


Article Figures & Data
Figures
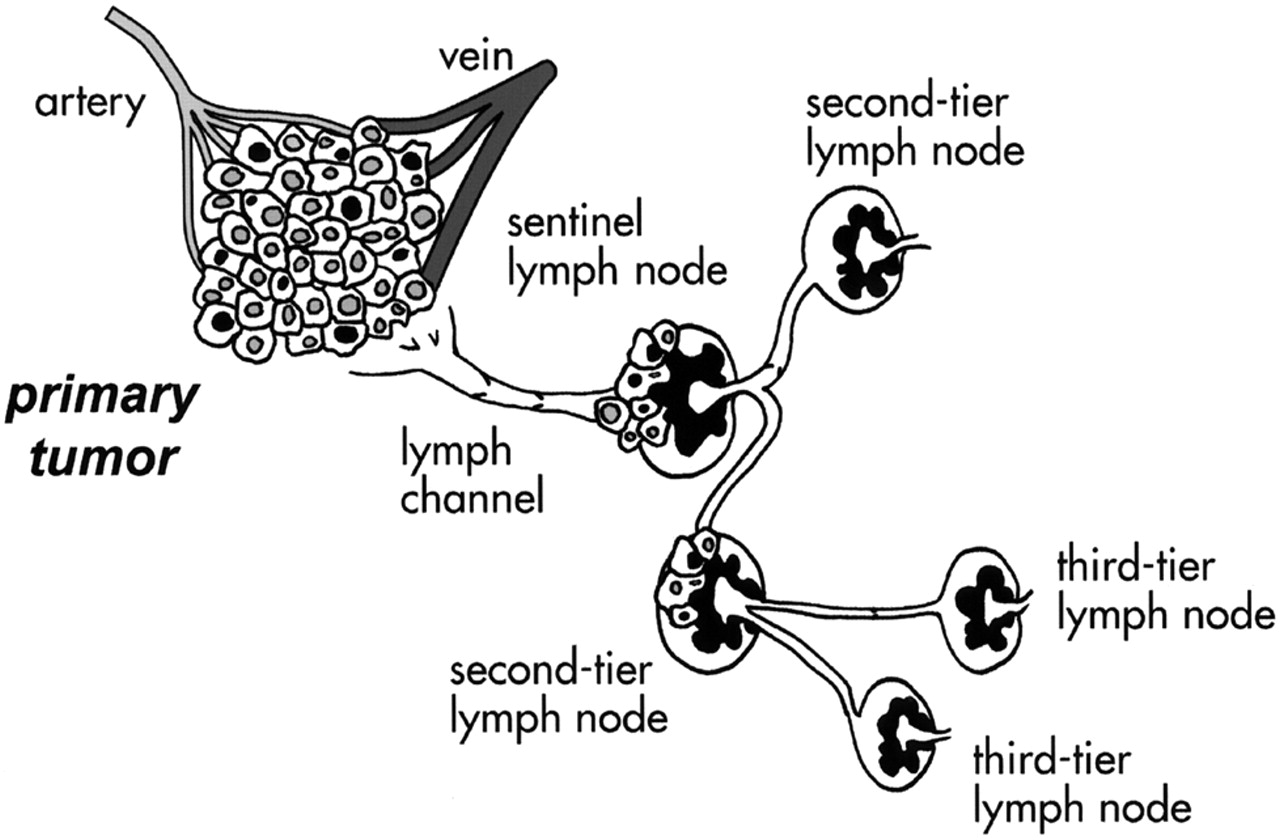
- FIGURE 1.
Schematic conceptualization of sentinel lymph node. Being first node encountered by lymph draining from primary tumor, sentinel lymph node should be site where clusters of tumor cells migrating through lymphatic channels are most likely to be entrapped and possibly proliferate before widespread tumor dissemination in body. Second-tier (or second-echelon) lymph nodes receive lymph (and possibly tumor cells) from sentinel lymph node and in turn drain lymph toward third-tier lymph nodes.
