


Abstract
The kidneys are critical organs in peptide receptor radiation therapy (PRRT). Renal function loss may become apparent many years after PRRT. We analyzed the time course of decline in creatinine clearance (CLR) in patients during a follow-up of at least 18 mo after the start of PRRT with 90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA),Tyr3-octreotide (90Y-DOTATOC) or 177Lu-DOTA0,Tyr3-octreotate (177Lu-DOTATATE). Methods: Twenty-eight patients with metastasized neuroendocrine tumors received 1–5 cycles of 90Y-DOTATOC, leading to renal radiation doses of 5.9–26.9 Gy per cycle and a total of 18.3–38.7 Gy. Median follow-up was 2.9 y (range, 1.5–5.4 y), with a median of 16 measurements (range, 5–53) per patient. Thirty-seven patients with metastasized neuroendocrine tumors received 3–7 cycles of 177Lu-DOTATATE, leading to renal radiation doses of 1.8–7.8 Gy per cycle and a total of 7.3–26.7 Gy. Median follow-up was 2.4 y (range, 1.7–4.0 y), with a median of 10 (range, 6–27) measurements per patient. All renal dose estimates were calculated with the MIRDOSE3 model. All patients were infused with renoprotective amino acids during the administration of the radioactive peptides. The time trend of CLR was determined by fitting a monoexponential function through the data of individual patients, yielding the decline in CLR in terms of percentage change per year. Results: The median decline in CLR was 7.3% per y in patients treated with 90Y-DOTATOC and 3.8% per y in patients treated with 177Lu-DOTATATE (P = 0.06). The time trend of decline in CLR was sustained during the follow-up period. Eleven patients had a >15% per y decline in CLR. Cumulative renal radiation dose, per-cycle renal radiation dose, age, hypertension, and diabetes are probable contributing factors to the rate of decline in CLR after PRRT. Conclusion: This study showed that the time course of CLR after PRRT was compatible with the pattern of sustained CLR loss in progressive chronic kidney disease.
- 90Y-DOTA0,Tyr3-octreotide
- 177Lu-DOTA0,Tyr3-octreotate
- peptide receptor radiation therapy
- radiation nephropathy
- chronic kidney disease
Peptide receptor radiation therapy (PRRT) with radiolabeled octreotide analogs is effective in patients with somatostatin receptor-positive tumors, most notably in neuroendocrine tumors. However, the radiation dose to the kidneys poses an important limit to the amount of radioactivity that can be administered safely. Renal function loss and even end-stage renal disease (ESRD) have been reported after PRRT with 90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA),Tyr3-octreotide (90Y-DOTATOC) (1,2). In the kidney, radiolabeled octreotide is efficiently reabsorbed by cells in the proximal tubule of the nephron, where a significant amount of activity is retained (3,4). From experience in external-beam radiation therapy it is generally accepted that a dose of 23 Gy to the kidneys, in fractions of about 2 Gy, leads to a 5% risk of renal failure in patients within 5 y and that a dose of 28 Gy leads to a 50% risk of renal failure within the same period (5). These figures cannot be simply translated to PRRT with radiolabeled octreotide. In PRRT, the dose rate is much lower and of longer duration than in external-beam radiation therapy. It is, therefore, important to observe renal function over a long period of time after PRRT to assess the long-term risk of clinically significant loss of renal function. We analyzed the time course of renal function loss after PRRT with 90Y-DOTATOC and 177Lu-DOTA0,Tyr3-octreotate (177Lu-DOTATATE) in patients during a follow-up period of at least 18 mo after the start of treatment.
In addition, we present an overview of the reported aspects involved in renal function loss after PRRT, as well as measures for prevention or treatment, including coinfusion of amino acids (4,6–8).
MATERIALS AND METHODS
PRRT with 90Y-DOTATOC
Patients in this study were all veterans of a multicenter phase 1, uncontrolled, open-label vertical (per cycle) and horizontal (number of cycles) dose-escalation study (9,10). The primary goals were to establish the single-cycle and 4-cycle maximum tolerated doses of 90Y-DOTATOC (90Y-SMT487, 90Y-edotreotide; Octreother, Novartis) and to evaluate immediate, 6-mo, and long-term (18-mo) safety profiles. All patients gave written informed consent. The study was approved by the local ethical committees of the 3 participating centers. Before entering the therapy study, all patients had undergone 86Y-DOTATOC PET for dosimetry (7). Biochemical data over 48 h; data from PET scans at 3.5, 24, and 48 h after injection; and the MIRDOSE program (version 3.1) were used to calculate dosimetry estimates for 90Y-DOTATOC in a reference human. Patients were not allowed to receive doses of more than 27 Gy of 90Y-DOTATOC to the kidneys within the frame of the study, although patients could receive extra cycles off protocol if the attending physicians judged that the benefit of treatment outweighed the risks.
The initial administered activity of 90Y-DOTATOC was 925 MBq/m2/cycle. Vertical escalation proceeded at 925 MBq/m2/cycle intervals for subsequent cohorts of patients. Patients were allowed to receive up to 4 cycles of their cohort activity (horizontal escalation). The interval between treatments was 6–9 wk. In the later phase of the study, the protocol was amended to allow further escalation of the activity per cycle. These patients then received several full cohort activities and a final smaller remainder of activity as the last cycle, until their measured cumulative renal radiation dose was reached.
For renal protection purposes all patients were coinfused with 2 L of a mixed amino acid solution over 4 h during the treatments with 90Y-DOTATOC, as in previous dosimetry studies with 86Y-DOTATOC (7).
Sixty patients were originally included in the study, of whom 30 were followed for at least 18 mo after the start of the first treatment cycle. Two patients were excluded because the uptake of 86Y-DOTATOC in the kidneys had not been measurable by PET, leaving 28 patients to be included in this analysis. Four of these 28 patients received renal radiation doses that differed from the planned dose of 27 Gy. One patient did not receive her last planned cycle because of persistent thrombopenia, and 3 patients, because of tumor status, were administered additional cycles while they had no evidence of renal toxicity. Table 1 includes relevant clinical details.
Clinical Parameters and Changes in Creatinine Clearance
PRRT with 177Lu-DOTATATE
Patients participated in an open-label phase 1 and 2 study on the side effects and the antitumoral effects of 177Lu-DOTATATE therapy, which has been ongoing in Rotterdam since 2000. All patients gave written informed consent to participate in the study, which was approved by the medical ethical committee of the hospital. Initial results of this study were published previously (11).
