


Abstract
Periareolar (PA) injection offers several potential advantages over other techniques for visualizing sentinel lymph nodes (SLNs) in patients with early breast cancer. However, few studies have been published on this procedure. This study was designed to validate PA injection technique and compare it with the subdermal/peritumoral (SD/PT) injection technique. Methods: The study included 324 patients in whom 330 breast cancers (T) had been identified by biopsy. This population was divided in 4 groups: (A) 148 patients (150 T) in whom lymphatic mapping was performed by injecting radiotracer with the SD/PT technique; (B) 59 patients (60 T) in whom lymphatic mapping was performed with a combination of blue dye injected with the PA technique and radiotracer injected with the SD/PT technique; (C) 58 patients (60 T) in whom blue dye was injected subdermally and radiotracer was injected periareolarly; and (D) 59 patients (60 T) in whom both blue dye and radiotracer were injected periareolarly. Results: Concordances in the SLN detection rate between blue dye and radiotracer in groups B, C, and D were 98.1%, 100%, and 100%, respectively. The SLN identification rates with the PA technique were 98.3% and 95%, respectively, for radiotracer and blue dye. With the SD/PT technique, these rates were 90.5% and 88.3%, respectively, for radiotracer and blue dye. At lymphoscintigraphy, SLN visualization required the acquisition of late images (3 h after the injection) in 20% of patients who received PA injections and 39.5% of patients who received SD/PT injections. Conclusion: These findings validate the PA injection technique and underline some of its reported advantages in comparison with the SD/PT technique.
Since its introduction in the mid 1990s, sentinel lymph node (SLN) biopsy has been rapidly and widely adopted for axillary staging in patients with early breast cancer. To identify the SLN, different injection techniques have been used, and the optimal site of injection remains a subject of study (1–3).
Periareolar (PA) injection offers several potential advantages in comparison with other approaches (2–4). Because a rich lymphatic network beneath the areola efficiently and rapidly clears the tracer, a high percentage of the injected agent reaches the SLN, making identification much easier and decreasing the learning curve (4). For the same reasons, the SLN is more rapidly visualized in the axilla (5). The need for image-guided injection is eliminated by the PA approach in patients with nonpalpable tumors (6). The so-called “shine-through” effect from tumors located in the upper outer quadrant of the breast is decreased, because the PA injection increases the distance between the injection site and the axillary SLN (4). Because lymphatic drainage of the breast goes to the same SLN, intraoperative mapping of the SLN with a PA injection could be feasible even in multifocal and multicentric tumors (7).
The rationale for PA injection is based on the fact that under normal circumstances the breast (the mammary gland and its overlying skin) can be considered as a single biologic unit with a common centrifugal lymphatic pathway to the same axillary lymph nodes, whereas only about 3% of the lymphatic flow drains to the parasternal and internal mammary chain (IMC) nodes and a minimal proportion to the posterior intercostal nodes (8–10).
In breast parenchyma, lymph vessels accompany the lactiferous ducts centripetally toward the subareolar (SA) plexus of Sappey, where pooling of lymph from all parts of the breast occurs. Then, lymph trunks (generally 2) leave the areolar region to course superficially toward the lower axillary (sentinel) lymph nodes. Therefore, a PA injection would be ideal to determine the primary lymph flow to the SLN.
To date, published studies on PA injection technique are few (4–7,10–16). However, if positive results receive additional validation, PA injection could replace other techniques (2,3).
The aim of this study is to validate the PA injection technique in patients with early breast cancer and compare it with the subdermal/peritumoral (SD/PT) technique, which has been used in our institution since 1998.
MATERIALS AND METHODS
Patient Population
The study population included 324 patients (mean age, 59.8 ± 10.6 y; range, 28–83 y) with histologically proven breast cancer who underwent lymphoscintigraphy in our institution between July 2000 and July 2003. Patients were referred for 99mTc-labeled albumin nanocolloid study for lymphatic mapping after identification of breast tumors. Six patients had bilateral breast cancers, so that a total of 330 breast cancers were included in this study (139 left and 191 right breast). Exclusion criteria were palpable axillary lymph nodes, tumor diameter > 2.5 cm, multifocal or multicentric cancer, and pregnancy.
All patients were studied after written informed consent was obtained.
Study Design
The 330 included tumors were assigned to 4 groups.
