


Abstract
With the approval of 2 radiolabeled antibody products for the treatment of non-Hodgkin’s lymphoma (NHL), radioimmunotherapy (RIT) has finally come of age as a new therapeutic modality, exemplifying the collaboration of multiple disciplines, including immunology, radiochemistry, radiation medicine, medical oncology, and nuclear medicine. Despite the many challenges that this new therapy discipline has encountered, there is growing evidence that RIT can have a significant impact on the treatment of cancer. Although follicular NHL is currently the only indication in which RIT has been proven to be effective, clinical trials are showing usefulness in other forms of NHL as well as in other hematologic neoplasms. However, the treatment of solid tumors remains a formidable challenge, because the doses shown to be effective in hematologic tumors are insufficient in the more common epithelial cancers. Nevertheless, there has been progress in locoregional applications and in the treatment of minimal residual disease. There is also optimism that pretargeting procedures, including new molecular constructs and targets, will improve the delivery of radioactivity to tumors, do so with less hematologic toxicity, and become the next generation of RIT.
At the turn of the 19th century, Paul Ehrlich conceived the idea that “magic bullets” could effectively target compounds and eradicate sites of disease, but it was not until the early 1950s that this idea was first explored with an antibody conjugated to a radionuclide (1). Another quarter of a century would pass before antibody-based tumor localization was achieved clinically (2). This then led to the first radioimmunodetection products in the mid-1990s (3). In the first years of the 21st century, the first agent of this type was approved for the treatment of non-Hodgkin’s lymphoma (NHL) (4,5). The first 30 y of this process were devoted mostly to the discovery and production of suitable antibodies, as well as developing radiolabeling technologies. Cellular biology led the way with the development of monoclonal antibodies and, more recently, with the engineering of antibodies in various configurations with reduced immunogenicity. It is worth noting that antitumor antibodies remain one of the best means for selective binding to suitable targets on cancer cells and have also stimulated the study of other delivery forms, such as oligonucleotides or aptamers (6,7). However, the use of antibodies in radioimmunotherapy (RIT) is still evolving, with the investigation of new molecular constructs, new radionuclides and radiochemistry, improved dosimetry, prediction of tumor response and host toxicities, and better targeting strategies to prevent or overcome host toxicities, particularly myelosuppression. The hope is that the advances made for RIT in hematologic malignancies will translate to progress in the therapy of more radioresistant solid tumors. The purpose of this article is not to review the many efforts and advances made in RIT, but to summarize our views of the current status and future prospects. Other reviews may be consulted for more comprehensive discussions of this subject (4,5,8–14).
HEMATOLOGIC MALIGNANCIES
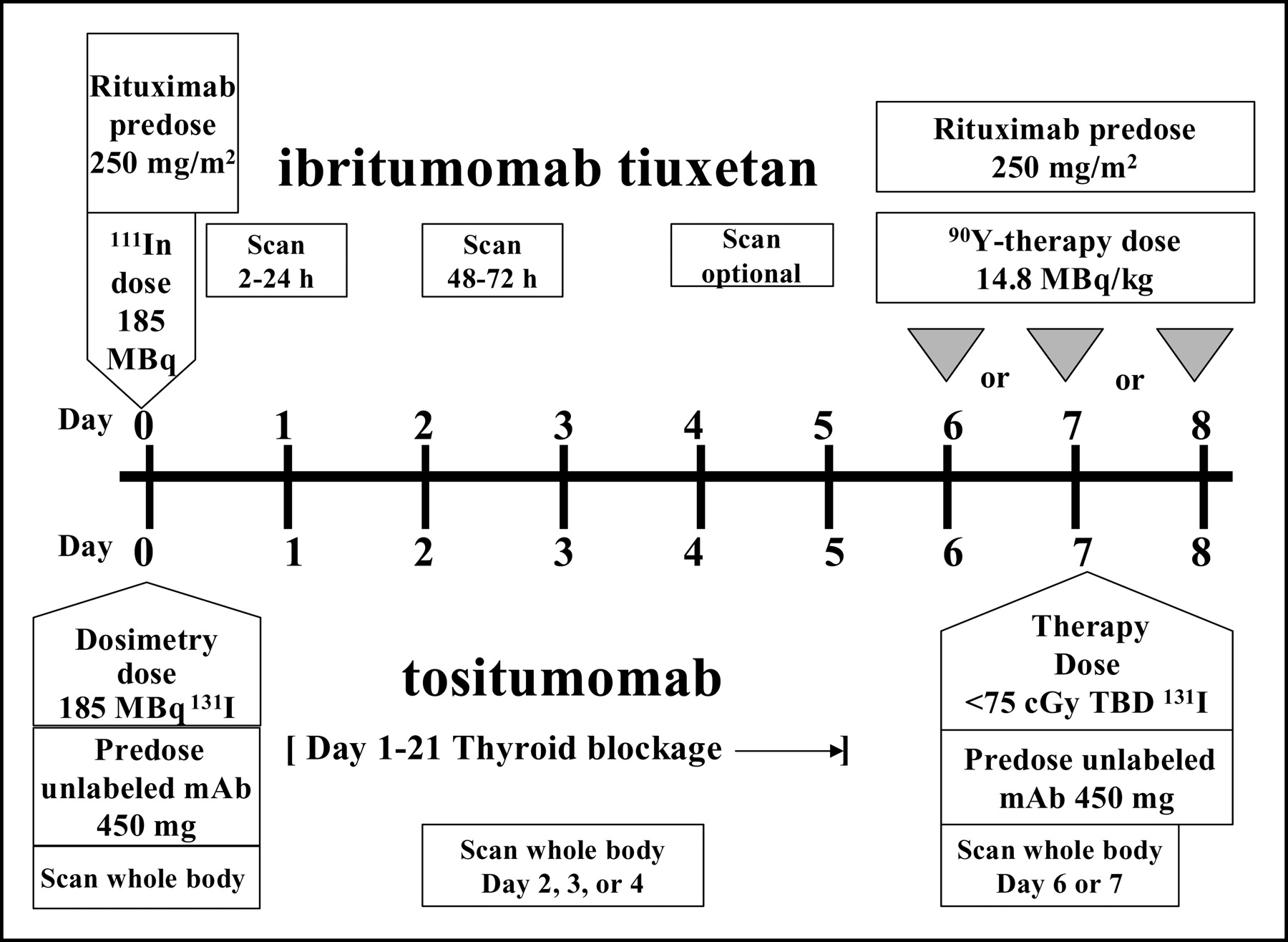
90Y-ibritumomab tiuxetan (Zevalin; IDEC Pharmaceuticals Corporation) and 131I-tositumomab (Bexxar; Corixa and GlaxoSmithKline Corporations) are currently the only radiolabeled antibodies approved for treatment of cancer. Each is registered for therapy of chemotherapy-refractive, follicular (low-grade) NHL, with or without transformation, and uses an antibody that is directed to CD20, an antigen that is abundantly present on a high percentage of both normal and malignant B-cells. Details of the treatment schemes for each of these approved agents are provided in Figure 1. Each is administered at radioactivity dose levels that result in severe myelosuppression that, for the most part, is reversible. A significant portion of patients in the registration trials for Zevalin and Bexxar, however, required supportive therapy, including platelet transfusions (22% and 15%, respectively), erythropoietin or epoetin alfa (8% and 7%, respectively), or filgrastim (13% and 12%, respectively) (15,16). The overall response rate for 131I-tositumomab in rituximab-refractory patients was similar to that reported with 90Y-ibritumomab tiuxetan, suggesting that the radionuclides are equally effective. However, the selection of the radionuclide has been shown to be more important for other radiolabeled antibodies being investigated as potential therapeutics for NHL, because these antibodies are internalized and then rapidly catabolized, which favors the use of radionuclides that remain inside the cell (17–20). 90Y-ibritumomab tiuxetan and 131I-tositumomab each have unique requirements for use, which have been extensively reviewed in several papers (21–26).
