


Abstract
The rupture of atherosclerotic vulnerable plaques and subsequent formation of thrombi are the main factors responsible for myocardial and cerebral infarctions. Because macrophage infiltration plays an essential role in plaque rupturing, pharmacologic therapy that reduces macrophage infiltration is required to stabilize the vulnerable plaques. The monitoring of therapeutic effect is important in assessing the therapeutic effects of drugs for individual patients. We previously reported that 18F-FDG accumulates in macrophage-rich plaques. The present study was undertaken to investigate the usefulness of 18F-FDG PET for monitoring therapies that target vascular inflammation. Methods: Myocardial infarction–prone Watanabe heritable hyperlipidemic rabbits were used in this study. The antioxidant probucol was included in the diet fed to 4 rabbits starting at 10 mo of age (probucol group). In a control study, 4 rabbits received standard rabbit chow (control group). 18F-FDG PET experiments were performed on both groups before the study and at 1, 3, and 6 mo after treatment. After the last imaging session, the rabbits were sacrificed at 3 h after injection of 18F-FDG, and the aortas were removed. The accumulated radioactivity was then measured, and the number of macrophages was determined by examination of stained sections. Results: At the age of 10 mo, before the treatment, the aorta could be imaged by 18F-FDG PET in all rabbits. The aorta could not be imaged after 6 mo of probucol treatment, whereas intense radioactivity was observed in the control rabbits throughout the investigation. The standardized uptake values (SUVs) of the aorta were decreased significantly in the probucol group after 3 mo of intervention as compared with the pretreatment period. The SUVs of the control group were increased gradually at 6 mo. Radioactivity in the aorta was significantly lower in the probucol group than that in the control group. Macrophages were already present at the beginning of the study, and probucol treatment for 6 mo resulted in a significant reduction of macrophage infiltration. Conclusion: 18F-FDG PET was able to image the reduction of inflammation by probucol. 18F-FDG PET should be useful for evaluating the therapeutic effect of drugs clinically and for the development of new drugs that can stabilize vulnerable plaques. 18F-FDG PET should be useful for evaluating the therapeutic effect of drugs clinically and for the development of new drugs that can reduce inflammation of vulnerable plaques.
The rupture of atherosclerotic plaque and ensuing thrombus formation are primarily responsible for myocardial and cerebral infarctions (1–3). Atherosclerotic plaques are classified into 2 types, stable and vulnerable, with the latter having a high risk of rupture. Thus, the detection of atherosclerotic plaques prone to rupture is clinically important for risk stratification and to provide early treatment. Inflammation plays an essential role in plaque rupturing, and macrophage infiltration is characteristic of the vulnerable plaques (4). Recently, we and another group have shown that 18F-FDG accumulates in macrophage-rich plaques, and 18F-FDG PET has been suggested to be useful for the selective detection of vulnerable plaques (5–7).
Many drugs have been tested for their ability to stabilize plaque (8), and macrophages are one of the targets of these pharmacologic therapies (9). However, because drug effects vary among individuals, monitoring the therapeutic effect is important for selecting the appropriate drug for individual patients. The present study was undertaken to investigate the usefulness of 18F-FDG PET for monitoring therapies that target vascular inflammation. We used probucol in Watanabe heritable hyperlipidemic rabbits with myocardial infarction (WHHLMI rabbits) (10)—a widely used animal model of atherosclerosis (11,12)—because probucol is an antioxidant known to reduce the extent of macrophage infiltration in atherosclerotic lesions in these rabbits (13). The atherosclerotic plaque of WHHLMI rabbits does not rupture but its pathologic characteristics have been reported to resemble those of the human lesion (10,14,15).
MATERIALS AND METHODS
Animals and Diets
Pure probucol powder was kindly supplied by Daiichi Pharmaceutical Co. Ltd. WHHLMI rabbits bred at Kobe University were used in this study. The animals were fed standard rabbit chow (type RC4; Oriental Yeast Co., Ltd.) until the age of 10 mo. One rabbit was killed under anesthesia with sodium pentobarbital, and the aorta was removed at the beginning of the experiment to be used as a pretreatment control to investigate atherosclerotic lesions of the aorta. Other rabbits were divided into 2 groups. Four rabbits were fed chow (130 g/d) containing 1% (w/w) probucol for 6 mo (probucol group). We chose this dose according to previously published methods (16–19), although this dose is about 20 times higher than the recommended human dose. Four rabbits in the control group were given standard rabbit chow (130 g/d) for 6 mo. Water was available ad libitum for all rabbits. Before drug treatment and at 1, 3, and 6 mo after drug administration, body weight and plasma levels of total, low-density lipoprotein (LDL), and high-density lipoprotein (HDL) cholesterol and triglycerides were evaluated. The Animal Care and Use Committee of the Hamamatsu University School of Medicine approved all experiments.
PET and CT
The animals were fasted for at least 6 h before receiving 18F-FDG. Before the imaging study, the individual body shape was taken with urethane hardening foam to maintain the stereotactic position. 18F-FDG PET and CT experiments were performed at 10 mo of age and after 1, 3, and 6 mo of intervention in both groups according to a previously reported method with slight modification (5). Briefly, the rabbits were anesthetized and 18F-FDG (37–185 MBq) was injected into a marginal ear vein. PET was performed for 15 min at 180 min after injection of 18F-FDG using an ECAT EXACT HR PET scanner (Siemens AG). We chose this time point according to the method of Tawakol et al. (6). After the PET study, a CT angiogram was acquired with an X-force CT scanner (Toshiba Medical Corp.) using iohexol as a contrast agent. PET images were calibrated to the injected dose of 18F-FDG. For measurement of radioactivity in the thoracic aorta, 4 circular regions of interests (ROIs) (3 mm2 for each ROI) were drawn on the aorta. The analysis was undertaken with no knowledge of the animal group. The standardized uptake value (SUV) was calculated by dividing the tissue concentration (kBq/mL) by the injected dose per gram of body weight (kBq/g).