Group A included 150 retrospectively and consecutively enrolled tumors (148 patients) previously studied in our institution from July 2000 to December 2001. Patients in this group had 110 tumors located rather superficially in the breast (palpable tumors) and 40 tumors located deep within the mammary gland (nonpalpable tumors). Lymphatic mapping was performed using a radiotracer, injected subdermally or peritumorally in the presence of palpable or nonpalpable tumors, respectively.
Group B included 60 tumors (59 patients) consecutively enrolled from January to July 2002. In this group, lymphatic mapping was performed with the radiotracer injected subdermally (42 palpable tumors) or peritumorally (18 nonpalpable tumors) and with blue dye injected periareolarly in both palpable and nonpalpable tumors.
Group C included 60 tumors (58 patients) consecutively enrolled from July to December 2002. In this group, lymphatic mapping was performed with the radiotracer injected periareolarly and the blue dye injected subdermally on the tumor. The group included 37 palpable and 23 nonpalpable tumors.
Group D included 60 tumors (59 patients) consecutively enrolled from January to July 2003. In this group, lymphatic mapping was performed with both radiotracer and blue dye injected periareolarly. The group included 41 palpable and 19 nonpalpable tumors.
The study, in which lymphatic mapping was performed with different tracers injected at different sites, was designed to compare the PA technique with the SD/PT technique and to verify which SLN was identified with the PA technique and which with the SD/PT technique and thereby derive the concordance rate between the 2 techniques.
Radiotracer
We used 99mTc-labeled human serum albumin nanocolloid (Nanocoll; Nycomed-Amersham-Sorin S.r.l.) with a particle size of 4–100 nm (95% of particles < 80 nm).
Radiotracer Injection
SD/PT Technique (Groups A and B).
Because it is reasonable to assume that the SD and PT injection techniques are complementary (1), our routine approach is to inject the radiocolloid subdermally when the tumor is located superficially in the breast (i.e., the tumor is palpable) and peritumorally when the tumor is located deep within the mammary gland (nonpalpable). For palpable tumors, 20–40 MBq 99mTc-nanocolloid in a volume of 0.5 mL were injected subdermally on the tumor 18–24 h before surgery. For nonpalpable tumors, 20–40 MBq 99mTc-nanocolloid in a volume of 0.5 mL were injected peritumorally under echographic or stereotactic guidance.
PA Technique (Groups C and D).
In these groups, 20–40 MBq 99mTc-nanocolloid in a volume of 0.5 mL were injected periareolarly the day before surgery. Injection was performed subdermally at the PA site as a single aliquot at the level corresponding to the tumor (Fig. 1).

