


Abstract
Our objective was to assess the role of 18F-FDG PET/CT in the evaluation of solid splenic masses in patients with a known malignancy and in incidentally found lesions in patients without known malignancy. Methods: Two groups of patients were assessed: (a) 68 patients with known malignancy and a focal lesion on PET or a solid mass on CT portions of the PET/CT study; and (b) 20 patients with solid splenic masses on conventional imaging without known malignancy. The standard of reference was histology (n = 16) or imaging and clinical follow-up (n = 72). The lesion size, the presence of a single versus multiple splenic lesions, and the intensity of 18F-FDG uptake expressed as a standardized uptake value (SUV) were recorded. The ratio of the SUV in the splenic lesion to the background normal splenic uptake was also calculated. These parameters were compared between benign and malignant lesions within each of the 2 groups of patients and between the 2 groups. Results: The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of 18F-FDG PET/CT in differentiating benign from malignant solid splenic lesions in patients with and without malignant disease were 100%, 100%, 100%, and 100% versus 100%, 83%, 80%, and 100%, respectively. In patients with known malignant disease, an SUV threshold of 2.3 correctly differentiated benign from malignant lesions with the sensitivity, specificity, PPV, and NPV of 100%, 100%, 100%, and 100%, respectively. In patients without known malignant disease, false-positive results were due to granulomatous diseases (n = 2). Conclusion: 18F-FDG PET can reliably discriminate between benign and malignant solid splenic masses in patients with known 18F-FDG–avid malignancy. It also appears to have a high NPV in patients with solid splenic masses, without known malignant disease. 18F-FDG–avid splenic masses in patients without a known malignancy should be further evaluated as, in our series, 80% of them were malignant.
Although not as common as focal hepatic masses, solid splenic masses are encountered in routine clinical practice and pose a diagnostic dilemma. Lesions may be discovered incidentally on imaging studies performed for unrelated causes. Malignant solid splenic lesions include lymphoma, leukemic infiltrates, metastases, and, rarely, angiosarcoma (1–5). The most frequently encountered benign solid splenic lesions are hemangiomas, hamartomas, and granulomas (6–8). Rarely, littoral cell angioma, inflammatory pseudotumor, or Gaucher nodules may be seen (9–11).
Almost all imaging modalities have been assessed regarding the identification and characterization of splenic lesions; however, conventional imaging modalities often cannot reliably differentiate benign from malignant lesions (12,13). 18F-FDG PET is a powerful tool for oncology imaging and is becoming widely available. This functional imaging modality is based on identification of hypermetabolic foci and has been shown to be accurate in staging of lymphoma, lung cancer, melanoma, and gastrointestinal and gynecologic malignancies among other tumors (14–18).
Recently, PET/CT systems, which enable the performance of PET and CT data acquisition at the same setting without changing the patient’s positioning, have been introduced in clinical practice (19). Lesions are characterized on the fused PET/CT images by both their metabolic status and their anatomic detail, enabling precise correlation of metabolic activity within a structural abnormality.
The purpose of this study was to assess the role of 18F-FDG PET/CT in the evaluation of splenic masses in patients with a known malignancy and in incidentally found lesions in patients without a known malignancy. The rationale behind using this imaging modality for characterization of splenic lesions was that malignant diseases most commonly involving the spleen are principally 18F-FDG–avid diseases, including lymphoma and metastases from malignant melanoma, lung cancer, ovarian cancer, and gastrointestinal malignancies. In contrast, the common benign splenic lesions—that is, hemangiomas and hamartomas—are not expected to show increased 18F-FDG uptake.
MATERIALS AND METHODS
Study Population
The study population included 2 groups of patients. Group A consisted of patients with a known malignancy who had splenic lesions on either the PET or CT portions of the study (a focal increased 18F-FDG uptake or a solid mass, respectively) (Table 1). Pure cystic lesions and small calcified lesions (the latter presumably representing calcified granulomas) were not included in this study. A retrospective review of our oncology PET/CT scan database for studies performed over an 18-mo period yielded 68 patients (38 men, 30 women; median age, 58.5 y; range, 21–84 y) with known malignant diseases and solid splenic lesions. These patients were sent for staging of a primary malignancy (n = 58) or restaging after therapy (n = 9). All patients sent for restaging were at least 4 mo after last anticancer systemic therapy. Group B consisted of 20 patients without known malignant disease (13 men, 7 women; median age, 56.5 y; range, 18–89 y) who were sent for 18F-FDG PET/CT because of a splenic mass on conventional imaging modalities. Data of this group of patients are summarized in Table 2. Our institutional review board does not require their approval and informed consent for review of a patient’s records, files, and images.
Primary Malignancies in Oncologic Patients (Group A) in Whom Splenic Lesions Were Suggested on PET/CT
Clinical Data, 18F-FDG Avidity, and Final Diagnosis of Splenic Lesions in Patients Without Known Malignancy (Group B)
Standard of Reference
For group A, a final diagnosis of the splenic lesions was made by splenic biopsy (n = 6) or clinical and imaging follow-up (n = 62). In group A, an 18F-FDG–avid lesion was considered true-positive for malignant involvement if proven by biopsy or if resolved after therapy or progressed on follow-up PET/CT or other imaging. An 18F-FDG–negative CT lesion was considered true-negative if it showed stability in size on conventional imaging follow-up or remained negative on repeated PET/CT.
Histology or clinical and imaging follow-up determined the final diagnosis of splenic lesions also in the 20 patients who did not have known malignant disease (group B). For 18F-FDG–avid splenic masses, the final diagnosis was achieved by splenectomy (n = 4), splenic biopsy (n = 4), or biopsy of a more accessible FDG–avid lesion found on the whole-body PET/CT scan (lymph node, n = 1; lung, n = 1). It is not practical to histologically confirm all 18F-FDG–avid lesions. Diagnoses obtained from sites other than the spleen are based on the fact that in routine clinical practice it is assumed that all pathologic sites of uptake are related to a single pathology. Patients with masses that did not show increased uptake of 18F-FDG had clinical and imaging follow-up (CT, n = 8; ultrasound, n = 2) (mean, 11 mo; range, 6–17 mo) with stability in the size of the splenic lesion and were free of malignant disease for the follow-up time period.
