


Abstract
The purpose of this study was to compare 18F-FDG PET to CT for evaluating the spleen during the initial staging of lymphoma. Methods: Seven patients with newly diagnosed lymphoma underwent 18F-FDG PET and CT. Splenic uptake of 18F-FDG, diffuse or focal, greater than hepatic uptake was interpreted as consistent with tumor. CT demonstrating a positive splenic index or focal hypodensities was classified as positive for tumor. PET and CT results were compared with final diagnoses, which were confirmed surgically for 6 patients and at autopsy for 1 patient. Results: Five of 7 patients had lymphomatous involvement of the spleen. 18F-FDG PET was true-positive for all 5 patients with splenic disease and true-negative for both patients without splenic disease. CT, in contrast, was true-positive for 4 of the 5 patients with splenic disease and false-positive for the 2 patients without splenic disease. The accuracies of 18F-FDG PET and CT for evaluating the spleen were 100% and 57%, respectively. Conclusion:18F-FDG PET correctly identified all patients with and without splenic disease and was superior to CT for this purpose.
Accurate staging of malignant lymphoma is essential, as it has an impact on clinical management and prognosis. CT evaluation of the spleen in patients undergoing initial staging of lymphoma has been the traditional mode of imaging but is associated with a high incidence of false-positive and false-negative results. Indeed, for patients who have lymphoma and in whom a change in therapy would be indicated if splenic disease were confirmed, surgical evaluation of the spleen may be required. Because of the morbidity and potential complications associated with surgery, it is important to identify a noninvasive technique that can accurately assess the spleen in patients undergoing initial staging of lymphoma.
18F-FDG PET is used to stage both Hodgkin’s disease and non-Hodgkin’s lymphoma. A recent report indicated that 18F-FDG PET accurately characterizes the spleen in Hodgkin’s disease and is superior to gallium imaging for this purpose (1). The results of splenic histologic analyses were available for a minority of patients, however. In the current series, we studied patients who had newly diagnosed malignant lymphoma and who had surgical confirmation of the presence or absence of splenic involvement by lymphoma. We compared the accuracies of 18F-FDG PET and CT for evaluating the spleen in this population.
MATERIALS AND METHODS
We reviewed the Department of Radiology database and the nuclear medicine patient charts at Long Island Jewish Medical Center from December 1998 to August 2002 to identify patients who had newly diagnosed lymphoma, who underwent pretreatment 18F-FDG PET and CT scans, and who subsequently had surgical confirmation of the presence or absence of splenic involvement.
For 18F-FDG PET, patients were injected with 150–220 MBq of 18F-FDG after a minimum 6-h fast. At approximately 1 h after injection, emission–transmission scanning was performed from the head to the pelvis by use of a dual-head, coincidence-detection-capable gamma camera or a Hybrid PET system (Solus MCD/AC; ADAC Laboratories) with measured attenuation correction (137Cs). For emission imaging, 64 angular samplings at an average of 40 s per sample were acquired on a 128 × 128 × 16 matrix. A 20% window centered on the 511-keV photopeak of 18F and a 30% window centered on the Compton centerline (usually about 310 keV) were used. For transmission imaging, 96 angular samplings at 2 s per sample were acquired on a 128 × 128 × 16 matrix. A 20% window centered on the 665-keV photopeak of 137Cs was used. Emission and transmission acquisitions were performed in an alternating sequence without moving the gantry. Data were reconstructed by use of an iterative method (ordered-subset expectation maximization). The system-reconstructed spatial resolution at full width at half maximum was 4.8 mm. Attenuation-corrected transaxial, coronal, sagittal, and 3-dimensional volume images were reviewed.
An experienced nuclear physician who had no knowledge of the CT results or final diagnoses interpreted the 18F-FDG PET scans according to previously described criteria; diffuse or focal splenic uptake of 18F-FDG more intense than hepatic uptake was interpreted as consistent with tumor (1). A semiquantitative approach also was applied. Using the transaxial image in which the intensity of 18F-FDG uptake was the highest, regions of interest were drawn over the spleen and the liver. The mean counts per pixel for each region were obtained, and a spleen-to-liver ratio (S/L ratio) was calculated.