18F-FDG Biodistribution Study
The biodistribution study was performed on the day after the CT and PET study, 6 mo after probucol administration. The rabbits were anesthetized and 18F-FDG (370 MBq) was injected into a marginal ear vein. Three hours after the 18F-FDG injection, the animals were sacrificed with an overdose of sodium pentobarbital. Perfusion fixation was then performed using PLP solution (75 mmol/L l-(+)-lysine hydrochloride and 4% paraformaldehyde in 37.5 mmol/L phosphate buffer, pH 7.4). The thoracic and abdominal aortas were subsequently removed, cut into 10-mm segments, and weighed. The segments were immediately postfixed in PLP solution, and radioactivity was measured with a well-type γ-counter (COBRA; Packard Co. Ltd.). The results are expressed as the differential uptake ratio (DUR):
Histology
Each arterial segment was embedded in paraffin after the radioactivity was measured. Consecutive 4-μm-thick sections were prepared from each segment and the sections were subjected to immunohistochemical staining or azan-Mallory staining. Immunohistochemistry was performed according to the method reported by Tsukada et al. using the rabbit macrophage-specific monoclonal antibody RAM-11 (Dako Corp.) (20). These slices were also costained with hematoxylin for identification of the nucleus. The number of macrophages was determined by counting the nuclei of RAM-11–positive cells in each slice. The intima and whole area were measured on an azan-Mallory–stained consecutive cross-section of RAM-11 staining.
Statistical Analysis
Data are presented as the mean ± SD. Statistical analysis was performed using the Mann–Whitney U test or paired t test for comparisons between or within groups, respectively. Statistical significance was established at P < 0.05.
RESULTS
Body Weight and Lipid Profile
