


Abstract
PET measurement of increased oxygen extraction fraction (OEF) identifies patients at high risk for subsequent stroke. OEF methodology remains controversial. In this study we compare the sensitivity and specificity of absolute OEF measurements with ipsilateral-to-contralateral ratios of absolute OEF and count-based OEF estimates. Methods: Multivariate analyses of OEF methods were performed using data from patients with symptomatic carotid artery occlusion (n = 68). Outcome and receiver operating characteristic (ROC) curve analyses were performed. Results: All 3 methods were predictive of stroke risk in univariate analysis. Only the count-based method remained significant in multivariate analysis. The area under the ROC curve was greatest for the count-based ratio: 0.815 versus 0.769 (absolute) and 0.737 (ratios of absolute). Conclusion: All 3 methods are predictive of stroke risk in patients with unilateral carotid artery occlusion. ROC curve analysis is useful for selecting optimal thresholds for maximal sensitivity and specificity.
The presence of increased oxygen extraction fraction (OEF) has been shown to be a powerful and independent predictor of subsequent stroke in patients with atherosclerotic cerebrovascular disease in 2 separate prospective investigations (1,2). However, the method used to determine if OEF was increased differed in these 2 studies. Furthermore, discordant results were reported, depending on methodology (3).
Yamauchi et al. (2) measured mean hemispheric values of OEF in the affected arterial territory in 40 patients with symptomatic stenosis or occlusion of the internal carotid or middle cerebral artery. OEF values above the 95% confidence limit (53.3%) from healthy volunteers were considered abnormal. OEF was increased in 7 patients and was found to be a powerful and independent predictor of subsequent stroke (2,3).
Grubb et al. (1) studied 81 patients with symptomatic carotid artery occlusion as part of the St. Louis Carotid Occlusion Study (STLCOS), a prospective study designed to test the hypothesis that increased OEF was a predictor of stroke risk. Patients were categorized on the basis of left-to-right hemispheric ratios of OEF. Ratios beyond the reference range observed in 18 healthy volunteers were considered increased. Increased OEF was found to be a powerful and independent predictor of subsequent stroke (11/13 strokes occurred in the 39 patients with increased OEF).
Measurement of absolute OEF was not possible in 13 of the 81 patients, and a count-based method for OEF estimation was used to generate hemispheric ratios (4). In the 68 patients with complete quantitative studies (the same cohort as for the present analysis), both methods were significant predictors of stroke risk (4).
Recently, Yamauchi et al. (3) reported 5-y follow-up data on their 40 patients, as well as an analysis of OEF methodology (comparing absolute OEF and hemispheric ratios of absolute values). Hemispheric ratios of absolute OEF failed to predict stroke risk. They concluded that absolute values of OEF were better predictors of stroke risk than hemispheric ratios.
The purpose of this brief communication is to reconcile these data: first, to repeat the STLCOS outcome analysis using absolute values of OEF as predictors of stroke risk; and second, to present a direct comparison of the different OEF methods as predictors of stroke risk, using clinical outcome and OEF data from the STLCOS.
MATERIALS AND METHODS
This study was a retrospective analysis of prospectively collected clinical and PET data from 68 patients with symptomatic atherosclerotic carotid artery occlusion and complete quantitative OEF studies enrolled in the STLCOS (1). All patients had atherosclerotic occlusion of 1 common or internal carotid artery and ipsilateral ischemic symptoms. Patients were followed for the occurrence of stroke or death for the duration of the study. Eighteen healthy volunteers were studied to establish a reference range of OEF values. All studies were performed under institutional review board–approved protocols. Informed consent was obtained from all subjects.
PET Measurements of OEF
PET studies were performed on 1 of 2 scanners (ECAT 953B or ECAT EXACT HR; Siemens, Iselin, NJ). PET images were reconstructed to a uniform resolution of 16-mm full width at half maximum using a 3-dimensional gaussian filter. The map of absolute OEF was created by the technique of Mintun et al. (5). The count-based OEF image was generated as the ratio of the counts in the oxygen image divided by the water image and normalized to a whole-brain mean of 0.40 (4). For each subject, 7 spheric regions of interest 19 mm in diameter were placed in the cortical territory of the middle cerebral artery in each hemisphere using stereotactic coordinates. Areas of prior infarction and their contralateral regions were excluded from analysis. Mean hemispheric absolute values and ipsilateral-to-contralateral hemispheric ratios of both OEF methods were calculated from the remaining regions.
Analysis for Present Study
Nine strokes occurred during 2.3 y of follow-up (all ischemic and ipsilateral to the occluded carotid artery). Kaplan–Meier analysis of absolute OEF was performed using ipsilateral stroke as the endpoint (Mantel–Cox log rank). The same analysis of the 2 ratio methods has been reported for these 68 patients (4). The Cox proportional hazards model was used to test the 3 different OEF methods. Forward and backward stepwise selection based on maximum partial likelihood estimation was used for multivariate analyses. Receiver operating characteristic (ROC) curves for the diagnosis of ipsilateral stroke risk were generated by progressively increasing the threshold value of absolute hemispheric OEF to define the OEF values of patients as abnormal. This curve was compared with previously published data for the 2 ratio methods (4).
