


Abstract
Many studies have shown that a one-time 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphic study during a stable period is useful for determining the prognosis of patients with chronic heart failure (CHF). However, the findings from this imaging modality are well known to be improved by medical treatment for heart failure. Accordingly, this study was performed to determine whether serial 123I-MIBG scintigraphic studies represent a reliable prognostic marker for patients with CHF. Methods: A total of 208 patients with CHF (left ventricular ejection fraction [LVEF] < 45%) and with no cardiac events for at least 5 mo were identified on the basis of a history of decompensated acute heart failure requiring hospitalization. The delayed percentage of denervation (% denervation), delayed heart-to-mediastinum count (H/M) ratio, and washout rate (WR) were determined from the patients' 123I-MIBG images just before they left the hospital and after they had received 6 mo of treatment. The left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), and LVEF were also determined by echocardiography at the same time points. Results: Of the 208 patients, 56 experienced fatal cardiac events during the study. The mean follow-up period was 4.45 ± 1.82 y. The baseline H/M ratio and WR; follow-up % denervation, H/M ratio, and WR; Δ-% denervation, H/M ratio, and WR; baseline LVEF; follow-up LVEDV, LVESV, and LVEF; and Δ-LVEDV, Δ-LVESV, and Δ-LVEF were significantly worse in the cardiac death group. A Cox regression analysis showed that the Δ-WR was an independent predictor of cardiac death. Moreover, sudden death occurred in 13 of the 56 patients with cardiac death. A Cox regression analysis also showed that the Δ-WR was an incremental predictor of sudden death. The cardiac death–free rate and sudden death–free rate were significantly higher in patients with Δ-WR less than −5% and Δ-WR less than −2% than in patients with Δ-WR greater than or equal to −5% and Δ-WR greater than or equal to −2%. Conclusion: Δ-WR obtained from serial 123I-MIBG scintigraphic studies can be useful for predicting cardiac death and sudden death in stabilized patients with CHF.
