


Abstract
Heart failure (HF) is characterized by activation of the sympathetic cardiac nerves. The condition of cardiac sympathetic nerves can be evaluated by 123I-metaiodobenzylguanidine (123I-MIBG) imaging. Most cardiac 123I-MIBG studies have relied on measurements from anterior planar images of the chest. However, it has become progressively more common to include SPECT imaging in clinical and research protocols. This review examines recent trends in 123I-MIBG SPECT imaging and evidence that provides the basis for the increased use of the procedure in the clinical management of patients with HF. 123I-MIBG SPECT has been shown to be complementary to planar imaging in patients with HF in studies of coronary artery disease after an acute myocardial infarction. Moreover, 123I-MIBG SPECT has been used in numerous studies to document regional denervation for arrhythmic event risk assessment. For better quantification of the size and severity of innervation abnormalities in 123I-MIBG SPECT, programs and protocols specifically for 123I have been developed. Also, the introduction of new solid-state cameras has created the potential for more rapid SPECT acquisitions or a reduction in radiopharmaceutical activity. Although PET imaging has superior quantitative capabilities, 123I-MIBG SPECT is, for the foreseeable future, the only widely available nuclear imaging method for assessing regional myocardial sympathetic innervation.
Heart failure (HF) is characterized by activation of the sympathetic cardiac nerves. The condition of cardiac sympathetic nerves can be evaluated with 123I-metaiodobenzylguanidine (123I-MIBG), which is a norepinephrine analog and therefore a tracer for sympathetic neuron integrity and function (1). Most of the literature on the use of 123I-MIBG imaging for evaluating patients with HF is based on measurements from anterior planar images of the chest, with cardiac uptake quantified in terms of the heart-to-mediastinum ratio (HMR) and the washout rate between early and late images (2,3). However, given the conversion from planar to SPECT techniques in clinical nuclear myocardial perfusion imaging (MPI) beginning in the 1980s, it is not surprising that 123I-MIBG SPECT was also performed by some early adopters of the radiopharmaceutical (4,5). Despite the challenges associated with performing 123I-MIBG SPECT and interpreting the images in patients with severely reduced cardiac 123I-MIBG uptake, it has become progressively more common for 123I-MIBG SPECT imaging to be included in clinical and research protocols; in such settings, it is usually performed as part of one or more imaging sessions in which planar images are acquired (2).
Both qualitative and quantitative image reviews of 123I-MIBG SPECT studies may be performed to identify focal areas of reduced uptake (similar to protocols used for the interpretation of MPI SPECT studies). Unfortunately, only small amounts of data from 123I-MIBG SPECT images of patients without heart disease are available; most often, segmental count density expressed as a percentage of total myocardial count density is used to compare affected areas with least affected areas in patients (6–8). Changes in relative uptake and absolute uptake between early and late SPECT images can be used to calculate parameters comparable to the planar washout rate (9). In general, SPECT results have been used in the same way as planar data—namely, to investigate the relationship between the quantitative value of 123I-MIBG uptake and a specific outcome event, such as worsening of chronic HF, the occurrence of an arrhythmic event or cardiac death, or another quantitative parameter, such as a change in the left ventricular ejection fraction or the MPI defect score. Consistent with findings on planar imaging, patients with larger or more severe regional 123I-MIBG SPECT defects usually have poorer outcomes (10).
This review examines recent trends in 123I-MIBG SPECT imaging and evidence that provides the basis for the increased use of the procedure in the clinical management of patients with HF. The focus of the article is primarily on work that has been done in the past 10–15 y, considering specifically how the technique can complement the established value of planar 123I-MIBG imaging and provide unique insight into the risk of arrhythmia and the need for advanced therapies. Recent advances in imaging technology and quantitation methods are also briefly reviewed, as these represent the future for the clinical use of cardiac 123I-MIBG SPECT.
