


Abstract
The activation of the renin-angiotensin-aldosterone system (RAAS) prevents the uptake of norepinephrine in the myocardium. Atrial natriuretic peptide (ANP), a circulating hormone of cardiac origin, has vasodilatory and diuretic properties and can inhibit the RAAS. However, its effect on cardiac sympathetic nerve activity has not been determined. Methods: We studied 58 patients with decompensated nonischemic acute heart failure who were treated with intravenous low-dose dopamine and diuretics. Twenty-nine patients (group A) were assigned to also receive intravenous ANP, whereas the remaining 29 patients (group B) continued their established drug regimen. The dopamine or ANP was continuously infused for >96 h. The left ventricular end-diastolic volume and ejection fraction were determined by echocardiography before and 4 wk after treatment. The delayed heart-to-mediastinum (H/M) count ratio, delayed total defect score, and washout rate were determined from 123I-metaiodobenzylguanidine (MIBG) images 3 wk after treatment. Results: Fifty-six patients enrolled in the trial completed the entire protocol. After treatment of group A (n = 28), the left ventricular end-diastolic volume decreased from 186 ± 42 to 174 ± 48 mL (P < 0.05), and left ventricular ejection fraction increased from 32% ± 9% to 36% ± 7% (P < 0.05). In group B (n = 28), these parameters did not change significantly. In addition, 3 wk after treatment of group A, the total defect score was significantly lower (30 ± 9 vs. 38 ± 9, P < 0.01), the H/M count ratio was significantly higher (1.86 ± 0.21 vs. 1.62 ± 0.23, P = 0.0001), and washout rate was significantly lower (42% ± 12% vs. 49% ± 12%, P < 0.05) than in group B. Conclusion: The present study demonstrates an improvement in echocardiographic parameters with ANP infusion. In addition, cardiac 123I-MIBG scintigraphic parameters were better in patients who received ANP infusion along with dopamine and diuretics than in patients who received standard conventional therapy. These findings indicate that intravenous administration of ANP can benefit cardiac sympathetic nerve activity and improve left ventricular remodeling in patients with acute heart failure.
In addition to its natriuretic, diuretic, and vasodilatory properties, atrial natriuretic peptide (ANP) can modulate the autonomic nervous system by sensitizing arterial and cardiac baroreceptor afferent nerve endings, thus inhibiting sympathetic ganglionic neurotransmission by a central neural action (1–7). Moreover, ANP has a wide range of potent biologic effects, including inhibition of the renin-angiotensin-aldosterone system (RAAS) (8). The efficacy of long-term administration of ANP to patients with acute heart failure has been reported previously (9). In that report, hemodynamic measurements significantly improved during ANP infusion, without the development of tolerance, in patients with acute heart failure.
Myocardial imaging with 123I-metaiodobenzylguanidine (MIBG), an analog of norepinephrine, is a useful tool for detecting abnormalities of the myocardial adrenergic nervous system in patients with congestive heart failure (CHF) (10–15). An association between the myocardial norepinephrine concentration and 123I-MIBG uptake in patients with nonischemic CHF has been reported (13). However, there have been no reports on changes in cardiac 123I-MIBG scintigraphic findings in response to long-term administration of ANP to patients with CHF. However, ANP treatment has been reported to improve muscle sympathetic activity in patients with CHF (16). In the present study, we evaluated the effects of intravenous ANP on cardiac sympathetic nerve activity in patients with CHF.
MATERIALS AND METHODS
Study Population
From December 2000 through May 2003, 58 patients were admitted to the intensive care unit of our institutions with a first episode of acute heart failure (New York Heart Association [NYHA] class III or IV). Patients with a history of myocardial infarction or coronary artery disease or who required mechanical support (intraaortic balloon pumping, mechanical ventilation, or both) were excluded from the study. None of the patients had a history of heart failure. The study was approved by the ethics review board of our institution, and written informed consent was obtained from all patients.
Study Protocol
After admission to the intensive care unit, low-dose dopamine was started at 2 or 3 μg/kg/min and furosemide was also started. After hemodynamic stability was established, 29 patients (group A) were randomized to receive ANP at 25 ng/kg/min in addition to standard therapy, and the remaining 29 patients (group B) continued their established drug regimen. If the systolic blood pressure was high (>150 mm Hg) or low (<90 mm Hg), the doses of dopamine or ANP were adjusted to maintain a constant blood pressure. The dopamine or ANP was continuously infused for >96 h (mean ± SD: 7 ± 2 d in group A; 8 ± 2 d in group B). After intravenous dopamine and ANP were stopped, all patients received angiotensin-converting enzyme inhibitors and diuretics.