The activation of the sympathetic nervous system is one of the cardinal pathophysiologic abnormalities associated with human heart failure (1). Therefore, plasma norepinephrine concentrations affect the morbidity and mortality of patients with chronic heart failure (CHF) (2). Myocardial imaging with 123I-metaiodobenzylguanidine (MIBG), an analog of norepinephrine, is useful for detecting abnormalities in the myocardial adrenergic nervous system in patients with CHF (3,4). Furthermore, cardiac sympathetic nerve activity evaluated by 123I-MIBG scintigraphy has useful prognostic value in patients with CHF (4–6), and this imaging modality has also been useful for predicting sudden death (7). Although a large number of reports have suggested that medical treatments for heart failure can improve 123I-MIBG scintigraphic parameters in patients with CHF (8–20), earlier studies (4–7) evaluated a one-time 123I-MIBG scintigraphic study during the stable period for prognosis of cardiac death or sudden death. Accordingly, the current study was performed to determine whether serial 123I-MIBG scintigraphic studies represent a reliable prognostic marker for predicting cardiac death and sudden death in stabilized patients with CHF.
MATERIALS AND METHODS
Study Patients and Protocol
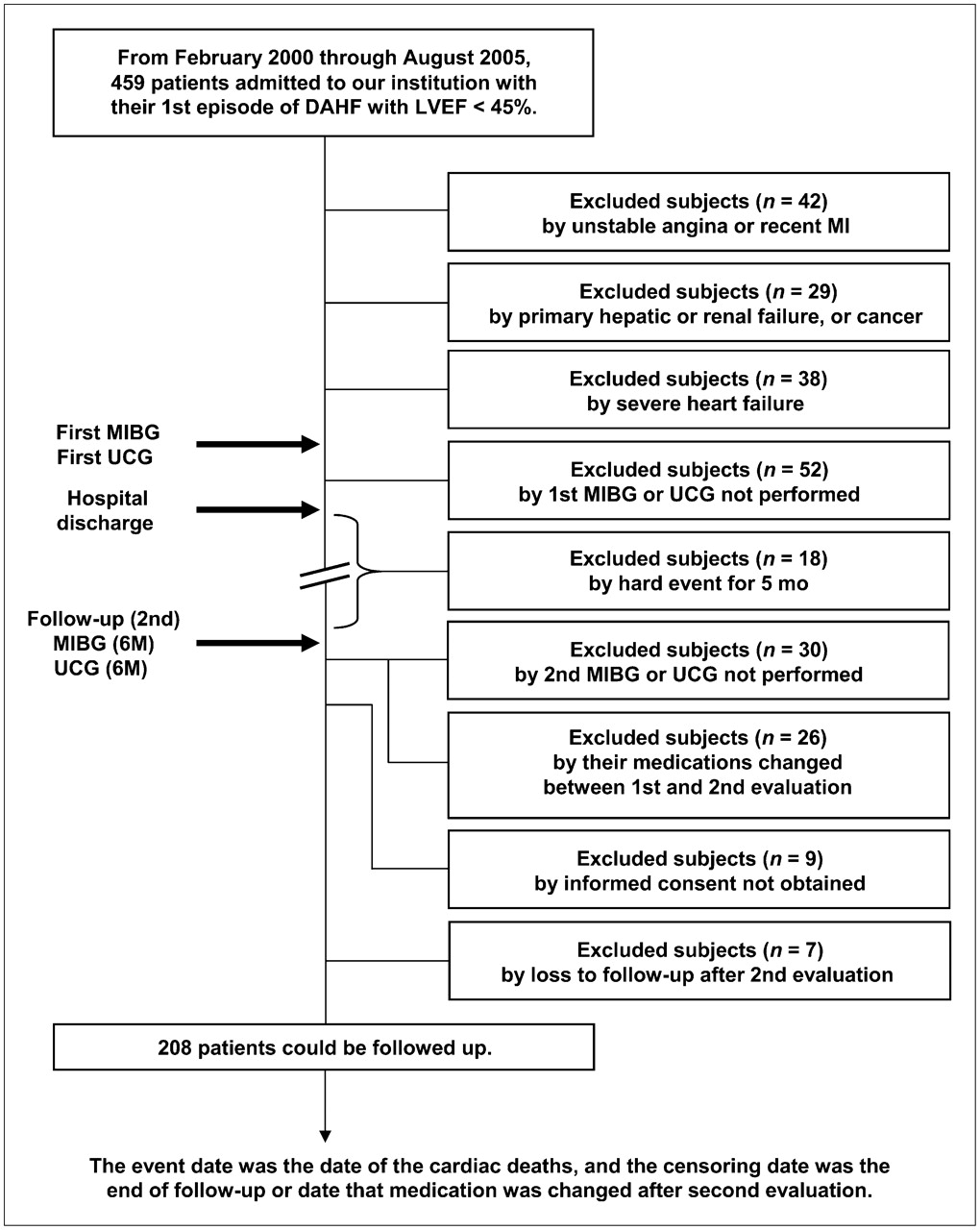
From February 2000 to August 2005, 459 patients were admitted to our institution with their first episode of decompensated acute heart failure with a left ventricular ejection fraction (LVEF) of less than 45%. Chest radiography, standard electrocardiography, and echocardiography were performed in all of the patients. In the acute phase, all patients were treated with standard therapy for heart failure. Patients with unstable angina or recent acute myocardial infarction (42 patients) and patients with primary hepatic failure, renal failure, or active cancer (29 patients) were excluded from the study. Moreover, patients with severe heart failure requiring mechanical support (intraaortic balloon pumping, left ventricular assist device, or cardiac resynchronization therapy) and patients requiring heart transplantation were also excluded (38 patients) (Fig. 1).
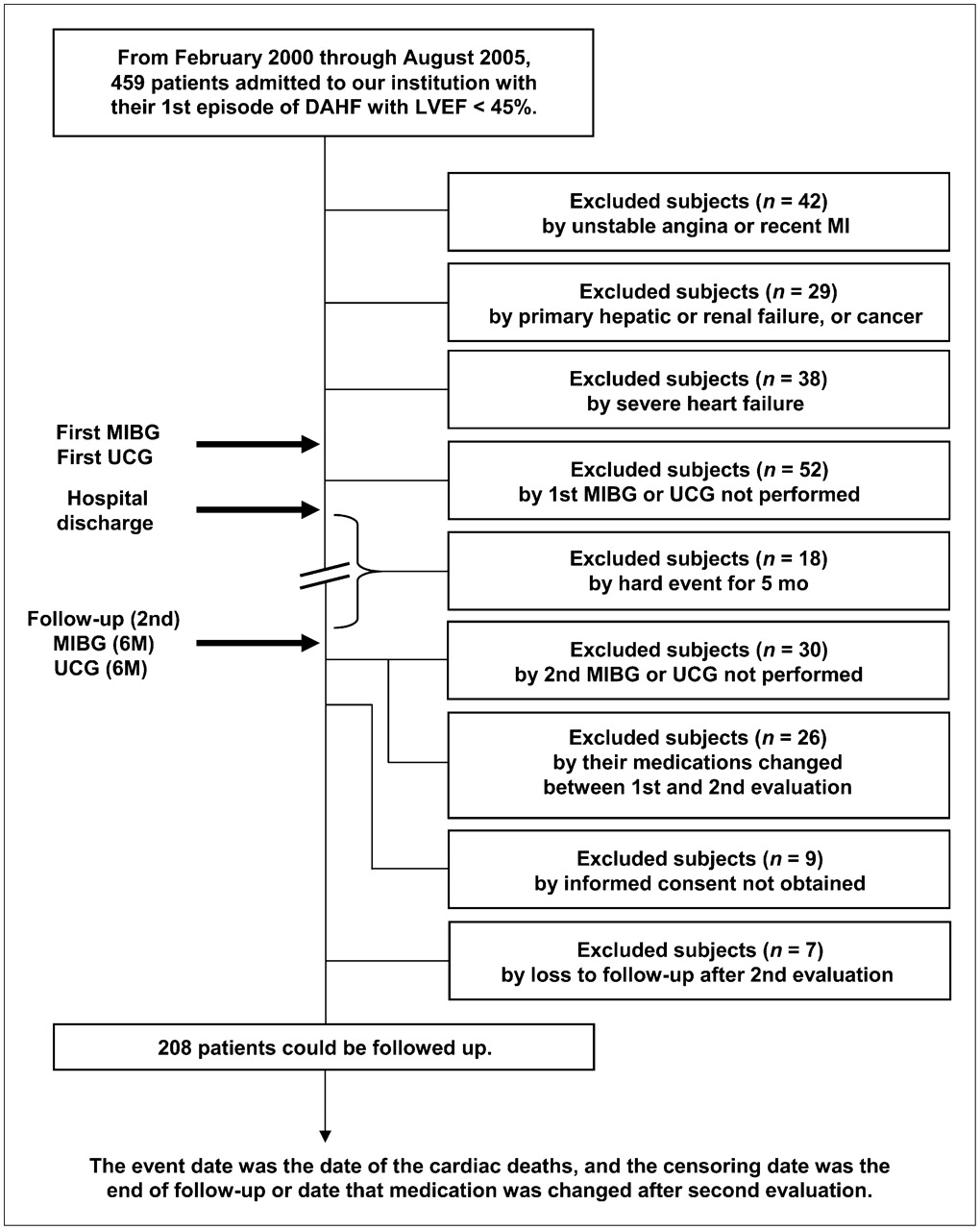
Flow diagram of participants in current study. DAHF = decompensated acute heart failure; UCG = ultrasound cardiography; 6M = after 6 mo of hospital discharge.