Body weight, plasma levels of cholesterols, and plasma levels of triglycerides in the probucol and control groups are given in Table 1. During the experiments, there was no statistically significant difference in body weight between or within the groups. No significant difference was seen in the plasma concentrations of total, LDL, and HDL cholesterol or triglycerides between the probucol and control groups. Total plasma cholesterol levels decreased over the 6 mo of intervention in both groups compared with the levels at the beginning of the study, although the differences were not significant at 3 and 6 mo in the probucol group.
Effect of Probucol Treatments on Body Weight and on Plasma Levels of Total, LDL, and HDL Cholesterol and Triglycerides in WHHLMI Rabbits
PET Study
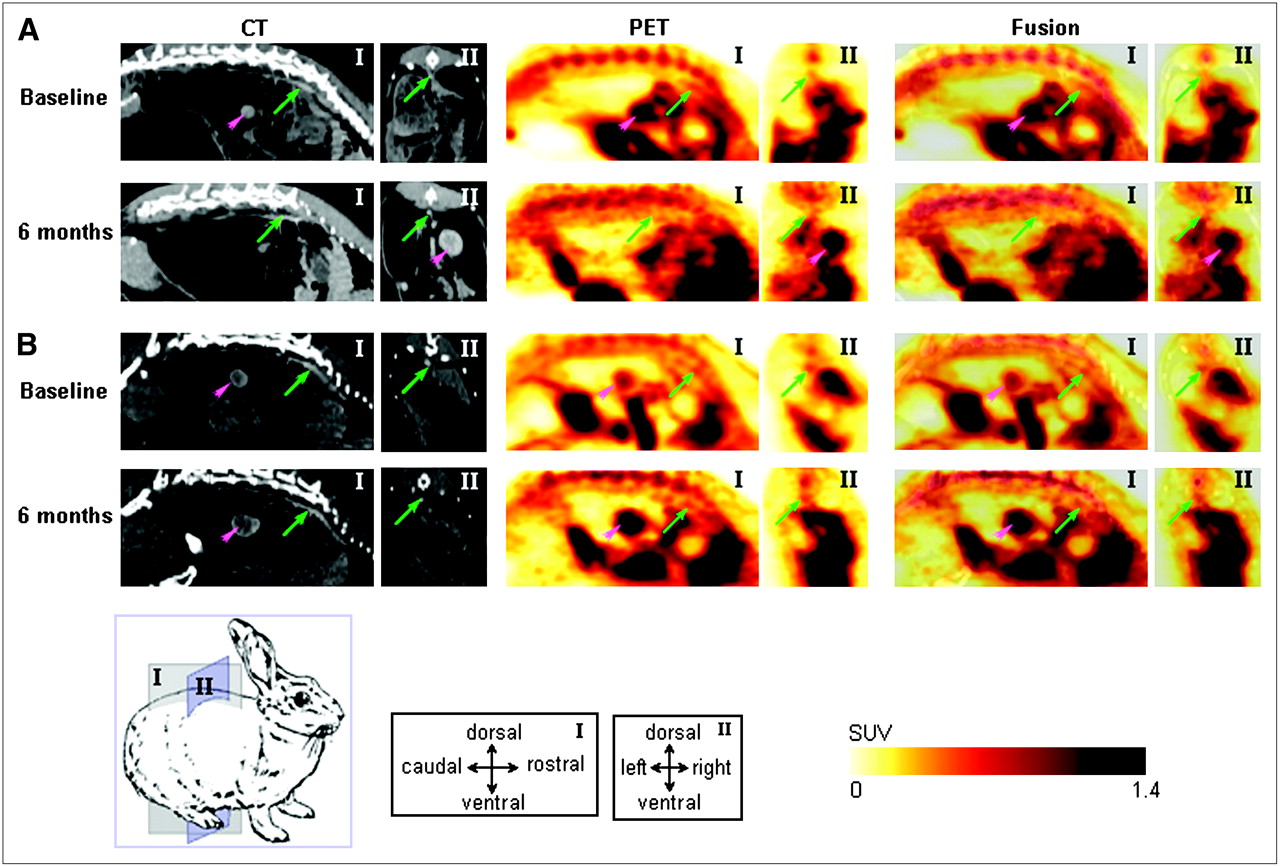
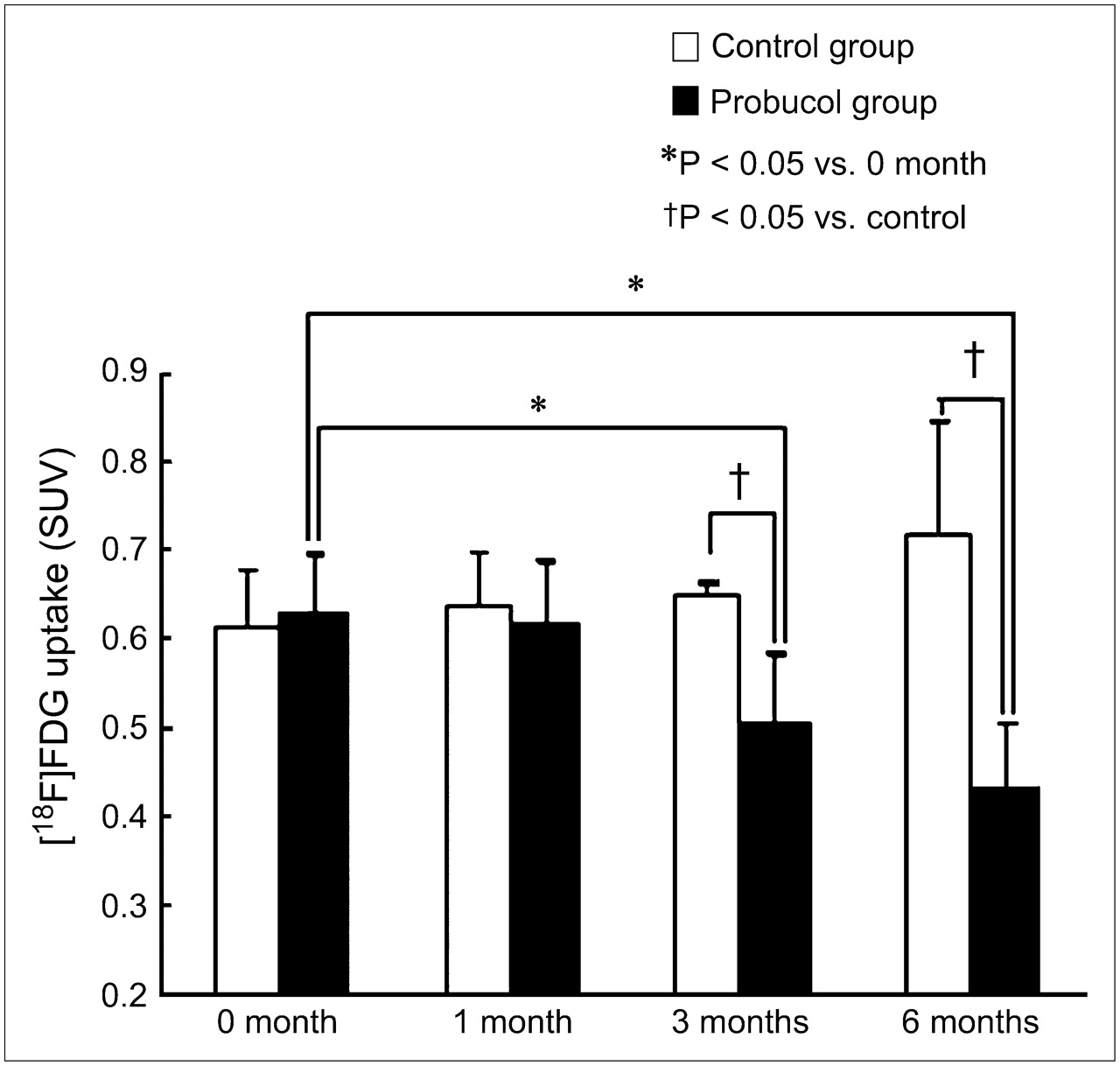
Figure 1 shows the CT, PET, and superimposed images of CT and PET of the WHHLMI rabbits. The arrows indicate the position of the aorta. At the age of 10 mo, the aorta could be imaged in all rabbits. In the probucol group, the aorta was not imaged after 6 mo of treatment. In contrast, intense radioactivity was observed in control rabbits throughout the 6-mo investigation. The time course of 18F-FDG uptake over the treatment period of the thoracic aortas in individual rabbits is shown in Figure 2. The SUVs decreased in all probucol-treated rabbits after 3 mo of drug treatment, whereas the SUVs remained constant or increased in control rabbits. SUVs for the 4 rabbits in each group are shown in Figure 3. The SUVs decreased significantly in the probucol group after 3 mo of treatment compared with the pretreatment period and the control group. The SUVs of the control group increased gradually with time.
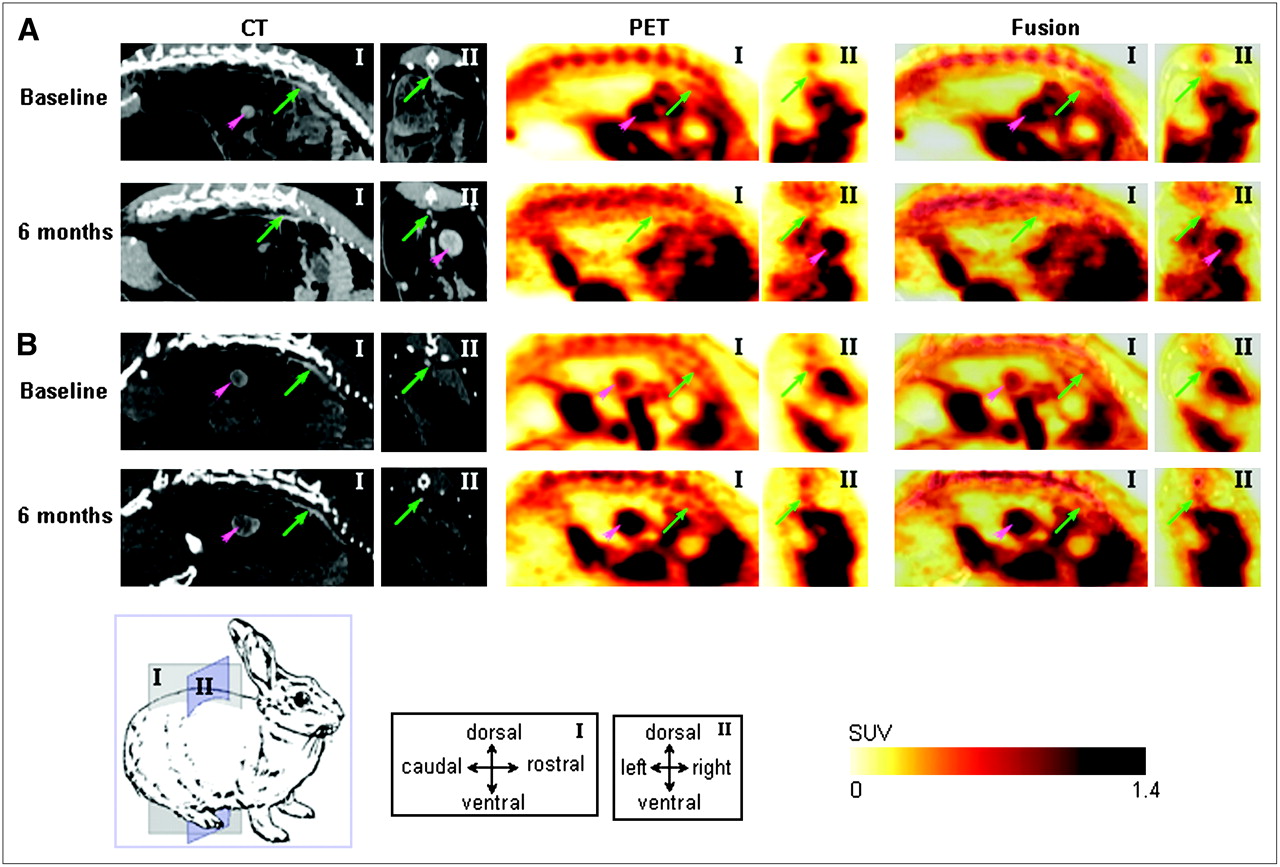
Typical PET, CT, and superimposed PET/CT images in sagittal (I) and coronal (II) planes for probucol-treated (A) or control (B) WHHLMI rabbits before intervention (baseline) and after 6 mo of intervention. Green arrows and pink arrowheads indicate aortas and kidneys, respectively.