- FIGURE 2.
(A) Schematic representation of structure of cutaneous blood and lymph vessels. For simplicity, blood and lymph vessel networks (which are intimately embedded in each other) are represented separately on left (red and blue) and on right (yellow). Embryologic origin in ectoderm places mammary gland in ideal space between subcutaneous plexus and deep lymphatic collectors (emphasized in figure). Each branch of periductal plexus drains lymph mostly toward skin surface (through subareolar plexus), whereas minor component drains toward deep collectors (draining in turn toward internal mammary chain). Radiocolloids injected intradermally over mammary gland drain to subcutaneous plexus, which is also terminal pathway of predominant lymph drainage from mammary gland. (B) Schematic representation of pathways of lymphatic drainage from mammary gland (modified from (150)). Most lymph produced in mammary gland surfaces at subareolar plexus, then merges with subcutaneous plexus of overlying skin, and flows with centrifugal pattern mostly toward axilla. Lymph from deeper portion of gland drains either through same pathway or through deep lymphatics to reach parasternal, internal mammary chain (and even contralateral side). abdom. = abdominal.
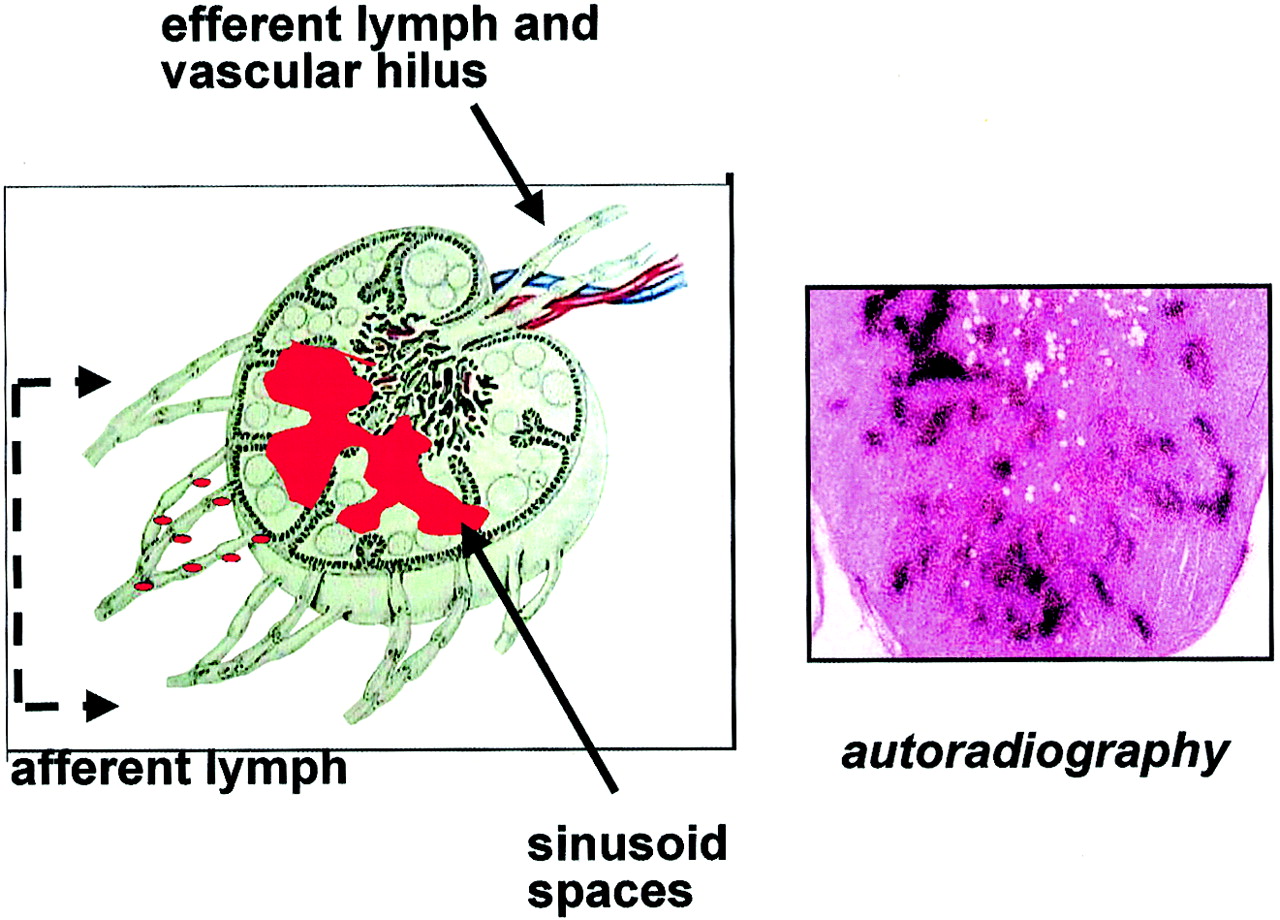
- FIGURE 3.