123I-MIBG SPECT COMPLEMENTS PLANAR IMAGING
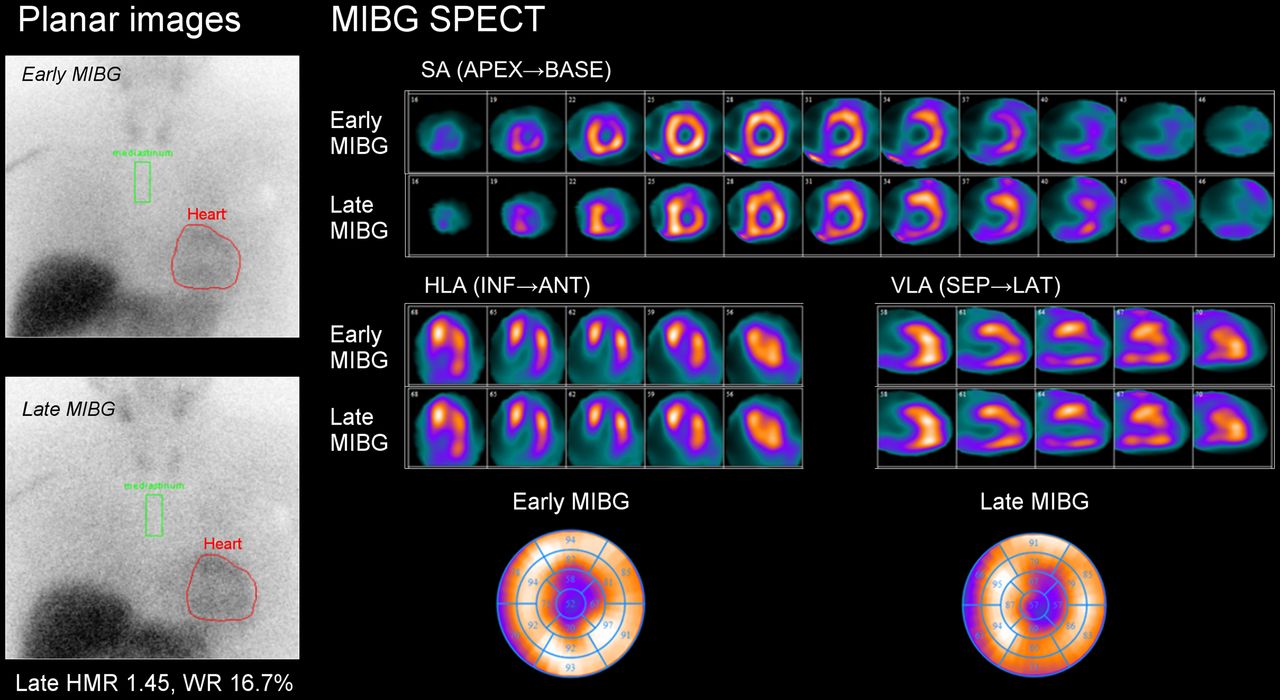
Several studies have examined the use of 123I-MIBG imaging as a diagnostic and prognostic tool in patients with HF (3,11). Although most of these studies relied primarily on planar imaging determinations of HMR and washout rate, some also included measurements from SPECT examinations because of the realization that SPECT may overcome the difficulties of planar imaging, including superposition of noncardiac structures and lack of segmental analysis (Fig. 1). Many such 123I-MIBG SPECT studies were performed by Kasama et al., who investigated the effects of a variety of HF medications on 123I-MIBG cardiac uptake and clinical outcomes, usually performing imaging before the initiation of a new medication and again after 6 mo (12–19). Early and late 123I-MIBG SPECT images (acquired at 15 min and at 4 h) were scored visually with 20- and 17-segment regional polar or bull’s-eye maps. Additionally, segmental count data were used to calculate regional washout rates in some studies. The various randomized studies demonstrated statistically significant reductions in late 123I-MIBG total defect scores after treatment with an angiotensin-converting enzyme inhibitor (perindopril), angiotensin receptor blockers (valsartan and candesartan), a loop diuretic (torasemide), and an aldosterone inhibitor (spironolactone). Similar results were obtained by other investigators, such as Somsen et al. (20) (for enalapril) and Lotze et al. (21) and de Milliano et al. (22) (for various β blockers).

123I-MIBG SPECT complements planar imaging on segmental analysis. Planar images and SPECT images in short axis (SA), horizontal axis (HLA), vertical long axis (VLA), and bull’s-eye of 123I-MIBG were obtained for 60-y-old patient. Reduced late HMR was 1.45. 123I-MIBG SPECT demonstrated fixed apical defect. ANT = anterior; INF = inferior; LAT = lateral; SEP = septal; WR = washout rate.