177Lu-DOTATATE was prepared as described previously (12). A concomitant infusion of amino acids (lysine 2.5% and arginine 2.5% in 1 L 0.9% NaCl at 250 mL/h for 4 h) was started 30 min before administration of the radiopharmaceutical (8). The radiopharmaceutical was coadministered through a second pump system. The administered activity per cycle was initially 1.85 GBq of 177Lu-DOTATATE. After escalation of the cycle activity in 1.85 GBq increments, the administered activity per cycle was determined at 7.4 GBq. The interval between treatments was 6–9 wk. Patients were treated up to a cumulative activity of 27.8–29.6 GBq (corresponding to a radiation dose to the bone marrow of 2 Gy), unless dosimetric calculations indicated that the radiation dose to the kidneys would then exceed 23 Gy. In these cases, cumulative activity was reduced appropriately. Dosimetry was based on serial planar scans obtained over several days after the first administration of 177Lu-DOTATATE. Calculations were performed using the MIRDOSE3 package, with S factors for 177Lu (12).
More than 300 patients had already been included in the 177Lu-DOTATATE study. Forty-three patients were followed for at least 18 mo after the start of the first treatment cycle. Six patients were excluded because uptake of 177Lu-DOTATATE in the kidneys was not measurable for dosimetry, leaving 37 patients to be included in this analysis. Table 1 includes relevant clinical details
Follow-Up and Data Analysis
Creatinine clearance (CLR) was chosen as an estimate of the glomerular filtration rate (GFR). In all patients administered 90Y-DOTATOC, CLR was determined at baseline based on two 24-h urine collections and serum creatinine (s-creat). This method is cumbersome, prone to sampling errors, and may vary from day to day, frequently by as much as 10%–20%. Changes during follow-up were assessed by calculated creatinine clearance (c-CLR) using the Cockcroft–Gault formula:
 in men and 15% less in women (13). The Cockcroft–Gault formula is a widely used, simple, and reproducible method to estimate CLR. However, the accuracy of this formula in predicting true CLR is limited, especially in patients with extensive liver disease and in end-stage patients. Therefore, a correction factor was calculated for each individual to compensate for the ratio between true CLR and c-CLR at baseline. All subsequent c-CLR values for that patient were multiplied by this factor to yield CLR. In this way, we combined the accuracy of measured CLR from 24-h urine collections with the reproducibility of c-CLR by the Cockcroft–Gault formula. To determine the percentage change in CLR per year, a monoexponential curve was fitted through the CLR data of each patient, from the start of treatment onward. The 95% confidence interval (CI) of the percentage change in CLR was calculated for each patient. Mean values ± SD were reported, unless indicated otherwise. For differences between patient groups, unpaired t tests or Mann–Whitney tests (continuous variables) or χ2 tests (ordinate variables) were used. The influence of age, hypertension, diabetes, and renal radiation dose per cycle on the percentage change in CLR as dependent variables was tested by univariate ANOVA in the combined group of 90Y-DOTATOC and 177Lu-DOTATATE patients (n = 65). For patients with different cycle doses, the highest dose was chosen. Statistical calculations were performed with version 10.0 of the package SPSS (SPSS, Inc).
in men and 15% less in women (13). The Cockcroft–Gault formula is a widely used, simple, and reproducible method to estimate CLR. However, the accuracy of this formula in predicting true CLR is limited, especially in patients with extensive liver disease and in end-stage patients. Therefore, a correction factor was calculated for each individual to compensate for the ratio between true CLR and c-CLR at baseline. All subsequent c-CLR values for that patient were multiplied by this factor to yield CLR. In this way, we combined the accuracy of measured CLR from 24-h urine collections with the reproducibility of c-CLR by the Cockcroft–Gault formula. To determine the percentage change in CLR per year, a monoexponential curve was fitted through the CLR data of each patient, from the start of treatment onward. The 95% confidence interval (CI) of the percentage change in CLR was calculated for each patient. Mean values ± SD were reported, unless indicated otherwise. For differences between patient groups, unpaired t tests or Mann–Whitney tests (continuous variables) or χ2 tests (ordinate variables) were used. The influence of age, hypertension, diabetes, and renal radiation dose per cycle on the percentage change in CLR as dependent variables was tested by univariate ANOVA in the combined group of 90Y-DOTATOC and 177Lu-DOTATATE patients (n = 65). For patients with different cycle doses, the highest dose was chosen. Statistical calculations were performed with version 10.0 of the package SPSS (SPSS, Inc).
RESULTS
Two patients developed delayed radiation nephropathy after PRRT with 90Y-DOTATOC. One patient (patient 7, Table 2) received a total of 11.6 GBq, equally divided over 4 treatments. Her renal radiation exposure was 27.5 Gy, based on 86Y-DOTATOC PET imaging. She experienced worsening of preexisting hypertension and mild proteinuria from 1 y onward, with concurrent increasing s-creat and urea levels. A renal biopsy was consistent with radiation nephropathy (14). At 4.5-y follow-up after the first treatment, s-creat and urea levels were consistent with National Cancer Institute (NCI) common toxicity criteria grade 3, indicating that she would soon require dialysis. A second patient (patient 1, Table 2) showed clinical signs of radiation nephropathy at 12 mo, with decreasing renal function (grade 3 s-creat) at 18 mo after his first treatment. He had received a cumulative activity of 22.9 GBq (first cycle, 13.7 GBq), with a renal radiation dose of 27.0 Gy based on 86Y-DOTATOC PET imaing. In the other 26 patients we observed maximal grade 2 renal toxicity during the follow-up period. Hypertension or worsening of preexisting hypertension occurred in 6 patients, including the 2 described previously. Only mild proteinuria was observed. Among the patients treated with 177Lu-DOTATATE, a single patient experienced early onset renal insufficiency. This patient had a baseline CLR of 41 mL per min and unexplained rises in s-creat levels in the year before PRRT. Because of the short follow-up period, this patient was not included in the current analysis.