Hemodynamic Measurements
The right heart was catheterized using a 7-French Swan–Ganz catheter. Hemodynamic measurements were performed before and 48 h after the infusion began. Right atrial pressure, mean pulmonary arterial pressure, and pulmonary capillary wedge pressure were determined from a transducer connected to the Swan–Ganz catheter. The cardiac index was determined by thermodilution.
We reexamined with right heart catheterization 2 wk later (when patients were receiving only oral drugs). All these parameters were determined again.
Echocardiography
Echocardiographic measurements were performed soon after admission and 4 wk after treatment using standard methods in a masked manner. Two independent, experienced echocardiographers who had no knowledge of the study performed all measurements. Left ventricular end-diastolic volume, end-systolic volume, and ejection fraction were calculated using the modified Simpson method (17).
123I-MIBG Imaging
123I-MIBG imaging was performed 3 wk after treatment, using a previously described method (18–21). The 123I-MIBG was obtained commercially (Daiichi Radioisotope Laboratories). Patients were injected intravenously with 123I-MIBG (111 MBq) while they were supine. Anterior planar and SPECT images were acquired 15 min after injection and repeated 4 h later. SPECT was performed with a dedicated single-head system (Millennium MPR; General Electric Medical Systems). Energy, uniformity, and linearity were continuously corrected. Images were acquired for 40 s each at 32 steps over a 180° orbit and were recorded at a digital resolution of 128 × 128 pixels from the anterior planar 123I-MIBG image.
The heart-to-mediastinum (H/M) count ratio was determined from the anterior planar delayed 123I-MIBG image. The washout rate was calculated using the following formula: {([H] − [M])early − ([H] − [M])delayed}/([H] − [M])early × 100 (%), where [H] = mean count per pixel in the left ventricle and [M] = mean count per pixel in the upper mediastinum. In our laboratory, the reference range for delayed H/M count ratio is 2.00–2.80, and the reference range for washout rate is 22%–32%. (These data were obtained from 16 healthy volunteers.)
The delayed myocardial SPECT images for each patient were divided into 20 segments. The short-axis images at the basal, middle, and apical ventricular levels were divided into 6 segments. The apical segment of the vertical long-axis image was divided into 2 segments. Regional tracer uptake was assessed semiquantitatively using a 4-point scoring system (0 = normal uptake; 1 = mildly reduced uptake; 2 = moderately reduced uptake; 3 = severely reduced uptake). The total defect score was calculated as the sum of the scores for all 20 segments.
Interobserver variability was determined by 2 independent observers who had no knowledge of the clinical status or medical therapy of the patients. The interobserver correlation was highly significant (r = 0.90; P < 0.001).
Data Analysis and Statistics
Statistical analysis was performed using StatView (Abacus Concepts) for Macintosh (Apple Computer, Inc.). Numeric results are expressed as the mean ± SD. Comparison of baseline categoric data between the 2 groups was by the χ2 test. Differences between continuous variables were evaluated using the unpaired Student t test. Changes in NYHA functional class were assessed using the Wilcoxon matched-pairs signed rank test. The intragroup effects of chronic treatment were assessed by the paired t test and by ANOVA to compare intergroup changes. A value of P < 0.05 was considered statistically significant.
RESULTS
There were no significant differences in the clinical characteristics of the 2 groups (Table 1). In group A, 1 patient had a cerebral hemorrhage, and in group B, 1 patient died from arrhythmia 6 d after admission. Therefore, 56 of 58 patients (32 men, 24 women; mean age, 65 ± 11 y; age range, 37–85 y) who had enrolled in the trial completed the entire protocol. The cause of heart failure was dilated cardiomyopathy in 36 patients, valvular heart disease in 13, and hypertensive heart disease in 7. The average infusion dose of dopamine was 3.0 ± 0.9 μg/kg/min in group A (n = 28) and 2.9 ± 0.8 μg/kg/min in group B (n = 28). The average infusion dose of ANP was 29 ± 11 ng/kg/min in group A (n = 28).