PET/CT
Patients were asked to fast for at least 4 h before undergoing the examination. All patients had glucose levels below 150 mg%. The patients received an intravenous injection of 370–666 MBq (10–18 mCi) 18F-FDG. Data acquisitions were performed within 60–120 min after injection using an integrated in-line PET/CT system (Discovery LS; General Electric Medical Systems). Iodinated oral contrast material was given to opacify loops of bowel on CT.
Data acquisition was as follows: CT was performed first, from the head to the pelvic floor with 140 kV, 80 mA, tube rotation time of 0.5 s, pitch of 6, and 5-mm section thickness, which was matched to PET section thickness. The CT part of the study was performed using a shallow breathing technique. Immediately after CT, a PET emission scan was obtained that covered the identical transverse field of view. The acquisition time was 5 min per each table position. PET image datasets were reconstructed iteratively by using CT data for attenuation correction, and coregistered images were displayed on a workstation (Xeleris; Elgems).
Data Analysis and Statistics
Studies of all patients in both study groups were retrieved and read in consensus by a panel of 2 experts. The panel recorded the largest diameter of the splenic masses, presence of a single mass versus multiple lesions within the spleen, and avidity of the splenic mass to 18F-FDG, visually and by obtaining standardized uptake value (SUV Lesion [SUV L]) measurements. On visual inspection, a lesion was considered as showing pathologically increased uptake if its uptake was higher than the physiologic uptake of the surrounding splenic parenchyma. A region of interest was drawn with a diameter of two thirds of the diameter of the lesion to minimize partial-volume effects. In cases in which a splenic lesion was identified on CT without increased 18F-FDG uptake, the SUV was measured based on the location of the lesion on coregistered images. The outline of the spleen was examined on coregistered images to confirm adequate image registration. In studies with >1 splenic mass, the largest and smallest lesions were analyzed. The SUV of the normal spleen was also measured with a similar-sized region of interest, at a location distant from the focal splenic lesion (SUV Background [SUV B]). To eliminate the possible effect of variability in the normal splenic 18F-FDG uptake of 18F-FDG among different individuals, the ratio between SUV L and SUV B was calculated. In addition, additional pathologic 18F-FDG–avid foci on the whole-body 18F-FDG PET/CT study were noted.
The SAS system for Windows, version 8.01, was used for statistical analysis. Comparison of SUVs in malignant and benign lesions (SUV L), SUVs of normal background splenic uptake of 18F-FDG (SUV B), and ratios of SUV L to SUV B was performed for patients with benign and malignant splenic lesions within each of the 2 groups of patients and between the 2 groups. The Student t test was used and P < 0.05 was considered statistically significant. Receiver operating characteristic (ROC) curve analysis determined the most suitable SUV threshold and the SUV L–to–SUV B ratio to differentiate benign and malignant splenic lesions in both groups of patients. For patients with >1 splenic lesion, the correlation coefficient was calculated for the correlation between lesion size and SUV measurements.