Patients with More Than 15% per Year Decline in Creatinine Clearance
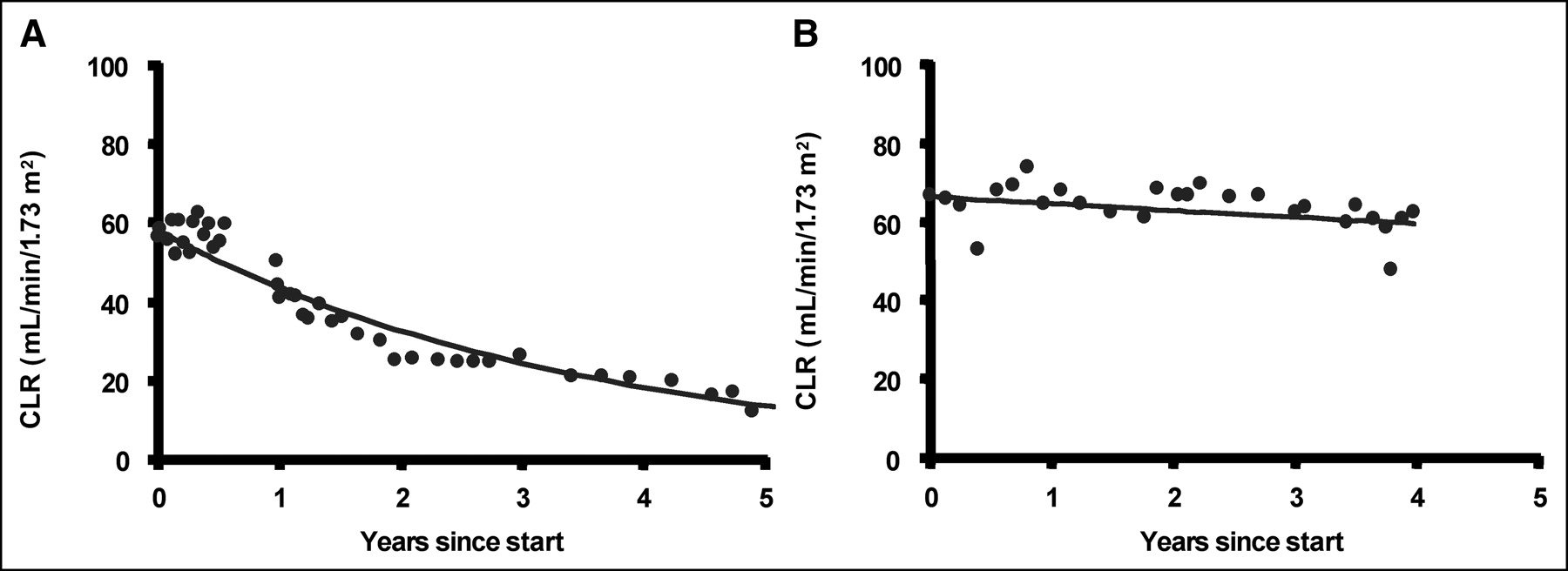
The observed percentage change in CLR differed widely among individual patients, but in most there was a clear, sustained decline in CLR throughout the follow-up period. In patients with a high loss of CLR in the first year after the start of treatment, this loss continued at a similar rate thereafter. Conversely, patients with stable CLR during the first years remained stable later (Fig. 1). Several patients treated with 177Lu-DOTATATE showed an apparent improvement in CLR, which was caused by their rapid weight gain rather than a decline in s-creat values. This gain in weight often was associated with a clear improvement in clinical condition as a result of a good response to treatment. However, we suspect that the true improvement in CLR is less than indicated by the Cockcroft–Gault formula, which was derived from a cross-sectional study in patients with a stable clinical condition (13). Therefore, we decided to use the baseline weight as a constant for weight in the follow-up of CLR calculations for all 177Lu-DOTATATE patients. This may have slightly overestimated the average decline in CLR in this group. The median CLR loss per patient was higher in the 90Y-DOTATOC patients than in 177Lu-DOTATATE patients but was not statistically significant (Mann–Whitney test, Table 1). The distribution of CLR change values was abnormal, and the 90Y-DOTATOC group contained a greater proportion of extreme values (P = 0.007; Moses extreme reactions test). There appeared to be a separate cluster of patients who had CLR losses of >15% per year (9 in the 90Y-DOTATOC group and 2 in the 177Lu-DOTATATE group) (Fig. 2, Table 2). From the data presented in Table 2, it is clear that most of these patients were at least 60 y old and that maximum renal radiation dose per cycle and hypertension may have been determining factors. In total, 2 patients had a combination of hypertension and diabetes and both had a very high rate of decline in CLR after PRRT. The univariate ANOVA showed significance for hypertension (n = 14; P = 0.005) and per-cycle radiation dose >14 Gy (n = 11, all 90Y-DOTATOC; P < 0.0005) as separate factors but not for diabetes (n = 11; P = 0.43) or age >60 y (n = 27; P = 0.37). However, the combination of hypertension, age, and diabetes (n = 2; P = 0.046) was significant in this 4-factor model (adjusted R2 = 0.45). Moreover, hypertension and age were related factors. The mean age was 62.8 ± 8.7 y in patients with hypertension (n = 14) and 55.6 ± 11.2 y in patients without hypertension (n = 51; P = 0.03, t test).
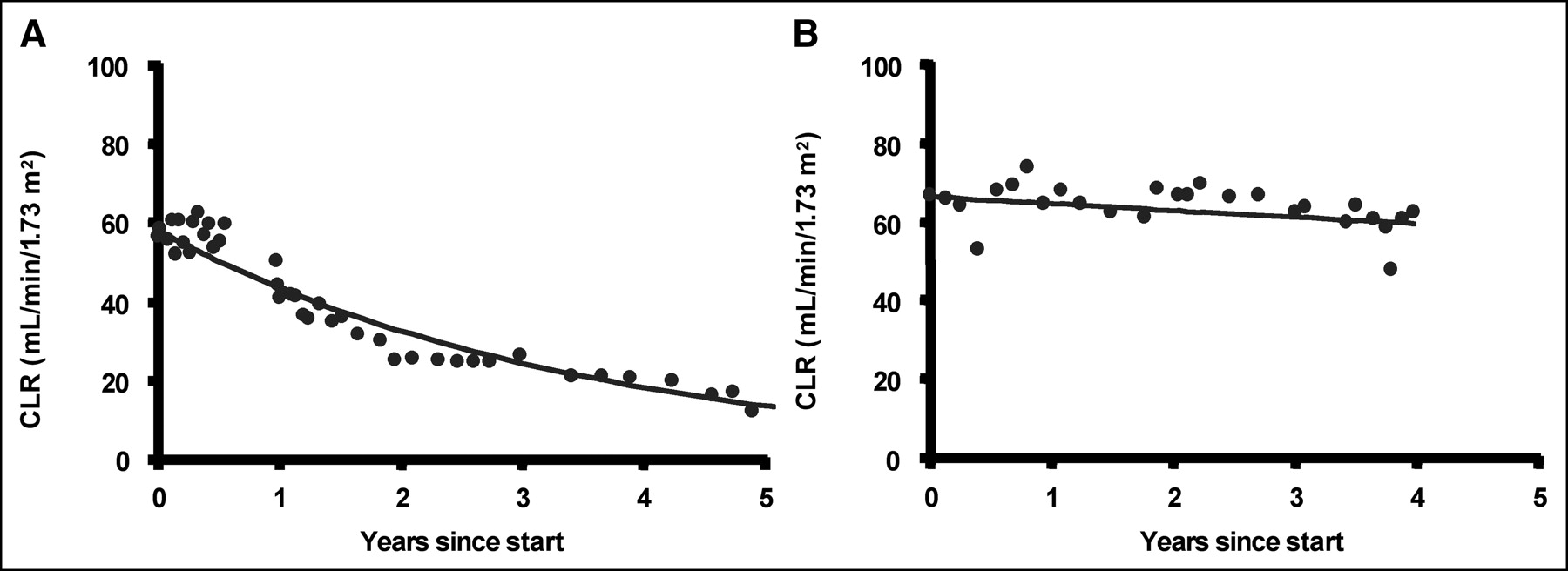
Time course of CLR and fitted monoexponential decay. (A) Patient was 75-y-old woman with insulinoma and hypertension who received 11.6 GBq of 90Y-DOTATOC, with estimated renal dose of 27.5 Gy. CLR loss was 26%/y (95% CI, 24.4%–27.5%), with ESRD at 5 y after first treatment. (B) Patient was 52-y-old man with papillary thyroid carcinoma who received 25.9 GBq of 177Lu-DOTATATE, with estimated renal dose of 23.3 Gy. CLR loss was 2.7%/y (95% CI, 0.2%–5.0%).