Demographics and Clinical Characteristics
For 30 patients (15 patients each in groups A and B), the hemodynamic parameters were evaluated by Swan–Ganz catheter at baseline and at 48 h after the infusion began (Table 2). In group A, right atrial pressure decreased significantly after 48 h of treatment (7.1 ± 4.5 mm Hg), compared with the baseline value (10.6 ± 4.8 mm Hg) (P < 0.05). In contrast, in group B, the values at baseline and after treatment did not significantly differ. In group A, mean pulmonary arterial pressure decreased significantly after 48 h of treatment (23.1 ± 6.3 mm Hg), compared with the baseline value (28.5 ± 7.8 mm Hg) (P < 0.05). In contrast, in group B, the values at baseline and after treatment did not significantly differ. In group A, pulmonary capillary wedge pressure decreased significantly after 48 h of treatment (14.5 ± 2.8 mm Hg), compared with the baseline value (21.4 ± 5.8 mm Hg) (P < 0.001). In contrast, in group B, the values at baseline and after treatment did not significantly differ. Furthermore, after 48 h of treatment, pulmonary capillary wedge pressure was significantly lower in group A than in group B (P < 0.05). In group A, cardiac index increased significantly after 48 h of treatment (2.54 ± 0.58 L/min/m2), compared with the baseline value (2.04 ± 0.60 L/min/m2) (P < 0.05). In contrast, in group B, the values at baseline and after treatment did not significantly differ.
Hemodynamic Findings of Right Heart Catheterization
However, 2 wk after treatment, there were no significant differences in the hemodynamic parameters (right atrial pressure, mean pulmonary arterial pressure, pulmonary capillary wedge pressure, and cardiac index) between the 2 groups (Table 3).
Hemodynamic Findings of Right Heart Catheterization After 2 Weeks
The left ventricular end-diastolic volume, end-systolic volume, and ejection fraction are reported in Table 4. In group A, left ventricular end-diastolic volume decreased significantly after 4 wk (174 ± 48 mL), compared with the baseline value (186 ± 42 mL) (P < 0.05). In contrast, in group B, the values at baseline and after 4 wk of treatment did not significantly differ. In group A, left ventricular end-systolic volume decreased significantly after 4 wk (112 ± 41 mL), compared with the baseline value (128 ± 43 mL) (P < 0.01). In contrast, in group B, the values at baseline and after 4 wk of treatment did not significantly differ. In group A, left ventricular ejection fraction increased significantly after 4 wk (36% ± 7%), compared with the baseline value (32% ± 9%) (P < 0.05). In contrast, in group B, the values at baseline and after 4 wk of treatment did not significantly differ.
Changes in LVEDV, LVESV, LVEF, and Functional Class
The NYHA functional class of the patients is summarized in Table 4. The functional class of the patients of both groups improved after treatment, compared with the baseline values (in group A, P < 0.0001; in group B, P < 0.01). After treatment, the NYHA functional class was better for group A than for group B (P < 0.05).
The total defect score, H/M count ratio, and washout rate are summarized in Table 5 and Figure 1. 123I-MIBG imaging was performed only 3 wk after treatment. The total defect score was significantly lower in group A than in group B (30 ± 9 vs. 38 ± 9, P < 0.01). The H/M count ratio was significantly higher in group A than in group B (1.86 ± 0.21 vs. 1.62 ± 0.23, P = 0.0001). Furthermore, the washout rate was significantly lower in group A than in group B (42% ± 12% vs. 49% ± 12%, P < 0.05). Representative 123I-MIBG images for both groups after treatment are shown in Figures 2 and 3.