RESULTS
Table 3 summarizes the results for the 2 groups of patients according to the number of splenic lesions identified. The multiplicity of lesions in the spleen (regardless of 18F-FDG uptake) had a positive predictive value (PPV) of 81.5%. However, solitary splenic lesions (regardless of 18F-FDG uptake) were malignant in 81.7% of cases.
Distribution of Splenic Lesions Based on Number of Lesions in Spleen and Type of Lesion in Both Groups of Patients
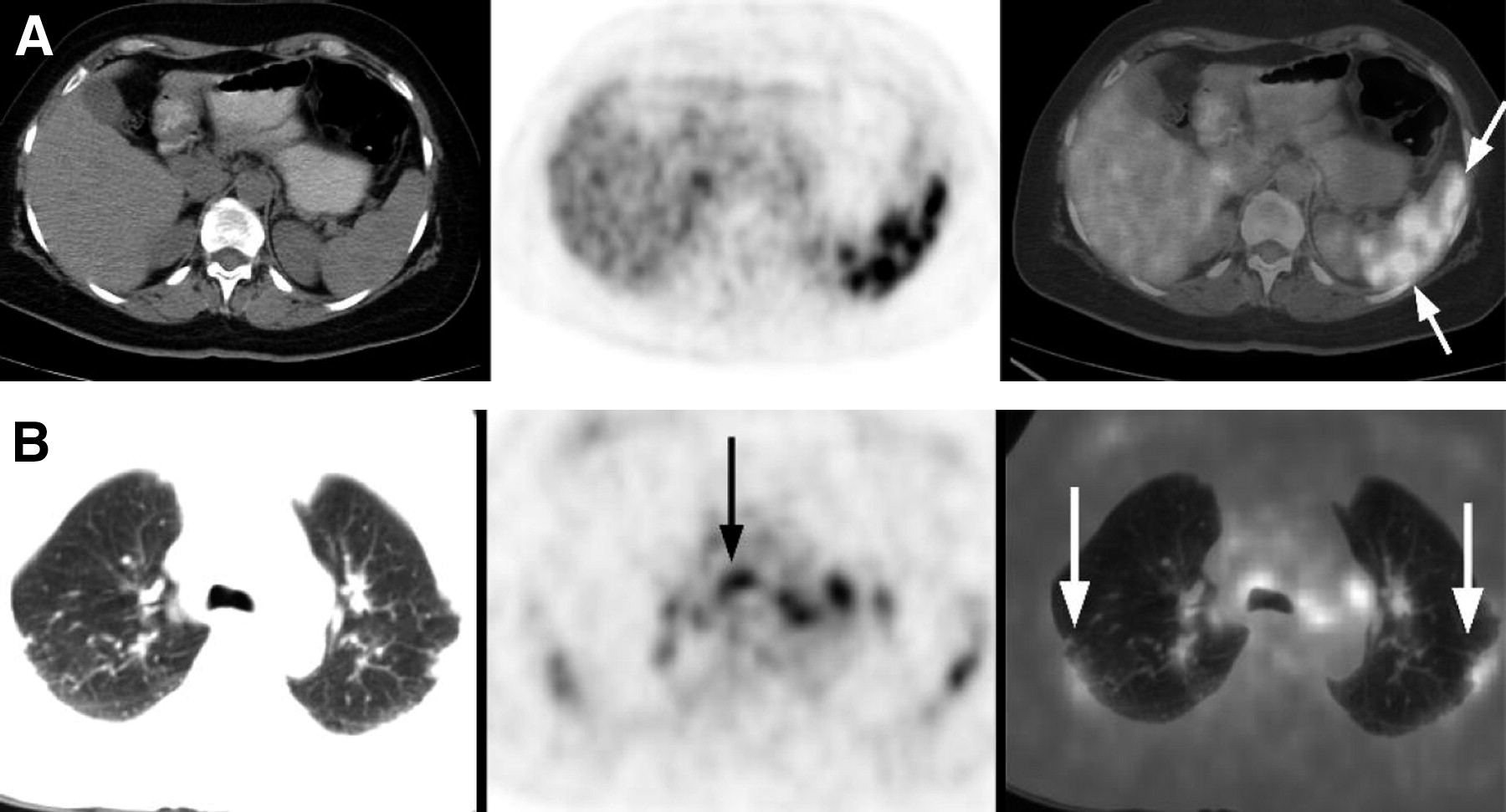
Twenty-seven patients in group A had nonlymphomatous malignancy and malignant splenic involvement. In 23 of them (23/27, 85.2%), the splenic metastases were in addition to widespread metastatic disease (Fig. 1); 1 patient with melanoma had metastatic disease limited to the spleen, and 3 patients (melanoma, n = 1; ovarian cancer, n = 1; squamous cell carcinoma of the anus, n = 1) had only 1 metastasis in addition to the spleen. This additional tumor site was located in a lymph node or the peritoneum). The mean size of malignant splenic lesions was 1.7 cm (range, 0.5–15.6 cm).

Solitary splenic metastasis in presence of disseminated metastatic disease: 62-y-old man with lung cancer. (A) Axial PET/CT images show 18F-FDG–avid metastatic deposit in anterior aspect of spleen (arrow). Follow-up contrast-enhanced CT showed progression of splenic mass (not shown). (B) Maximum-intensity-projection PET image shows disseminated metastatic disease in bone, liver, lymph nodes, and spleen.
The mean SUV L of all benign lesions was 1.87 ± 0.32 (minimum value, 1.17; maximal value, 2.1; variation coefficient, 17.19; 95% confidence interval, 1.6–2.13). The mean SUV L of all malignant lesions was 7.86 ± 5.57 (minimum value, 2.42; maximal value, 29.6; variation coefficient, 70.85; 95% confidence interval, 6.59–9.12). Ratios of the mean SUV L of benign splenic lesions to the SUV B were 1.04 ± 0.21 (minimum value, 0.63; maximal value, 1.24; variation coefficient, 19.91; 95% confidence interval, 0.87–1.21). Ratios of the mean SUV L of malignant splenic lesions to the SUV B were 3.91 ± 2.78 (minimum value, 1.23; maximal value, 14.03; variation coefficient, 71.11; 95% confidence interval, 3.28–4.45). Differences in SUV L and in the SUV L–to–SUV B ratios between benign and malignant groups were statistically significant (P < 0.01 and P < 0.01, respectively). In the group of patients with splenic mass and known malignant disease, the sensitivity, specificity, PPV, and negative predictive value (NPV) of visual analysis of 18F-FDG PET/CT in differentiating benign from malignant solid splenic lesions were 100%, 100%, 100%, and 100%, respectively. Using ROC curve analysis, the best SUV threshold for 100% NPV, with the highest possible PPV, was 2.3 (with a sensitivity, specificity, accuracy, PPV, and NPV of 100%, 100%, 100%, 100%, and 100%, respectively) and the best ratio threshold was 1.2 (with a sensitivity, specificity, accuracy, PPV, and NPV of 100%, 75%, 98%, 97%, and 100%, respectively).