Helical CT scans of the chest, abdomen, and pelvis were obtained after oral and intravenous administration of contrast material with 7-mm collimation. An experienced radiologist who had no knowledge of the 18F-FDG PET results or final diagnoses retrospectively reviewed the CT scans. Studies were classified as positive for splenic disease if discrete hypodensities within the spleen were identified or if the splenic index was increased. The splenic index was determined by multiplying the spleen thickness, width, and length, as visualized on CT (2). For adults, the spleen was classified as positive for tumor if the splenic index exceeded 480 mL (2,3). For children (patients ≤ 18 y), the spleen was classified as positive for tumor if the splenic index exceeded 500 + (20 × age [in years]) mL (4).
The 18F-FDG PET and CT results were compared with the final diagnoses, which were confirmed surgically for 6 patients and at autopsy for 1 patient.
RESULTS
The results are presented in Table 1. Seven patients (14–59 y old) with newly diagnosed lymphoma (4 Hodgkin’s disease, all nodular sclerosing, and 3 non-Hodgkin’s lymphoma, all large cell) were included. All 7 patients had extrasplenic sites of biopsy-proven, 18F-FDG-avid malignant lymphoma.
Patient Characteristics and CT and 18F-FDG PET Results
Five patients (patients 2 and 4–7) had a final diagnosis of lymphoma with splenic involvement. The methods of diagnosis were splenectomy for 3 patients (patients 4–6), diagnostic laparoscopy with visual inspection of the spleen for 1 patient (patient 2), and autopsy for 1 patient (patient 7). For the remaining 2 patients (patients 1 and 3), the spleen was free of tumor. The method of diagnosis for these 2 patients was splenectomy.
18F-FDG PET was true-positive for all 5 patients with splenic disease (patients 2 and 4–7) and true-negative for both patients without splenic disease (patients 1 and 3). Both visually and semiquantitatively, splenic uptake of 18F-FDG was greater than hepatic uptake in patients with splenic disease but not in patients without splenic disease. The semiquantitative method yielded S/L ratios of 1.4–5.2 for patients with splenic disease. The S/L ratio was 0.8 for both patients without splenic disease.
CT was true-positive for 4 of 5 patients with splenic disease (patients 4–7). Two had positive splenic indices of 1,612 and 1,474 mL and focal hypodensities (patients 4 and 6, respectively), and 2 had positive splenic indices of 958 and 932 mL and no focal abnormalities (patients 5 and 7, respectively). CT was false-negative for 1 patient (patient 2) with splenic disease, a 16-y-old female patient with a normal splenic index of 780 mL (normal for this age was up to 820 mL) and a homogeneous parenchyma. CT was false-positive for both patients without splenic disease but with splenic indices of 1,458 and 910 mL (patients 1 and 3, respectively); there were no focal abnormalities in these patients.
The accuracies of 18F-FDG PET and CT for identifying the presence or absence of splenic disease were 100% and 57%, respectively (Figs. 1–3).