(Left) Red dots symbolize radiocolloids migrating with afferent lymph from site of interstitial injection to lymph node, where they are entrapped by macrophages lining sinusoid spaces (red area). (Right) Low-magnification histoautoradiograph of sentinel node removed about 20 h after injection of 99mTc-HSA nanocolloid. Black dots (silver grains) show retention of radioactive agent in sinusoid spaces. (Hematoxylin–eosin, about ×8)
- FIGURE 4.
(A) Time–radioactivity curves from region-of-interest (ROI) analysis after dynamic recording of lymphoscintigraphy performed by intradermal injection of 6 MBq (150 μCi) 99mTc-HSA nanocolloid; y-scale is arbitrary to plot all 3 curves within same order of magnitude. Injection site shows minimal reduction over 60 min, barely discernible from physical decay. Tracer appears in sentinel node starting few minutes after injection, with quasiplateau maintained over 60 min. Lymphatic channel shows early passage of radioactivity, continuing with quasipulsatile pattern. Direct supply of radiocolloid draining from injection site (continuing over several hours) keeps radioactivity content of sentinel node at relatively higher level than that of second- or third-tier nodes, even if active retention of tracer by macrophages is saturated. (B) Definition of 3 ROIs on representative frame set from dynamic recording: ROI 1 = injection site; ROI 2 = lymphatic channel; ROI 3 = sentinel node.
- FIGURE 5.
Scintigraphs obtained in right anterior oblique view 15 min after subdermal injection of radiocolloids with different particle size: 99mTc-sulfide (left), 99mTc-HSA nanocolloid (center), and special formulation of 99mTc-HSA microcolloid, not available commercially (151) (right). Even on early imaging, radiocolloids with small and intermediate particle size visualize several nodes in addition to sentinel node, whereas only sentinel node is visualized by radiocolloid with relatively large particles.