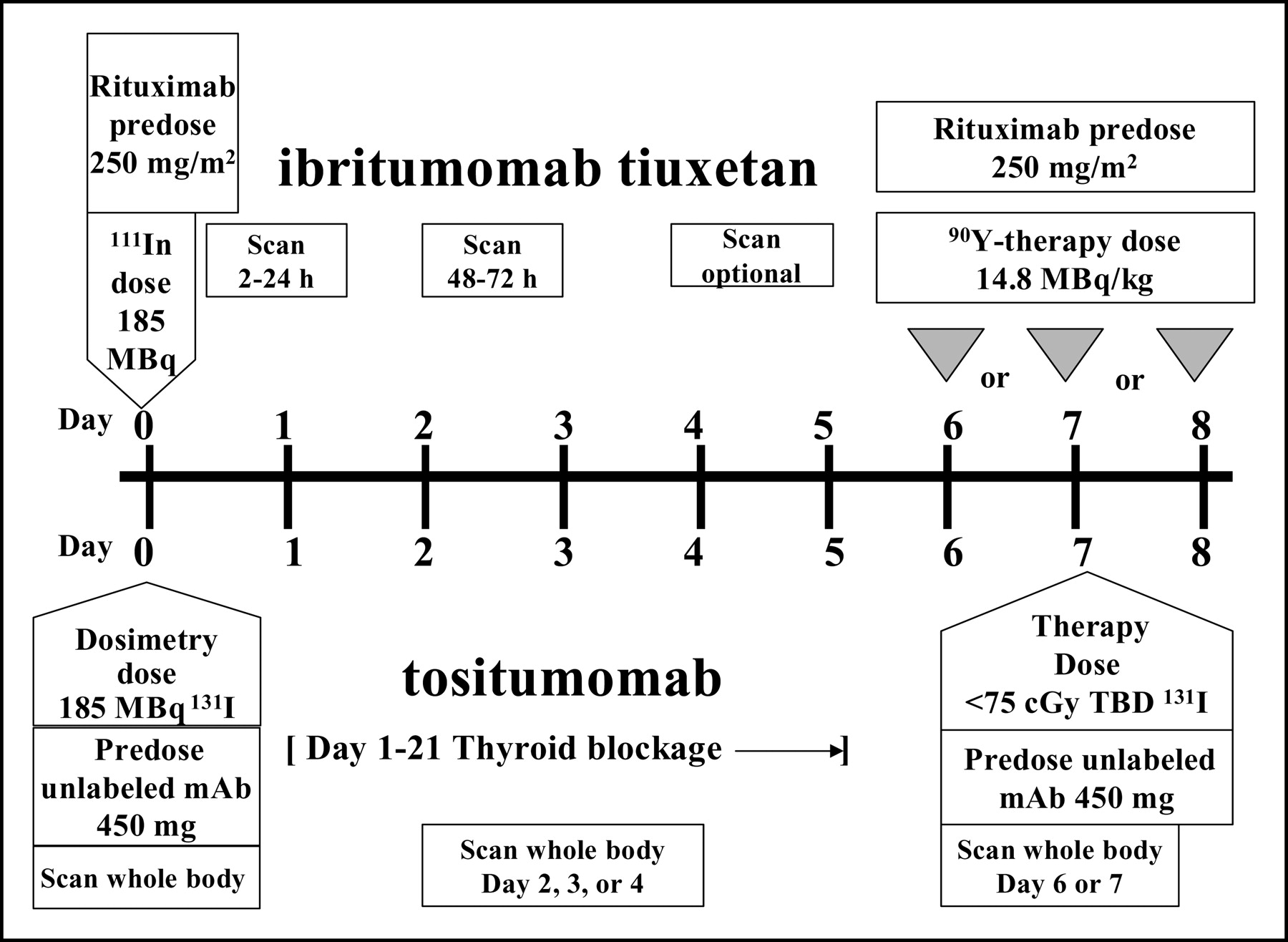
Comparison of administration conditions for 131I-tositumomab) and 90Y-ibritumomab tiuxetan. Reprinted with permission from Goldenberg, DM. Therapeutic use of radiolabeled antibodies: hematopoietic tumors. In: Ell PJ, Gambhir SS, eds. Nuclear Medicine in Clinical Diagnosis and Treatment. 3rd ed. London, UK: Churchill Livingstone; 2004:428–434.