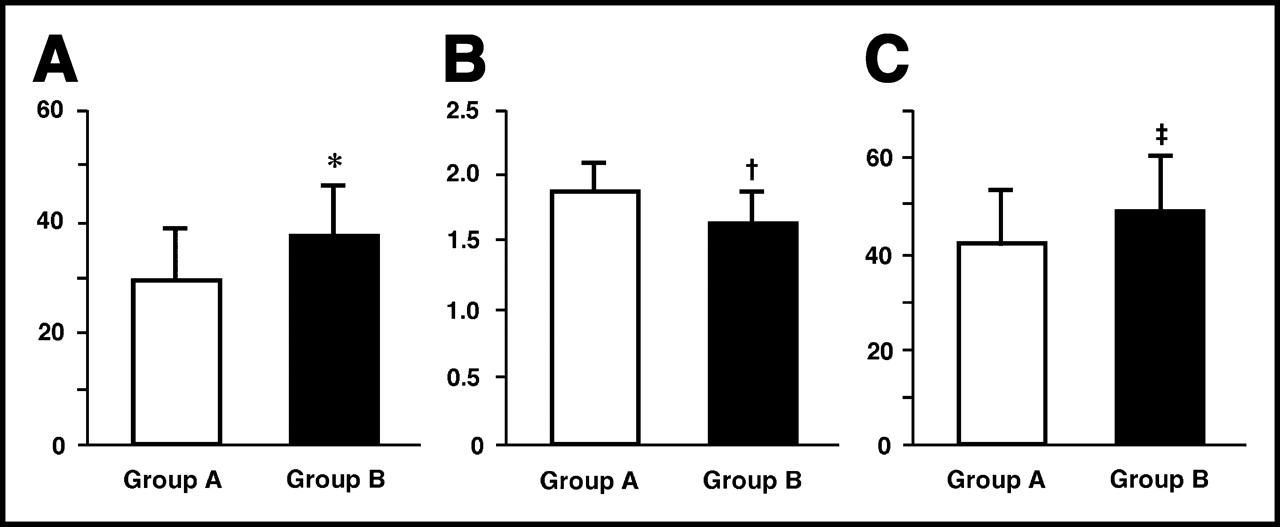
Comparison of cardiac 123I-MIBG scintigraphic findings for total defect score (A), H/M count ratio (B), and washout rate (C) 3 wk after treatment. *P < 0.01 compared with group A; †P = 0.0001 compared with group A; ‡P < 0.05 compared with group A.

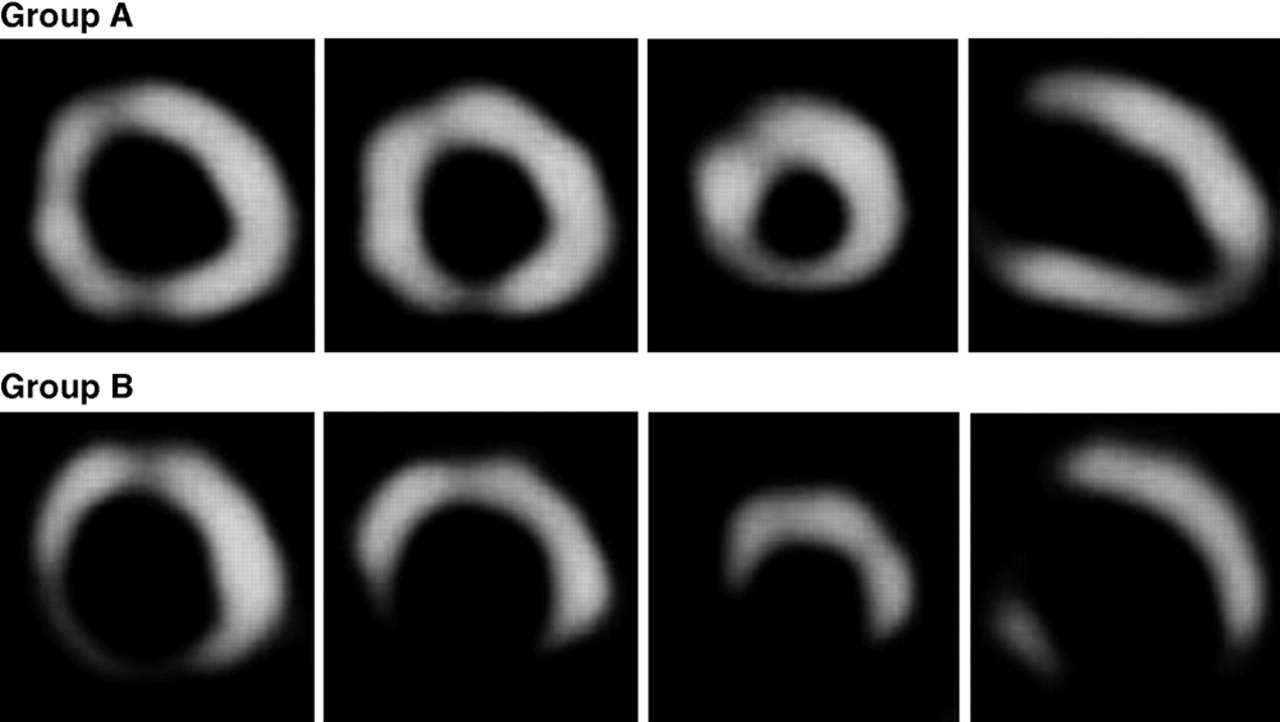
Representative SPECT 123I-MIBG images 3 wk after treatment for both groups.