Course of 18F-FDG uptake (SUV) over treatment period in WHHLMI rabbit thoracic aorta determined by PET. Solid lines and open symbols represent data from each control rabbit (n = 4); dashed lines and closed symbols represent data from each probucol-treated rabbit (n = 4).
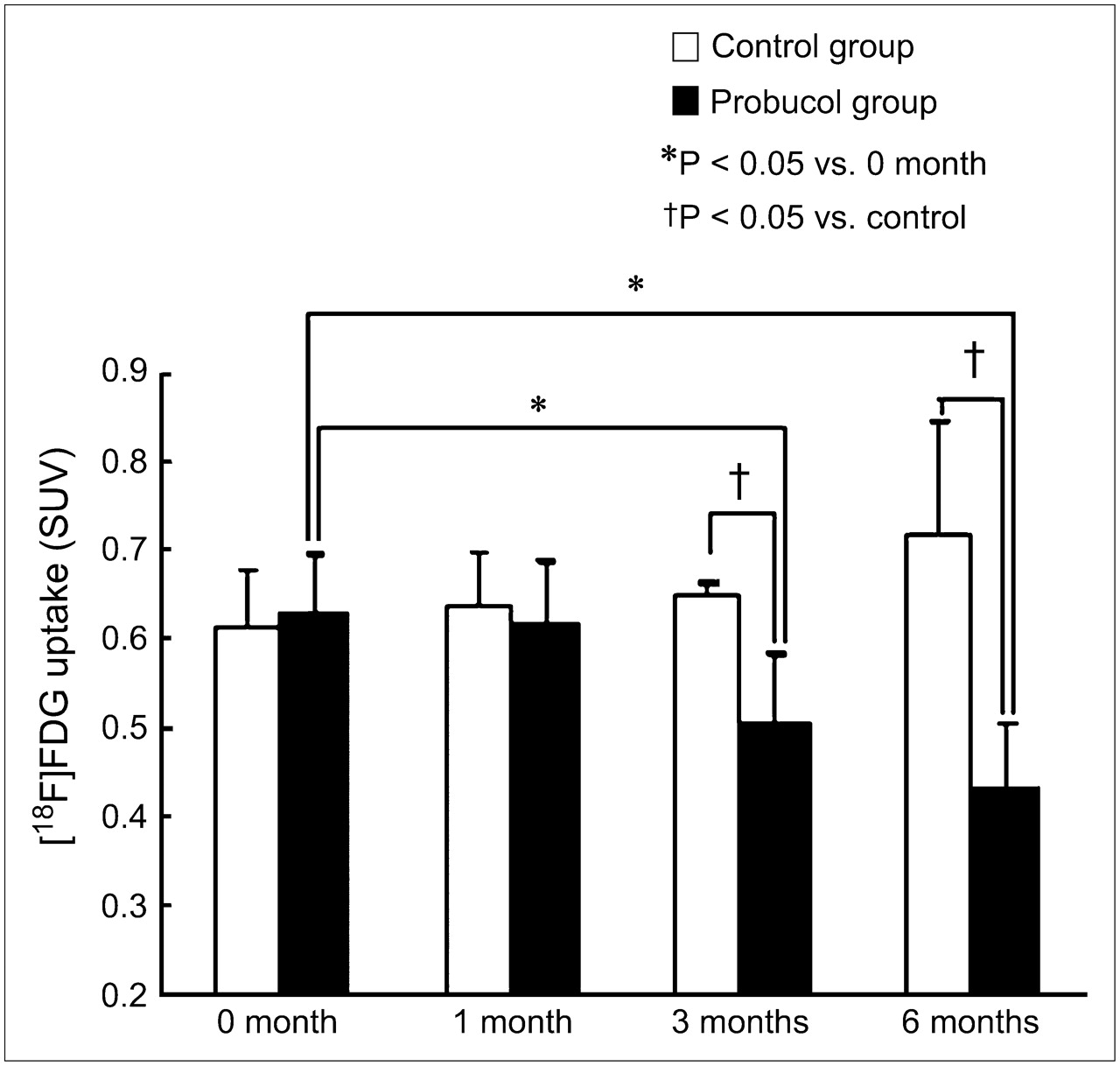
Sequential effect of probucol on 18F-FDG uptake in WHHLMI rabbit thoracic aorta. Data were obtained using PET. Each bar represents summed results for 4 rabbits per group.