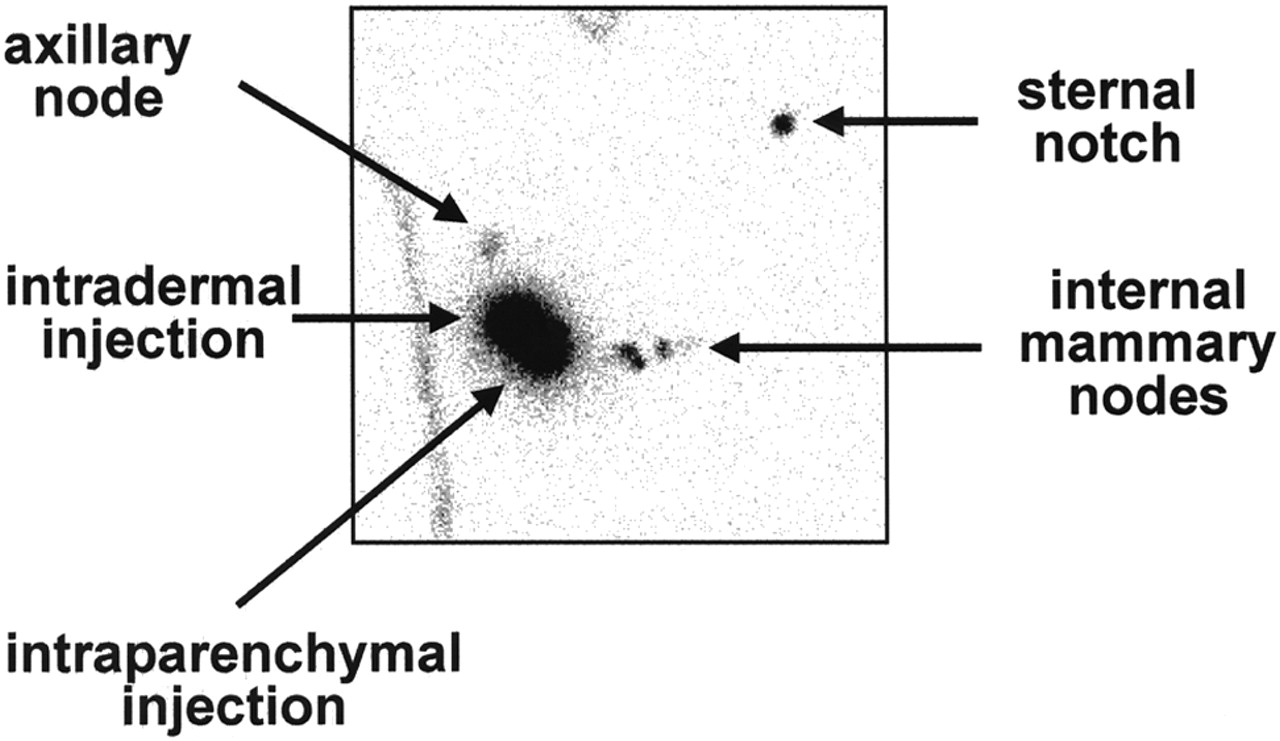
- FIGURE 6.
Scintigraph obtained in anterior view about 45–60 min after injecting 2 separate aliquots of 99mTc-HSA nanocolloid (about 7 MBq [200 μCi] each) intradermally and, 15 min later, intraparenchymally in right breast; contour of body in area under evaluation is identified with aid of radioactive point source. Intradermal injection ensures visualization of single sentinel lymph node between breast and axilla, whereas intraparenchymal injection visualizes lymphatic drainage toward internal mammary chain (at least 3 sequential lymph nodes).
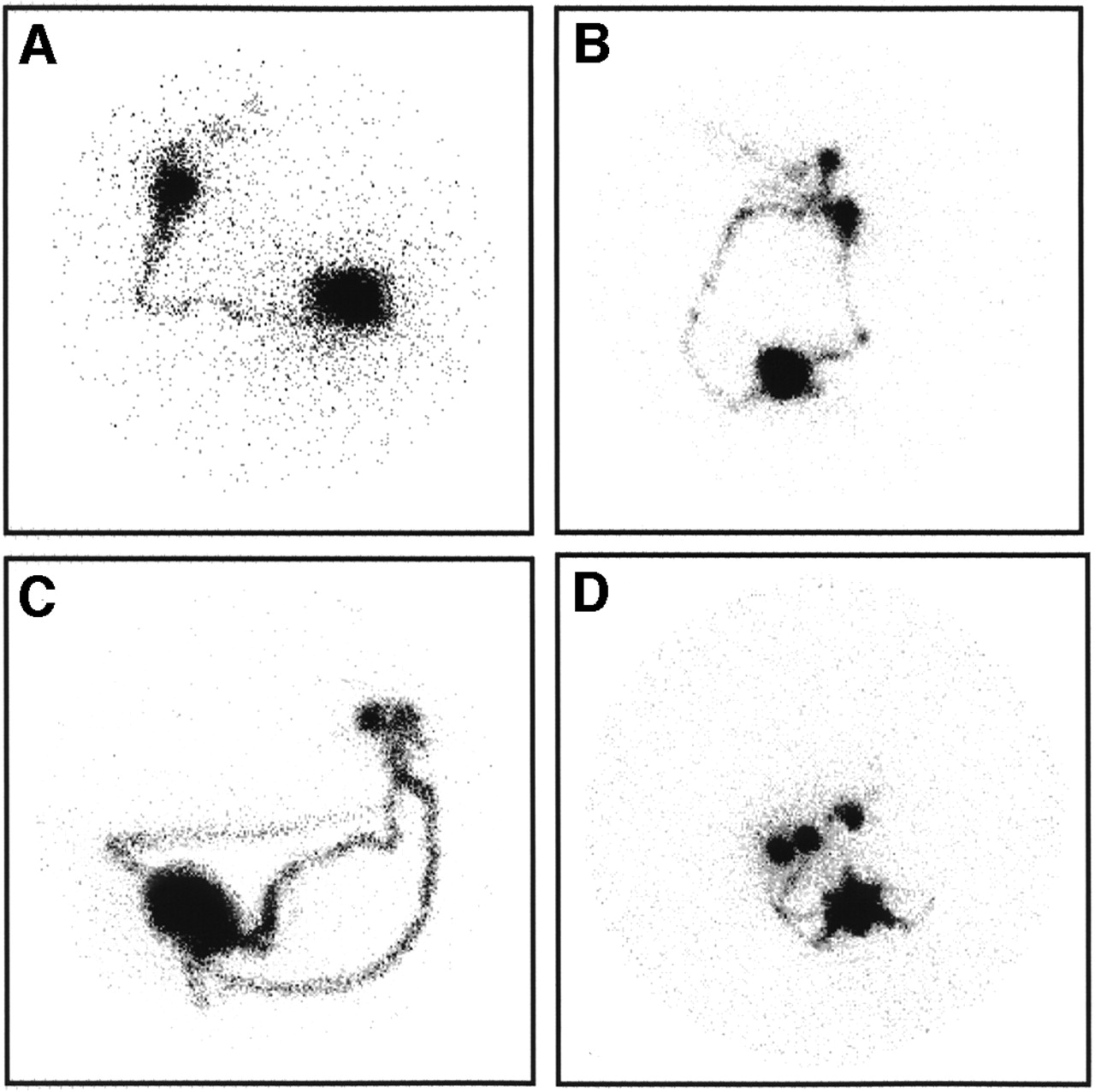
- FIGURE 7.
Representative scans illustrate variable patterns of lymphatic drainage that would not be discerned only by intraoperative γ-probe counting. Imaging times were between 30 and 60 min after intradermal injection of 99mTc-HSA nanocolloid. (A) Right anterior oblique (RAO) view shows single lymphatic vessel leading to single sentinel lymph node, with serial visualization of subsequent-tier nodes. (B) Left anterior oblique (LAO) view shows 2 separate lymphatics leading, through widely diverging pathways, to 2 separate but adjacent sentinel nodes (with serial