. After the static planar images were acquired, SPECT images were obtained. The camera was rotated over 180° from the 45° right anterior oblique position to the 45° left posterior oblique position in 32 views with an acquisition time of 40 s per view. Scans were acquired in a 64 × 64 matrix by a filtered backprojection method for reconstruction.
The heart-to-mediastinum count (H/M) ratio was determined from the anterior planar delayed 123I-MIBG image. The washout rate (WR) was calculated using the following formula: {([H]-[M])early − ([H] − [M])delayed}/([H] − [M])early × 100 (%), where [H] = mean counts per pixel in the left ventricle and [M] = mean counts per pixel in the upper mediastinum. In this study, time decay was not corrected for the calculation of WR.
The delayed myocardial SPECT images of each patient were divided into 17 segments as recommended by American Heart Association (24). Regional tracer uptake was assessed semiquantitatively using a 5-point scoring system (0 = normal uptake, 1 = mildly reduced uptake, 2 = moderately reduced uptake, 3 = significantly reduced uptake, and 4 = no uptake). The total defect score (TDS) was calculated as the sum of all defect scores. The TDS was converted to a percentage of the total denervated myocardium (% denervation). The % denervation was calculated using the following formula: (TDS/68 [maximum score = 4 × 17] × 100).
Plasma Brain Natriuretic Peptide (BNP) Concentrations
Blood samples were collected into tubes containing ethylenediaminetetraacetic acid after the patient had rested in a supine position for at least 30 min. Plasma was separated by centrifugation and frozen at −84°C. Then the plasma concentration of BNP was measured with a specific immunoradiometric assay for human BNP using a commercially available kit (Shionogi) as previously reported (14–16,25).
Data Analysis and Statistics
Statistical analysis was performed by using SPSS 12.0 for Windows (SPSS Inc.). The numeric results are expressed as the mean ± SD. Comparison of baseline categoric data between the 2 groups was done by the 1-sided χ2 contingency table method, and differences between continuous variables were evaluated using the unpaired t test. Changes in NYHA functional class were assessed using the Wilcoxon matched pairs signed rank test. In patients who underwent repeated assessment, changes from baseline were evaluated within each treatment group using a paired t test and between the 2 groups using 2-way ANOVA. Linear regression analysis was used to determine the relationship between continuous variables. In all analyses, P < 0.05 was considered statistically significant.
RESULTS
Clinical Characteristics
There were no significant differences in hemodynamic characteristics or cardiac medications between the 2 groups on entry into the study. The cause of heart failure was ischemic heart disease (IHD) (n = 23), idiopathic dilated cardiomyopathy (DCM) (n = 18), or other diseases (n = 9 (mitral regurgitation, n = 4; aortic regurgitation, n = 3; hypertensive heart disease, n = 2). At baseline, the % denervation, H/M ratio, WR, LVEDV, LVESV, LVEF, NYHA functional class, and plasma BNP concentrations were similar in both groups (Table 1).
Clinical Characteristics of Patients
The mean maintenance dose of candesartan was 10.0 ± 1.9 mg/d in group A versus 10.2 ± 1.8 mg/d in group B (P = not significant [NS]). The mean dose of carvedilol was 13 ± 6 mg/d in group A versus 14 ± 6 mg/d in group B (P = NS). The mean dose of furosemide was 54 ± 26 mg/d in group A versus 55 ± 28 mg/d in group B (P = NS). All patients were clinically stable, and no major events occurred during the follow-up period.
Comparison of Changes in Hemodynamics Before and After Treatment
After 6 mo, the systolic and diastolic blood pressure tended to decrease in both groups (group A, 130 ± 17 vs. 127 ± 18 mm Hg and 78 ± 13 vs. 75 ± 10 mm Hg, respectively; group B, 131 ± 20 vs. 128 ± 19 mm Hg and 78 ± 14 vs. 76 ± 13 mm Hg, respectively). However, there were no significant differences in these parameters. Moreover, in both groups, the heart rate did not change significantly after 6 mo (group A, from 72 ± 12 to 72 ± 13 bpm; group B, from 74 ± 14 bpm to 73 ± 14 bpm).