123I-MIBG SPECT has been shown to be complementary to planar imaging in studies of coronary artery disease after an acute myocardial infarction (MI) (23,24). Viable but denervated myocardium has been shown to be supersensitive to the effects of infused catecholamines (25), which may provide a substrate for the genesis of ventricular arrhythmias. For this reason, the results of 123I-MIBG SPECT and MPI SPECT are often compared by identifying segments with adrenergic/perfusion mismatches. As in MPI SPECT studies, the myocardium is usually subdivided into several segments (ranging from 5 to 20), and each location is scored for severity (on scales from 0 to 3 or 0 to 4).
Three categories of 123I-MIBG SPECT and MPI SPECT findings are commonly reported: both normal; both equivalently abnormal (matched defects); or 123I-MIBG SPECT defect more severe than MPI SPECT defect (mismatched defects) (Fig. 2). A defect less severe on 123I-MIBG SPECT than on MPI SPECT is rarely, if ever, observed. Mismatched defects may be subcategorized in terms of whether the area in question demonstrates ischemia on stress MPI or remains unchanged.

Innervation–perfusion mismatch between 123I-MIBG SPECT and rest MPI with 99mTc-tetrofosmin. Rest MPI demonstrated large inferoposterolateral expanding apical defect in 63-y-old patient with ischemic cardiomyopathy. 123I-MIBG SPECT demonstrated more extended inferolateral defect. HLA = horizontal axis; SA = short axis; VLA = vertical long axis.
Most studies of 123I-MIBG imaging in patients after MI have compared defects on 123I-MIBG SPECT with results on rest and stress MPI to assess the relationship between areas of infarction and denervation. Three small studies (26–28) in which 58 patients were examined within 3 mo after MI arrived at the joint conclusion that the 123I-MIBG defects were generally larger than those on MPI, whether determined from quantitative count–based assessments or from semiquantitative scoring of SPECT myocardial segments. Given that sympathetic nerve fibers in the heart travel in the subepicardium parallel to the vascular structures and penetrate the underlying myocardium, it is conceivable that this difference in defect size, among others, is caused by the fact that neural tissue has a greater sensitivity to hypoxia than myocardial fibers and has a longer recovery time (29,30). More recent studies, such as those by Simões et al. (31), Marini et al. (32), and Hayashi et al. (33), confirmed the presence of denervated areas extending beyond the infarct borders and proposed associations with depolarization abnormalities, unappreciated myocardial necrosis, and long-term variability in induced ventricular tachyarrhythmias.
Interest has been shown in the potential for the global quantitation of 123I-MIBG SPECT images to replace the planar HMR for diagnostic and prognostic purposes. An analysis of the 123I-MIBG SPECT studies from the AdreView Myocardial Imaging for Risk Evaluation in Heart Failure (ADMIRE-HF) trial, which is a prospective trial evaluating 123I-MIBG imaging for identifying patients who have HF and are most likely to experience cardiac events, demonstrated that the SPECT HMR was equivalent to the planar HMR for discriminating between patients with HF and control subjects (6,34). Additionally, the ability of 123I-MIBG SPECT to provide regional information not available on planar images remains a driver for efforts to incorporate this procedure into assessments of patients with HF for arrhythmic event risk (35).
123I-MIBG SPECT FOR ARRHYTHMIC EVENT RISK ASSESSMENT
Better arrhythmic event risk assessment is necessary given that in the MADIT II trial, only 23.5% of the 720 patients with HF and a prophylactic implantable cardioverter defibrillator (ICD) received antiarrhythmia device therapy for ventricular tachyarrhythmia (36). Early research on experimentally denervated myocardium suggested that such regions were much more sensitive to norepinephrine infusion than normally innervated regions, a situation considered potentially proarrhythmic (37). Over the subsequent decades, 123I-MIBG SPECT was used in numerous studies to document such regional denervation and its association with naturally occurring or inducible ventricular arrhythmic events. The dominant observation was that the larger the extent of the 123I-MIBG SPECT abnormality, the higher the likelihood of ventricular tachyarrhythmia (38–41).