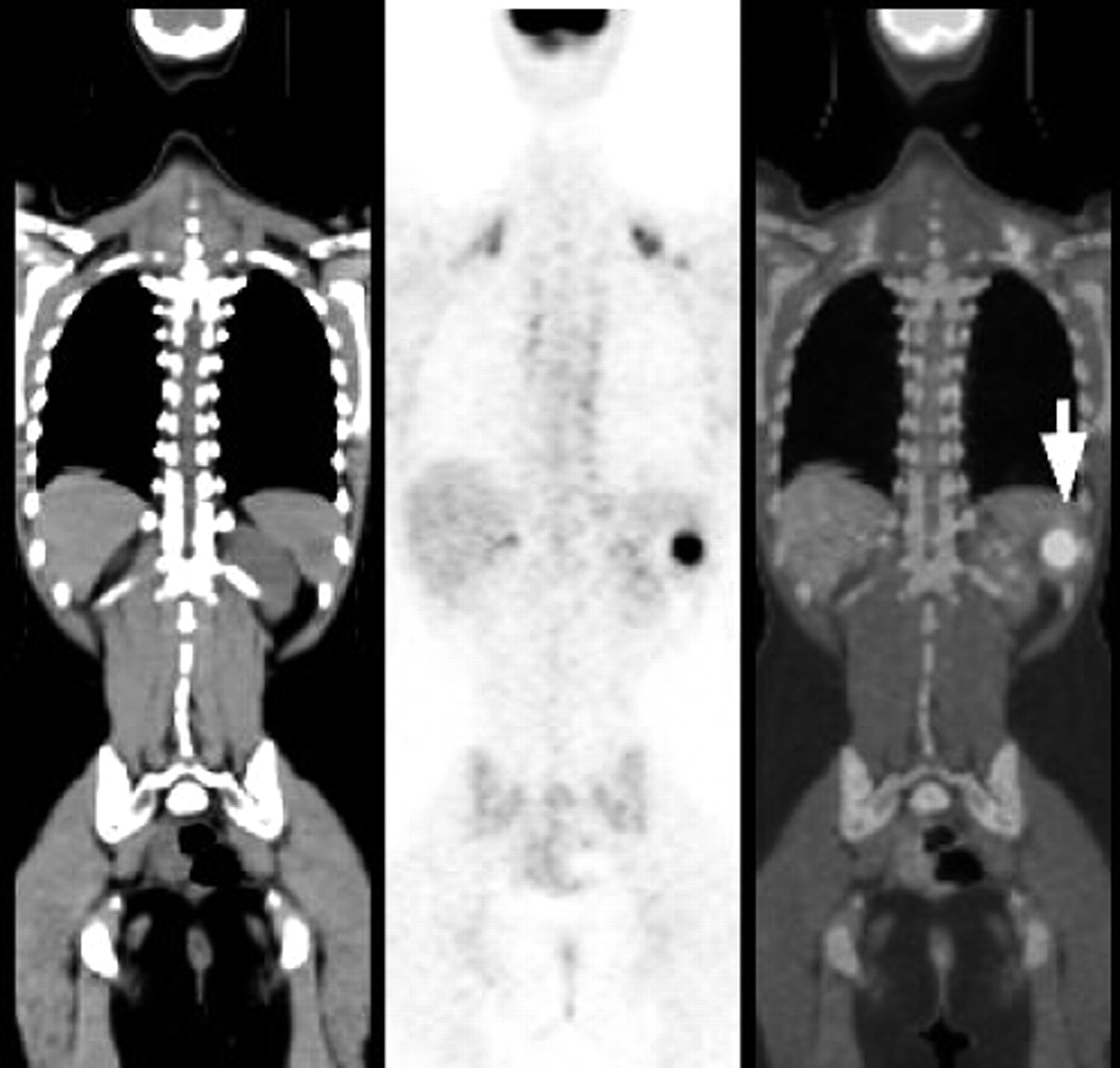
Of the 20 patients referred for evaluation of a splenic mass without a previously diagnosed malignancy, 10 patients (50%) had abnormal uptake of 18F-FDG in a splenic lesion. Of these 10 patients, 2 had inflammatory lesions (sarcoidosis, n = 1; brucellosis, n = 1) and 8 patients had malignant disease (lymphoma, n = 7; metastatic deposit from gastric cancer, n = 1). Five of the 7 (71.4%) patients with lymphoma had additional 18F-FDG–avid disease in lymph nodes, whereas 2 patients had lymphoma limited to the spleen, consistent with primary splenic lymphoma (Fig. 2). The mean size of splenic lesions was 2.05 cm (range, 0.5–12.5 cm). Of these 20 patients (with 29 splenic lesions analyzed), 9 (45%) had ≥2 lesions in the spleen. The mean SUV of all benign lesions was 2.29 ± 1.36 (minimum value, 0.63; maximal value, 6.30; variation coefficient, 59.30; 95% confidence interval, 1.62–2.96). The mean SUV of all malignant lesions was 9.11 ± 6.95 (minimum value, 2.3; maximal value, 26.6; variation coefficient, 76.25; 95% confidence interval, 4.74–13.49). In this group of patients, ratios of the mean SUV L to SUV B in benign splenic lesions were 1.49 ± 1.06 (minimum value, 0.34; maximal value, 4.5; variation coefficient, 70.68; 95% confidence interval, 0.53–1.58). Ratios of the mean SUV L to SUV B in malignant splenic lesions were 4.48 ± 3.02 (minimum value, 1.51; maximal value, 11.57; variation coefficient, 65.56; 95% confidence interval, 2.45–6.51). Differences in SUV L and in SUV L–to–SUV B ratios between benign and malignant groups were statistically significant (P < 0.005 and P < 0.005, respectively). In the group of patients without known malignant disease, the sensitivity, specificity, PPV, and NPV of visual analysis of 18F-FDG PET/CT in differentiating benign from malignant solid splenic lesions was 100%, 83%, 80%, and 100%, respectively. Using ROC curve analysis, the best SUV threshold for 100% NPV, with highest possible PPV, was 2.2 (with sensitivity, specificity, accuracy, PPV, and NPV of 100%, 71%, 83%, 71%, and 100%, respectively) and a ratio threshold of 1.5 (with sensitivity, specificity, accuracy, PPV, and NPV of 100%, 76%, 86%, 75%, and 100%, respectively).