Representative anterior planar delayed 1123I-MIBG images 3 wk after treatment for both groups. In these 2 examples, delayed H/M count ratio and washout rate were 1.94 and 40%, respectively, for a patient from group A and 1.48 and 53%, respectively, for a patient from group B.
Cardiac 123I-MIBG Scintigraphic Findings
DISCUSSION
ANP, a circulating hormone of cardiac origin, has vasodilatory and diuretic properties and can inhibit the RAAS (8). Kitashiro et al. (9) reported that long-term continuous ANP infusion is clinically useful in patients with severe acute heart failure. In that study, hemodynamic measurements evaluated by Swan–Ganz catheter significantly improved during ANP infusion. In this study, a marked improvement in hemodynamic indices, characterized by decreases in right atrial pressure, mean pulmonary arterial pressure, and pulmonary capillary wedge pressure and an increase in cardiac index, were observed after ANP infusion began. These data indicate that continuous ANP infusion benefited left ventricular performance, without the development of tolerance, in patients with severe acute heart failure. However, 2 wk after treatment, these hemodynamic parameters did not significantly differ between the 2 groups. Therefore, addition of ANP infusion therapy may improve hemodynamic parameters more immediately than does standard conventional therapy in patients with acute heart failure.
The activation of the RAAS promotes structural remodeling of the heart and progression of heart failure (22,23). An increase in the left ventricular ejection fraction has been identified as a marker of beneficial left ventricular remodeling that is manifested as a reduced chamber volume (24). This structural effect is associated with an improvement in survival (25). Saito et al. (26) reported that ANP infusion improves left ventricular function in patients with heart failure. In our study, left ventricular volume and cardiac function evaluated by echocardiography were significantly improved by ANP infusion, compared with the standard conventional therapy. Furthermore, we evaluated other echocardiographic data, including mitral regurgitation and diastolic parameters (E/A ratio [the mitral ratio of peak early to late diastolic filling velocity] and deceleration time). Although a marked improvement was observed in these parameters in both groups, there were no significant differences in intergroup changes (data not shown). Moreover, ANP treatment also improved the symptoms of heart failure, as measured by changes in the NYHA functional class.
123I-MIBG, an analog of the adrenergic-neuron–blocking agent guanethidine, is thought to use the same mechanism of myocardial uptake and release as norepinephrine (27). The myocardial norepinephrine concentration and 123I-MIBG uptake have been shown to correlate in patients with CHF (13). Therefore, cardiac 123I-MIBG imaging is a useful tool for detecting abnormalities of the myocardial adrenergic nervous system in patients with CHF (10–15). Furthermore, myocardial uptake of 123I-MIBG has been shown to be a strong prognostic marker for overall mortality in patients with CHF (14). In patients with nonischemic cardiomyopathy, a large proportion of the decrease in uptake of norepinephrine is probably due to loss of neuronal norepinephrine uptake in the failing myocardium. However, some of the reduction in norepinephrine uptake appears to be functional and reversible and is mediated by hormonal factors, including angiotensin and aldosterone. Struthers et al. (28,29) reported that once norepinephrine is taken up into cardiac cells, it is rapidly metabolized and inactivated so that uptake is equivalent to local disposal in the myocardium. Therefore, several reports have suggested that inhibition of the RAAS can improve cardiac sympathetic nerve activity, based on cardiac 123I-MIBG scintigraphic studies, in patients with heart failure (19–21,30,31).
It is known that ANP inhibits the RAAS and sympathetic nerve systems (16). However, there are no reports on cardiac 123I-MIBG scintigraphic findings in response to long-term administration of ANP in patients with CHF. In this study, the total defect score, H/M count ratio, and washout rate determined by cardiac 123I-MIBG scintigraphy were better in patients treated with ANP than in patients treated with standard conventional therapy. Therefore, long-term administration of ANP may mediate its effect by increasing myocardial uptake of norepinephrine. We did not evaluate 123I-MIBG scintigraphy at baseline. Because clinical status in patients with heart failure before treatment was of NYHA III or IV severity, we could not evaluate 123I-MIBG scintigraphy at baseline. However, before treatment, no clinical characteristics, hemodynamics, or echocardiographic parameters differed significantly between the 2 groups. Therefore, we speculate that ANP infusion can benefit cardiac sympathetic nerve activity in patients with acute heart failure.