Comparison of Cardiac 123I-MIBG Scintigraphic Findings Before and After Treatment
The % denervation, H/M ratio, and WR data are shown in Table 2. In both groups, the % denervation decreased significantly after 6 mo compared with the baseline values (group A, P < 0.001; group B, P < 0.01). However, the absolute change of % denervation in group A was significantly greater than that in group B (P < 0.05). In both groups, the H/M ratio increased significantly after 6 mo compared with the baseline values (group A, P < 0.001; group B, P < 0.01). However, the absolute change of H/M ratio in group A was significantly greater than that in group B (P < 0.05). Finally, the WR in both groups decreased significantly after 6 mo compared with the baseline values (group A, P < 0.001; group B, P < 0.05). However, the absolute change of WR in group A was significantly greater than that in group B (P < 0.05).
Changes in % Denevation, H/M Ratio, and WR of Patients in Both Groups
Among 3 etiologies (IHD, DCM, and other diseases) at baseline in both groups, 123I-MIBG scintigraphic parameters tended to be worse in patients with IHD and tended to be better in patients with other diseases. However, they were not significantly different (Table 3). Moreover, the response to therapies was not different in these parameters between baseline and 6 mo after treatment in any disease groups (Table 3).
Changes in % Denevation, H/M Ratio, and WR of Each Etiology
Comparison of Echocardiographic Findings Before and After Treatment
The LVEDV, LVESV, and LVEF data are shown in Table 4. In both groups, the LVEDV and LVESV decreased significantly after 6 mo compared with the baseline values (LVEDV: group A, P < 0.001, and group B, P < 0.05; LVESV: group A, P < 0.001, and group B, P < 0.01). The LVEF in both groups increased significantly after 6 mo compared with the baseline values (group A, P < 0.001; group B, P < 0.05). The degree of change in LVEDV, LVESV, and LVEF in group A tended to be more favorable than that in group B, but these changes were not statistically significant.