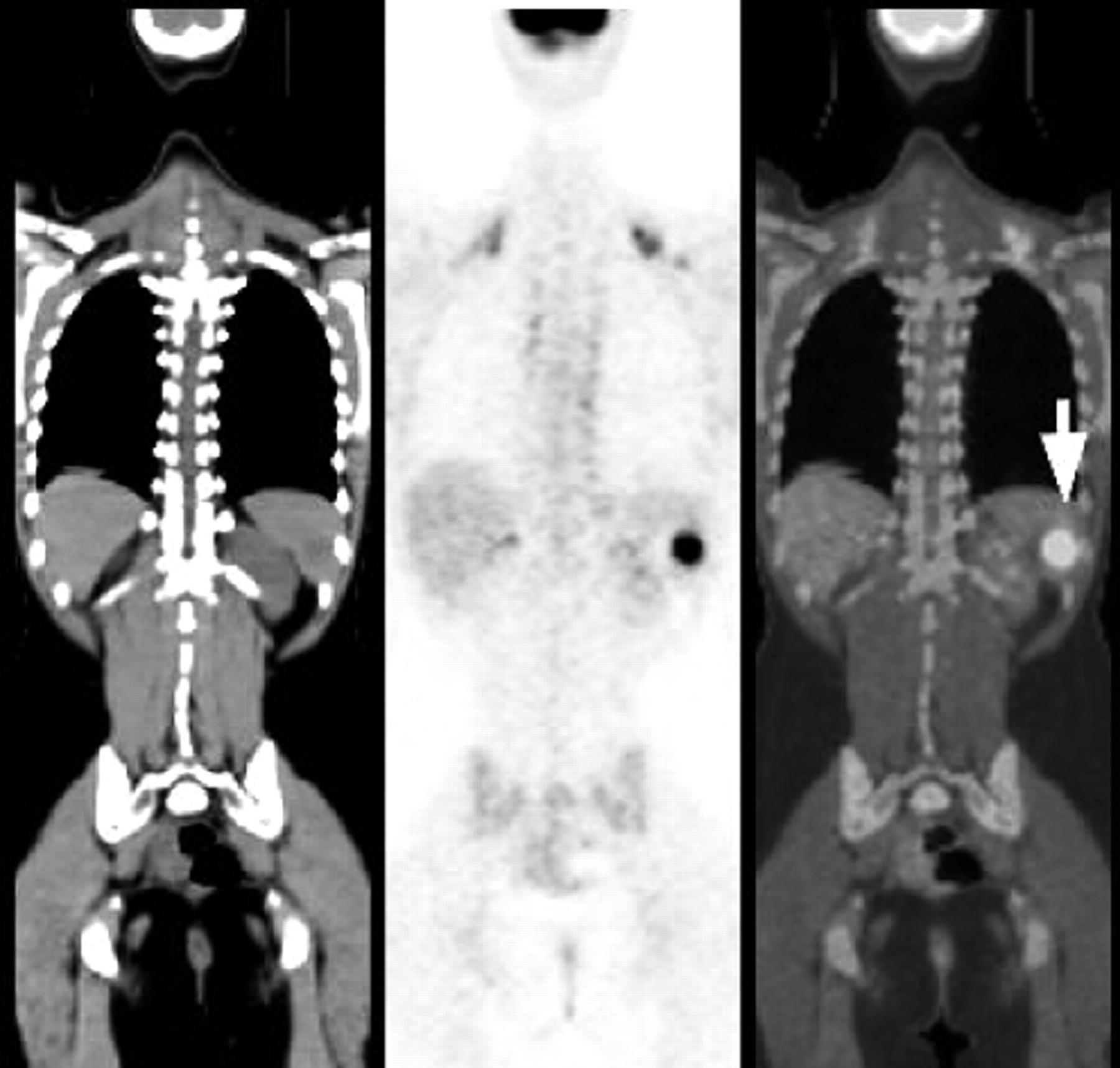
Primary splenic lymphoma: 66-y-old man without previously diagnosed malignancy. Coronal PET/CT images show multiple 18F-FDG–avid splenic masses, proven to be non-Hodgkin’s lymphoma on biopsy, in absence of other 18F-FDG–avid disease.
No statistically significant difference was noted between SUV B of patients with malignant lesions in both groups of patients (with and without known malignancy) or between SUV B of patients with malignant splenic lesions and benign splenic lesions in either group of patients (P = not significant for all).
Twenty-one patients had >1 splenic mass. Although all smaller lesions had lower SUVs in comparison with larger lesions in the same patients, only a weak correlation was found when comparing the SUV with the lesion size in the group as a whole (r = 0.65, P < 0.001).
DISCUSSION
Splenic metastases are encountered in 2.3%–12.9% of postmortem examinations in cancer patients (20). The most common primary sites of malignancy to metastasize to the spleen are lung, breast, ovary, and melanoma (20,21). Splenic metastases are a relatively uncommon clinical event, usually occurring in the setting of disseminated metastatic disease (20,22), as was also seen in this study. To our knowledge, only 22 case reports of solitary splenic metastases are reported to date in the English literature, with more than one third of them secondary to lung cancer and malignant melanoma (23).
Although the spleen is a frequent site of involvement in patients with non-Hodgkin’s lymphoma and may be involved in one third of patients with Hodgkin’s disease (24), primary malignant lymphoma of the spleen (PMLS) is uncommon. The definition of PMLS is controversial; however, it has been suggested that only cases with disease limited to the spleen and splenic hilum should be included in this entity (25). Although rare, PMLS is the most common primary malignancy of the spleen. Splenomegaly is not a reliable indicator of lymphomatous involvement of the spleen because the organ’s size is normal in one third of patients with splenic disease (26). On imaging, lymphomatous involvement of the spleen may manifest as either focal lesions or diffuse disease. Recent reports have shown that 18F-FDG PET is more accurate than CT and gallium scintigraphy for identifying splenic involvement by lymphoma (27,28).
Primary nonhematopoetic tumors of the spleen are extremely rare. Tumors may arise from the sinus epithelium (angiosarcoma and hemangioendotheliomas) or from connective tissue (spindle cell sarcoma and fibrosarcoma). Of these rare entities, angiosarcoma is the most common tumor to involve the spleen with <100 cases reported in the literature (29). Clinically, left upper quadrant abdominal pain, anemia, coagulopathy, and spontaneous rupture may be encountered. Hematogenous metastases at diagnosis are common and the overall prognosis is poor (30). Although there are no reports of 18F-FDG PET in the diagnosis of splenic angiosarcoma, angiosarcoma of the pleura and chest wall has been shown to be 18F-FDG avid (31).
As in the literature, the most common nonlymphomatous malignancies to metastasize to the spleen in our series were melanoma, lung, colon, and ovarian cancer. Although most patients with splenic metastases had disseminated metastatic disease, a few patients had disease limited to the spleen or the spleen and a solitary additional site, allowing a surgical approach to be considered as was the case in 2 of these patients in our series. In routine clinical practice, it is not possible to histologically confirm all sites of metastatic disease; therefore, we had to assume that an 18F-FDG–avid splenic lesion was a metastasis, based on positive histologic proof from another 18F-FDG–avid site and imaging follow-up of the splenic lesion.