Antitumor responses in NHL occur at very low absorbed doses (e.g., much less than 1,000 cGy). Koral et al. (27,28) reported a trend for higher absorbed doses to tumors that ultimately had a complete response, but others have disputed this relationship and even whether the lesions that responded were visualized by the radioimmunoconjugate (29,30). Although clear evidence for a dose–response relationship is lacking, it is likely present, but technical limitations in the way radiation dose and tumor size are measured create considerable inaccuracies in these estimates. Another variable is the fact that some antibodies used in these trials have therapeutic activity by themselves (31,32). Evidence suggests a role for anti-CD20 antibody in enhancing the therapeutic response from low-dose radiation (33,34). A randomized trial comparing the efficacy of a full course of rituximab (375 mg/m2/week × 4) with that of 90Y-ibritumomab tiuxetan (250 mg/m2 rituximab/week × 2 with the radiolabeled murine anti-CD20) showed the radiolabeled antibody to be superior to the naked antibody (i.e., statistically improved overall and complete response rates), but the difference in median time to progression was not statistically significant. Nevertheless, durable responses have been reported for patients who achieved a complete response (35,36). A similarly randomized trial with the naked murine B1 anti-CD20 antibody used with 131I-tositumomab was not performed. However, despite evidence that its mechanisms of action are somewhat different from those of rituximab, B1 alone has been shown to be active in animal models (37–39). Furthermore, responses were described in patients after they received a pretherapy diagnostic imaging dose (40,41). Anti-CD22 and anti-human leukocyte antigen (anti-HLA) antibodies also have been shown to be active as naked antibodies (42,43). Thus, the antibody itself is likely contributing to the antitumor responses observed with some of the radiolabeled antibodies used in NHL. In contrast, evidence for this has not been documented for the antibodies used in RIT of solid tumors.
Although the acceptance of these approved treatment modalities appears to be slow, it is important to remember that this technology is still in the early stages of development. With several opportunities to improve the overall response and survival rates, this treatment modality should become more established. For example, RIT is currently used in patients in whom chemotherapy fails, but clinical studies using 131I-tositumomab as a frontline treatment for NHL were highly encouraging, not only because of the excellent response rate, but also because the regimen had far fewer side-effects than chemotherapy (44). Press et al. (45) reported encouraging therapeutic results when 131I-tositumomab was administered as a frontline therapy 4–6 wk after standard cyclophosphamide, adriamycin, vincristine, and prednisone treatment for follicular NHL. It is notable that in this trial hematologic toxicity was more severe with chemotherapy than with RIT. Most of the data for RIT are based on a single treatment, yet Kaminski et al. (35) reported that 9 of 16 patients re-treated with 131I-tositumomab after progression responded a second time, with 5 attaining a complete response. Others have reported safety and efficacy of radioantibody treatment in patients who previously received another radioantibody therapy, and standard chemotherapy can also be given after nonmyeloablative radioantibody treatment without additional side effects (46–48). Thus, not only can multiple cycles of radioantibody treatment be given, but RIT can also be integrated safely with various treatment modalities as a means of further improving response.
Although each radioantibody treatment has established a dosing regimen that ultimately results in a majority of patients experiencing severe, dose-limiting thrombocytopenia and neutropenia, the tolerance of the therapy is related more to the patient’s treatment history as it affects their bone marrow status than is the actual radiation dose delivered to the red marrow (49). Perhaps further refinement in optimizing the manner in which the radioactivity dose is assigned individually could ensure that each patient receives the maximum dose allowed and improves responses. A retrospective analysis of hematologic toxicity based on red marrow dose and the measurement of Flt-3 ligand, a biologic marker for bone marrow status, indicated that the inclusion of the biologic marker assessment could improve toxicity outcome prediction significantly compared with dosimetry alone, at least in patients with solid tumors (50). RIT is also being used in high-dose therapy regimens with chemotherapy and external beam radiation (and possibly as a replacement for whole-body radiation) in cytoreductive marrow conditioning regimens (51–56).
Other radioantibody conjugates being tested clinically could improve responses or expand indications. A phase 2 trial with 131I-rituximab (i.e., with the chimeric antibody labeled and not the murine antibody as in Zevalin) has been reported (57). In this study, 375 mg/m2 of rituximab were given as a predose for both the imaging and subsequent therapy dose. An objective response rate of 71% was observed in 35 patients, including a complete response in 54% of patients, with a median duration of 20 mo. This response rate was similar to that reported with 131I-tositumomab and 90Y-ibritumomab tiuxetan, but the median duration was longer and appeared to have been better tolerated. Only 2 of 42 patients experienced a grade 4 hematologic toxicity. Early clinical trials examining the potential utility of radiolabeled epratuzumab (humanized anti-CD22 IgG; Immunomedics, Inc.) and Oncolym (anti-HLA-DR10; Peregrine Pharmaceuticals, Inc.) in NHL also have shown promising antitumor effects, including results in patients with aggressive forms of NHL (30,58,59).
Thus, there likely will be several opportunities to expand the application of radiolabeled antibodies in the treatment of NHL. However, because radiation, like chemotherapy, can have potential long-term effects, it could take several years before its full safety profile is known. In 5 clinical trials with 90Y-ibritumomab tiuxetan in 349 patients, 3 cases of acute myeloid leukemia (AML) were reported in addition to 2 cases of myelodysplastic syndrome (MDS). MDS was also reported in 32 of 995 patients administered 131I-tositumomab, with 27 mo as the median time to development. Therefore, the rate of MDS may continue to increase as the use of these agents expands. However, the probability for the development of MDS/AML in NHL patients given myeloablative doses of 131I-anti-CD20 IgG (n = 27) was 0.076 at 8 y and 0.086 at 7 y in patients who received high-dose chemotherapy (n = 98), suggesting that the overall risk of developing secondary malignancies or complications with RIT may be no higher than that ascribed to chemotherapy (60). Patients administered 131I-tositumomab also have a risk of developing mild-to-moderate hypothyroidism, must be given a thyroid blocking regimen at least 1 d in advance of the diagnostic injection, and must be maintained for at least 2 wk after the therapy regimen.
Patients with >25% bone marrow involvement are not currently referred for treatment with either 131I-tositumomab or 90Y-ibritumomab tiuxetan, because of increased risk of severe myelosuppression. This restriction exists primarily because these agents use β-emitting radionuclides with several-millimeter pathlengths that can cause collateral damage to the surrounding normal marrow. It is possible that smaller, fractionated doses of these radiolabeled antibodies could be given safely to reduce the infiltration of marrow. Indeed, studies have already shown that if the pathlength of the radionuclide is shortened RIT can be applied to blood-borne (leukemias) or other hematologic malignancies primarily involving the bone marrow, potentially without the need for supportive measures (e.g., peripheral blood stem cell transplant).