Accumulation of 18F-FDG in Aortic Segments
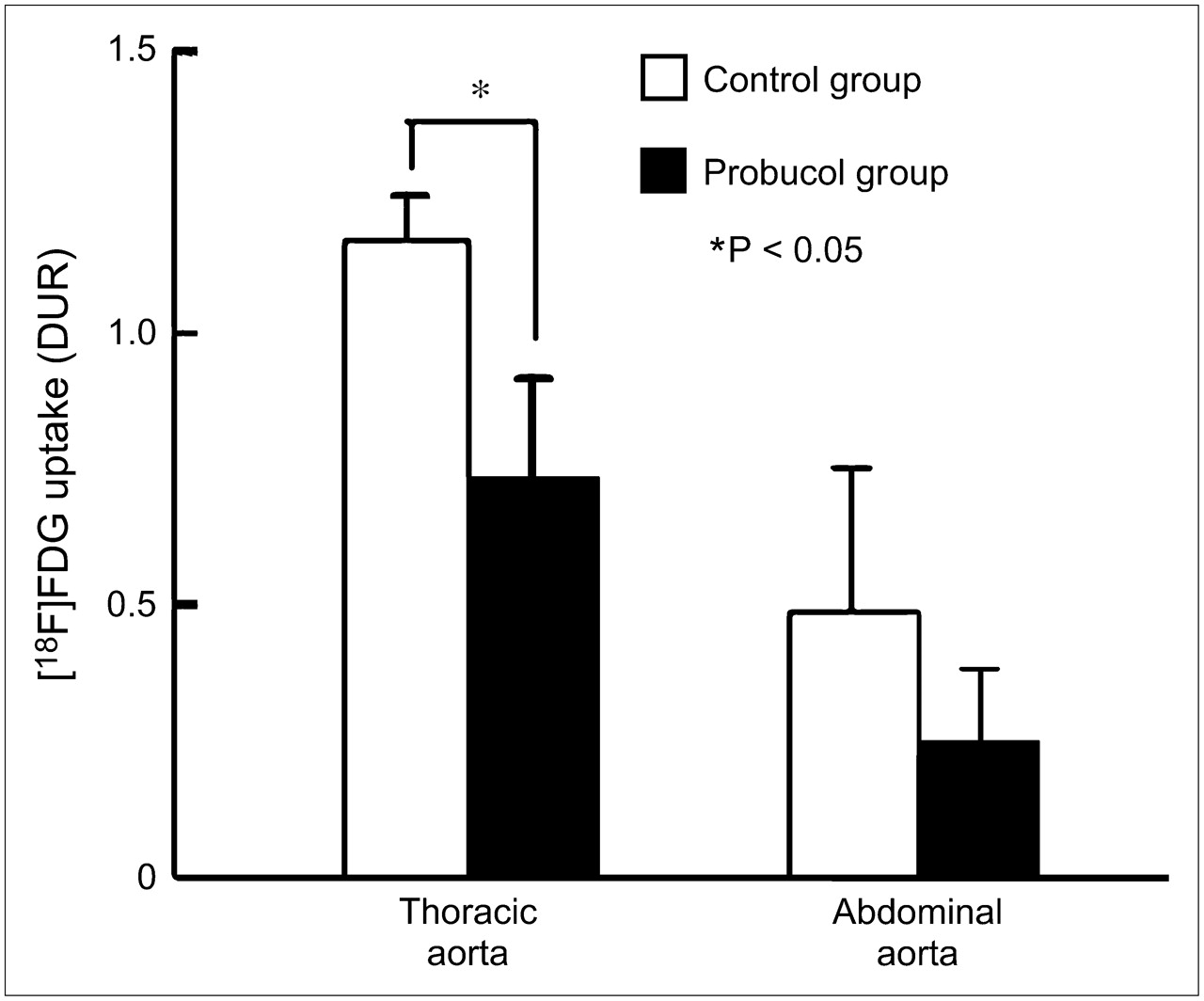
DURs in the removed aortic segments after 6 mo of intervention are summarized in Figure 4. 18F-FDG uptake in the thoracic aorta was significantly lower in the probucol-treated group than that in the control group. Uptake in the abdominal aorta was also lower in the probucol group than that in the control group, although the difference was not significant.
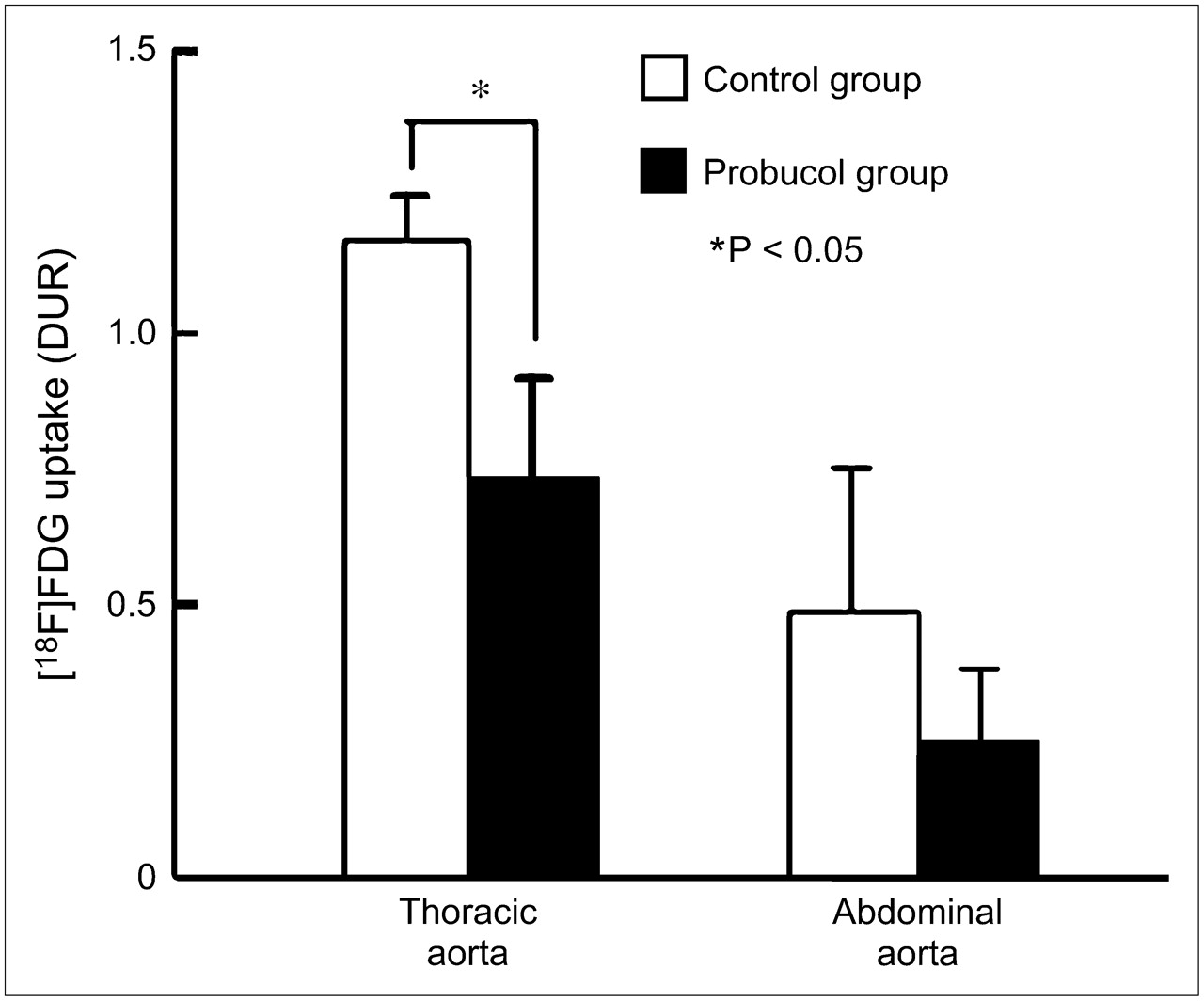
18F-FDG uptake by aortic segments from WHHLMI rabbits in each group after 6 mo of intervention. 18F-FDG uptake was measured using a γ-counter.