In the stable period, all patients were treated with oral medications for heart failure, including angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers (ARBs), β-adrenergic blocking agents, loop diuretics, and the aldosterone-receptor antagonist spironolactone. None of the patients was treated with tricyclic antidepressants or other serotonin reuptake inhibitors. We performed 123I-MIBG scintigraphy and echocardiography on patients just before their hospital discharge. However, 52 patients were excluded from this study because scintigraphy or echocardiography had not been performed during their hospitalization. The medical management of the patients was directed by an internist or a cardiologist from our institution, and 123I-MIBG scintigraphic and echocardiographic parameters were available to them. In this study, 18 patients were excluded because there were hard events (10 with cardiac events, 5 with cerebral events, and 3 with other events) for 5 mo after enrollment.
The 123I-MIBG scintigraphy and echocardiography were repeated about 6 mo after the patients' hospital discharge (mean, 6.4 mo); the date was defined as day 0 of observation. Patients were excluded from the study if the second evaluation had not been performed (30 patients) or if their medication had changed between the first and the second evaluations (26 patients). The study was approved by the ethics review board of our institution, and informed written consent was obtained from all patients except 9, who were excluded because informed consent was not obtained. Moreover, 7 patients were excluded because there was no follow-up after the second evaluation.
Finally, we were able to follow 208 patients with highly reliable information about their prognosis from the patients themselves, their families, or their affiliated hospitals (Fig. 1). The 208 study patients consisted of 130 men and 78 women with a mean age of 68.6 y (range, 35–87 y). In the present study, cardiac deaths were classified as sudden death, heart failure death, or death secondary to myocardial infarction. Death was considered sudden if it was unexpected (based on the patient's clinical status) and if it occurred out of the hospital within 15 min of the onset of unexpected symptoms or during sleep. Death during hospitalization for worsening congestive symptoms was considered the heart failure death.
123I-MIBG Imaging
The 123I-MIBG imaging method has been described previously (21,22). The 123I-MIBG was obtained from a commercial source (FUJIFILM RI Pharma Co. Ltd.). Patients were injected intravenously with 123I-MIBG (111 MBq) while in a supine position. At 15 min and at 4 h after injection, static data were acquired in the anterior view with a single-head γ-camera (Millennium MPR; GE Healthcare) equipped with a low-energy, general-purpose, parallel-hole collimator. Static images on a 128 × 128 matrix were collected for 5 min with a 20% window centered on 159 keV, corresponding to the 123I photopeak. After the static planar images were acquired, SPECT images were obtained. The camera was rotated over 180° from the 45° right anterior oblique position to the 45° left posterior oblique position in 32 views with an acquisition time of 40 s per view. Scans were performed in a 64 × 64 matrix, and the images were reconstructed by a filtered backprojection method.
The heart-to-mediastinum count (H/M) ratio was determined from the anterior planar delayed 123I-MIBG image using a method reported by Merlet et al. (4). The washout rate (WR) was calculated using the following formula: {([H] − [M]) × early − ([H] − [M]) × delayed} ÷ ([H] − [M]) × early × 100 (%), where [H] equals the mean count per pixel in the left ventricle and [M] equals the mean count per pixel in the upper mediastinum. In this study, time decay was not corrected for the calculation of WR. The delayed myocardial SPECT images of each patient were divided into 17 segments as recommended by the American Heart Association (23). Regional tracer uptake was assessed semiquantitatively using a 5-point scoring system (0, normal uptake; 1, mildly reduced uptake; 2, moderately reduced uptake; 3, significantly reduced uptake; 4, no uptake). The total defect score (TDS) was calculated as the sum of all defect scores. The TDS was converted to percentage of the total denervated myocardium (% denervation). The % denervation was calculated using the following formula: (TDS ÷ 68 [maximum score = 4 × 17] × 100). At our laboratory, the normal range for the % denervation is 6–18, for the delayed H/M ratio it is 218–270, and for the WR it is 20%–30%, as previously reported (19).
Echocardiography
Echocardiography was performed by 2 experienced, independent echocardiographers using standard methods in a masked manner. The left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), and LVEF were calculated using the modified method of Simpson (24).
Serial Changes Between the First and Second Scintigraphic and Echocardiographic Parameters
Changes between the first and second 123I-MIBG scintigraphic parameters (% denervation, H/M ratio, and WR) and echocardiographic parameters (LVEDV, LVESV, and LVEF) were calculated using the following formula: Δ-(X) = ([X] value after 6 mo) – (baseline value of [X]), where [X] equals the 123I-MIBG scintigraphic or echocardiographic parameters.
Data Analysis and Statistics
Analysis was performed using statistical software (SPSS 12.0 for Windows; SPSS Inc.) and R language (a programming language used for statistical computation and graphics). Numeric results are expressed as mean ± SD. In all analyses, a P value of less than 0.05 was considered statistically significant. Comparison of baseline categoric data between the 2 groups was performed using 2-sided χ2 tests, and differences between continuous variables were evaluated using the unpaired t test. Comparison of the New York Heart Association (NYHA) functional class was assessed with the Wilcoxon matched-pairs signed rank test.