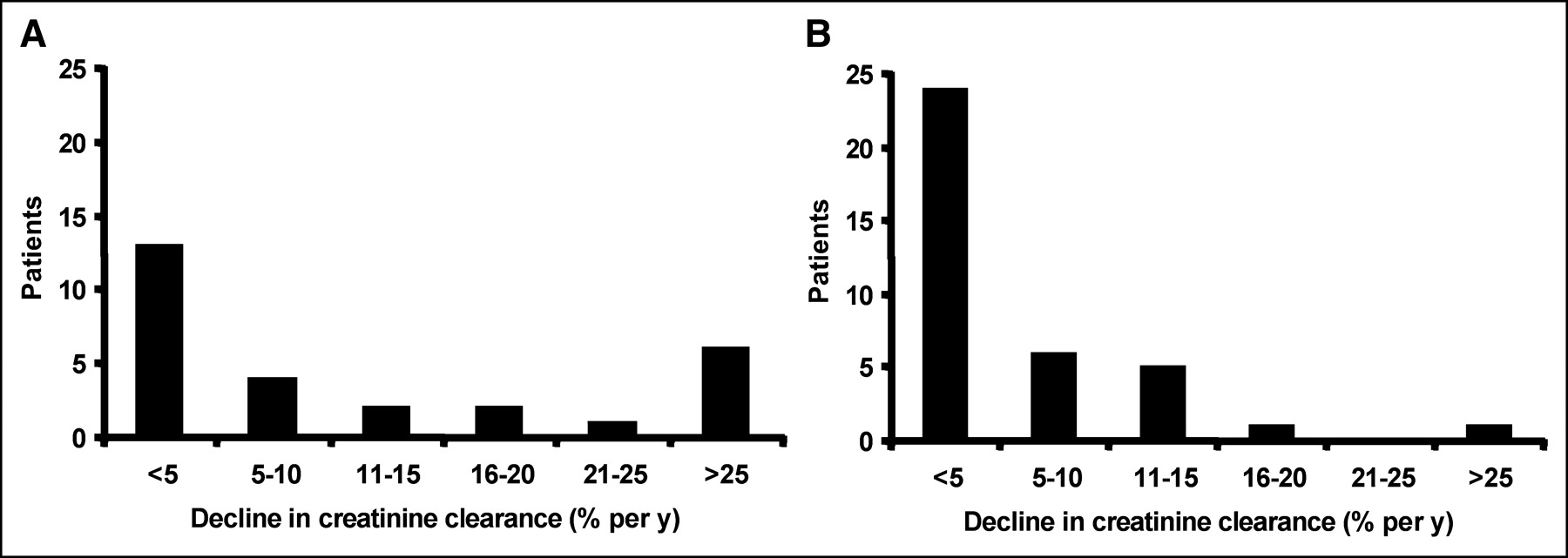
Comparison of decline in CLR in 28 patients treated with 90Y-DOTATOC (A) and 37 patients treated with 177Lu-DOTATATE (B). Especially with 177Lu-DOTATATE, most patients have CLR loss <5%/y (normal age-related CLR loss is 1%/y). Only patients with CLR loss >25%/y are expected to develop ESRD within 5 y.
In patient 1 in the 177Lu-DOTATATE group (Table 2), the high loss in CLR may be attributed in part to a hepatorenal syndrome in the presence of extensive liver metastases, in addition to the combination of age, hypertension, and diabetes mellitus.
The majority of patients showed a <15% yearly decline in CLR (19 of 28 patients in the 90Y-DOTATOC group and 35 of 37 patients in the 177Lu-DOTATATE group). Within this large combined subgroup, the distribution of CLR rates was within normal limits (P = 0.27, Kolmogorov–Smirnov test). There was no significant difference between the mean yearly decline in CLR between the 90Y-DOTATOC (3.7%/y) and 177Lu-DOTATATE subgroups (3.9%/y; P = 0.92), despite significant differences in cumulative renal radiation dose (26.9 ± 3.7 Gy and 19.7 ± 4.4 Gy, respectively; P < 0.0005) and per-cycle dose (10.5 ± 5.7 Gy and 4.7 ± 1.5 Gy, respectively; P < 0.0005).
The expected time to ESRD (defined as CLR <15 mL/min/1.73 m2) was calculated using the baseline CLR and the decline in CLR. Only in patients with a yearly loss in CLR >25% could ESRD be expected to occur within 5 y after the start of treatment (Table 2).
In Figure 3, another more straightforward and simplified approach is presented. For patients treated with 90Y-DOTATOC, hypertension, age, diabetes, and renal radiation dose >14 Gy per cycle were taken as risk factors for a decline in CLR of >20% and an associated high risk of ESRD within 5 y (Fig. 3A). This approach was repeated for the combined 90Y-DOTATOC and 177Lu-DOTATATE groups, with a cumulative renal radiation dose >25 Gy as an additional risk factor (Fig. 3B). The prevalence of >20% decline in CLR increased sharply when the number of risk factors increased within the 90Y-DOTATOC group (P = 0.021, Pearson χ2; Spearman rank correlation coefficient = 0.61) or when both groups were combined (P < 0.0005, Pearson χ2; Spearman rank correlation coefficient = 0.52).

(A) Yearly loss in CLR >20% (black bars) and <20% (white bars) in 28 patients treated with 90Y-DOTATOC who had 0–4 risk factors from hypertension, diabetes, age >60 y, and maximal per-cycle renal radiation dose >14 Gy. (B) Yearly loss in CLR >20% and <20% in 65 patients treated with 90Y-DOTATOC or 177Lu-DOTATATE who had 0–5 risk factors from hypertension, diabetes, age >60 y, cumulative renal radiation dose, and maximal per cycle radiation dose.