Apart from accurate localization, one of the advantages of evaluation of lesions with PET/CT is the ability to evaluate non-18F-FDG–avid lesions, both visually and semiquantitatively, as accuracy of coregistration can be assessed. Known 18F-FDG–avid malignancies that had non-18F-FDG–avid splenic masses were all stable in size on follow-up of patients; although we do not have histologic diagnoses for most, these masses are presumed to be benign incidental masses. Splenic masses in patients with a known 18F-FDG–avid malignancy were accurately dichotomized by PET/CT assessment into benign or malignant. The sensitivity and specificity of visual PET reading for differentiating benign and malignant splenic lesions were 100% for patients with lymphoma or nonlymphomatous tumors. In this group of patients, using a SUV threshold of 2.3, all lesions would be correctly classified. However, it should be noted that there is a selection bias in this group of patients because it included patients that were sent for staging or restaging of primary malignancies that are considered 18F-FDG avid.
In the group of patients without a known malignancy, 18F-FDG PET had a high NPV. In fact, all lesions that did not show abnormal 18F-FDG uptake were stable on clinical and imaging follow-up and patients did not have evidence of malignancy during the follow-up time period (Fig. 3). Caution should be taken to avoid false-negative 18F-FDG PET results. Although no such cases were encountered in this study, it should be borne in mind that non-18F-FDG–avid tumors, such as some renal cell carcinomas or thyroid cancers, may metastasize to the spleen. In cases of non-18F-FDG–avid splenic lesions, the whole-body CT portion of the PET/CT studies should be thoroughly evaluated to assess for possible non-18F-FDG–avid malignancies. Using visual inspection and a SUV threshold of 2.2, false-positive 18F-FDG PET results were found in 2 patients. One of these patients had innumerable small foci of 18F-FDG uptake in the spleen as well as in subpleural lung densities and small mediastinal and hilar lymph nodes, a pattern suggestive of sarcoidosis (32), which was later verified on lung