In this regard, α-emitters are prime candidates for such applications and are being explored for the treatment of myeloid leukemia (61–63). An α-particle has a path length that will traverse several cell diameters, making it effective against small cell clusters, and its high linear energy transfer increases the probability for cell killing even when targeting low-density antigens. However, even Auger-emitting radionuclides have been shown to be highly effective in animal models with disseminated human NHL (64). Auger-emitters exert their activity mostly to the targeted cell and, therefore, could be ideally suited for treating micrometastatic disease, even in the bone marrow, because nontargeted cells would be unaffected. However, because of their low energy, a substantial number of Auger particles must be delivered to kill a cell. We have shown, for example, that an antibody to CD74 is capable of delivering large quantities of Auger-emitters inside the cell. This is not because of large numbers of antigen sites on the cell surface but because the antigen is internalized and constantly recycling, thereby transporting and emptying the antibody with its radioactive payload inside the cell and then returning to the cell surface, where it is available to bind additional antibodies (65). Although antibodies radiolabeled with α-emitters and Auger-emitters are typically considered for applications such as leukemia, they may have a role in the treatment of other hematologic malignancies (and potentially solid tumors). For example, a radiolabeled antibody conjugated to an α-emitter or Auger- emitter could be administered in patients with follicular lymphoma who have >25% bone marrow involvement, making these patients eligible for subsequent RIT with β-emitters or chemotherapy, particularly if these treatments can be shown to be effective at doses that would not affect the tolerance of subsequent therapy. It is also intriguing to speculate that α- or Auger-emitting antibodies could be given after these other treatments as a means of scavenging smaller pockets of disease that might not otherwise be as effectively treated with β-emitters or drugs.
SOLID CANCERS
Chemotherapy has been more successful in hematologic than in solid tumor malignancies, and this seems to be true for RIT as well. Clinical trials of NHL treatment have yielded reports of significant antitumor responses (in fact, complete responses) with the delivery of considerably less than 1,000 cGy to a tumor (27,66). Yet RIT in a variety of solid tumors has failed to elicit responses in patients with disease burdens similar to those treated in NHL trials, even with the delivery of as much as 3,000 cGy to the tumor using 131I- or even 90Y-labeled antibodies (67,68). With little evidence of clinically significant responses with RIT alone, other strategies to augment the targeting of the radiolabeled antibody have been explored. For example, Meredith et al. (69) combined an anti-carcinoembryonic antigen (anti-CEA) antibody (COL-1) and the CC49 anti–tumor-associated glycoprotein (TAG)–72 IgG radiolabeled with 131I, because by immunohistology the combination gave a more homogeneous distribution within the tumor than either antibody alone. In addition, patients received α-interferon, which had been reported to enhance CEA and TAG-72 expression in gastrointestinal tumors. Tumor imaging was judged to be excellent in most cases. The combination of anti-CEA and anti-TAG-72 antibodies together with interferon appeared to result in a modest increase in the absorbed dose to the tumor when compared with other trials that used only 131I-CC49, but yielded no objective responses. Radiolabeled anti-TAG-72 antibodies have been used in other cancers, including breast, prostate, and ovarian cancer, but few if any objective responses have been observed in patients with bulky disease (70–72). Despite failing to observe objective antitumor responses with a 90Y-anti-CEA antibody, Wong et al. (73) reported substantial reductions (e.g., 41%–68%) in a few colorectal cancer lesions (size, 2.0–6.5 cm in diameter) and some tumor stabilization with the delivery of <1,000 cGy. Thus, the challenge remains to understand the underlying mechanisms of the refractoriness of solid tumors to RIT.
In many respects, clinical testing has ignored what was observed in preclinical models over many years: RIT alone usually is not effective against bulky disease (74). Evidence in support of using RIT in minimal disease came from investigations of RIT in the treatment of a colon cancer in a lung metastasis model, where animals bearing multiple small foci of disease could be cured with RIT alone (75). RIT’s efficacy in preventing the death of animals bearing these small microscopic colonies of colon cancer in the lung was significantly reduced if bulky disease (i.e., a large subcutaneous tumor) co-existed at the time of treatment (76). In addition, animal models have typically shown the uptake of radiolabeled antibodies to be highest on a per-gram basis in small tumors, which has been confirmed clinically (77–80). Despite these observations, RIT is still being tested in patients with multiple lesions that are mostly large (>5 cm in diameter). This is probably attributable to regulatory requirements that initial trials be conducted in patients with advanced disease for which other options have failed. In contrast, encouraging results are emerging with RIT in patients with minimal or occult disease. For example, after a phase 1 trial determining the maximum tolerated dose (MTD) and initial evidence of efficacy in either patients with small colorectal cancer metastases or patients given RIT after salvage resection of liver metastases (81), Liersch et al. (82) reported on an exploratory trial using an 131I-humanized anti-CEA IgG in 22 patients who had undergone liver resection for metastatic colorectal cancer. The median survival from the time of liver resection of the 19 patients who could be assessed for response was 54 mo, which is encouraging compared with a median survival of between 24 and 42 mo reported in 12 separate clinical trials involving more than 5,000 colorectal cancer patients after salvage surgery of liver metastases (83).