DISCUSSION
Nephrotoxicity from PRRT with 90Y-DOTATOC has been recognized as an important clinical problem that has been discussed in the literature (15–23). Cumulative experience with 90Y-DOTATOC by the Basel group consists of a pilot study with 29 patients (1), 2 phase 2 clinical studies with 41 patients (24) and 39 patients (25), and a study in 20 patients with medullary thyroid cancer (26). They reported 4 cases of early renal insufficiency and 2 additional cases of delayed renal failure (1,2,27) from their initial study, without amino acids for renal protection. In their later studies, always performed with amino acids, only a single patient was reported with late grade 2 renal toxicity (25). The cumulative experience from Milan was reported in 3 studies, with a total of 128 patients who received different regimens of amino acids (28–30). In addition, many patients were treated outside protocols, reaching a total of 256 patients (29). None of the patients developed acute renal toxicity, although 1 had delayed grade 2 toxicity, 2 had delayed grade 1 toxicity, and 2 had transient grade 1 toxicity. We have previously reported preliminary results from a multicenter dose-escalating phase 1 and 2 study of 60 patients who all received amino acids for renal protection (10). At the time of analysis, one patient was reported with delayed grade 3 renal function loss. Together, these reports include more than 400 patients treated with 90Y-DOTATOC, including 7 patients with severe and 6 patients with mild renal toxicity. These used different administered activities, renal dosimetry estimations, renal protection schemes, and follow-up periods.
In the current study, we analyzed the time course of the most relevant parameter of renal function, the GFR, at individual and group levels in patients with long follow-up after PRRT with 90Y-DOTATOC or 177Lu-DOTATATE. Because we had long-term follow-up with many measurements per patient, the time trends in CLR (as a substitute for GFR) could be reliably assessed on an individual basis. Our results demonstrated that after PRRT, individual rates of decline vary widely among patients. In those patients who have a decline in CLR, this decline is sustained during the entire follow-up period after the start of therapy. This suggests that treatment with radioactive peptides may trigger a process at the level of the glomerulus that continues long after the end of radiation exposure.
We encountered no clinically notable impairment of tubular function, such as excessive loss of electrolytes, changes in phosphate reabsorption, or failure to concentrate urine, either shortly after administration of PRRT or during long-term follow-up. This is entirely in agreement with the histopathologic findings of radiation nephropathy as reported previously (27). In biopsies of 3 patients with renal insufficiency after PRRT with 90Y-DOTATOC, typical signs of thrombotic microangiopathy (TMA) involving glomeruli, arterioles, and small arteries were seen, as well as tubular atrophy and interstitial fibrosis. Comparing patient data with the earlier report of this group, we estimate that biopsies were taken between 1 and 2 y after the start of the therapy (1). A similar case was reported by Stoffel et al. (31), who also found prominent glomerular changes accompanied by tubular atrophy and compensatory interstitial fibrosis in a biopsy of a patient who developed renal insufficiency 1 y after PRRT with 90Y-DOTATOC.
In our series, renal biopsies were performed in 3 patients. In 1 patient with declining renal function, the biopsy showed signs of TMA, consistent with radiation nephropathy (14). In 2 other patients, renal biopsies were performed after an extra cycle of PRRT. They showed no clinical or biochemical signs of renal failure, and their renal biopsies were normal. Declines in their CLRs were 2% per y (95% CI, 0.7%–3.3%/y) and 9.4% per y (95% CI, 6.3%–12.4%/y), respectively.
From histologic studies it is known that the major focus of changes after external-beam irradiation is in the arteriolar–glomerular area, rather than the tubular epithelium, leading to glomerular sclerosis, and that the common denominator linking radiation nephropathy and TMA is presumably endothelial cell injury (32,33). Such changes may be seen many years after the radiation exposure.
Clinical observation of steadily progressive loss of CLR, with wide variations among individual patients, and the type of histologic changes as seen after PRRT with 90Y-DOTATOC or external-beam radiation are compatible with the clinical and histologic spectrum of chronic kidney disease. Chronic kidney disease is defined clinically as either kidney damage or GFR <60 mL/min/1.73 m2 for more than 3 mo (34). The leading causes of chronic kidney disease are hypertension and diabetes mellitus, but many other causes are known (34,35). It is now becoming accepted that progressive renal disease cannot be attributed to a single aberration in glomerular physiology but is characterized by a progressive loss of the microvasculature (36,37). The pathophysiology of chronic renal failure is complex. Regardless of the primary cause of nephron loss, some glomeruli usually survive or are less severely damaged. Adaptation mechanisms involve hypertrophy of the remaining glomeruli, with a cascade of events that has been termed “the final common path,” in which the adaptation processes eventually cause further loss of nephrons, leading to progressive loss of function. Well documented intermediate agents for these deleterious processes are angiotensin II, endothelin, and transforming growth factor.
With renal microvascular injury and the central role of the renin–angiotensin system in this process, it is clear that hypertension and diabetes may accelerate renal function loss in chronic kidney disease. In clinical practice, drugs that interfere with the renin–angiotensin system, such as angiotensin-converting enzyme (ACE) inhibitors and angiotensin II inhibitors, are becoming the drugs of choice in slowing down the progression of chronic renal failure (35). In radiation nephropathy, experimental studies have also demonstrated the pivotal role of the renin–angiotensin system and the efficacy of ACE-inhibitors and angiotensin II inhibitors in diminishing the incidence of renal failure (38,39). Angiotensin II blockade was also successful in a patient with late radiation nephropathy (40).
In our study, 11 of 65 patients had a >15% yearly loss of CLR (Table 2). We infer from our observations that hypertension, old age, and diabetes (particularly in combination with hypertension) may be relevant risk factors (Table 2, Fig. 3). Paganelli et al. (28) cited preexisting hypertension as a possible contributing factor in their single patient with grade 2 renal toxicity after PRRT with 90Y-DOTATOC.
Despite the contributing role of hypertension, age, and diabetes, the most prominent cause of renal toxicity with PRRT is probably the radiation to the kidney. The significant differences in cumulative renal radiation dose and renal radiation dose per cycle may be the most important factors to account for the fact that 9 out of 28 patients treated with 90Y-DOTATOC had high yearly losses of CLR, compared with 2 out of 37 177Lu-DOTATATE patients. The numbers of patients with hypertension, old age, and diabetes were comparable in the 2 treatment groups. Therefore, it is possible that these risk factors become relevant only in the presence of a high cumulative or per-cycle radiation dose to the kidneys. On the other hand, it is reassuring that the risk of severe renal function loss seems low after PRRT with either 90Y-DOTATOC or 177Lu-DOTATATE in the absence of additional factors. At present, subtle dependencies between the proposed risk factors or relative weight of such factors are uncertain.