PA injection technique. The tracer is injected subdermally as a single aliquot at the PA site at the corresponding level of the tumor.
In all groups, independently from the site of the injection, a gentle massage was performed for 2–3 min to aid the clearance of radiocolloid.
Lymphoscintigraphy
All patients underwent lymphoscintigraphy. Scintigraphic images were acquired with a γ-camera (model 400T; General Electric) fitted with a high-resolution collimator. The acquisition window was set at 140 keV. Matrix size was 256 × 256.
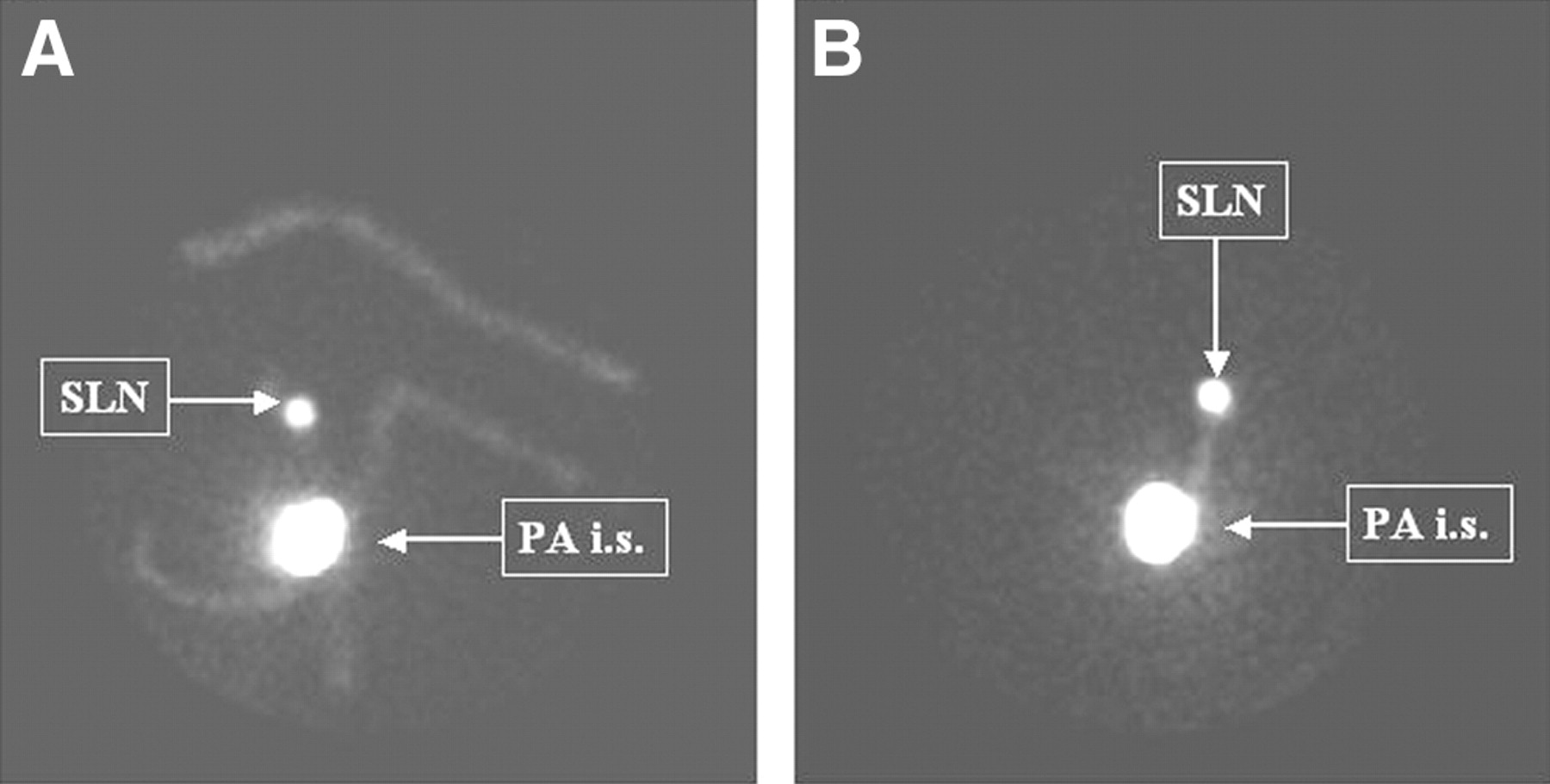
Acquisitions were acquired with patients’ arms in the surgical position. Static images were acquired at 1 h after radiotracer injection (early images) and, if an SLN was not visualized, at 3 h (late images). We acquired static anterior and lateral views to locate SLNs (Fig. 2), and the locations were marked on the skin with indelible ink.

Early lymphoscintigraphy images. Periareolar injection site (i.s.) and an axillary SLN are imaged after PA injection. Anterior (A) and lateral (B) views are shown.
Blue Dye Injection and Surgery
Between 5 and 20 min before surgery, all patients were injected with 1% Lymphazurin blue dye in 2.5–5 mL solution either subdermally on the tumor (group C) or in the PA area of the tumor-bearing breast (group B and D). Although the volume of the injections was large, patients reported no discomfort and no permanent tattoo resulted. After the injection, a gentle massage was performed for 2–3 min, independently from the site of injection.
In all patients, the SLN procedure was performed before removal of the breast tumor. Axillary skin was incised and a careful dissection was performed in search of the blue lymphatic channels draining to a blue-stained lymph node.
An intraoperative γ-detecting probe (neo2000 [Neoprobe Corp.] equipped with a 14-mm reusable probe) was used to identify the site of greater radioactivity before skin incision.
SLNs were identified if they were blue, had in vivo radioactive counts at least 3 times greater than background counts in the axilla, or had both characteristics.
A level I and II axillary lymph node dissection was performed if no SLNs were identified or if SLNs were positive for tumor metastasis (micro- or macrometastases).
Pathologic Evaluation
Lymph nodes were identified as sentinel or nonsentinel. No intraoperative frozen section analyses were performed. The SLNs were formalin fixed, paraffin embedded, and sectioned (at least 36 sections, 50-μm spaced). Histologic evaluation was performed with hematoxylin and eosin and with cytokeratin antibody (AE1/3, monoclonal antibody, 1:250; Boehringer Mannheim) with a negative control. All non-SLNs were evaluated with standard hematoxylin-and-eosin–stained sections.