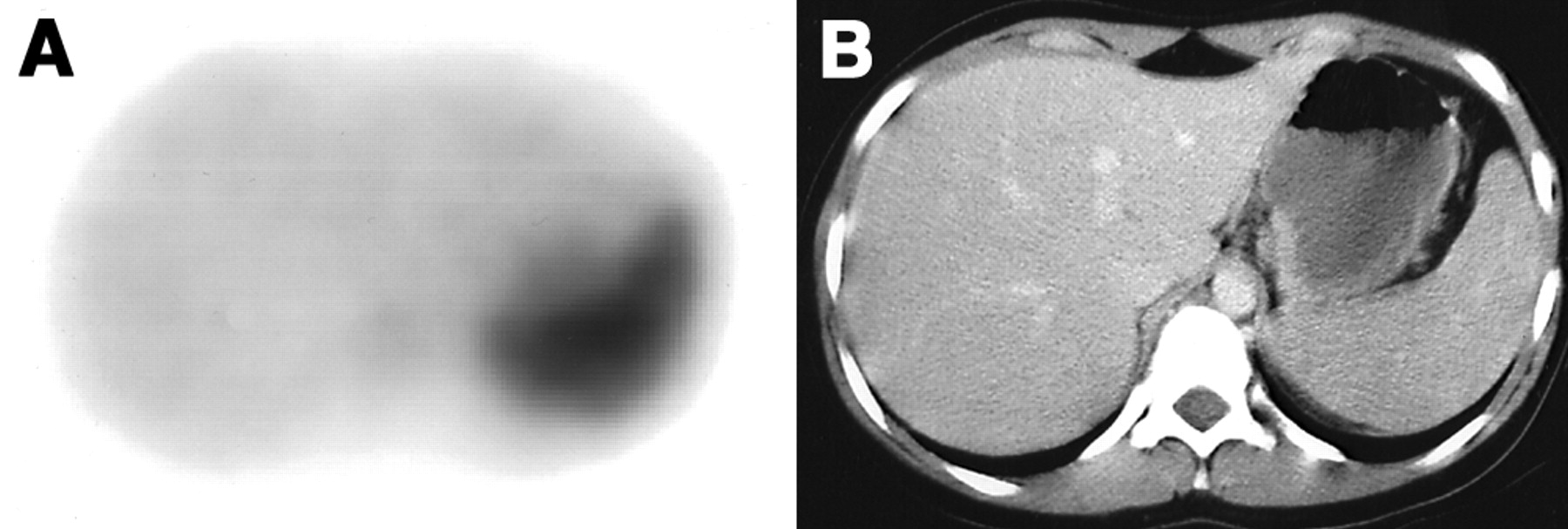
Stage IV non-Hodgkin’s lymphoma with splenic involvement in 77-y-old man (patient 4). (A) 18F-FDG PET image shows diffusely increased splenic uptake of 18F-FDG that is greater than hepatic uptake. S/L ratio was 1.9. (B) CT image shows multiple splenic hypodensities. Splenic index was 1,612 mL.
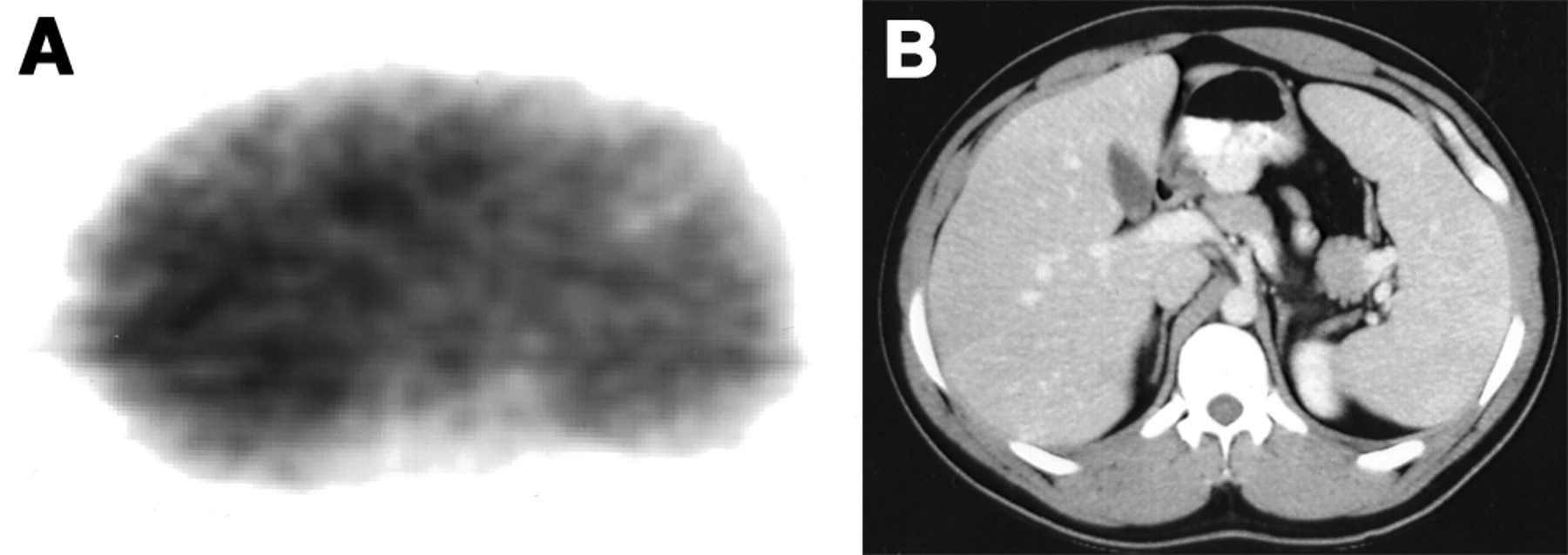
Stage IVB nodular sclerosing Hodgkin’s disease and splenic involvement in 16-y-old female patient (patient 2). (A) 18F-FDG PET image shows diffusely increased splenic uptake