biopsy (Fig. 4). Because PET/CT studies combine both anatomic and functional imaging, patterns of disease on fused images may aid in suggesting a correct diagnosis. The second false-positive study was in a young woman with subcapsular 18F-FDG–avid masses shown on splenectomy to represent caseating granulomas due to Brucella melitensis (Fig. 5). Although absent in this patient, abscesses due to Brucella described in the literature often show central calcific densities within the hypodense masses on CT (33). Similarly, it may be assumed that other granulomatous diseases involving the spleen, such as tuberculosis and histoplasmosis, as well as noninfectious inflammatory diseases, such as inflammatory pseudotumor, may abnormally accumulate18F-FDG and imitate malignancy. A multiplicity of lesions, as expected, had a high PPV for malignancy (81.5%); however, granulomatous disease, which appears to be the most frequent etiology for false-positive 18F-FDG PET scans of the spleen, is not infrequently associated with multiple splenic lesions.

Presumably benign solid splenic mass: 62-y-old woman without previously diagnosed malignancy. Axial PET/CT images show no increased uptake of 18F-FDG within hypodense mass on CT (arrows). Mass was stable on sonography for >1 year.

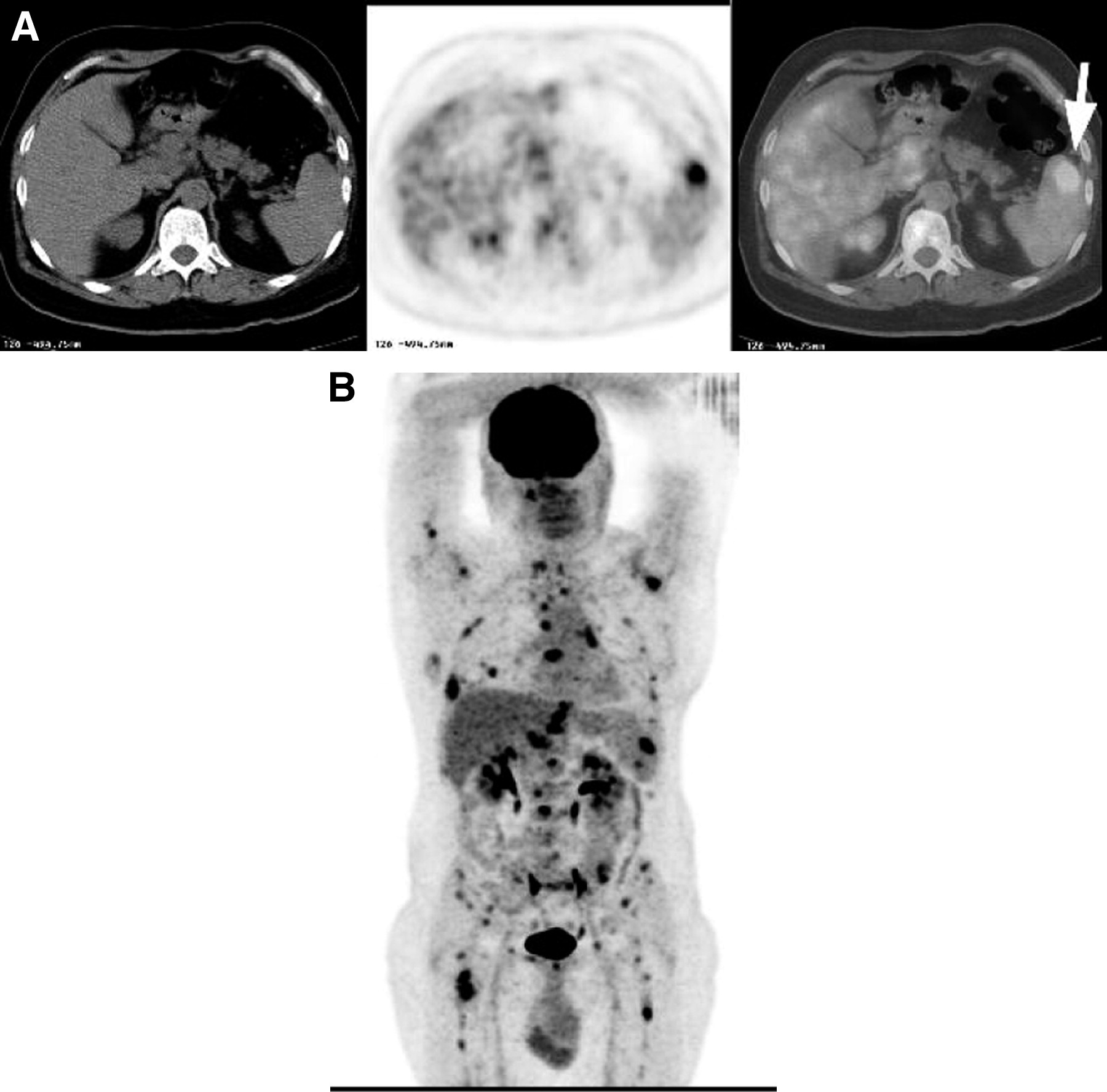
False-positive 18F-FDG PET/CT in sarcoidosis: 55-y-old woman without known malignancy. Multiple hypodense splenic nodules discovered on CT performed for abdominal pain. (A) Axial PET/CT images show innumerable 18F-FDG–avid nodules within spleen. (B) Axial PET/CT images (lung windows) show abnormal uptake of 18F-FDG in mediastinal lymph nodes (black arrow) as well as increased 18F-FDG uptake in subpleural lung densities (white arrows) proven to be sarcoidosis on lung biopsy.
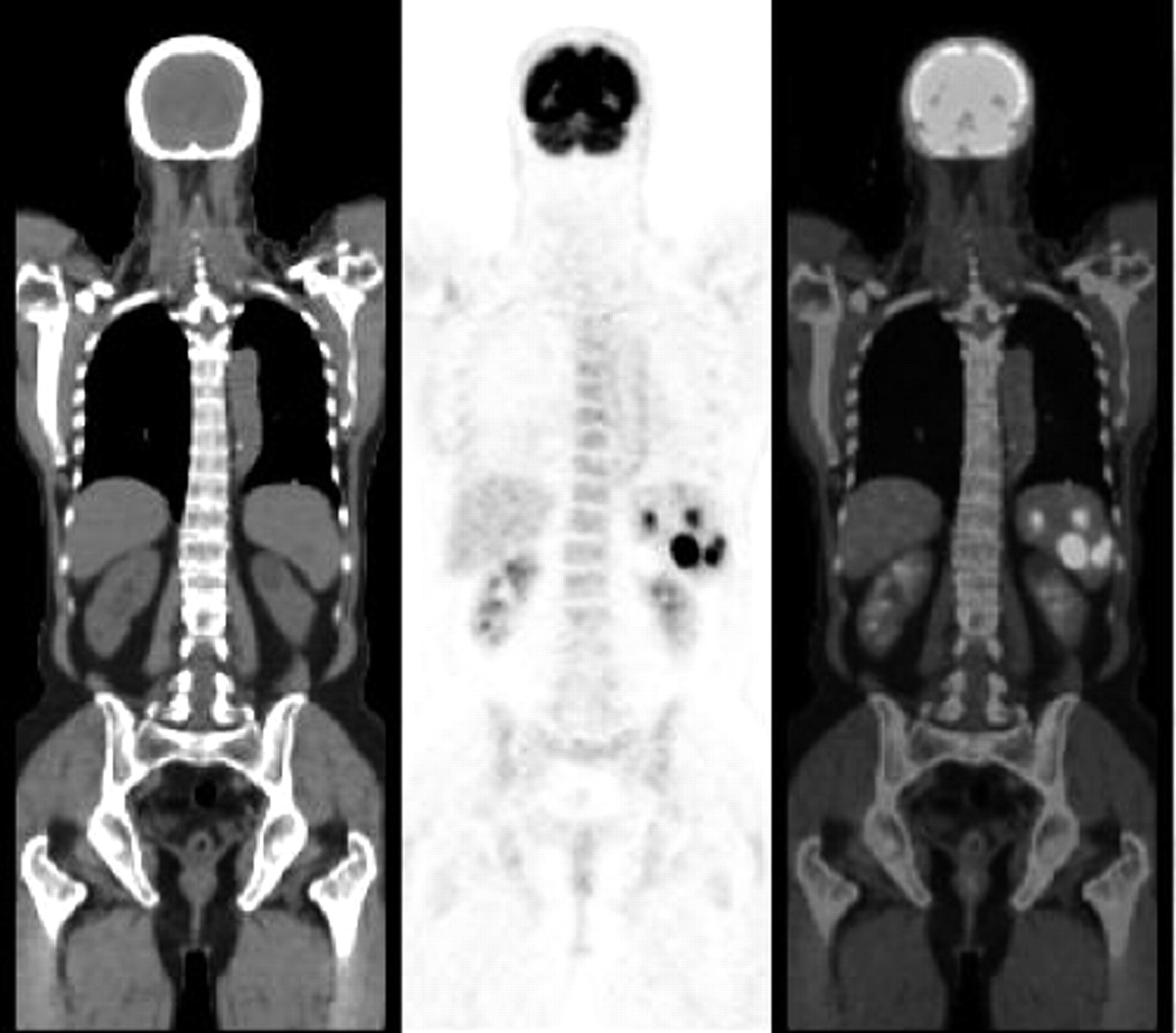
False-positive 18F-FDG PET/CT in splenic granulomas due to Brucella melitensis: 18-y-old woman with incidentally discovered solid splenic masses (arrow) on sonography performed because of epigastric pain. Coronal PET/CT images show abnormal uptake of 18F-FDG in splenic nodule, proven to be granuloma due to Brucella on splenectomy.