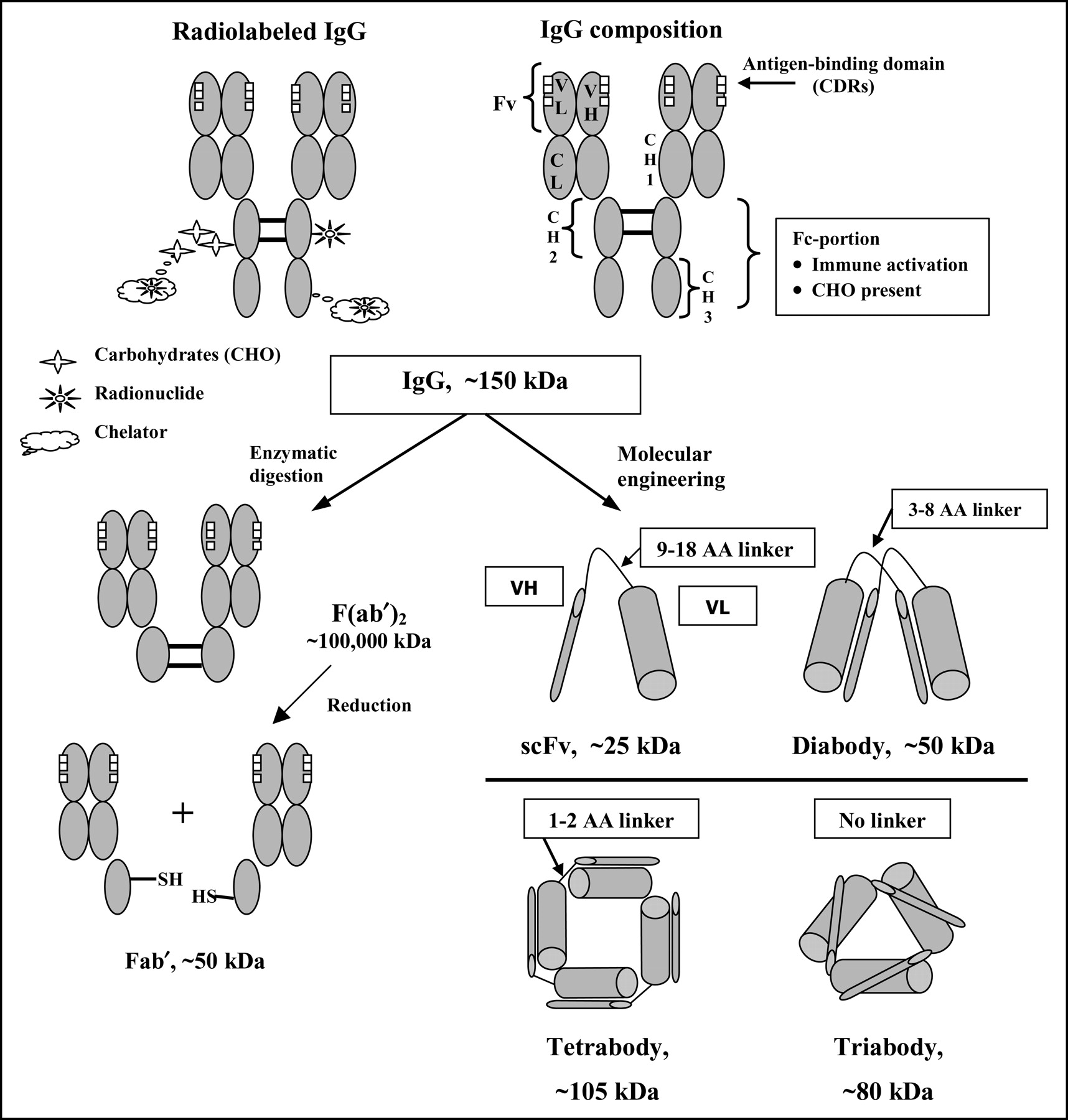
Although the majority of clinical trials to date have used whole IgG, several studies have suggested that antibody fragments would be better delivery vehicles. Although modeling/dosimetry studies predict that IgG is a better vehicle for therapy than an antibody fragment, empirical studies in animals show improved therapy with radiolabeled antibody fragments when compared with therapy with whole IgG (84–90). Enzymatically digested antibody fragments have been used clinically. In the future, engineered antibodies, such as single chains (single-chain variable fragment [scFv], ∼25,000 Da) or diabodies (∼50,000 Da), which are smaller monovalent and divalent binding proteins, respectively, or even one of a variety of other types of constructs, will be the focus of clinical testing as possible alternatives to intact IgG (91–94). Figure 2 depicts the commonly used antibody fragments as well as several of their molecularly engineered counterparts. Various candidate molecules and their properties are summarized in Table 1. Although F(ab′)2 and Fab′ fragments have been used extensively in patients, less clinical data are available for the molecularly engineered products, so their precise targeting and distribution properties reflect findings in animal models.

Schematic representation of various forms of antibody fragments prepared by enzymatic digestion or molecular engineering. The most commonly used form of antibody, IgG, has been radiolabeled by conjugating directly to the protein (e.g., radioiodination of tyrosine) or radiolabeling a coupled chelator. Chelators have been coupled directly to the protein or to the carbohydrates that reside on the Fc-portion of the molecule. Single chains are formed by linking the variable light (VL) and variable heavy (VH) chains with amino acid (AA) linker. Diabodies, triabodies, and even tetrabodies are formed spontaneously when smaller length AA chains are used to hold the VH and VL units together. Recombinant bispecific diabodies and other bispecific constructs can be prepared by pairing VH and VL of 2 antibodies with different specificities.
Comparison of Targeting Properties of Representative Forms of Antibody and Chemically Prepared or Engineered Fragments
The primary deterrent for using antibody fragments, particularly those with a molecular size <50,000 Da, is that they are cleared through the kidneys, which raises concern for renal toxicity, particularly when a radionuclide is used that is reabsorbed and retained by the kidney, such as a radiometal. Behr et al. (95) reported that a high predose of cationic amino acids could significantly reduce renal tubular reabsorption of radiometal-labeled (e.g., 99mTc- or 111In-) Fab′. They showed subsequently in mice that with this procedure higher doses of a radiometal-labeled Fab′ could be administered with less renal toxicity. However, bone marrow support was also required to escalate the radioactivity dose, indicating that, just as with an IgG, bone marrow toxicity is dose limiting even for an antibody fragment (96). Cationic amino acids have been used clinically in combination with 90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA), Tyr3-octreate (90Y-DOTATOC), a somatostatin peptide analog, to reduce renal accretion. Even with this method, care was taken not to exceed 2,500 cGy to the kidneys, because of late renal toxicity, and myelosuppression proved to be dose limiting (97,98). Having to contend with renal toxicity is also a significant deterrent for treatment with radiometal-labeled antibody fragments, because renal toxicity is not manifested until at least 3 mo after treatment and careful monitoring is required for more than 1 y (99,100). Because radioiodine is not retained in the kidneys, it is a more likely choice for labeling antibody fragments for studies. For example, clinical studies using a radioiodinated CH2-deletion construct, a type of engineered antibody fragment, are currently under way (101).
The use of RIT locally is another example of treating smaller tumors. The most prevalent locoregional treatment strategies include intraperitoneal delivery of antibodies for ovarian cancer and intracranial administration for brain cancers. The route of administration is based on preclinical data that showed an advantage for intraperitoneal over intravenous injection, particularly but not conditionally in the presence of malignant ascites (102–106). Colcher et al. (107) showed in patients who were coadministered intraperitoneal and intravenous injections of 131I-/125I-B72.3 IgG that the majority of lesions (33 of 55) isolated in surgery had a 2-fold higher uptake for the intraperitoneally administered antibody, whereas 13 lesions were found to have a 2-fold higher uptake with the intravenously injected antibody. In 7 tumors uptake did not differ between the two administration routes. Pathologic assessment of these lesions led to the conclusion that peritoneal implants were more likely to benefit from intraperitoneal injection, whereas nonimplants (i.e., those metastases in the peritoneal cavity resulting from hematogeneous spread) were more likely to have higher uptake by intravenous injection. In this regard, it is possible that both routes of injection should be contemplated. We reported a complete response in a patient with ovarian cancer who presented with malignant ascites and peritoneal implants at the time of her intravenous treatment with 1,480 MBq/m2 of 131I-labeled anti-CEA IgG (108). Except for one other patient in this trial who experienced a brief minor response, all other enrolled patients with advanced disease progressed (109).