visualization of subsequent-tier nodes). (C) LAO view shows 3 separate lymphatics leading, through widely diverging pathways, to 2 separate but very close sentinel nodes (2 of vessels, originating at opposite poles of injection site, merge in single channel before crossing path of third vessel). (D) RAO view shows multiple lymphatics leading from site of injection in outer upper quadrant to at least 3 separate sentinel nodes (with serial visualization of subsequent-tier nodes).





Tables
Agent Estimate Median (nm) Concordant (nm) Other (nm) 99mTc-dextran 2–4 2 198Au-colloid 9–15 4–20/30 5–15 99mTc-antimony trisulfide 3–12/30 15–25 17–22 99mTc-sulfur colloid (prefiltered)* 5/15–50 5–25 <30 99mTc-HSA nanocolloid† 4–100 5–80 99mTc-stannous fluoride 50–600 99mTc-rhenium sulfide 50–200/400 40–2,200 440 99mTc-stannous phytate 200–1,000 99mTc-HSA microcolloid‡ 200–2,000/3,000 <1,000 99mTc-sulfur colloid (unfiltered)§ 15/50–>5,000 100/200–1,000 100–600 99mTc-sulfur colloid (modified protocol)¶ <30–>10,000 99mTc-sulfur colloid (filtered)∥ 50–100 50–200 <40 ↵* Commercial preparation microfiltered before freeze-drying and radiolabeling (Lymphoscint; Nycomed-Amersham-Sorin, Sorin, Italy).