Changes of LV Volume, LVEF, NHYA Functional Class, and Plasma BNP Concentration of Patients in Both Groups
Comparison of NYHA Functional Class Before and After Treatment
The NYHA functional class status of the patients is shown in Table 4. Patients from both groups showed improvement after 6 mo of treatment relative to the baseline status (in group A, P < 0.001; in group B, P < 0.05). After 6 mo, the NYHA functional class status of patients in group A was better than that of patients in group B (P < 0.05).
Comparison of BNP Concentrations Before and After Treatment
The plasma BNP concentrations are shown in Table 4. In both groups, the plasma BNP concentrations decreased significantly after 6 mo compared with the baseline value (group A, P < 0.001; group B, P < 0.05). However, the absolute change of BNP in group A was significantly greater than that in group B (P < 0.05).
Relationship Between LV Volume and 123I-MIBG Scintigraphic Findings Before and After Treatment
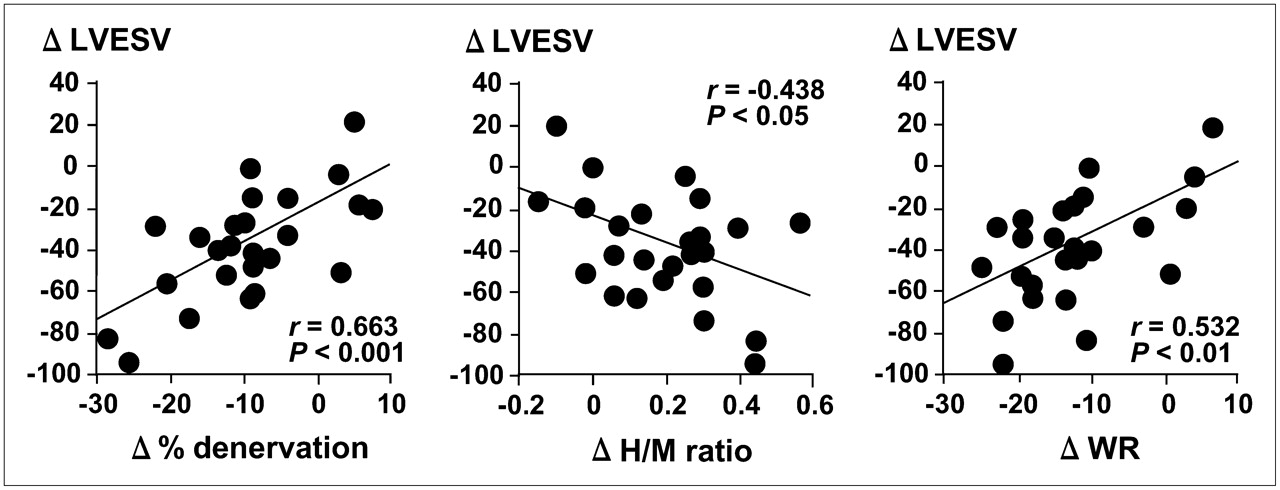
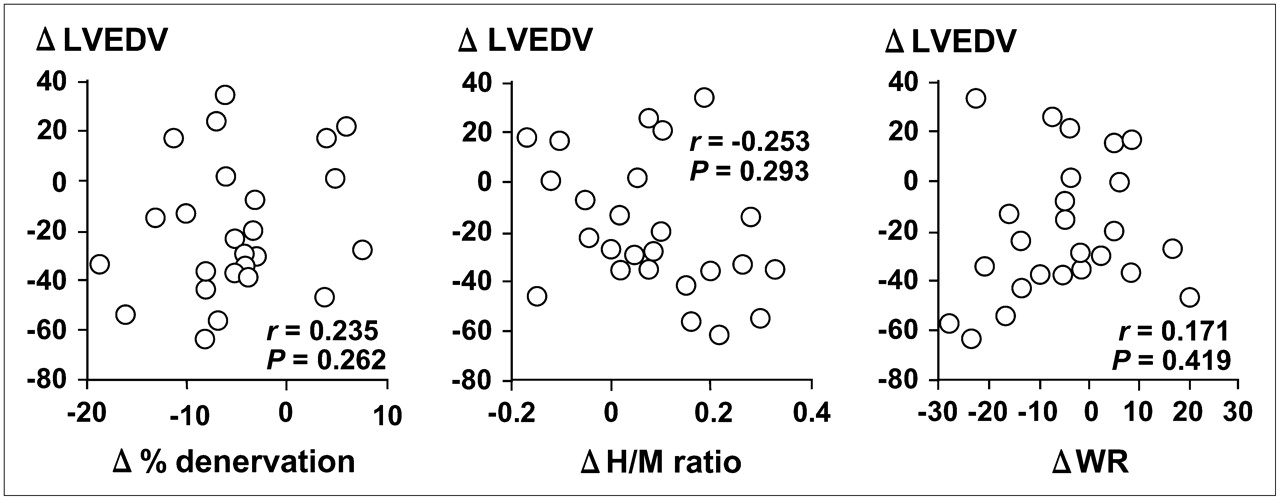
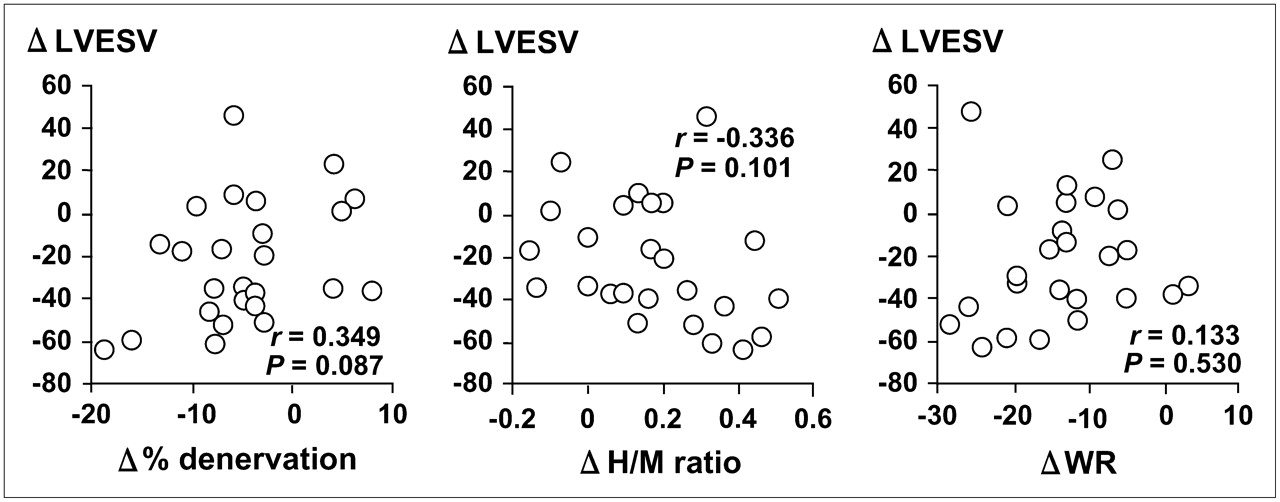
There were significant correlations between changes in the 123I-MIBG scintigraphic findings and changes in the LVEDV (% denervation, r = 0.692, P < 0.001; H/M ratio, r = −0.437, P < 0.05; and WR, r = 0.505, P < 0.01) (Fig. 1) or the LDESV in group A (% denervation, r = 0.663, P < 0.001; H/M ratio, r = −0.438, P < 0.05; and WR, r = 0.532, P < 0.01) (Fig. 2). In contrast, there was no relationship between these parameters in group B (Figs. 3 and 4).