Unfortunately, it is difficult to derive from available studies a clear relationship between cumulative or per-cycle radiation dose and renal damage. In the studies from the Basel group, no individual dosimetry is reported, whereas the Milan group reported only individual dosimetry in a limited number of patients (30). An extensive dosimetric study in 18 patients using 111In-DOTATOC predicted variable absorbed renal doses (3.31 ± 2.22 mGy/MBq) during treatment with 90Y-DOTATOC, but the outcome after therapy was not reported specifically for these 18 patients (41). In a recent review from the Milan group, 16 other patients were evaluated, with cumulative administered activities of 4.1–13.9 GBq of 90Y-DOTATOC, renal radiation doses of 1.6–6.0 mGy/MBq, and cumulative renal radiation doses of 6.6–47.1 Gy (42). During a follow-up period of 6–50 mo, 4 of these 16 patients developed NCI grade 1 s-creat levels, apparently not clearly correlated to the cumulative or per-cycle renal radiation dose.
In our studies, there was a substantial variation in uptake of 86Y-DOTATOC and in mean residence time in the kidneys between individual patients, leading to different cumulative activities of 90Y-DOTATOC required to reach the targeted renal radiation dose of 27 Gy (7). These differences are clear from the patient data in Table 2. A similar variability in the relation between administered activity and estimated renal radiation dose was found in the 177Lu-DOTATATE patients, despite the different method that was used. Renal dose calculations were based on the MIRDOSE3 model, which assumes a homogeneous distibution of activity in a standard-sized kidney volume. Alternative methods include individual renal volume and inhomogeneous activity distributions. The results of these new approaches, which lead to a better (radiation) dose–effect relationship, are discussed by Pauwels et al. (43) elsewhere in this supplement.
The average distance from the tubular uptake (source) and the glomerulus (being the relevant target) is probably important for the dosimetry of different radionuclides that may be coupled to the peptides. The range of β-particles from 90Y is maximally 12 mm, long enough to reach the glomeruli, whereas the low-energy Auger electrons travel only 10 μm, not far enough to leave the tubular cell. The range of the 177Lu electrons is maximally 2.1 mm, thus the sensitive glomeruli may be partially spared. This means that 1 Gy from 177Lu may lead to a lower average glomerular dose than 1 Gy from 90Y, which may be an additional explanation for the much lower average decline in CLR in the 177Lu-DOTATATE patients than in the 90Y-DOTATOC patients. This also provides an explanation for the low renal toxicity (5 patients with grade 1 s-creat) in 50 patients who were treated with high doses of 111In-diethylenetriaminepentaacetic acid (DTPA) octreotide (111In-pentetreotide; OctreoScan), despite high renal dose estimates up to 45 Gy in 2 patients who were treated with a cumulative activity of >100 GBq (44). In a study including 27 patients treated with 111In-DTPA-octreotide, one patient developed grade 2 renal toxicity, but this may have been caused by bilateral ureter obstruction rather than radiation nephropathy (45). Apart from a better scientific understanding of renal radiation dosimetry with PRRT, it is of utmost importance to have simple and practical dosimetric methods to be used in daily practice. Dosimetry methods based on 111In-DTPA-octreotide scans or in combination with simple clinical parameters have been developed (46). Other methods are probably more accurate, based on the use of the chemically identical 86Y-DOTATOC or nearly identical 111In-DOTATOC, but these radiopharmaceuticals are not readily available (7,41).
Prevention of radiation nephropathy from PRRT can be accomplished in different ways. The affinity of radiolabeled 177Lu-DOTATATE for the type 2 somatostatin receptors is twice as high as the affinity of 90Y-DOTATOC, which gives a greater tumor-to-kidney uptake ratio and a better therapeutic window (47). The uptake mechanism of radiolabeled peptides in the kidney is mainly tubular reabsorption, not receptor binding. Coinfusion of positively charged amino acids, in particular lysine and arginine, has been found to be useful in experimental and clinical studies to counteract the reabsorption of peptides (4). Hammond et al. (6) showed that a mixture of amino acids inhibited the uptake of radiolabeled octreotide. Typically, renal dose reductions of 25% can be reached with these mixed amino acids. Additional investigations revealed that solutions with a combination of 25 g of lysine and 25 g of arginine in 1 L were safe and more effective than mixed amino acids (Fig. 4) (8). We now routinely use this combination in all patients receiving 177Lu-DOTATATE. Alternative amino acid regimens have been investigated in Milan, with an average reduction in kidney dose of 25% (30). Reductions in renal radiation dose of up to 65% can be reached when additional 4-h amino acid infusions are administed 1 and 2 d after therapy (42). New studies in rats have shown that 1 mg per kg of colchicine, which disrupts cellular microtubules, adds significantly to the renal-protecting effects of lysine, which may be promising for future clinical use (48). Further prevention of renal radiation damage may be achieved by treatment with ACE inhibitors or angiotensin II inhibitors, in parallel with the recommendations for treatment of chronic kidney disease and with emerging experimental and clinical results with these drugs in external-beam radiation nephropathy.