Primary tumors or reexcision specimens were evaluated by routine histology.
Statistical Analysis
In each group, we calculated the percentage of cases in which an SLN was identified by radiotracer and blue dye (when used). In groups B, C, and D, we calculated the concordance between radiotracer and blue dye in identifying SLNs. Differences between SLN identification rate obtained with the PA and SD/PT injection techniques were statistically tested with the χ2 test. The same test was used to evaluate differences in the number of late images necessary to visualize SLNs when radiotracer was injected with the PA or SD/PT techniques.
RESULTS
Patient population characteristics for each group are reported in Table 1.
Patient Population
Group A
Radioguidance (combined lymphoscintigraphy and intraoperative γ-probe counting) enabled the detection of one or more SLNs in 135 of 150 tumors (90%). SLNs were detected in the axilla in 96 of these (71.1%), in the IMC in 27 (20%), in both axilla and IMC in 5 (3.2%), and in the supraclavicular region in 7 (5.2%). In tumors with positive scans, an average of 1.47 SLNs (n = 176; range, 1–6) were visualized.
Group B
With nanocolloid and blue dye tracers combined, we identified one or more SLNs in 59 of 60 (98.3%) breast tumors. Blue dye alone detected SLNs in 56 of 60 cancers (93.3%). Radioguidance alone enabled the detection of one or more SLNs in 55 of 60 cancers (91.7%). SLNs were detected in the axilla in 47 (85.5%) of these, in both axilla and IMC in 5 (9.1%), and in the IMC in 3 (5.4%). In tumors with positive scans, an average of 1.42 SLNs (n = 78; range, 1–5) were visualized.
SLNs were identified by both blue dye and radiotracer in 52 of 60 cancers (86.7%). In 51 of 52 tumors, the lymph nodes were blue and “hot.” The concordance rate was 98.1%. SLNs were identified by blue dye alone in 4 tumors (6.7%) and by isotope alone in 3 (5%).
Group C
With nanocolloid and blue dye tracers combined, one or more SLNs were identified in all 60 tumors. Blue dye alone detected SLNs in 53 of 60 cancers (88.3%). Radioguidance alone enabled the detection of one or more SLNs in 59 of 60 cancers (98.3%). SLNs were detected in the axilla in 57 (95%) of these and in both axilla and IMC in 2 (3.3%). In tumors with positive scans, an average of 1.9 SLNs (n = 113; range, 1–4) were visualized.
SLNs were identified by both techniques in 52 cancers. In all these tumors, lymph nodes were blue and “hot” and the concordance rate was 100%. SLNs were identified by blue dye alone in 1 tumor (1.7%) and by isotope alone in 7 (11.7%).
Group D
With nanocolloid and blue dye tracers combined, one or more SLNs were identified in 59 of 60 (98.3%) breast tumors. Blue dye alone detected SLNs in 58 of 60 cancers (96.7%). Radioguidance alone enabled the detection of one or more SLNs in 59 of 60 cancers (98.3%). SLNs were detected in the axilla in 57 (95%) of these and in the IMC in 2 (3.3%). In tumors with positive scans, an average of 1.8 SLNs (n = 106; range, 1–5) were visualized.
SLNs were identified by both techniques in 58 cancers (96.7%). In all of these tumors, lymph nodes were blue and “hot”; therefore, the concordance rate was 100%. SLNs were identified by isotope alone in 1 case (1.7%).