In this study, delayed 123I-MIBG images were used to determine the total defect score and H/M count ratio. There are 2 types of norepinephrine and 123I-MIBG uptake. Uptake-1 (neuronal uptake), which takes place even if the concentration of norepinephrine or 123I-MIBG is low, depends on sodium and adenosine triphosphate and is suppressed by tricyclic antidepressants. Uptake-2 (extraneuronal uptake), which takes place only when the concentration is high, represents simple diffusion and is unaffected by tricyclic agents (32–34). Early images result from both the uptake-1 mechanism and the uptake-2 mechanism (35,36), whereas delayed images are less dependent on uptake-2 and therefore more accurately reflect cardiac sympathetic nerve activity. Furthermore, because neuronal accumulation of 123I-MIBG reaches a peak 4 h after its administration, neuronal uptake of norepinephrine can be evaluated accurately if 123I-MIBG imaging is performed at that time (36). For these reasons, we used delayed 123I-MIBG imaging in this study.
Recent articles have reported that aldosterone is produced in the ventricles of the failing human heart (37) and that the aldosterone synthase gene is expressed in cardiac tissue (38). Furthermore, ANP has been reported to inhibit aldosterone synthase gene expression in cultured neonatal rat cardiocytes (39). ANP treatment has been shown to decrease the plasma aldosterone concentration (9,26). We did not measure plasma aldosterone or ANP concentrations. However, aldosterone may be produced in cardiac tissue, even if the plasma aldosterone concentration is normal. Therefore, we speculate that it is important to inhibit aldosterone produced in cardiac tissue by the administration of ANP in patients with CHF.
The small number of patients with CHF included in this study was a limitation. In addition, we examined various diseases (dilated cardiomyopathy, valvular heart disease, and hypertensive heart disease) in patients with nonischemic acute heart failure. However, the response to ANP treatment did not significantly differ in patients with idiopathic and other cardiomyopathies. Therefore, we believe that ANP infusion can mediate its effect by increasing myocardial uptake of norepinephrine in patients with acute heart failure irrespective of its etiology.
In our study, hemodynamic parameters (evaluated by Swan–Ganz catheter) and echocardiographic measurements after treatment were slightly better in patients who received ANP infusion than in patients who received standard conventional therapy. We need to study the effects of ANP infusion therapy on cardiac sympathetic nerve activity, cardiac function, and hemodynamic parameters in a larger group of patients.
CONCLUSION
The total defect score, H/M count ratio, and washout rate determined by cardiac 123I-MIBG scintigraphy were better in patients who received ANP infusion along with dopamine and diuretics than in patients who received standard conventional therapy. In addition, left ventricular volume and cardiac function improved with this treatment. These findings indicate that intravenous administration of ANP can benefit cardiac sympathetic nerve activity and improve left ventricular remodeling in patients with acute heart failure.
Footnotes
Received Sep. 19, 2003; revision accepted Jan. 26, 2004.
For correspondence or reprints contact: Shu Kasama, MD, Department of Cardiovascular Medicine, Gunma University School of Medicine, 3-39-15, Showa-machi, Maebashi, Gunma 371-0034, Japan.
E-mail: s-kasama{at}bay.wind.ne.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Value of Serial Cardiac 123I-MIBG Imaging in Patients with Stabilized Chronic Heart Failure and Reduced Left Ventricular Ejection Fraction
- Additive Effects of Spironolactone and Candesartan on Cardiac Sympathetic Nerve Activity and Left Ventricular Remodeling in Patients with Congestive Heart Failure
- Long-Term Nicorandil Therapy Improves Cardiac Sympathetic Nerve Activity After Reperfusion Therapy in Patients with First Acute Myocardial Infarction
- Effects of Intravenous Atrial Natriuretic Peptide on Cardiac Sympathetic Nerve Activity and Left Ventricular Remodeling in Patients With First Anterior Acute Myocardial Infarction
- Effects of torasemide on cardiac sympathetic nerve activity and left ventricular remodelling in patients with congestive heart failure
- Comparative effects of valsartan and enalapril on cardiac sympathetic nerve activity and plasma brain natriuretic peptide in patients with congestive heart failure
- Effects of candesartan on cardiac sympathetic nerve activity in patients with congestive heart failure and preserved left ventricular ejection fraction