Most investigators performing 123I-MIBG SPECT studies had expected to find that arrhythmic event risk would increase with the size of the denervated area as well as the amount of innervation–perfusion mismatch, as reflected by paired 123I-MIBG and MPI SPECT studies. Another expectation was that there would be a dividing point in 123I-MIBG defect size between patients with “low risk” and patients with “high risk” for arrhythmic events. In the small study by Arora et al. (38), both mean 123I-MIBG defect scores and the number of late mismatches were higher in the 10 patients who had experienced appropriate ICD discharges than in the 7 who had not. Patients who had ischemic heart disease and inducible ventricular tachycardia on electrophysiology testing had higher total 123I-MIBG SPECT defect scores than patients who did not have inducible ventricular tachycardia, with a late total defect score threshold of 37, yielding a 77% sensitivity and a 75% specificity (39). In the prospective study by Boogers et al. (40), patients with an ICD and a late total defect score of greater than 26 were 10 times more likely to receive appropriate ICD therapy (cumulative 3-y event rate: 52% vs. 5%; P < 0.01). Interestingly, in the latter 2 studies, 123I-MIBG SPECT defect size was a significant predictor of arrhythmic events but not mismatch scores. In contrast, Marshall et al. (42) found differences in both the total 123I-MIBG SPECT defect score (37.0 ± 9.4 [mean ± SD] vs. 25.5 ± 7.7; P = 0.001) and the mismatch score (18.5 ± 8.5 vs. 8.4 ± 5.0; P < 0.01) between patients with ICD firing and those without ICD firing. As in the study of Bax et al. (39), a total 123I-MIBG SPECT defect score of greater than or equal to 31 had a sensitivity of 78% and a specificity of 77%.
Recent evidence suggests that quantitative characterization of myocardial transition zones (between normal and infarcted or denervated myocardium) may supplement the more simple definition of innervation–perfusion mismatch. In a quantitative reanalysis of the SPECT images that were interpreted visually in the study of Bax et al. (39), MPI scar extent, border zone extent, and 123I-MIBG uptake in the border zone were analyzed; the best prediction accuracy for ventricular tachycardia inducibility was achieved with the last (area under the receiver operating characteristic curve, 0.78) (43). In a prospective study of 15 patients referred for ischemic ventricular tachycardia ablation, 3-dimensional innervation models were derived from 123I-MIBG SPECT examinations and registered to high-density voltage maps (44). 123I-MIBG innervation defects were approximately 2.5-fold larger than bipolar voltage–defined scars, all ventricular tachycardia ablation sites were within areas of abnormal innervation, but 36% of successful ablation sites demonstrated normal voltages (>1.5 mV). These studies strongly suggested that innovations in quantitative analysis techniques represent the future of 123I-MIBG SPECT for identifying arrhythmic event risk and guiding therapy.
Studies have also raised questions about the relationship between 123I-MIBG defect severity and arrhythmic event risk. Planar HMR data showed that the highest occurrence of arrhythmic events was seen in patients with HF and an intermediate reduction in uptake rather than the lowest values. In 2014, Verberne et al. presented the results of an informed reinterpretation of 123I-MIBG and MPI SPECT studies from the ADMIRE-HF trial; the results showed that patients with HF and an intermediate severity of total defect scores (14–28 of a possible maximum of 68) had higher arrhythmic event rates than those with more severe defects (45). As part of the same study, visual scoring of regions (anterior, inferior, septal, lateral, and apical) on 123I-MIBG and MPI SPECT studies as normal, matched, or mismatched resulted in similar findings; patients with HF and 1 or 2 mismatched regions had the highest arrhythmic event rates (46). In both of those analyses, the largest absolute number of arrhythmic events was seen in patients with the most severe defects, but the highest proportion was seen in patients with intermediate-severity defects.
The aforementioned results attest to the mechanistic complexity of arrhythmia generation and support the conclusion that no single test can identify all at-risk patients with HF. Nevertheless, there is growing evidence that 123I-MIBG SPECT imaging should be considered for the assessment of patients with HF for appropriate therapeutic interventions.