of 18F-FDG that is more intense than hepatic uptake. S/L ratio was 2.2. (B) CT image shows homogeneous appearance of spleen. Splenic index of 780 mL was normal for age (normal = ≤820 mL).
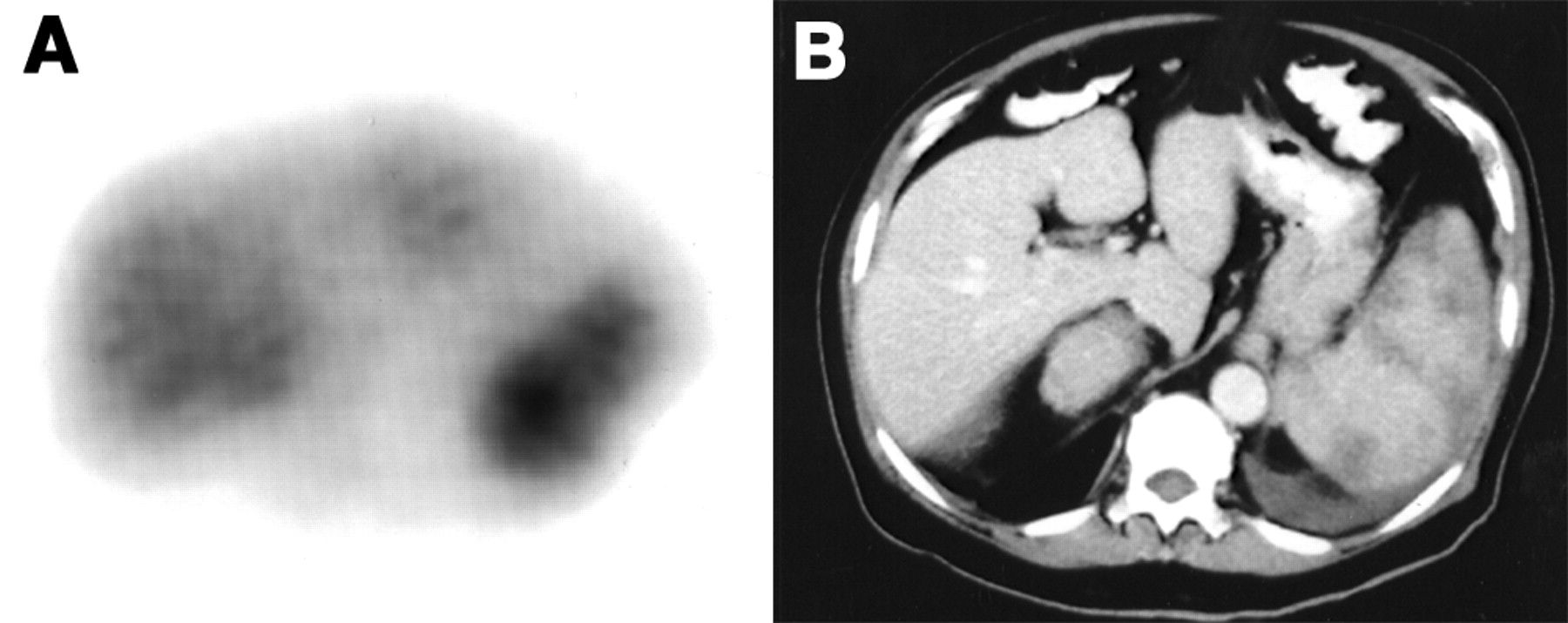
Stage II nodular sclerosing Hodgkin’s disease in 20-y-old male patient (patient 1). (A) 18F-FDG PET image shows that intensity of 18F-FDG uptake in spleen was similar to that in liver. S/L ratio was 0.8. (B) CT image shows homogeneous appearance of spleen. However, splenic index of 1,458 mL (normal = ≤480 mL) was elevated.