As previously shown for 18F-FDG PET of malignant lung nodules (34), smaller lesions in same patient had lower SUVs in comparison with larger lesions. A weak correlation between the SUV and the size of lesions in patients with >1 splenic mass as a group may be attributed to differences in uptake of 18F-FDG in the different primary tumors.
Because conventional imaging often cannot differentiate benign from malignant solid splenic masses, a new noninvasive imaging technique is needed. This study has shown that 18F-FDG PET/CT can be used to help discriminate benign from malignant splenic masses. 18F-FDG PET/CT can also identify additional unsuspected sites of disease, which may be more accessible for biopsy. This may obviate the need to biopsy the spleen itself, a procedure associated with a complication rate of 1.5%–13% (35,36). On the basis of this study’s results, a possible scheme for interpretation of a splenic lesion on PET/CT is presented in Figure 6. This algorithm is suggested only if the primary tumor is 18F-FDG avid.
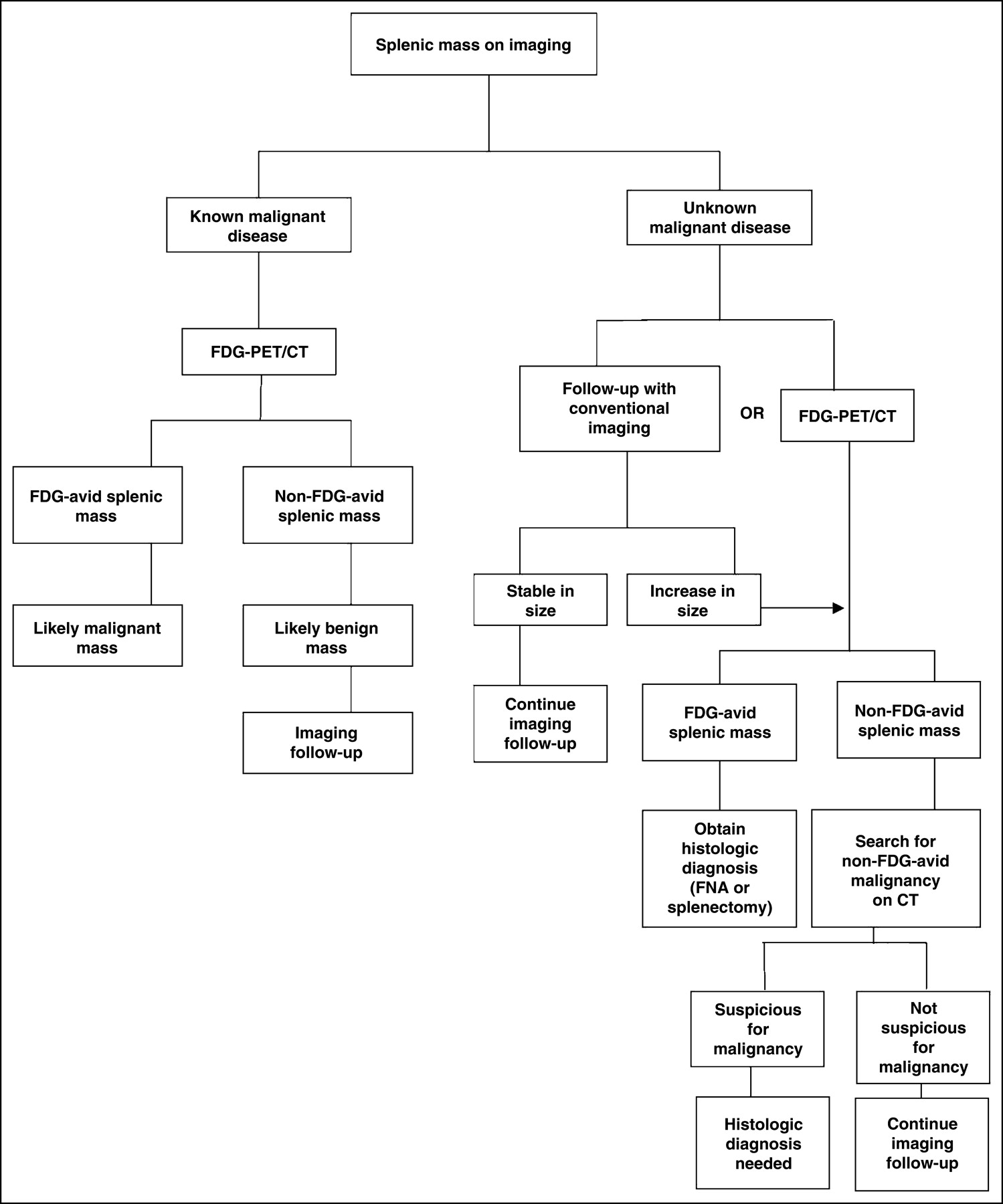
Suggested scheme for interpretation of a splenic lesion on PET/CT. FNA = fine-needle aspiration.
CONCLUSION
18F-FDG PET can reliably discriminate between benign and malignant solid splenic masses in patients with known 18F-FDG–avid malignancy. 18F-FDG PET also appears to have a high NPV in patients with solid splenic masses, without known malignant disease. 18F-FDG–avid splenic masses in patients without a known malignancy should be further evaluated—in our series, 80% of them were malignant.
Acknowledgments
The authors thank Israel Friedman for editorial assistance.
Footnotes
Received Apr. 19, 2004; revision accepted Jul. 27, 2004.
For correspondence or reprints contact: Ur Metser, MD, Department of Nuclear Medicine, Tel-Aviv Sourasky Medical Center, 6 Weizman St., Tel-Aviv, 64239 Israel.
E-mail: umetser{at}tasmc.health.gov.il





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}