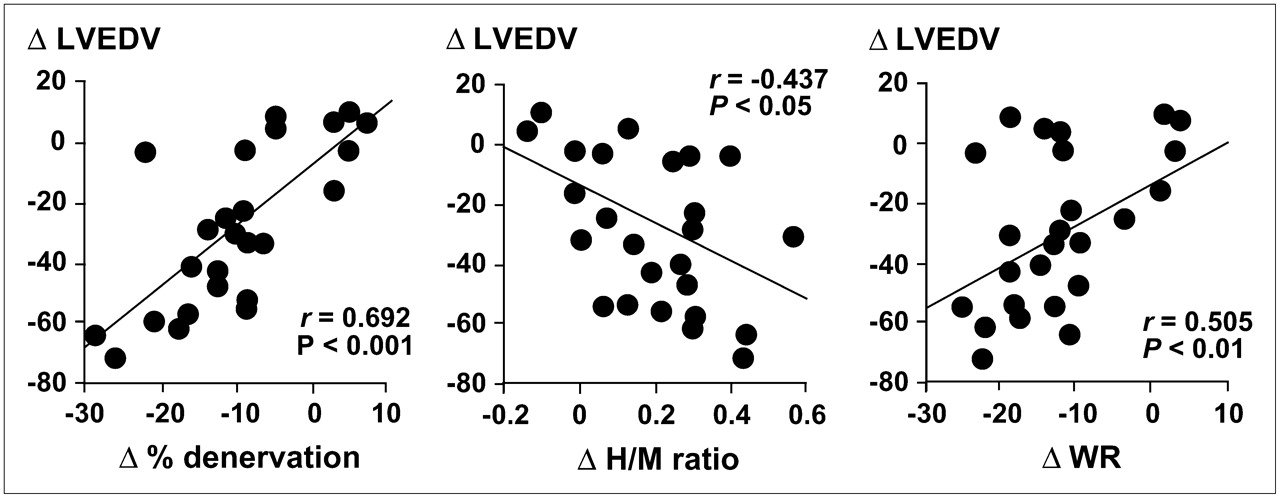
Correlations between changes of 123I-MIBG scintigraphic findings and LVEDV after combination of spironolactone and candesartan treatment in 25 patients with heart failure. Δ LVEDV = value of LVEDV after treatment – pretreatment value of LVEDV; Δ % denervation = value of % denervation after treatment – pretreatment value of % denervation; Δ H/M ratio = value of H/M ratio after treatment – pretreatment value of H/M ratio; Δ WR = value of WR after treatment – pretreatment value of WR.