DISCUSSION
Splenic involvement by lymphoma is characterized by one or more tumor nodules, often less than 1 cm in diameter. Although marked splenomegaly is almost always indicative of tumor, lymphomatous spleens frequently are normal in size, and modestly enlarged spleens often contain no evidence of tumor (5).
Detecting lymphomatous involvement of the spleen with CT depends on identifying morphologic changes, including enlargement or discrete tumor nodules. Splenomegaly, unless massive, is a nonspecific finding, and focal hypodensities, although specific, are rarely seen. Reported accuracies of CT for identifying splenic involvement by Hodgkin’s disease range from 37% to 91% (3,6). Munker et al. (6) used the criterion of splenic enlargement (e.g., exceeding 11 × 7 × 4 cm) or splenic hypodensities on CT as indicative of tumor involvement and found that CT had an accuracy of 37%. Strijk et al. (3) used the criterion of a splenic index exceeding 480 mL as indicative of splenic involvement by Hodgkin’s disease and found that CT detected splenic involvement with an accuracy of 91%. These investigators concluded that the detection of splenic involvement by Hodgkin’s disease is improved when a more exact definition of splenic size is used, that is, the splenic index. In a study of the Pediatric Oncology Group’s experience with laparotomy for patients with Hodgkin’s disease, although the splenic index correlated with the probability of splenic involvement, the false-positive and false-negative rates of predictive models based on the splenic index alone were approximately 25% and 20%, respectively (4).
Detecting lymphomatous involvement of the spleen with 18F-FDG PET as opposed to CT depends on identifying increased glucose metabolism by tumor cells. Metabolic changes are evident when there is diffuse or focal tumor infiltration, regardless of whether frank morphologic changes are present. This comparative study illustrates the importance of metabolic imaging: 18F-FDG PET correctly identified or excluded splenic involvement in all 7 patients studied and was superior to CT, which was correct for only 4 of 7 patients.
CONCLUSION
With the development of increasingly sophisticated noninvasive diagnostic techniques, the need for surgical staging of lymphoma has steadily decreased over the years. Currently, surgery is reserved for patients for whom clinical assessment is inconclusive and for whom therapy would be altered if disease were found. The results of 18F-FDG PET in this small series, if validated with a larger population, suggest that it may be possible to further reduce the need for staging laparotomy in patients with lymphoma.
Acknowledgments
The authors gratefully acknowledge the assistance of Gungor Karayalcin, MD, and Diane Hart, NP, of the Division of Pediatric Hematology and Oncology, Schneider’s Children Hospital, Long Island Jewish Medical Center, and Mark A. Hoffman, MD, Bhoomi Mehrotra, MD, and Dilip Patel, MD, of the Division of Hematology and Oncology, Long Island Jewish Medical Center.
Footnotes
Received Dec. 12, 2002; revision accepted Mar. 24, 2003.
For correspondence or reprints contact: Christopher J. Palestro, MD, Division of Nuclear Medicine, Long Island Jewish Medical Center, 270-05 76th Ave., New Hyde Park, NY 11040.
E-mail: Palestro{at}LIJ.edu




{kind=link}
{kind=link}
{kind=link}