↵† About 80% of particles < 40–50 nm, 95% < 80 nm, 4% between 80 and 100 nm, and 1% > 100 nm.
↵‡ About 90% of particles < 1,000 nm.
↵§ About 15%–20% of particles < 100 nm, 70%–80% between 100 and 600 nm, and 2%–4% between 700 and 5,000 nm (minor fraction > 5,000 nm).
↵¶ Reduced heating, with 72-h ingrowth of 99mTc: about 47% of particles < 30 nm, 1% between 50 and 80 nm, 5% between 80 and 200 nm, 21% between 200 and 400 nm, 16% between 400 and 800 nm, 5% between 800 and 2,000 nm, 1% between 2,000 and 5,000 nm, and 5% > 10,000 nm.
↵∥ Depending on pore size used for microfiltration after radiolabeling.
Particle sizes are derived from manufacturers or other sources (11,87,95–98). For comparison scale, molecular size of HSA is approximately 7.2 × 10−6 nm.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- CLINICAL PROBLEM
- ANATOMY AND PHYSIOLOGY OF LYMPHATIC SYSTEM AS IT RELATES TO BREAST CANCER
- RADIOPHARMACEUTICALS
- TECHNIQUES
- RESULTS, CLINICAL SIGNIFICANCE, INDICATIONS, AND CONTRAINDICATIONS FOR SENTINEL LYMPH NODE BIOPSY IN BREAST CANCER SURGERY
- LEARNING CURVE IN SENTINEL LYMPH NODE BIOPSY
- EVALUATING γ-PROBES FOR SENTINEL LYMPH NODE BIOPSY
- RADIATION PROTECTION ISSUES
- CONCLUSION
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Radioguided Surgery
- Clinical Evaluation of 99mTc-Rituximab for Sentinel Lymph Node Mapping in Breast Cancer Patients
- Results of a Prospective Multicenter International Atomic Energy Agency Sentinel Node Trial on the Value of SPECT/CT Over Planar Imaging in Various Malignancies
- In vivo albumin labeling and lymphatic imaging
- Particle-Size and Radiochemical Purity Evaluations of Filtered 99mTc-Sulfur Colloid Prepared with Different Heating Times
- Does the Preparation and Utilization of 99mTc-Sulfur Colloid Affect the Outcomes of Breast Lymphoscintigraphy?
- The Sentinel Node Procedure in Breast Cancer: Nuclear Medicine as the Starting Point
- Evaluation of the Efficacy of a Small CdTe {gamma}-Camera for Sentinel Lymph Node Biopsy
- Sentinel Lymph Node Mapping of the Breast
- Usefulness of Medium-Energy Collimator for Sentinel Node Lymphoscintigraphy Imaging in Breast Cancer Patients.
- Is the "Ideal" {gamma}-Probe for Intraoperative Radioguided Surgery Conceivable?
- Sentinel Lymph Node Detection in Patients with Early-Stage Breast Cancer: Comparison of Periareolar and Subdermal/Peritumoral Injection Techniques
- Patient effective dose from sentinel lymph node lymphoscintigraphy in breast cancer: a study using a female humanoid phantom and thermoluminescent dosemeters
- Lymphoscintigraphy for Sentinel Node Mapping Using a Hybrid SPECT/CT System
- Factors Affecting Visualization Rates of Internal Mammary Sentinel Nodes During Lymphoscintigraphy
- Radioguided Sentinel Lymph Node Biopsy in Malignant Cutaneous Melanoma*