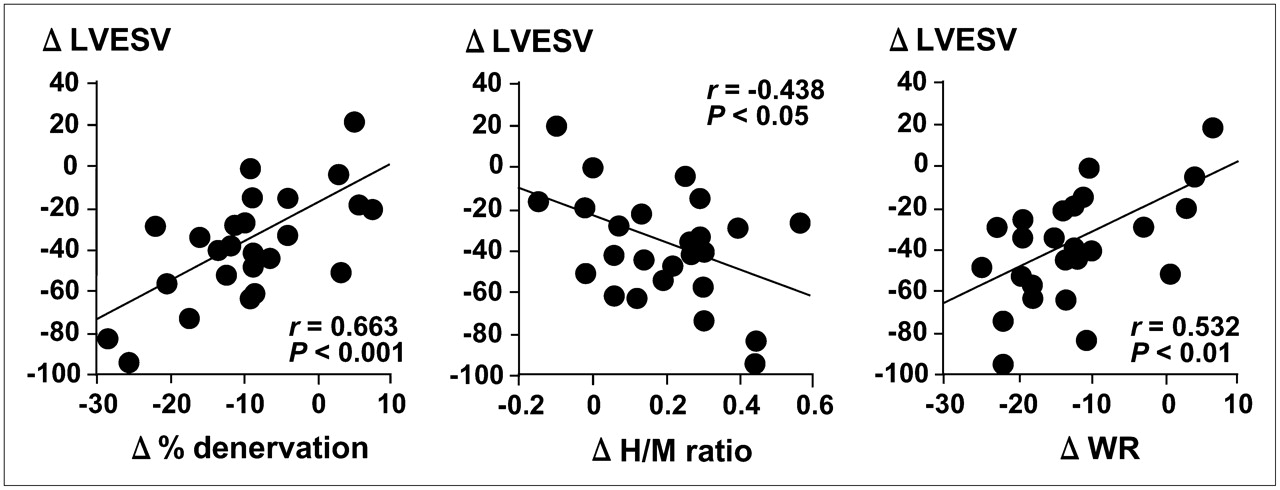
Correlations between changes of 123I-MIBG scintigraphic findings and LVESV after combination of spironolactone and candesartan treatment in 25 patients with heart failure. Δ LVESV = value of LVESV after treatment – pretreatment value of LVESV; Δ % denervation = value of % denervation after treatment – pretreatment value of % denervation; Δ H/M ratio = value of H/M ratio after treatment – pretreatment value of H/M ratio; Δ WR = value of WR after treatment – pretreatment value of WR.
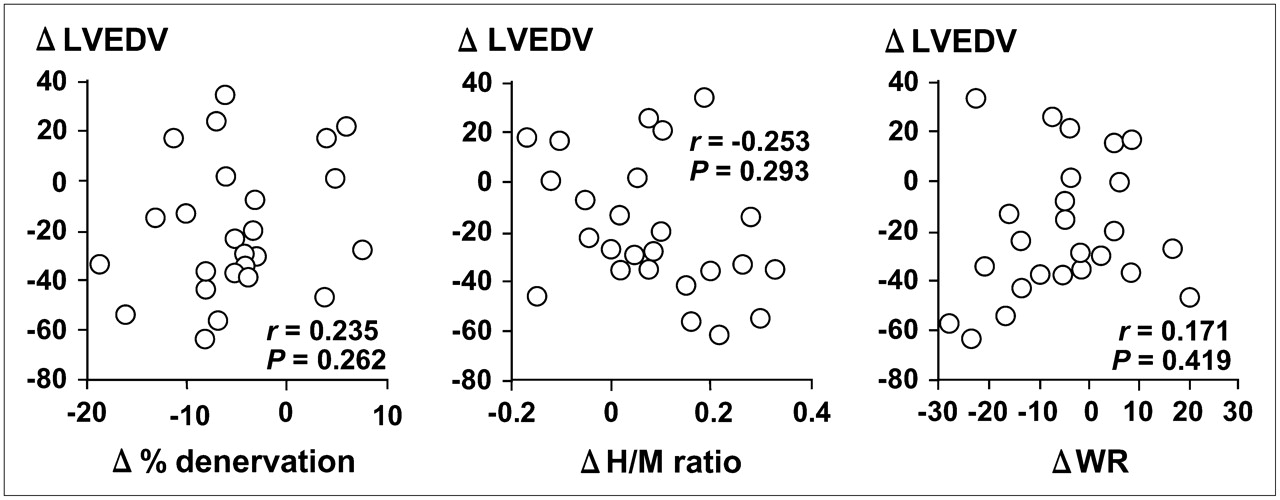
Correlations between changes of 123I-MIBG scintigraphic findings and LVEDV after candesartan treatment in 25 patients with heart failure. Abbreviations as in Figure 1.

Correlations between changes of 123I-MIBG scintigraphic findings and LVESV after candesartan treatment in 25 patients with heart failure. Abbreviations as in Figure 2.