ADVANCES IN 123I-MIBG SPECT QUANTITATION
123I-MIBG is internalized by neuroendocrine cells through the rapid energy-dependent uptake mechanism (47), reaching a relative plateau within a few minutes after injection. It is stored, unmetabolized, in the neurosecretory granules, resulting in a specific concentration, unlike in cells of other tissues. Because of flow-limited uptake of the 123I-MIBG tracer, retention measures are insensitive to low to moderate levels of regional denervation and decline only when nerve losses become fairly severe (48).
Since the earliest investigations of 123I-MIBG SPECT in cardiology, quantitation of the size and the severity of innervation abnormalities has been performed (49). Initially, semiquantitative scoring from a visual analysis, analogous to that used in MPI, was performed, as noted earlier for studies of patients after MI (27,28). When quantitative bull’s-eye mapping for MPI SPECT became readily available, it was also applied to 123I-MIBG SPECT analysis (23,50–52). However, because the quantitative programs were usually adapted from those developed for MPI SPECT, they did not take into account the unique physical properties of MIBG iodinated with 123I, which affects image quality. These include the presence of a significant number of high-energy photons (1.1% yield of 529-keV γ rays) (53); accumulation in the liver that overlaps the inferior wall (Fig. 3); and scattering from the lung field to the lateral left ventricular wall (54), as a result of which the normal cardiac 123I-MIBG distribution includes relatively low uptake in the inferior wall (55), which is more pronounced in the elderly. Therefore, in contrast to what is observed in PET examinations with 11C-hydroxyephedrine and 18F-fluorodopamine, the regional 123I-MIBG uptake in the left ventricle is heterogeneous in healthy subjects, as observed by Morozumi et al. (56) and Yoshinaga et al. (57).

123I-MIBG SPECT images in short axis (SA), horizontal axis (HLA), vertical long axis (VLA), and bull’s-eye demonstrate that accumulation of 123I-MIBG in liver and bowel overlaps inferior wall and affects image quality.
More recently, programs and protocols have been developed specifically for 123I-labeled compounds such as 123I-MIBG. These have included the introduction of iterative reconstruction techniques with compensation for scatter and septal penetration (53,58,59) and the use of volumetric analysis techniques (60). The development of 123I-MIBG databases for healthy subjects has also provided a more reliable means for quantifying the significance of reduced uptake in HF and other cardiology patients (6).
The potential of improved 123I-MIBG quantitation techniques has been explored in recent reevaluations of the large 123I-MIBG SPECT imaging database from the ADMIRE-HF trial. Through the use of a variable reference threshold for pixel-based abnormalities based on the planar HMR, quantitative differences between 123I-MIBG SPECT patterns in patients with ischemic HF and patients with nonischemic HF could be reliably demonstrated with satisfactory reproducibility by both voxel- and region-based methods (7,61). In a separate analysis, global denervation (≥9 abnormal 123I-MIBG segments from the standard 17-segment map) was associated with the highest cardiac mortality rates in both patients with ischemic HF and patients with nonischemic HF, but further distinction was possible on the basis of MPI SPECT findings. In patients with ischemic HF, mortality risk was highest among those with 3–7 rest MPI segmental defects, whereas in patients with nonischemic HF, the highest risk was associated with nearly normal rest MPI studies (0–3 segmental defects) (62).
Pellegrino et al. demonstrated excellent observer reproducibility of a visual evaluation of 123I-MIBG SPECT studies with a low-dose 123I-MIBG protocol (63). Nevertheless, it can be challenging to evaluate 123I-MIBG SPECT studies visually, especially in patients with HF and a global reduction in uptake (35). Automated quantitation of 123I-MIBG SPECT studies offers the potential to overcome some of the limitations of visual image interpretation and improves the clinical utility of such studies for diagnosis and prognosis.
123I-MIBG SPECT WITH SOLID-STATE CAMERAS
The recent introduction of new solid-state cardiac nuclear cameras that provide 180° of imaging without the need for gantry rotation, improved collimator design, and optimized acquisition geometry with increased photon sensitivity and contrast resolution has created the potential for more rapid SPECT acquisitions or a reduction in radiopharmaceutical activity and thus a lower dose for patients (64–66).