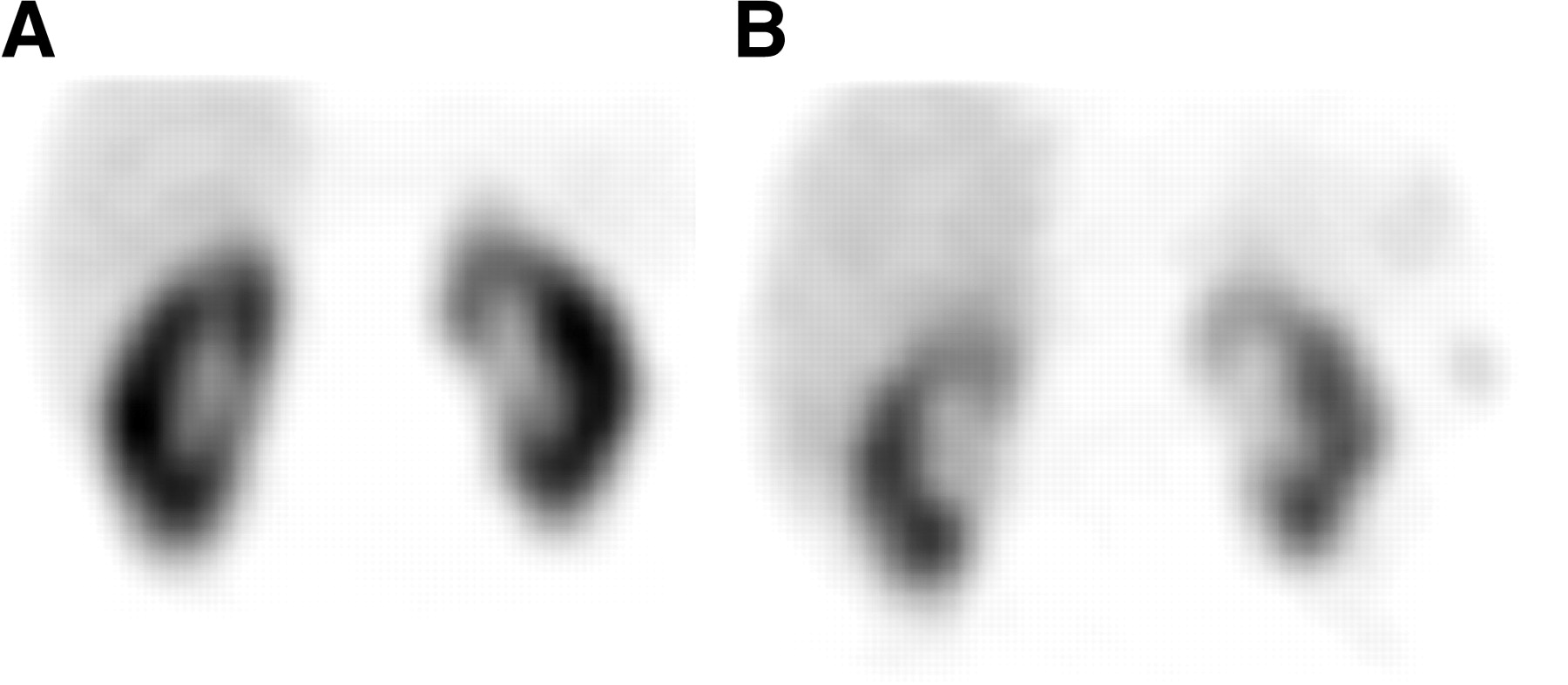
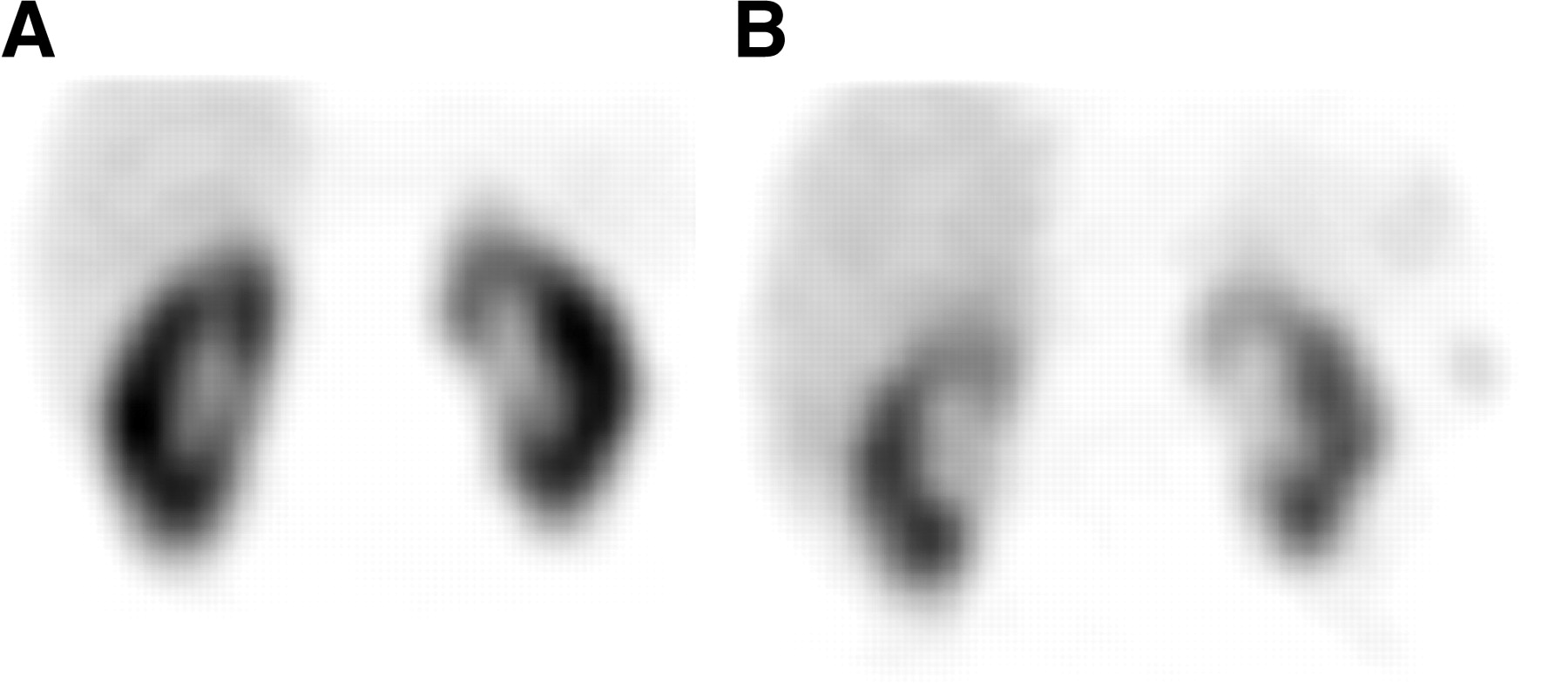
Coronal SPECT images 24 h after injection of 220 MBq 111In-DTPA-octreotide in the same patient at separate occasions. (B) Study was performed with coinfusion of lysine 25 g + arginine 25 g in 1,000 mL, with 40% reduction of renal activity compared with the control investigation (8).
With the assessment of renal toxicity by the commonly used NCI grades 0–4 for s-creat and blood urea nitrogen, it is difficult to predict which patient will develop nephrotoxicity after PRRT. On the basis of the time trend in c-CLR, one may predict, within a certain margin of error, when a patient will develop ESRD, even at a time when the s-creat is still NCI grade 1 or 2. This agrees with the guidelines for the diagnosis and treatment of chronic kidney disease, in which serial monitoring of CLR is recommended in all patients with GFR <60 mL/min/1.73 m2, to install treatment to slow down the rate of loss in GFR (34).
Limitations of the Study
The PRRT studies with 90Y-DOTATOC and with 177Lu-DOTATATE were performed as separate open-label phase 1 and 2 studies and not as a single comparative study. However, many features of the studies were similar, in particular the population of patients with mainly neuroendocrine tumors and the prospective method of planned follow-up of renal function in all patients. As a result, both groups had comparable baseline characteristics (Table 1). Therefore, we think that the analysis of the individual time trends, based on prospectively gathered data, is valid. Additional analysis was performed retrospectively, based on observations from the group of patients studied. Information about hypertension and diabetes mellitus status was taken from patient charts, and not formulated prospectively in the protocols. Moreover, the risk factors that we found in this study are not independent of each other, which may have induced bias. We propose that in future trials of PRRT the contribution of all risk factors for renal function loss should be studied prospectively.