DISCUSSION
Our findings demonstrate that the addition of spironolactone to candesartan can be more beneficial for CSNA and LV performance than candesartan alone in patients with CHF. Aldosterone promotes retention of sodium and loss of magnesium and potassium and causes myocardial and vascular fibrosis (26), direct vascular damage (27), and baroreceptor dysfunction by altering Na,K-ATPase activity (28). The ARBs target angiotensin production by the RAAS. However, they do not directly block the effects of aldosterone at the receptor level or its deleterious effects on the cardiovascular system (1). Thus, a strategy of providing more complete blockade of aldosterone with the combination of spironolactone and candesartan for the treatment of heart failure appears rational. Naruse et al. (29) reported that the combination of spironolactone and candesartan more strongly inhibits RAAS and has cardioprotective effects compared with candesartan alone in hypertensive rats.
123I-MIBG is an analog of the adrenergic neuron-blocking agent guanethidine, which is thought to use the same myocardial uptake and release mechanisms as norepinephrine (30). Therefore, cardiac 123I-MIBG imaging is a useful tool for detecting abnormalities of the myocardial adrenergic nervous system in patients with CHF (5,6). Furthermore, many reports have suggested that the treatment of CHF with ACE inhibitors (8,9,16), ARBs (13,15,17), β-blockers (9,10,19), spironolactone (11,12), or torasemide (18) can improve CSNA, on the basis of cardiac 123I-MIBG scintigraphic findings. However, to our knowledge, there have been no reports on the additive effects of spironolactone and candesartan on CSNA in patients with CHF compared with candesartan alone. In this study, we examined whether the combination of spironolactone and candesartan improves CSNA in patients with CHF using 123I-MIBG scintigraphy and found that the % denervation, H/M ratio, and WR improved with combination therapy compared with candesartan therapy alone.
On the other hand, CSNA evaluated by 123I-MIBG scintigraphy also has a useful prognostic value in patients with CHF (6,7). Merlet et al. (6) reported that the delayed H/M ratio was the best predictor for survival in 90 CHF patients with reduced cardiac function. Moreover, a multicenter trial from Imamura et al. (7) concluded that the WR was a powerful predictor of subsequent mortality and morbidity in 171 patients with CHF. For these reasons, an increasing effort has been directed toward pharmacologic improvement of CSNA in patients with CHF. This study found that the combination of spironolactone and candesartan treatment significantly improved 123I-MIBG scintigraphic parameters compared with candesartan alone. Therefore, further study to compare the long-term effects of combination therapy and candesartan therapy alone on mortality and morbidity in patients with CHF enrolled in this study is warranted.
The plasma BNP concentration is a useful prognostic indicator in patients with CHF (31), because it is a hormone produced by the left ventricle (32). The plasma BNP concentration correlates with abnormalities in the LVEF and LV end-diastolic pressure (32) as well as with LV mass (33). Therefore, a decrease in the plasma BNP concentration after combination therapy with spironolactone and candesartan may be due to a decreased LV filling pressure, improvement in LV remodeling, or both factors. A decrease in the BNP concentration during combination therapy may also reflect improvement in LV diastolic function secondary to the effects of this drug on cardiac hypertrophy and fibrosis. Treatment of CHF guided by plasma BNP concentration has been reported to reduce cardiovascular events (31), so a decrease in BNP may be associated with a better outcome, as was the case in previous studies (4,34).
Spironolactone has been reported to improve CSNA (11,12) and decrease myocardial fibrosis in patients with heart failure (35), whereas CSNA and cardiac function are correlated in patients with CHF (6). In this study, there were significant correlations between changes in the LV volume and the 123I-MIBG scintigraphic parameters after treatment with a combination of spironolactone and candesartan in patients with CHF. However, no significant correlations were found in the candesartan treatment group. With respect to the influence of spironolactone, it is still unclear whether improvement of LV function (due to the antifibrotic effect of spironolactone) increases myocardial uptake of norepinephrine or whether increased myocardial uptake of norepinephrine leads to improvement in LV function. Therefore, further studies are necessary to clarify the relationship between the improvement of LV function and increased myocardial uptake of norepinephrine. On the other hand, in this study, the relationship between LV volume and % denervation was more favorable than that between LV volume and H/M ratio or WR. The % denervation was calculated from SPECT, whereas the H/M ratio and WR were determined from the anterior planar imaging. It is known that lung congestion more strongly affects planar imaging compared with SPECT. All of our study patients had CHF and reduced cardiac function. Therefore, the baseline data for the H/M ratio and WR might not have been more accurate than that of % denervation, because baseline 123I-MIBG scintigraphy was performed during hospitalization after treatments for acute heart failure. For these reasons, the LV volume might have a better correlation with % denervation than with H/M ratio or WR in our study.