RESULTS
Mean hemispheric (±SD) absolute OEF in the healthy volunteers was 0.41 (±0.09; range, 0.26–0.64). Absolute OEF was not a significant predictor of ipsilateral stroke using the upper limit of the reference range (4 patients categorized with increased OEF, P = 0.21). When the upper 95% confidence limit for absolute OEF (0.44) was used, 33 of the 68 patients were categorized as having increased OEF. Eight of the 9 strokes occurred in these patients (P = 0.0042).
All 3 methods were significant predictors of stroke risk as individual continuous variables. In multivariate analysis comparing all 3 methods, only the count-based method remained in the final model (P = 0.0028). Absolute hemispheric values performed better than ratios of absolute values (P to remove = 0.0043). ROC analysis (Fig. 1) revealed a similar order of performance, with the area under the curve for the absolute OEF (0.769) falling between the count-based ratio method (0.815) and the ratio of absolute hemispheric values (0.737).
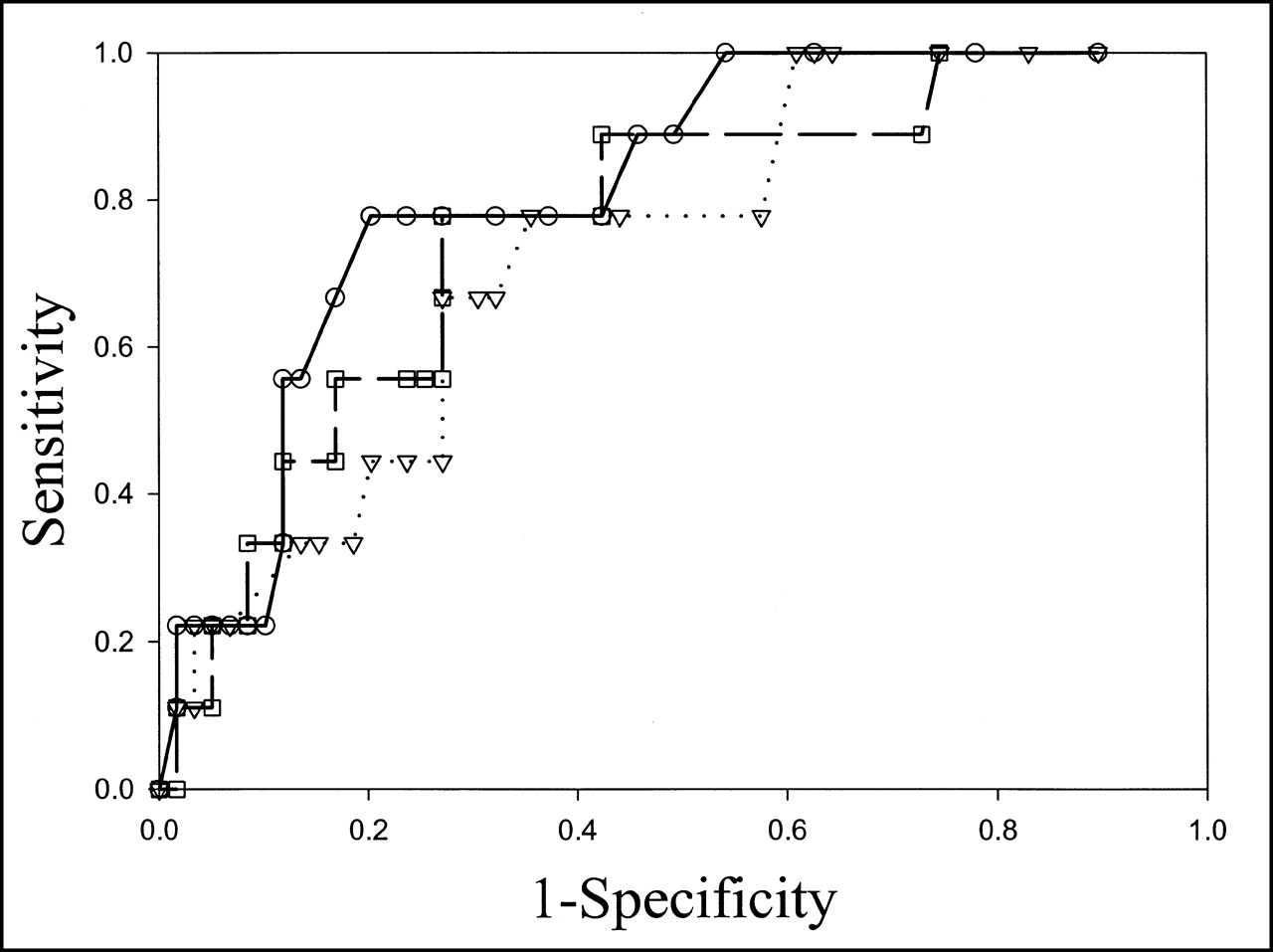
ROC curves for all 3 OEF methods. On solid line, ○ indicates hemispheric ratios of count-based OEF; on dotted line, ▿ represents hemispheric ratios of absolute OEF; and on dashed line, □ indicates absolute values of OEF. These curves were generated by progressively increasing threshold for determining whether OEF was increased. At lowest thresholds (far upper right of curve), all patients had increased OEF and all 9 strokes occurred in these patients. At this point in curve, all methods have 100% sensitivity (ability to identify patients with subsequent stroke) but poor specificity (ability to identify patients without subsequent stroke). As threshold becomes higher (moving leftward toward origin), sensitivity falls as specificity improves. The curves are similar; however, there is greater area beneath curve for count-based ratio method, which suggests best performance.