A Cox proportional hazards regression analysis was performed to identify independent predictors of cardiac death or sudden death by using variables including age, male sex, ischemic etiology, NYHA functional class, and each pharmacotherapy (ACE inhibitor, ARB, β-blocker, and spironolactone). Similarly, the Δ-123I-MIBG scintigraphic or echocardiographic parameters (% denervation, H/M ratio, WR, LVEDV, LVESV, and LVEF) were included in these analyses. After we recognized the interaction of variables of Δ-scintigraphic or echocardiographic parameters with those at either baseline or follow-up, we determined the variables of Δ to be a model with interaction terms. Moreover, according to the value of Akaike's information criterion (25) and on the basis of clinical judgment and experience, as well as previous studies, variables shown in Tables 1 and 2 were related to the outcome. The event date was the date of the cardiac deaths, and the censoring date was the date of the end of follow-up or the date a patient's medication was changed after a second evaluation.
Univariable and Multivariable Predictors of Cardiac Death
Univariable and Multivariable Predictors of Sudden Death
The cutoff point of Δ-WR was selected to define a large patient group with a low risk of cardiac death or sudden death. Kaplan–Meier survival curves were used for survival comparisons between patient groups stratified according to this cutoff point and compared by log-rank test.
RESULTS
Follow-up Periods
The mean follow-up period was 4.45 ± 1.82 y (0.78–7.48 y) for all study patients, and cardiac death occurred in 56 of the 208 patients (26.9%). The fatal cardiac events in this study occurred an average of 2.15 ± 0.90 y (range, 0.78–5.07 y) after the second evaluation. Progressive heart failure death accounted for 38 (68%) of the deaths, whereas 13 deaths were sudden (23%) and the remaining 5 (9%) were because of myocardial infarction.
Comparison of Clinical Characteristics, 123I-MIBG Scintigraphic and Echocardiographic Parameters, and Pharmacotherapy Between the Non–Cardiac Death Group and the Cardiac Death Group
Clinical characteristics and scintigraphic and echocardiographic parameters of the study patients who had and did not have a cardiac death are shown in Table 3. Age, sex, ischemic etiology, and NYHA functional class were similar in both groups. With respect to pharmacotherapy in the 2 groups, only the use of β-blocker in the non–cardiac death group was significantly higher than in the cardiac death group.
Clinical Characteristics of Patients Who Had and Who Did Not Have Cardiac Death
In the baseline 123I-MIBG scintigraphic parameters, the H/M ratio in the non–cardiac death group was significantly higher than that in the cardiac death group. The WR in the non–cardiac death group was significantly lower than that in the cardiac death group. In the follow-up 123I-MIBG scintigraphic parameters, second % denervation and second WR in the non–cardiac death group were significantly lower than those in the cardiac death group. The second H/M ratio in the non–cardiac death group was significantly higher than that in the cardiac death group. With respect to the changes in imaging parameters between the first and second 123I-MIBG scintigraphy, Δ-% denervation and Δ-WR in the non–cardiac death group were significantly lower than those in the cardiac death group. The Δ-H/M ratio in the non–cardiac death group was significantly higher than that in the cardiac death group.
For the baseline echocardiographic parameters, the LVEF in the non–cardiac death group was significantly higher than that in the cardiac death group. In the follow-up echocardiographic parameters, second LVEDV and second LVESV in the non–cardiac death group were significantly lower than those in the cardiac death group. The second LVEF in the non–cardiac death group was significantly higher than that in the cardiac death group. With respect to the changes in the echocardiographic parameters, Δ-LVEDV and Δ-LVESV in the non–cardiac death group were significantly lower than those in the cardiac death group. Furthermore, the Δ-LVEF in the non–cardiac death group was significantly higher than that in the cardiac death group.
Univariable and Multivariable Predictors of Cardiac Death
Table 1 shows the results of univariable and multivariable Cox proportional hazards model analyses for cardiac death. In the univariable analysis, β-blocker use, Δ-% denervation, Δ-H/M ratio, Δ-WR, Δ-LVESV, and Δ-LVEF were predictive factors. In the multivariable analysis, Δ-WR was the only incremental predictor of cardiac death.
Comparison of Clinical Characteristics, 123I-MIBG Scintigraphic and Echocardiographic Parameters, and Pharmacotherapy Between Non–Sudden Death and Sudden Death Groups
Clinical characteristics and scintigraphic and echocardiographic parameters of the patients who had and did not have a sudden death are shown in Table 4. Age, sex, ischemic etiology, NYHA functional class, and pharmacotherapy were similar in both groups.
Clinical Characteristics of Patients Who Had and Who Did Not Have Sudden Death
In the baseline 123I-MIBG scintigraphic parameters, the WR in the non–sudden death group was significantly lower than that in the sudden death group. In the follow-up 123I-MIBG scintigraphic parameters, second % denervation and second WR in the non–sudden death group were significantly lower than those in the sudden death group. The second H/M ratio in the non–sudden death group was significantly higher than that in the sudden death group. With respect to the changes in imaging parameters between the first and second 123I-MIBG scintigraphy, Δ-% denervation and Δ-WR in the non–sudden death group were significantly lower than those in the sudden death group. The Δ-H/M ratio in the non–sudden death group was significantly higher than that in the sudden death group.