Histologic Analysis
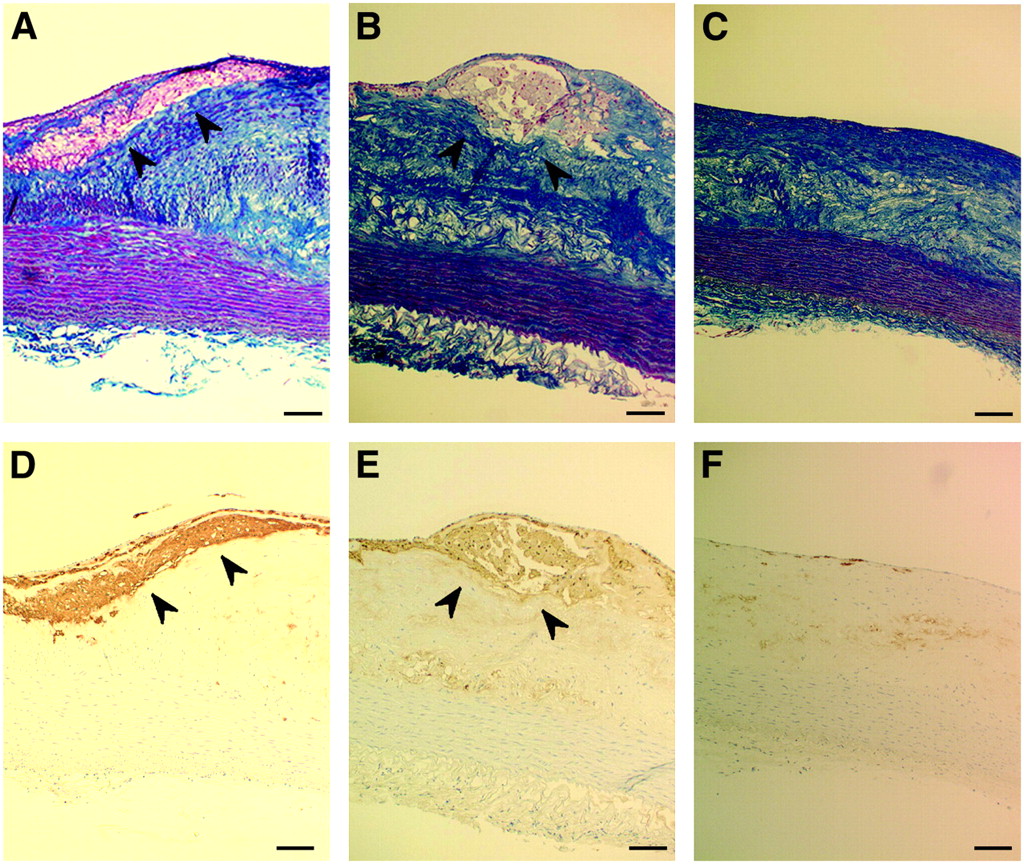
Typical images of azan-Mallory–stained and immunohistochemically stained slices are shown in Figure 5. As expected, macrophages were already found at the beginning of the study—that is, at the age of 10 mo. Probucol treatment for 6 mo resulted in a reduction of macrophage infiltration. The number of infiltrated macrophages in the thoracic and abdominal aortas was significantly lower in the probucol-treated group than that in the control group at the end of the 6-mo investigation (Fig. 6A). Intimal thickening was affected negligibly by probucol treatment (Fig. 6B).

Photomicrographs of atherosclerotic lesions in thoracic aortas of pretreatment control 10-mo-old WHHLMI rabbits (A and D), control WHHLMI rabbits (B and E), and probucol-treated WHHLMI rabbits (C and F) after 6 mo of intervention. Azan-Mallory staining (A–C) and immunohistochemical staining with antimacrophage monoclonal antibody RAM-11 (D–F) are shown. Macrophages can be seen (arrowheads) in each stained serial section from pretreatment control rabbits (A and D) and control rabbits (B and E). Bars = 100 μm.