The most advanced agent in clinical testing for intraperitoneal RIT in ovarian cancer is pemtumomab (R1549; Antisoma plc), a 90Y-labeled murine antihuman milk fat globulin 1 (MUC-1) murine antibody. This agent was tested in ovarian cancer patients with measurable and occult disease. The most promising data were from a phase 2 trial, in which 666 MBq/m2 of this agent were administered intraperitoneally to 21 women with stage IC–IV ovarian cancer who had no detectable disease after surgery and completing a platinum-based chemotherapy regimen. Seventy-eight percent of these patients were alive 10 y after receiving this treatment, whereas the median survival for a historical control group (72 patients) was less than 4 y (110). However, according to a recent announcement by Antisoma, preliminary findings from a multicenter phase 3 trial showed no significant difference between ovarian cancer patients with no evidence of disease who were given a single intraperitoneal treatment of the 90Y-labeled antibody and those in the control arm. It is important to keep in mind that this single experience does not necessarily detract from the prospects of RIT in this indication. An investigation of different antibodies, radionuclides, or specific treatment regimens with the radiolabeled antibody alone or in combination with other agents may still provide evidence that RIT could have a role in the management of occult disease. In this regard, another study using intraperitoneally administered 177Lu-CC49 anti-TAG-72 IgG has noted a similar trend toward improved responses in ovarian cancer patients with minimal disease. For example, a response was observed in only 1 of 13 patients who had gross disease at the time of treatment, whereas 7 of 9 patients with nodules smaller than 1 cm did not progress until at least 21 mo. Of the 5 patients with occult disease, 4 were without evidence of disease for a range of 6 to 35 mo (111).
Using the intracranial route, clinical studies with an 131I-labeled antitenascin antibody for the local treatment of glioblastoma multiforma have been very encouraging, with median survival rivaling that with brachytherapy or stereotactic radiosurgery but with a lower rate of radionecrosis (112,113). These investigators also reported a correlation between the radiation-absorbed dose delivered to the rim of the cavity, where the radioantibody was deposited, and various parameters that reflected a positive outcome for the patient (114). A similar intracranial approach has also been shown in animal models to be useful for treating brain metastases of other cancers (115). Quang et al. (116) also reported the successful use of 125I-labeled antiepidermal growth factor receptor antibody in a phase 1 and 2 trial, where patients received the radiolabeled antibody after surgical resection of primary brain cancer and in concert with external beam therapy. Thus, intracavity treatment with radiolabeled antibodies is an approach that can be administered safely, alone or in combination with other treatment modalities, but appears to be most promising in minimal residual disease.
Nearly every form of cancer therapy at some time has been examined in combination with another form of treatment in the hope of improving efficacy, and RIT is no exception. Combination approaches fall into 2 categories: those designed to improve radioantibody distribution and uptake and those in which RIT is combined with other therapy modalities.
Some examples of the first category of combinations have already been cited, such as administering interferon to up-regulate antigen expression and thereby improve targeting (70,71,117). Other reports have documented attempts to manipulate a tumor’s vascular properties through hyperthermia, radiation, or biologically active compounds in an effort to enhance the amount of radiolabeled antibody targeted (118–123). Each of these methods has unique dosing and temporal requirements to optimize the targeting of the radiolabeled antibody. Whereas radiation and hyperthermia are designed to provide increased vascular permeability within the tumor, other systemically applied treatments with a variety of vasoactive agents have been used to enhance antibody uptake in tumors. Pedley et al. (124–126) observed improved targeting of antibodies using several agents known to affect the vasculature. The agents proved effective in killing or even curing established colorectal cancer xenografts when used in combination with radiolabeled antibodies. Kurizaki et al. (127) showed that the coadministration of an agonist peptide of human C5a with a radiolabeled antibody could improve antibody uptake and its therapeutic effects in nude mice. Other methods that are designed to inhibit neovascular formation also have been used effectively in combination with RIT (128–130). One innovative approach fuses gene therapy and RIT targeting by first introducing a gene product so that the tumor expresses a unique antigen. This antigen can then be targeted by a radiolabeled antibody (131).
Considerable attention has been given to combining RIT with chemotherapeutic agents. In such an approach, drugs that are known to be radiosensitizers or have other potential additive or synergistic properties are added to a full dose of RIT. The drug is given at a reduced dose or modified schedule primarily to enhance the therapeutic response of RIT over that with RIT alone. DeNardo et al. (132,133) were the first to report the enhancement of a subtherapeutic dose of paclitaxel when used in combination with a 90Y-labeled antibody in a nude mouse–human breast cancer model. Others have used this combination successfully in breast and prostate cancers (134,135). In addition to the taxanes, other chemotherapeutic agents have been reported to enhance the activity of RIT when used at submaximal doses (136,137). As with any combination modality, numerous dosing and scheduling issues are involved in optimizing the therapy. Several reports have reviewed this process, particularly as it relates to the p53 status of a given cell line (138–140). For example, starting with the SKOV-3 p53-null cell line, Blumenthal et al. (140) examined 3 p53-transfected cell lines that differed in their p53 mutation locus. They found considerable differences in each cell line’s sensitivity to various drugs and to the drug–RIT combination. Several combinations were found to be antagonistic, highlighting the difficulty that may be encountered in the future with certain chemotherapy–RIT combinations as well as indicating ways in which prescreening of cancer biopsies could be used to optimize treatment planning (140).
The second approach, combining RIT with more conventional doses of drugs, rests on the assumption that RIT can enhance the chemotherapeutic regimen. However, this may prove difficult, because many conventional drugs are also myelosuppressive. Nevertheless, several reports in animal models have suggested promise for this approach (141–146).
Initial results of feasibility trials have been reported for combining intraperitoneal RIT with 177Lu- or 90Y-labeled anti-TAG-72 CC49 and chemotherapy in regional therapy of ovarian cancer as well as for 90Y-labeled anti-CEA antibody combined with a continuous infusion treatment regimen of 5-FU in chemorefractive colorectal cancer (147–149). Although each of these regimens has been tolerated, with hematologic toxicity being dose limiting, it is too early to assess whether these combination modalities significantly enhance the effects of RIT for any specific chemotherapy regimen. However, based on studies in ovarian cancer, the trend continues to favor the treatment of less advanced disease with these combinations.
PRETARGETING: THE NEXT GENERATION OF RIT
Pretargeting evolved as a method to overcome the difficulties presented by high levels of radioactivity retained in the blood during RIT. Several types of pretargeting have been developed, but all strive to overcome the limitation of slow blood clearance of directly radiolabeled IgG by separating the targeting performed by the antibody from the subsequent delivery of the radionuclide (149–156).