For the baseline echocardiographic parameters, the LVEF in the non–sudden death group was significantly higher than that in the sudden death group. In the follow-up echocardiographic parameters, second LVEDV and second LVESV in the non–sudden death group were significantly lower than those in the sudden death group. The second LVEF in the non–sudden death group was significantly higher than that in the sudden death group. With respect to the changes in the echocardiographic parameters, Δ-LVEDV and Δ-LVESV in the non–sudden death group were significantly lower than those in the sudden death group.
Univariable and Multivariable Predictors of Sudden Death
Table 2 shows the results of univariable and multivariable Cox proportional hazards model analyses for sudden death. In the univariable analysis, β-blocker use and Δ-WR were predictive factors. In the multivariable analysis, Δ-WR was the only incremental predictor of sudden death.
Kaplan–Meier Survival Analysis
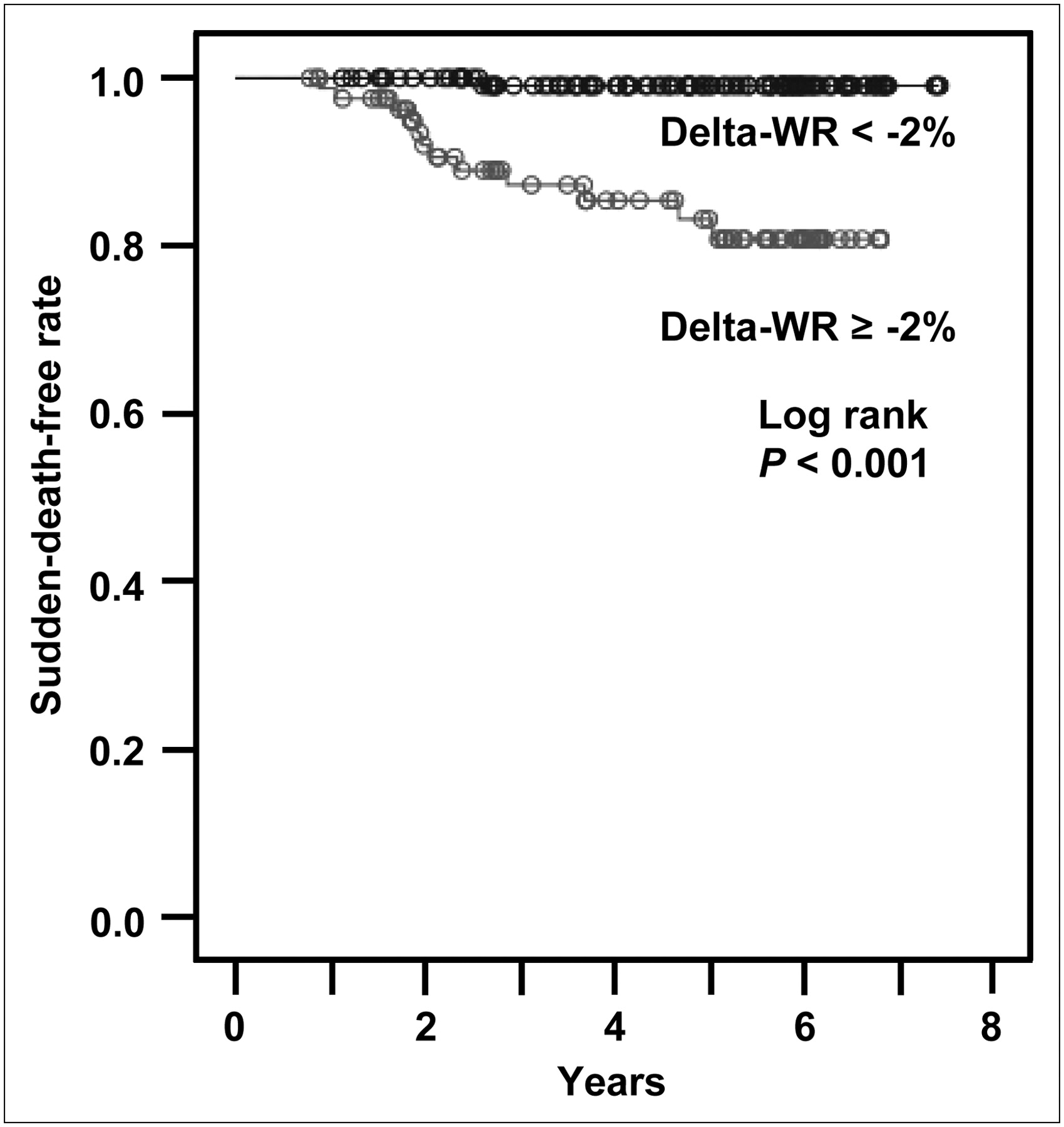
We examined the sensitivity and specificity of various cutoff values of Δ-WR for predicting cardiac death or sudden death. Optimal cutoff was defined as the threshold where the sum of sensitivity and specificity was maximal. The best values of Δ-WR for cardiac death and sudden death with the highest sensitivity and specificity were −5% and −2%, respectively. Figure 2 shows that the cardiac death–free rate was significantly higher in the patients with a Δ-WR less than −5% than in those with a Δ-WR greater than or equal to −5%. Figure 3 shows that the sudden death–free rate was significantly higher in the patients with a Δ-WR less than −2% than in those with a Δ-WR greater than or equal to −2%.