The relatively small number of patients with CHF included in our study was one limitation. Despite the group with candesartan therapy alone, the study design omitted the treatment group with a combination of spironolactone and ACE inhibitor as well as the group with ACE inhibitor alone. We need to examine the effects of 123I-MIBG scintigraphic and echocardiographic parameters using a larger numbers of patients and to compare the effects of the spironolactone plus ACE inhibitor group and ACE inhibitor group with the results of this study.
It has been reported that aldosterone is produced in the ventricles of the failing human heart (36) and that the aldosterone synthase gene is expressed in cardiac tissue (37). The same group has also demonstrated that aldosterone induces the expression of ACE messenger RNA in cultured neonatal cardiocytes (38). Furthermore, Buss et al. (39) reported that aldosterone directly prevents myocardial uptake of norepinephrine in an experimental animal model, and the mineralocorticoid receptor-antagonist spironolactone preserves cardiac norepinephrine uptake in the failing heart. We did not measure plasma aldosterone concentrations. However, aldosterone may be produced in cardiac tissue, even if the plasma aldosterone concentration is normal. Therefore, we believe that it is important to inhibit aldosterone produced in cardiac tissue by adding spironolactone to candesartan in patients with CHF.
At our institution (Cardiovascular Hospital of Central Japan), cardiac 123I-MIBG scintigraphy is routinely performed using a low-energy, general-purpose collimator. Chen et al. (40) has reported that there is significant septal penetration using this collimator, and septal penetration can degrade image quality and quantitative accuracy. In their study, the optimized protocols based on deconvolution of septal penetration using a low-energy, high-resolution collimator were useful for quantification of 123I cardiac SPECT. Thus, we need to evaluate 123I-MIBG SPECT using that protocol in the future.
Currently, many independent reports from different centers around the world support the idea that 123I-MIBG myocardial scintigraphy provides useful information for assessing patients with heart failure. However, quantitative 123I-MIBG parameters differ between institutions and between instruments, and this tracer is not widely available. For these reasons, cardiac 123I-MIBG has yet to achieve broad clinical acceptance, and the evidence supporting the clinical value of this imaging technique remains inadequate. We believe that multicenter studies are needed to establish the efficacy of this imaging modality.
CONCLUSION
Cardiac 123I-MIBG scintigraphic and echocardiographic parameters are improved 6 mo after treatment with both spironolactone and candesartan as well as with candesartan alone. Furthermore, the plasma BNP concentration decreases significantly with both therapies. However, the degree of change in these parameters with combination treatment tends to be better than that with candesartan alone. These findings indicate that the combination of spironolactone and candesartan can be more beneficial for CSNA and LV performance than candesartan alone in patients with CHF.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 18, 2007.
- Accepted for publication September 6, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 123I-MIBG SPECT for Evaluation of Patients with Heart Failure
- An Electrophysiologist Perspective on Risk Stratification in Heart Failure: Can Better Understanding of the Condition of the Cardiac Sympathetic Nervous System Help?
- Impact of Mineralocorticoid Receptor Antagonists on Changes in Cardiac Structure and Function of Left Ventricular Dysfunction: A Meta-analysis of Randomized Controlled Trials
- Aldosterone antagonists improve ejection fraction and functional capacity independently of functional class: a meta-analysis of randomised controlled trials
- Drug and Device Effects on Peak Oxygen Consumption, 6-Minute Walk Distance, and Natriuretic Peptides as Predictors of Therapeutic Effects on Mortality in Patients With Heart Failure and Reduced Ejection Fraction
- Influence of Diabetes Mellitus on Prognostic Utility of Imaging of Myocardial Sympathetic Innervation in Heart Failure Patients
- Aldosterone and Angiotensin II Synergistically Stimulate Migration in Vascular Smooth Muscle Cells Through c-Src-Regulated Redox-Sensitive RhoA Pathways
- Prognostic Value of Serial Cardiac 123I-MIBG Imaging in Patients with Stabilized Chronic Heart Failure and Reduced Left Ventricular Ejection Fraction