CONCLUSION
Our data demonstrate that PRRT with 90Y-DOTATOC leads to a decline in CLR, which is sustained at the same rate during years of follow-up and may vary between patients from no measurable loss to a loss of more than 50% per year. Probable contributing factors are the cumulative and per cycle renal radiation dose, age, hypertension, and diabetes, but the number of patients in this study is too small to allow definitive conclusions. In the absence of additional contributing factors, the rate of decline in CLR is low, and ESRD is not expected to occur within 5 y after PRRT with 90Y-DOTATOC. The average rate of decline in CLR is less in patients treated with 177Lu-DOTATATE, who received a lower renal radiation dose. This is encouraging, because with the chosen administered activities, both treatments are effective in patients with neuroendocrine tumors as PRRT with 90Y-DOTATOC, as described elsewhere in this issue (49). The pattern of CLR loss is compatible with that of chronic kidney disease from other causes; the histologic changes found in patients after 90Y-DOTATOC therapy resemble closely the changes as reported after external-beam radiation therapy and resemble the glomerular/microvascular changes as reported in progressive renal failure. This suggests that the spectrum of radiation nephropathy after PRRT and external-beam radiation therapy fits within the multifactorial pathophysiology of chronic kidney disease with its final common pathway leading to ESRD. To prevent unnecessary risks of PRRT, we recommend that radiolabeled peptides with high specific receptor binding be used, that the administration of PRRT be accompanied by amino acids, and that hypertension, diabetes mellitus, and other known risk factors of chronic kidney disease be considered in the treatment of individual patients. The current treatment schedule of 90Y-DOTATOC as used in phase 2 studies is a fixed cumulative activity of 13.3 GBq, divided in 3 equal cycles of 4.4 GBq. With this schedule the renal dose per cycle remains low; thus a high dose per cycle is no longer a practical risk factor. In addition, simplified dose estimation using 111In-pentetreotide scans may be considered to identify patients with exceptionally high renal uptake of peptides and thus a risk of high cumulative renal radiation dose with PRRT.
Acknowledgments
We are grateful for support from the nursing staff in the participating centers, in particular Joelle de Camps, Jane Hadley, and Jolande Kip. The phase 1 study with 90Y-SMT487 was sponsored by Novartis Pharmaceuticals. Principle investigators were Stanislas A. Pauwels, MD; Larry K. Kvols, MD; and Eric P. Krenning, MD.
Footnotes
Received Jun. 17, 2004; revision accepted Sep. 30, 2004.
For correspondence or reprints contact: Roelf Valkema, MD, Department of Nuclear Medicine, Erasmus Medical Center, Dr Molewaterplein 40, Rotterdam, The Netherlands 3015 GD.
E-mail: r.valkema{at}erasmusmc.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Long-Term Nephrotoxicity of 177Lu-PSMA Radioligand Therapy
- Safety of Peptide Receptor Radionuclide Therapy with 177Lu-DOTATATE in Neuroendocrine Tumor Patients with Chronic Kidney Disease
- The Effects of Monosodium Glutamate on PSMA Radiotracer Uptake in Men with Recurrent Prostate Cancer: A Prospective, Randomized, Double-Blind, Placebo-Controlled Intraindividual Imaging Study
- Phase I study of the 177Lu-DOTA0-Tyr3-Octreotate (lutathera) in combination with nivolumab in patients with neuroendocrine tumors of the lung
- Recombinant {alpha}1-Microglobulin Is a Potential Kidney Protector in 177Lu-Octreotate Treatment of Neuroendocrine Tumors
- Proof of Therapeutic Efficacy of a 177Lu-Labeled Neurotensin Receptor 1 Antagonist in a Colon Carcinoma Xenograft Model
- 177Lu-DOTATATE PRRT in Patients with Metastatic Neuroendocrine Tumor and a Single Functioning Kidney: Tolerability and Effect on Renal Function
- Feasibility of Affibody-Based Bioorthogonal Chemistry-Mediated Radionuclide Pretargeting
- MIRD Pamphlet No. 26: Joint EANM/MIRD Guidelines for Quantitative 177Lu SPECT Applied for Dosimetry of Radiopharmaceutical Therapy
- GEP-NETS UPDATE: Radionuclide therapy in neuroendocrine tumors
- Individualized Dosimetry of Kidney and Bone Marrow in Patients Undergoing 177Lu-DOTA-Octreotate Treatment
- Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs)
- 68Ga-DOTATOC Versus 68Ga-DOTATATE PET/CT in Functional Imaging of Neuroendocrine Tumors
- Nuclear medicine techniques for the imaging and treatment of neuroendocrine tumours
- In Vitro Evaluation of Targeted Antisense 177Lu Radiotherapy
- Phase I Trial of 90Y-DOTATOC Therapy in Children and Young Adults with Refractory Solid Tumors That Express Somatostatin Receptors
- 68Ga-DOTATATE PET/CT for the Early Prediction of Response to Somatostatin Receptor-Mediated Radionuclide Therapy in Patients with Well-Differentiated Neuroendocrine Tumors
- MIRD Pamphlet No. 20: The Effect of Model Assumptions on Kidney Dosimetry and Response--Implications for Radionuclide Therapy
- Treatment With the Radiolabeled Somatostatin Analog [177Lu-DOTA0,Tyr3]Octreotate: Toxicity, Efficacy, and Survival
- Utility of Radiolabeled Somatostatin Receptor Analogues for Staging/Restaging and Treatment of Somatostatin Receptor-Positive Pediatric Tumors
- Gastrointestinal neuroendocrine tumors: a role for targeted therapies?
- Radiation Dose Distribution in Human Kidneys by Octreotides in Peptide Receptor Radionuclide Therapy
- Dosimetry in Peptide Radionuclide Receptor Therapy: A Review
- Gelatin-Based Plasma Expander Effectively Reduces Renal Uptake of 111In-Octreotide in Mice and Rats
- Renal Uptake of Radiolabeled Octreotide in Human Subjects Is Efficiently Inhibited by Succinylated Gelatin
- Oral Versus Intravenous Administration of Lysine: Equal Effectiveness in Reduction of Renal Uptake of [111In-DTPA]Octreotide
- Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues
- Patient-Specific Dosimetry in Predicting Renal Toxicity with 90Y-DOTATOC: Relevance of Kidney Volume and Dose Rate in Finding a Dose-Effect Relationship