Pretargeting was initiated with the notion that a bispecific monoclonal antibody (bsmAb) could be constructed with one binding arm directed to a target (e.g., a tumor antigen), and a second binding arm specific to a metal chelator (157). The metal chelator could then be radiolabeled and injected separately after the bsmAb had localized to the target antigen and cleared from the blood. This technique was first developed and tested clinically using a bispecific antibody composed of an anti-CEA Fab′ joined chemically with an antichelate Fab′ used in conjunction with the 111In-labeled chelate (158). Le Doussal et al. (159) made a significant improvement to this initial pretargeting system by using a radiolabeled compound that included 2 haptens. This concept was called an affinity enhancement system, because a bsmAb bound monovalently to its target antigen would be cross-linked by the divalent hapten with a second bsmAb to form a divalent binding bridge to the tumor antigen (Fig. 3). Hnatowich et al. (160) were the first to describe an ingenious approach to pretargeting with avidin (mammalian produced) or streptavidin (bacterial product) in conjunction with biotin in a variety of configurations. This system appeared to be ideally suited for pretargeting, because the avidins could bind as many as 4 biotin molecules with an exceptionally high binding constant (10−15 mol/L). The reagents could be produced in plentiful amounts, were nontoxic, and were amenable to chemical modification for coupling to antibodies or radiolabeling.

The next generation of radionuclide targeting; examples of pretargeting approaches: (A) Two-step streptavidin IgG/radiolabeled biotin procedure (177,191). (B) Three-step biotinylated IgG/radiolabeled biotin pretargeting procedure (160,161). (C) Bispecific antibody pretargeting procedure (164). (D) Oligonuclide pretargeting procedure (165–167).
Several configurations of an avidin/biotin pretargeting system were described, but 2 have prevailed (Fig. 3). One system, typically described as a 2-step approach, includes 3 agents: a streptavidin-conjugated antibody, a clearing agent, and the radiolabeled biotin. The clearing step is essential to the procedure, because the streptavidin–antibody conjugate, with its molecular weight of ∼200,000 Da, takes a considerable time to clear from the blood. This technique usually allows 1–2 d for the streptavidin antibody to localize to the tumor. The radiolabeled biotin is administered 1 d after the clearing step. The second approach, which has been referred to as a 3-step pretargeting procedure, also involves the use of 3 agents: a biotinylated antibody, a clearing/bridging agent, and radiolabeled biotin. In this method, avidin is used as a clearing agent, because it is glycosylated and has a natural tendency to clear from the blood by binding to sugar receptors in the liver. However, avidin will also bind to the tumor-localized, biotinylated antibody. Because avidin has up to 4 binding sites for biotin, it is still available to bind the radiolabeled biotin administered in the third injection (161,162).
Although it may be debated as to which technique is best, there is a growing consensus that pretargeting can deliver as much radioactivity to a tumor as a directly radiolabeled antibody but with much less exposure to the red marrow (163,164). In addition, as with antibody fragments, the pretargeting of the radiolabeled biotin or hapten/peptide occurs very quickly, and thus the dose rate to the tumor is also higher than that observed with a directly radiolabeled IgG. Moreover, all published investigations of pretargeting report far less renal accretion of radiolabeled biotin and hapten/peptides than with radiometal-labeled antibody fragments. Although the interaction of avidin/biotin is extremely strong, both the avidin/biotin and bsmAb pretargeting methods are bound to the tumor by the primary antitumor antibody, and the residence time in the tumor will likely reflect the antibody’s binding affinity in both procedures. The avidins are immunogenic, whereas bsmAb can be humanized and, therefore, should be less immunogenic (165). Biotin occurs naturally in humans, but this does not seem to have hindered tumor targeting by these methods. Conjugates are prepared in a manner to protect against biotinylase activity.
A third type of pretargeting now explores the use of morpholinos, complementary synthetic DNA analogs, as bridging agents (166–168). These morpholino compounds should have low immunogenicity. When fully optimized, this approach could lead to further improvements in radionuclide targeting. Apart from the advantages and potential disadvantages for the bsmAb and avidin/biotin pretargeting systems that have been discussed in several reviews, all these approaches appear to hold promise as important advances in RIT (155,156).
Early imaging trials with the bsmAb and avidin/biotin pretargeting methods showed superior tumor-to-nontumor ratios in a shorter period of time than with directly radiolabeled antibody or fragments, which suggests that these methods could also be used for therapy (169–173). Axworthy et al. (174) were among the first to show that tumor uptake with a pretargeting procedure could be similar to that of a directly radiolabeled IgG while retaining superior tumor-to-nontumor ratios. Since this initial report, others have shown similar capabilities with either a bsmAb or an avidin/biotin pretargeting approach. Several investigators have reported improved therapy in a variety of models for solid tumors and hematologic malignancies when compared with results from directly radiolabeled antibodies or even antibody fragments (175–186). These promising preclinical studies resulted in several clinical therapy trials (most were phase 1 trials) designed to determine optimal targeting conditions, with subsequent accrual to determine the MTD. Despite the fact that preclinical studies show exceptionally rapid clearance of radioactivity from the blood, hematologic toxicity generally has been found to be dose limiting (187–191). In addition, reports from clinical trials using a 90Y-DOTA-biotin in conjunction with the NR-LU-10-streptavidin conjugate indicated that patients experienced severe diarrhea. However, this was most likely caused by the antibody’s specific binding to antigen in the lower GI tract and would not otherwise be expected with other pretargeting approaches (192,193). Renal toxicity was also observed. In all pretargeting approaches, the radiolabeled biotin or hapten-peptide is designed to clear quickly from the body by urinary excretion. Although renal retention of these agents is much lower than that seen with directly radiometal-labeled antibody fragments or even the radiolabeled somatostatin receptor peptides, renal toxicity is a concern.