This technology also offers advantages for 123I-MIBG SPECT imaging, including better energy discrimination and temporal resolution (67). List-mode acquisition analogous to that used in PET presents an opportunity to obtain true dynamic SPECT data, which could provide new physiologic insights to enhance the information content of the examination.
Initial experiences with 123I-MIBG SPECT imaging and solid-state cadmium–zinc–telluride cameras have been promising. Patients with left ventricular dysfunction were shown to have higher 123I-MIBG summed defect scores than those with normal function (68). Similar results were obtained when mechanical dyssynchrony on MPI SPECT was compared with 123I-MIBG SPECT findings (69).
Data on the in vivo myocardial kinetics of 123I-MIBG are rare. Dynamic 123I-MIBG SPECT has the potential for defining new quantitative parameters, as shown in early human experiments. Tinti et al. demonstrated the feasibility of dynamic 3-dimensional 123I-MIBG kinetic analysis for providing additional information on cardiac innervation, particularly through the analysis of time–activity curves for 123I-MIBG (70). Also, in an experimental pig model, myocardial peak uptake was observed earlier than had been previously described (71).
Although the possibilities of dynamic 123I-MIBG SPECT were initially explored with conventional rotating γ cameras (72), the clinical potential of this technique with cadmium–zinc–telluride cameras likely will be established as the new solid-state camera technology matures and more users gain experience with it.
COMPARISON OF SPECT AND PET TECHNIQUES
The superior quantitative capabilities of PET imaging make PET an attractive alternative to SPECT. However, unlike compounds such as 123I-MIBG, which can be centrally manufactured and widely distributed commercially, most PET agents are labeled with short–half-life isotopes such as 11C and therefore are available only in facilities with an on-site cyclotron. Nevertheless, as a research tool, PET remains extremely valuable. The PET agent most analogous to 123I-MIBG is metahydroxyephedrine (mHED), as the uptake of both by sympathetic neurons is mediated by the norepinephrine transporter. However, in only a few studies has the cardiac uptake of 123I-MIBG been directly compared with that of mHED.
In a study of rabbits injected with both 123I-MIBG and mHED, similar reductions in uptake in denervated myocardium were observed (73). However, pretreatment with the norepinephrine-depleting compound reserpine had a greater effect on mHED uptake than on 123I-MIBG uptake, suggesting that the former might be more specific for intravesicular uptake than the latter. Luisi et al. showed that the relative retention of mHED was significantly greater than that of 123I-MIBG in pigs, reflecting improved specificity as a result of less nonspecific uptake of the former tracer (74). Rischpler et al. (75) reported that the 131I-MIBG uptake defect in rats matched the area of an earlier MI, whereas the mHED uptake defect was larger. However, in a direct comparison of 123I-MIBG SPECT and mHED PET in 21 patients with left ventricular dysfunction, Matsunari et al. (76) reported a high correlation between defect sizes in the 2 methods; however, late 123I-MIBG SPECT overestimated defect sizes in the inferior and septal regions, presumably because of image quality issues caused by adjacent liver activity.
Although the early development of an 18F-labeled compound for PET imaging of sympathetic neurons is continuing (77), for the foreseeable future 123I-MIBG SPECT will remain the only widely available nuclear imaging method for assessing regional myocardial sympathetic innervation.
CONCLUSION
The shift from planar to SPECT techniques in 123I-MIBG imaging has been slow in comparison with what occurred in clinical MPI 25–30 y ago. Nevertheless, the accumulation of evidence regarding the value of 123I-MIBG SPECT results, along with improvements in imaging equipment and image processing techniques, should result in acceleration of the growth and clinical use of the technique in the coming years.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 13, 2015.
- Accepted for publication April 10, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Illuminating the Hidden: Standardizing Cardiac MIBG Imaging for Sympathetic Dysfunction
- Molecular Imaging Biomarkers in Cardiooncology: A View on Established Technologies and Future Perspectives
- Simplified Quantification and Acquisition Protocol for 123I-MIBG Dynamic SPECT
- Sleep-disordered breathing, impaired cardiac adrenergic innervation and prognosis in heart failure
- Quantitative Analysis of Dynamic 123I-mIBG SPECT Imaging Data in Healthy Humans with a Population-Based Metabolite Correction Method