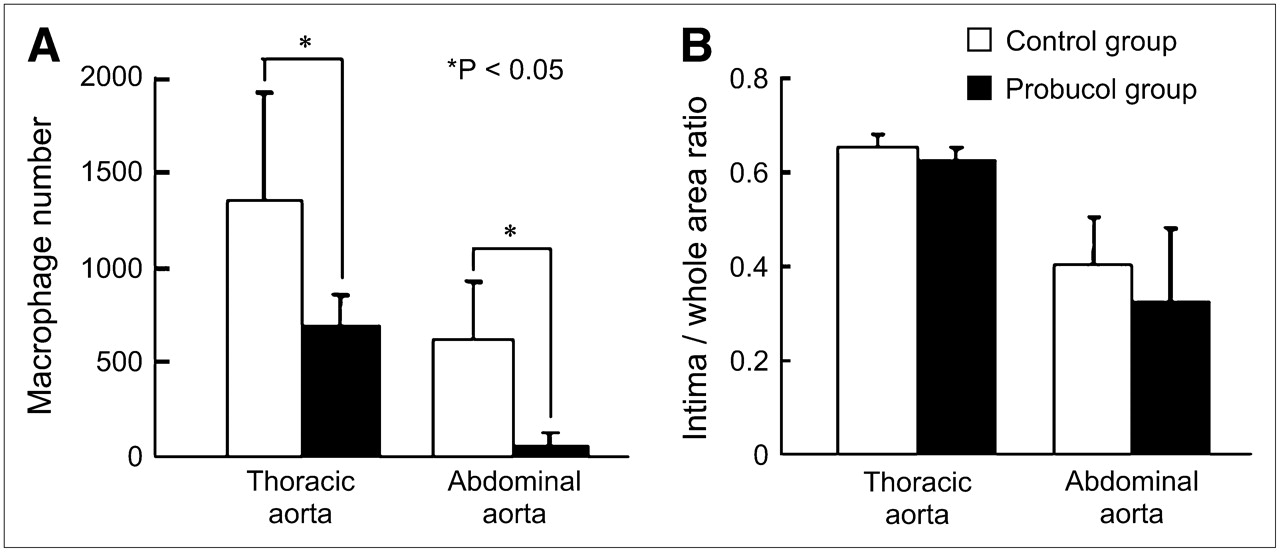
Effect of 6-mo probucol treatment on macrophage number (A) and ratio of intima to whole cross-section area (B).
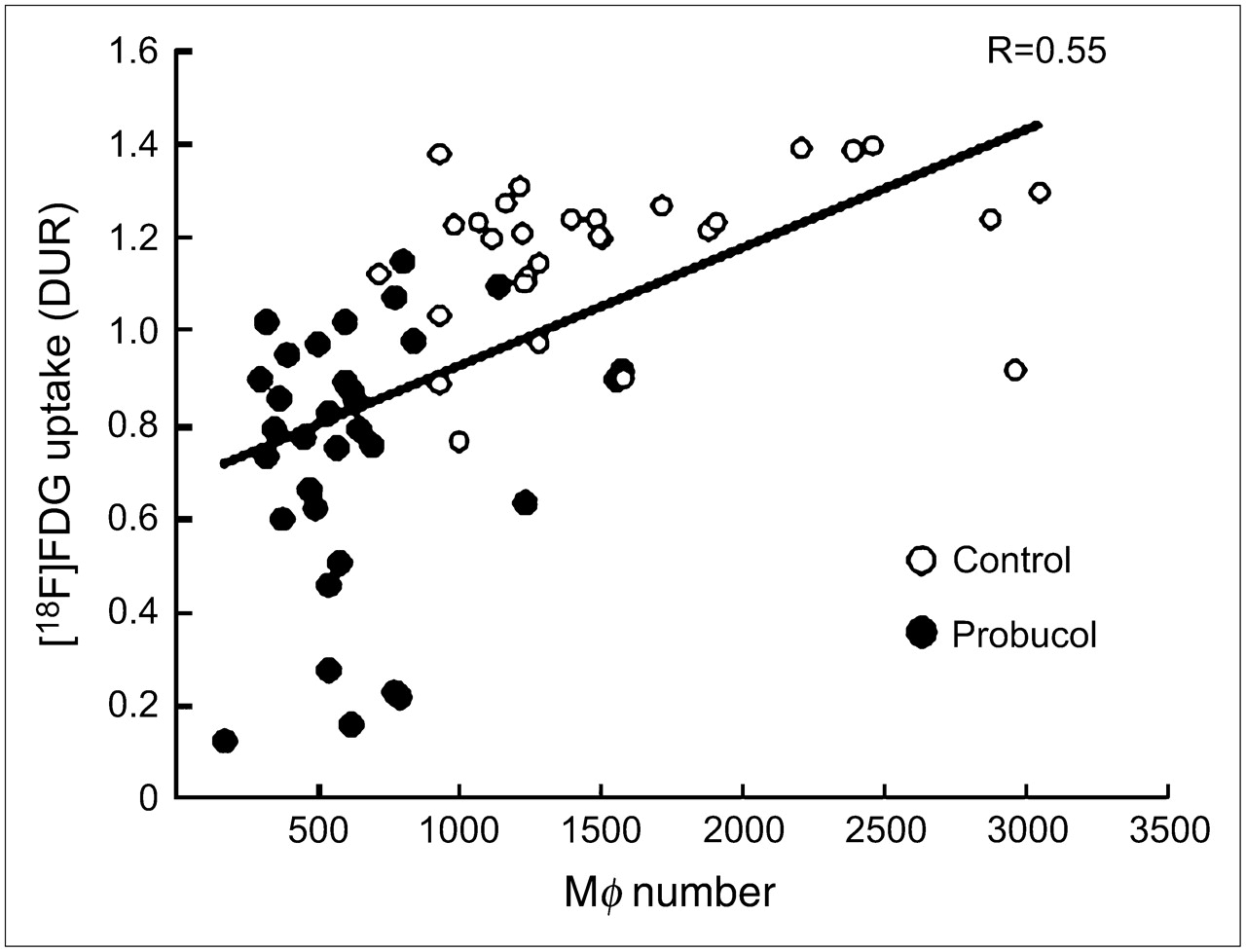
The relationship between 18F-FDG uptake and macrophage number in the thoracic segments is plotted in Figure 7. The segments from probucol-treated rabbits showed lower 18F-FDG uptake and macrophage infiltration than that of the control group.

Correlation between 18F-FDG uptake and macrophage (Mϕ) number in thoracic aortic segments from WHHLMI rabbits.