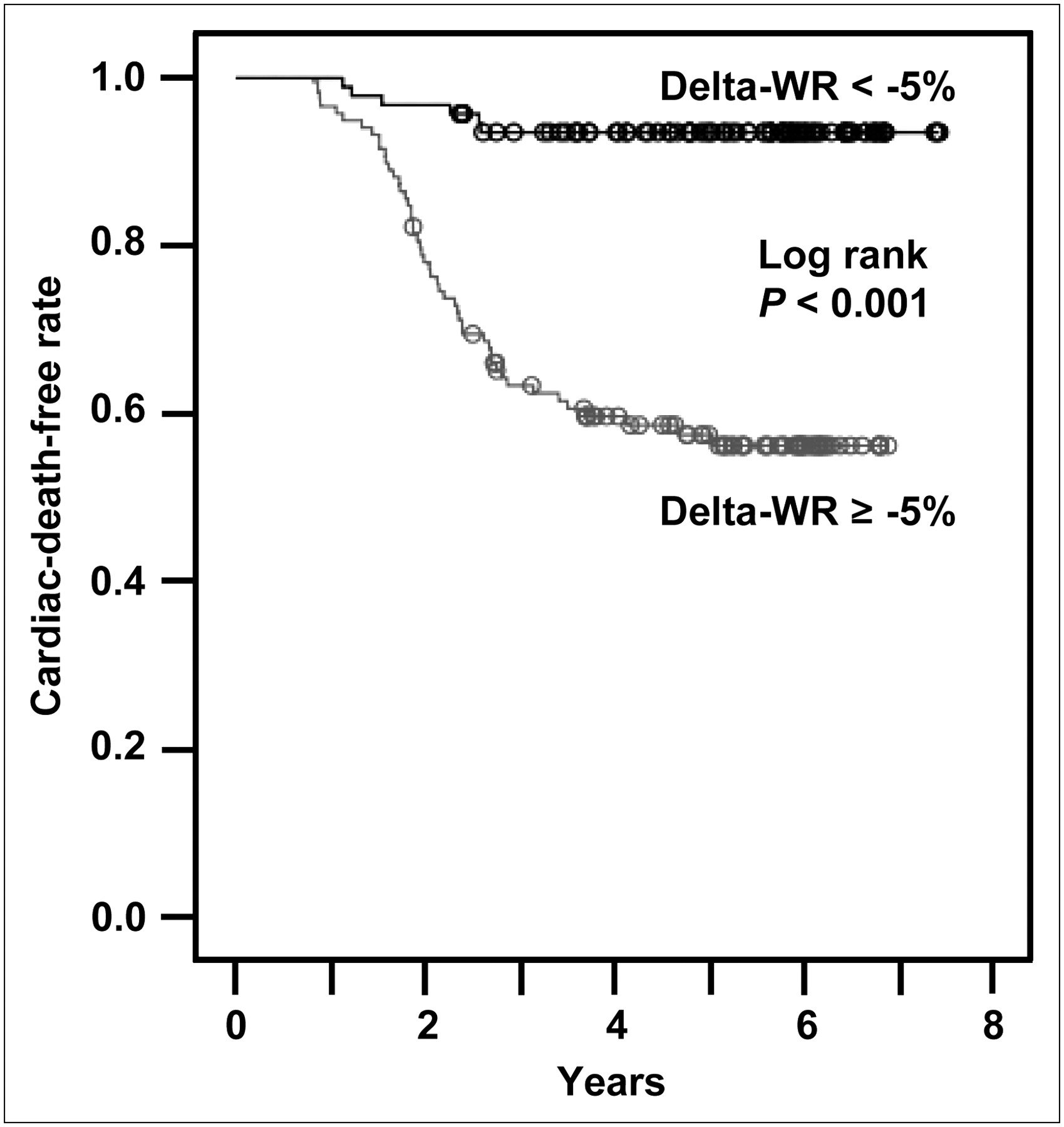
Kaplan–Meier survival curves of cardiac death–free rates in patients with CHF divided into 2 groups according to Δ-WR. Patients with Δ-WR greater than or equal to −5% had significantly greater cardiac death rates than their counterparts (P < 0.001).