Most clinical trials with pretargeting have involved patients with advanced cancer. Although modest but encouraging antitumor activity has been reported, these results continue to suggest that even with pretargeting, the treatment should be directed to use in patients with more radiosensitive tumors or minimal disease or in locoregional applications (188–190). For example, Paganelli et al. (194) reported a 25% objective response rate in patients with glioblastomas or astrocytomas after 2 treatments of a 3-step pretargeting procedure that used a biotinylated antitenascin antibody followed by an avidin chase/bridging step and, finally, by 90Y-DOTA-biotin. All injections were given intracranially, and, although no hematologic toxicity was reported, neurotoxicity was dose limiting. Based on these promising data, a phase 1 and 2 trial was initiated in patients with high-grade gliomas. The study included 31 patients who underwent surgical debulking followed by radiotherapy, with 19 patients subsequently receiving the intracavity pretargeting procedure. All 12 of the patients who did not receive the additional pretargeting procedure died, with a median survival of 8 mo. For the patients who received the pretargeting RIT, median survival was 33.5 mo (195). Not surprisingly, antitumor responses have been observed more frequently in patients with NHL (190,196,197). At least in the experience of Weiden et al. (190), who used a pretargeting method involving a streptavidin–rituximab conjugate, a clearing agent, and 90Y-DOTA-biotin, it appears that NHL patients might be able to tolerate only about 50% of the dose given to patients in the phase 2 trial reported by Knox et al. (192) in colorectal cancer patients, using the NR-LU-10-streptavidin conjugate followed by a clearing agent and 90Y-DOTA-biotin. A clinical trial is currently underway to test a streptavidin-anti-CD20 scFv fusion protein and a 90Y-DOTA-biotin in NHL and should thus re-examine this issue (197).
Although these early clinical trials with pretargeting have not yet produced substantial improvements in response rates in the indications in which these methods have been tested, the data continue to suggest that pretargeting can deliver at least similar, if not higher, radiation-absorbed doses to tumors per unit radioactivity administered. With evidence that higher levels of radioactivity can be administered using a pretargeting procedure than with a directly radiolabeled IgG, this should result in a higher total dose delivered to the tumors. In addition, because maximum radioactivity uptake occurs within the first few hours (whereas radiolabeled antibodies can take 1–2 d), the radiation absorbed dose rate is also increased for pretargeting. Whether these enhancements will be sufficient to improve responses remains to be determined. However, in circumstances in which a directly radiolabeled antibody can already produce significant antitumor response or improve survival, pretargeting should represent a means for reducing toxicity, particularly when the pretargeting method can deliver the same radiation dose to the tumor with less hematologic toxicity. Indeed, combinations of pretargeting approaches with chemotherapy may be better tolerated than when used with a directly radiolabeled antibody. Studies are examining combinations with chemotherapy as well as other enhancements used with directly radiolabeled antibodies that suggest that these methods will also improve radionuclide delivery with a pretargeting method (198–200). New approaches are being explored that could enhance the binding stability of antibodies to their ligands and further improve tumor retention (201). In many respects, pretargeting is still in an early stage of development, providing optimism that further advances will be forthcoming.
CONCLUSION
The history of RIT clearly indicates that the development of tumor-targeting radiolabeled antibodies is more complex than seeking a drug that affects a biochemical target. Yet in almost every preclinical model, as well as in some recent clinical studies comparing drugs with RIT in NHL, RIT has proven to be superior to chemotherapy in efficacy (137,143,202). It has also been shown that a combination of the 2 appears to be more effective than either modality alone (132,134,138,144). Therefore, scientific perspectives should be separated from commercial pressures in making an assessment of the current status and future prospects of RIT. Scientific evidence, in our view, supports the clinical prospects of this modality, but the slow adoption of the first RIT products by medical oncologists requires inducing them to become part of the management paradigm of RIT, both clinically and economically. In solid tumors, trials in minimal disease settings and involving combinations of RIT with chemotherapy should lead to better treatment outcomes. Support for such trials should come from government, regulatory, and industrial sources, with nuclear and radiation physicians championing these efforts.
Footnotes
Received Apr. 12, 2004; revision accepted Aug. 16, 2004.
For correspondence or reprints contact: David M. Goldenberg, ScD, MD, Center for Molecular Medicine and Immunology, 520 Belleville Ave., Belleville, NJ 07109.
E-mail: dmg.gscancer{at}att.net
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 188Re-ZHER2:V2, a Promising Affibody-Based Targeting Agent Against HER2-Expressing Tumors: Preclinical Assessment
- Site-Specific Radiometal Labeling and Improved Biodistribution Using ABY-027, A Novel HER2-Targeting Affibody Molecule-Albumin-Binding Domain Fusion Protein
- Treatment of Early and Established Cryptococcus neoformans Infection with Radiolabeled Antibodies in Immunocompetent Mice
- Antitumor Effects of a Human Dimeric Antibody Fragment 131I-AFRA-DFM5.3 in a Mouse Model for Ovarian Cancer
- Treatment of Advanced Pancreatic Carcinoma with 90Y-Clivatuzumab Tetraxetan: A Phase I Single-Dose Escalation Trial
- Combination Radioimmunotherapy and Chemoimmunotherapy Involving Different or the Same Targets Improves Therapy of Human Pancreatic Carcinoma Xenograft Models
- Targeting of drugs and nanoparticles to tumors
- Radioimmunotherapy with Anti-CD66 Antibody: Improving the Biodistribution Using a Physiologically Based Pharmacokinetic Model
- Radiolabeled Antibodies to Bacillus anthracis Toxins Are Bactericidal and Partially Therapeutic in Experimental Murine Anthrax
- A comparative analysis of conventional and pretargeted radioimmunotherapy of B-cell lymphomas by targeting CD20, CD22, and HLA-DR singly and in combinations
- Some like it hot: lymphoma radioimmunotherapy
- A re-examination of radioimmunotherapy in the treatment of non-Hodgkin lymphoma: prospects for dual-targeted antibody/radioantibody therapy
- Radioimmunotherapy of Experimental Human Metastatic Melanoma with Melanin-Binding Antibodies and in Combination with Dacarbazine
- Improving Anti-CD45 Antibody Radioimmunotherapy Using a Physiologically Based Pharmacokinetic Model
- Multifunctional Antibodies by the Dock-and-Lock Method for Improved Cancer Imaging and Therapy by Pretargeting
- Adjuvant and Combined Radioimmunotherapy: Problems and Prospects on the Road to Minerva
- Anti-CD45 Monoclonal Antibody YAML568: A Promising Radioimmunoconjugate for Targeted Therapy of Acute Leukemia
- Radioimmunotherapy Against the Tumor Vasculature: A New Target?
- Medullary Thyroid Cancer: Options for Systemic Therapy of Metastatic Disease?
- Enhanced Efficacy of 90Y-Radiolabeled Anti-Lewis Y Humanized Monoclonal Antibody hu3S193 and Paclitaxel Combined-Modality Radioimmunotherapy in a Breast Cancer Model
- Antibody Pretargeting Advances Cancer Radioimmunodetection and Radioimmunotherapy
- Molecular Targeting with Peptides or Peptide-Polymer Conjugates: Just a Question of Size?
- 89Zr as a PET Surrogate Radioisotope for Scouting Biodistribution of the Therapeutic Radiometals 90Y and 177Lu in Tumor-Bearing Nude Mice After Coupling to the Internalizing Antibody Cetuximab