DISCUSSION
Macrophage infiltration has been identified as one of the leading causes of plaque disruption. We have recently shown that 18F-FDG PET can detect macrophage-rich plaques (5). Once a vulnerable plaque is detected, a sequential follow-up of that plaque is important to ensure the effectiveness of drug therapy for the prevention of myocardial and cerebral infarctions. Lipid-lowering therapy does not always lead to stabilization of vulnerable plaques. Some statins can reduce plasma cholesterol, but they do not decrease macrophage infiltration (21,22). Thus, monitoring plasma lipids alone is not sufficient for determining the therapeutic effect of drugs.
In this study, we aimed to investigate whether 18F-FDG PET can be used to monitor the effectiveness of therapies that target vascular inflammation. The lipid-lowering effect of probucol is moderate, and probucol did not decrease plasma cholesterol in some animal studies (13,23); however, probucol can reduce macrophage-rich, fatty-streak lesions even in advanced atherosclerosis (13). Thus, probucol was selected as a model therapeutic drug, because it is known to decrease macrophage infiltration, which can be imaged by 18F-FDG PET. Although no difference in plasma cholesterol levels was shown between the probucol group and the control group in our investigation, macrophage infiltration was decreased in the probucol-treated rabbits, in agreement with the earlier study (13).
Ten-month-old WHHLMI rabbits, which have established atherosclerotic lesions with macrophage infiltration, were used in this study. The aorta could be imaged at the beginning of the study by 18F-FDG PET. The accumulation of radioactivity decreased over the course of probucol treatment and we were able to monitor the therapeutic outcome using 18F-FDG PET. These results were supported by the measurement of radioactivity in aortic segments with a well-type γ-counter. No difference in blood glucose level was observed between groups during the PET studies throughout the experimental period. Our previous report showed that macrophages are responsible for 18F-FDG accumulation in atherosclerotic lesions but not intimal thickening (5). Because the ratio of the intima to the whole cross-section area was unaffected by probucol treatment, the decrease in 18F-FDG uptake likely resulted from the decrease in the number of infiltrated macrophages. Thus, 18F-FDG PET enabled us to image the reduction of inflammation that is responsible for plaque rapture.
Monitoring of coronary plaques is important for the prevention of cardiovascular disease. Because coronary plaques are small and the spatial resolution of PET is low, it may be difficult to detect these small plaques. However, Johnson et al. recently demonstrated the usefulness of 99mTc-annexin V SPECT for identifying plaque apoptosis in coronary vessels of swine (24). Therefore, 18F-FDG PET would be available for evaluation of the drug effect in reducing inflammation on coronary plaque.
CONCLUSION
This study has shown the usefulness of 18F-FDG PET for monitoring the reduction of inflammation in plaque. Because the stabilization of vulnerable plaques is important for atherosclerosis therapy, clinical application of this imaging system would be efficient for assessing the therapeutic effect of drugs. In addition, this method would also be useful for developing new drugs that can reduce inflammation in atherosclerotic plaque independently of lowering the level of cholesterol.
Acknowledgments
The authors thank Eri Mikata (Hamamatsu University School of Medicine) and Kumiko Yoshimura (National Center for Geriatrics and Gerontology) for technical assistance. We also thank Junichiro Abe (National Center for Geriatrics and Gerontology) for cyclotron operation and 18F-FDG synthesis. This study was supported by Health and Labor Sciences Research Grants, Research on Advanced Medical Technology. This study was also supported in part by a Grant in Aid for the Center of Excellence at Hamamatsu University School of Medicine (Medical Photonics) from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 30, 2006.
- Accepted for publication July 28, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Investigating the Lowest Threshold of Vascular Benefits from LDL Cholesterol Lowering with a PCSK9 mAb Inhibitor (Alirocumab) in Patients with Stable Cardiovascular Disease (INTENSITY-HIGH): protocol and study rationale for a randomised, open label, parallel group, mechanistic study
- Combined PET/DCE-MRI in a Rabbit Model of Atherosclerosis: Integrated Quantification of Plaque Inflammation, Permeability, and Burden During Treatment With a Leukotriene A4 Hydrolase Inhibitor
- 64Cu-Labeled Divalent Cystine Knot Peptide for Imaging Carotid Atherosclerotic Plaques
- 99mTc-cAbVCAM1-5 Imaging Is a Sensitive and Reproducible Tool for the Detection of Inflamed Atherosclerotic Lesions in Mice
- Comparison of Contrast Agents for Atherosclerosis Imaging Using Cultured Macrophages: FDG Versus Ultrasmall Superparamagnetic Iron Oxide
- Effects of p38 Mitogen-Activated Protein Kinase Inhibition on Vascular and Systemic Inflammation in Patients With Atherosclerosis
- Regression of Inflammation in Atherosclerosis by the LXR Agonist R211945: A Noninvasive Assessment and Comparison With Atorvastatin
- Pioglitazone Modulates Vascular Inflammation in Atherosclerotic Rabbits: Noninvasive Assessment With FDG-PET-CT and Dynamic Contrast-Enhanced MR Imaging
- Hypoxia But Not Inflammation Augments Glucose Uptake in Human Macrophages: Implications for Imaging Atherosclerosis With 18Fluorine-Labeled 2-Deoxy-D-Glucose Positron Emission Tomography
- Imaging the Vulnerable Plaque
- Imaging Atherosclerotic Plaque Inflammation by Fluorodeoxyglucose With Positron Emission Tomography: Ready for Prime Time?
- Feasibility of FDG Imaging of the Coronary Arteries: Comparison Between Acute Coronary Syndrome and Stable Angina
- 18F-FDG PET/CT Identifies Patients at Risk for Future Vascular Events in an Otherwise Asymptomatic Cohort with Neoplastic Disease
- Inflammation Imaging in Atherosclerosis
- Vascular Inflammation Imaging with 18F-FDG PET/CT: When to Image?
- Relationships Among Regional Arterial Inflammation, Calcification, Risk Factors, and Biomarkers: A Prospective Fluorodeoxyglucose Positron-Emission Tomography/Computed Tomography Imaging Study
- Comparison of Methods for Magnetic Resonance-Guided [18-F]Fluorodeoxyglucose Positron Emission Tomography in Human Carotid Arteries: Reproducibility, Partial Volume Correction, and Correlation Between Methods
- Radionuclide Techniques for Identifying Vulnerable Plaque
- 18Fluorodeoxyglucose Positron Emission Tomography Imaging of Atherosclerotic Plaque Inflammation Is Highly Reproducible: Implications for Atherosclerosis Therapy Trials