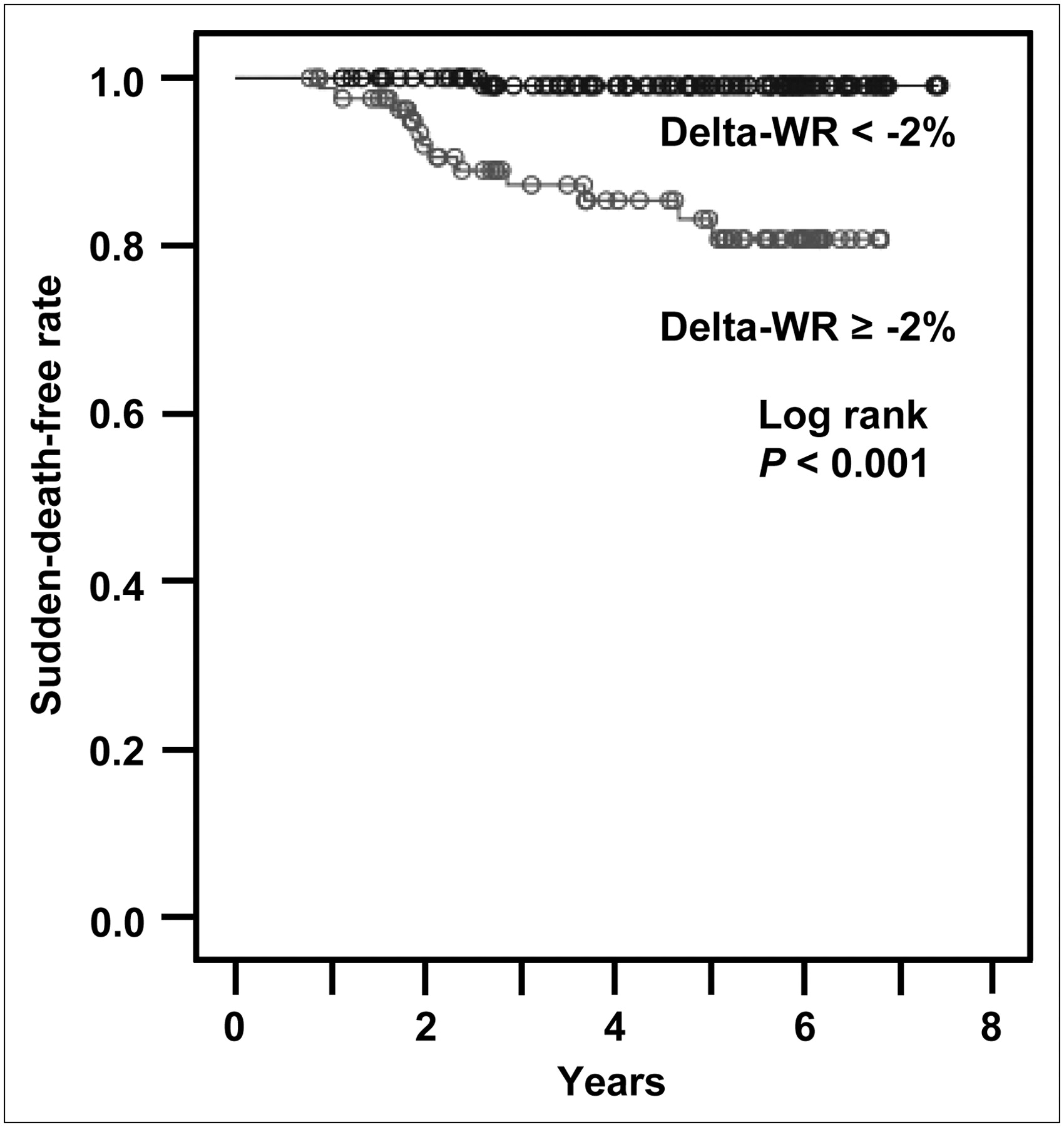
Kaplan–Meier survival curves of sudden death–free rates in patients with CHF divided into 2 groups according to Δ-WR. Patients with Δ-WR greater than or equal to −2% had significantly greater sudden death rates than their counterparts (P < 0.001).
DISCUSSION
During the follow-up period, 56 patients died of cardiac death. The Δ-WR obtained by serial 123I-MIBG scintigraphy in patients with CHF was significantly lower in the non–cardiac death group (n = 152) than in the cardiac death group (n = 56). The multivariable Cox proportional hazards model analysis showed that the Δ-WR was an independent predictor of cardiac death. The cardiac death–free rate was significantly higher in the patients with a Δ-WR less than −5% than in those with a Δ-WR greater than or equal to −5%. In this study, we also evaluated the usefulness of serial 123I-MIBG scintigraphy for predicting sudden death in patients with CHF. Sudden death during the follow-up period occurred in 13 of the 56 patients with cardiac death. The multivariable Cox proportional hazards model analysis showed that the Δ-WR was the only independent predictor of sudden death. Furthermore, the sudden death–free rate was significantly higher in the patients with a Δ-WR less than −2% than in those with a Δ-WR greater than or equal to −2%.
123I-MIBG is an analog of the adrenergic-neuronal–blocking agent guanethidine, which is thought to use the same myocardial uptake and release mechanisms as norepinephrine (26). Because the myocardial norepinephrine concentration and 123I-MIBG uptake are correlated in patients with CHF (27), cardiac 123I-MIBG imaging may be a useful tool for detecting abnormalities of the myocardial adrenergic nervous system in these patients (3,4).
The cardiac sympathetic nerve activity evaluated by 123I-MIBG scintigraphy also has useful prognostic value in patients with CHF (4,5). Merlet et al. (4) reported that the delayed H/M ratio was the best predictor of survival in 90 patients with CHF with reduced cardiac function. Moreover, a multicenter trial from Imamura et al. (5) concluded that the WR was a powerful predictor of subsequent mortality and morbidity in 171 patients with CHF. Kioka et al. (7) also reported that abnormal WR can predict sudden death in 97 patients with mild-to-moderate CHF. However, in those studies (4,5,7), a one-time 123I-MIBG scintigraphic study was evaluated for prognosis of cardiac death or sudden death, despite reports that have suggested, on the basis of cardiac 123I-MIBG scintigraphic findings, that treatment for CHF with ACE inhibitors (8,9,16), ARBs (13,15,17,20), β-blockers (9,10,19), spironolactone (11,12,20), or torasemide (18) can improve cardiac sympathetic nerve activity. In our study, we found that the Δ-WR evaluated by serial scans can be useful for predicting not only cardiac death but also sudden death in 208 patients with CHF. Therefore, serial 123I-MIBG scintigraphic studies may be useful for making decisions about implantable cardioverter defibrillator therapy. Furthermore, our findings demonstrate for, what is to our knowledge, the first time that serial 123I-MIBG scintigraphy has greater prognostic value than a one-time scan in stabilized patients with CHF. From the viewpoint of daily practice, it is ideal to determine the prognosis not by the serial 123I-MIBG but by a one-time scan. However, our data suggest that serial 123I-MIBG shows better predicative value than a one-time scan. The evaluation of cardiac sympathetic nerve activity by 123I-MIBG soon after recovery from the first scan may not give us sufficient information, though, probably because of the instability of cardiac sympathetic nerve activity. In fact, 10 patients met the entry criteria but deteriorated and died before second evaluations.