DISCUSSION
All 3 methods are predictive of stroke risk as both continuous and dichotomous variables. Both ratio techniques were previously shown to be significant predictors of risk for ipsilateral stroke as dichotomous variables for this same group of 68 patients (Kaplan–Meier log rank, P = 0.0048 [count-based] and P = 0.025 [absolute ratios]) (4). The failure of hemispheric ratios of absolute OEF as a dichotomous variable to predict stroke in the study of Yamauchi et al. (3) may be caused by several factors, including the threshold used to identify increased OEF and the inclusion of patients with bilateral carotid occlusion. The importance of optimizing the threshold used to identify increased OEF is emphasized by the initial failure of absolute OEF to predict stroke in this study.
The multivariate and ROC analyses of our data support the conclusion of Yamauchi et al. (3) that absolute values of OEF are better predictors of future stroke than hemispheric ratios of absolute OEF values. This study also suggests that the count-based OEF method performs better than absolute values of OEF measured by the technique of Mintun et al. (5). In part, this may be because of the effect of blood volume asymmetry. Blood volume may increase with autoregulatory vasodilation. Hemispheric increases in the count-based OEF image may reflect the effects of both increased oxygen extraction and increased blood volume, because there is no correction for unextracted oxygen remaining in the blood with the count-based method.
CONCLUSION
All 3 methods are predictive of stroke risk in patients with unilateral carotid occlusion. Count-based ratios of OEF perform as well as or better than absolute values or ratios of absolute values of OEF, when OEF is measured using the technique of Mintun et al. (5). The count-based OEF method does not require arterial input data, a measurement of blood volume, or complicated metabolic processing. The count-based method is a practical and accurate technique for identification of patients with increased OEF, particularly in the setting of a multicenter trial.
Acknowledgments
This study was supported by grants NS02029 and NS28947 from the National Institute of Neurological Disorders and Stroke, National Institutes of Health.
Footnotes
Received Dec. 19, 2000; revision accepted Apr. 9, 2001.
For correspondence or reprints contact: Colin P. Derdeyn, MD, Mallinckrodt Institute of Radiology, 510 S. Kingshighway Blvd., St. Louis, MO 63110.
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Hemodynamic Impairment Measured by Positron-Emission Tomography Is Regionally Associated with Decreased Cortical Thickness in Moyamoya Phenomenon
- Baseline Hemodynamic Impairment and Future Stroke Risk in Adult Idiopathic Moyamoya Phenomenon: Results of a Prospective Natural History Study
- Cortical Cerebral Blood Flow, Oxygen Extraction Fraction, and Metabolic Rate in Patients with Middle Cerebral Artery Stenosis or Acute Stroke
- William M. Feinberg Award for Excellence in Clinical Stroke: Hemodynamics and Stroke Risk in Carotid Artery Occlusion
- Oxygen Extraction Fraction and Stroke Risk in Patients with Carotid Stenosis or Occlusion: A Systematic Review and Meta-Analysis
- Failure of Cerebral Hemodynamic Selection in General or of Specific Positron Emission Tomography Methodology?: Carotid Occlusion Surgery Study (COSS)
- Shorter Examination Method for the Diagnosis of Misery Perfusion with Count-Based Oxygen Extraction Fraction Elevation in 15O-Gas PET
- Diagnosis of Misery Perfusion Using Noninvasive 15O-Gas PET
- Cerebral Oxygen Metabolism and Neuronal Integrity in Patients With Impaired Vasoreactivity Attributable to Occlusive Carotid Artery Disease
- Guidelines and Recommendations for Perfusion Imaging in Cerebral Ischemia: A Scientific Statement for Healthcare Professionals by the Writing Group on Perfusion Imaging, From the Council on Cardiovascular Radiology of the American Heart Association
- Re: Stages and Thresholds of Hemodynamic Failure