Although a decline of the cardiac death–free rate was not observed before 0.78 y even in the patients with a high Δ-WR, only a few cardiac deaths occurred after 1.5 y, according to our Kaplan–Meier survival analysis. This result is explained by the exclusion of the patients with severe heart failure and the patients who had hard events after the first evaluation. Thus, the patients in our study were initially likely to be stable. Although the reason for the decline of the cardiac event–free rate after that point is not certain, we speculate that cardiac remodeling of the high Δ-WR group patients cannot be ameliorated by the medical treatment.
The H/M ratio determined by 123I-MIBG scintigraphy was higher in our study than in the study by Merlet et al. (4). In general, the 123I-MIBG used in Japan had a higher specific activity (1,665–2,035 MBq/mg) than that of other 123I-MIBG provided by CIS BIO-International (6); thus, the control value of the H/M ratio was significantly higher in our laboratory (n = 10) (19) than in Merlet's (n = 12) (4) (244 ± 26 vs. 196 ± 33; P < 0.001, evaluated unpaired t test). Although no-carrier-added 123I-MIBG scintigraphy with a greater specific activity has been tested in animal models of heart failure in Europe (28), such research has not been performed in Japan.
It is well known that structural remodeling of the heart promotes the progression of heart failure (29). Thus, an increased left ventricular volume (30) and a decreased cardiac function (31) have been shown to be independent predictors of cardiac death in the failing human heart. In the present study, univariable Cox proportional hazards regression analysis identified Δ-LVESV and Δ-LVEF obtained from serial echocardiographic data as the significant predictors. However, multivariable analysis did not identify these echocardiographic parameters as independent predictors of cardiac death. Moreover, in the Seattle Heart Failure Model, NYHA functional status was good information for predicting cardiac death or sudden death in patients with CHF (32,33). In this study, though, functional status was not a significant predictor of cardiac death. Such discrepancies may be partly due to differences in the patient population in our study compared with previous studies (30–33), particularly a difference in the severity of heart failure. In our study, we evaluated prognosis in stabilized patients with mild-to-moderate CHF; patients with severe heart failure requiring mechanical support or heart transplantation were excluded. Therefore, in the future, we need to evaluate the role of parameters identified in this study in predicting the long-term prognosis in patients with CHF, including those patients with severe heart failure.
Study Limitations
The small number of patients with CHF enrolled proved to be a limitation of the present study. In general, pharmacotherapy for CHF has advanced considerably in recent years as clinical trials have demonstrated favorable long-term effects of ACE inhibitors (34,35), ARBs (36,37), β-blockers (38,39), and spironolactone (40) on morbidity and mortality. In our study, only β-blocker therapy was identified as an independent predictor of cardiac death by univariable Cox proportional hazards regression analysis; however, it was not identified by multivariable analysis. Accordingly, we need to evaluate long-term prognosis in patients with CHF in a larger number of patients in the future.
In addition, this study included the patients with heart failure caused by various etiologies (ischemic and nonischemic heart disease). There was no significant difference in our results between the non–cardiac death group and the cardiac death group. Moreover, ischemic etiology was not a significant predictor of cardiac death. 123I-MIBG scintigraphy is useful in predicting cardiac death in patients with CHF, irrespective of its etiology. However, further studies are required to confirm this hypothesis.
CONCLUSION
The Δ-WR obtained by serial 123I-MIBG scintigraphy in patients with CHF was significantly lower in the non–cardiac death group than that in the cardiac death group. The multivariable Cox proportional hazards model analysis showed that the Δ-WR was the only independent predictor of cardiac death. Moreover, this parameter was also useful for predicting sudden death in patients with CHF. These findings indicate that serial 123I-MIBG scintigraphy can be useful for predicting cardiac death and sudden death in stabilized patients with CHF.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 23, 2007.
- Accepted for publication February 26, 2008.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparative effects of long-acting and short-acting loop diuretics on cardiac sympathetic nerve activity in patients with chronic heart failure
- An Electrophysiologist Perspective on Risk Stratification in Heart Failure: Can Better Understanding of the Condition of the Cardiac Sympathetic Nervous System Help?
- 2013 ACCF/ACR/ASE/ASNC/SCCT/SCMR Appropriate Utilization of Cardiovascular Imaging in Heart Failure: A Joint Report of the American College of Radiology Appropriateness Criteria Committee and the American College of Cardiology Foundation Appropriate Use Criteria Task Force
- Assessment of cardiac sympathetic activity by MIBG imaging in patients with heart failure: a clinical appraisal
- Advances in SPECT and PET for the management of heart failure
- Iodine-123 Metaiodobenzylguanidine Imaging and Carbon-11 Hydroxyephedrine Positron Emission Tomography Compared in Patients With Left Ventricular Dysfunction
- 123I-Metaiodobenzylguanidine Imaging in the Era of Implantable Cardioverter Defibrillators: Beyond Ejection Fraction
- Recent Developments in Heart Failure Imaging
- Myocardial Sympathetic Innervation and Long-Term Left Ventricular Mechanical Unloading
- Cardiac Sympathetic Imaging With mIBG in Heart Failure