Periareolar Versus Subdermal/Peritumoral Injection Technique
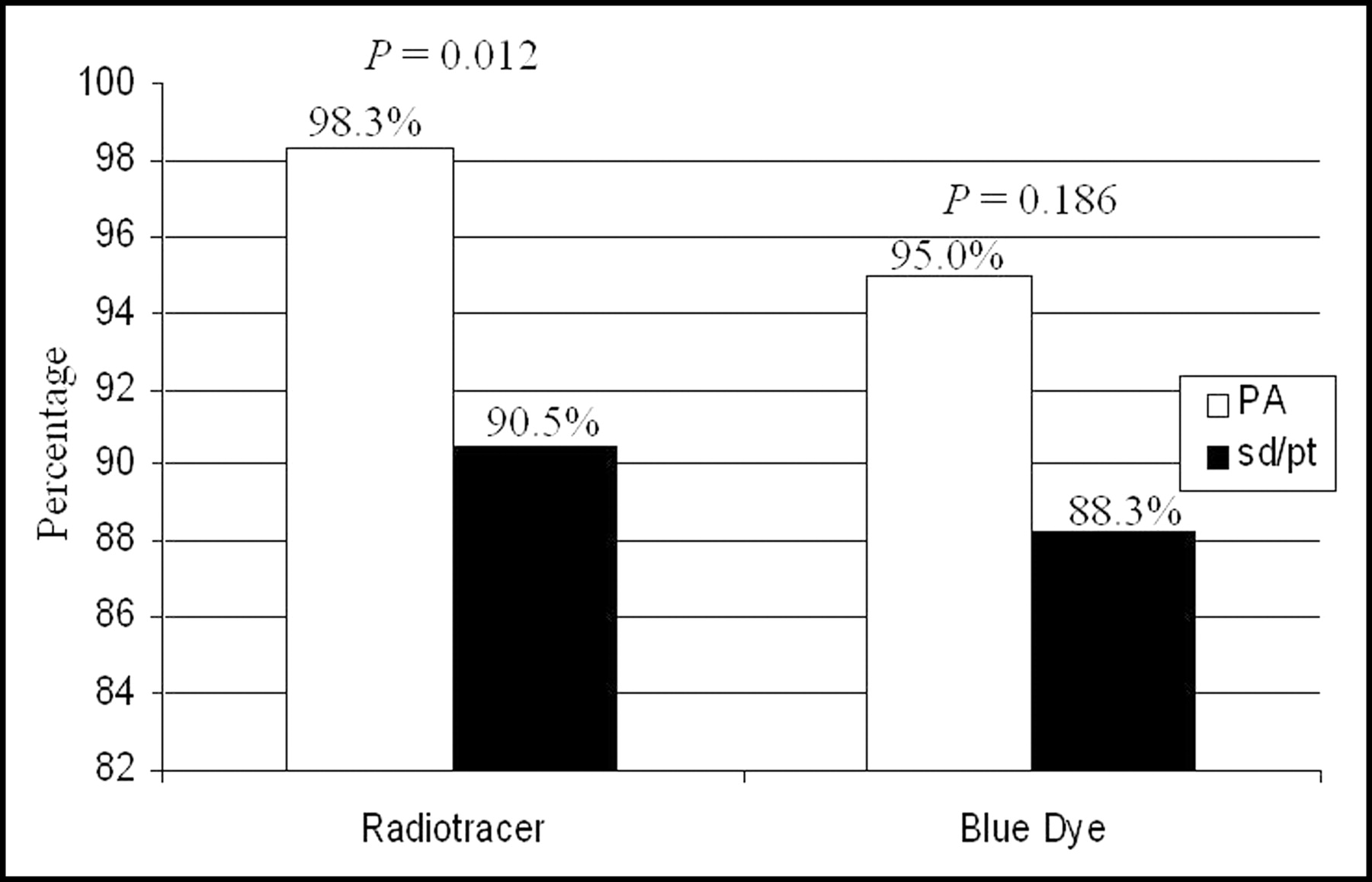
Significant differences in SLN identification rate were observed with different injection sites (Fig. 3). When the radiotracer was injected with the PA technique (groups C and D), SLNs were visualized in 118 of 120 cancers (98.3%). When the radiotracer was injected with the SD/PT technique (groups A and B), SLNs were visualized in 190 of 210 cancers (90.5%; χ2 = 6.366; P = 0.012). Similar results (although not statistically significant) were obtained using blue dye, with which PA injection allowed identification of 114 of 120 (95%) cancers, whereas the SD injection allowed identification of 53 of 60 (88.3%; χ2 = 1.751; P = 0.186).

SLN identification rates with the PA and SD/PT injection techniques.
When radiotracer was injected with the PA technique (groups C and D), the acquisition of late images was necessary in 24 of 120 cancers (20%) for SLN visualization. On the other hand, with SD/PT injection, late images were necessary in 83 of 210 cancers (39.5%; χ2 = 12.409, P < 0.001).
Image-guided injection of radiotracer was necessary in 58 of 210 cancers (27.6%) in groups A and B (40 and 18 cancers, respectively).
DISCUSSION
A number of techniques have been used in SLN mapping in breast cancer, including variations in choice of localizing agent, particle size, timing of injection, scintigraphic imaging, surgery, and site of injection (1–3). However, in a recent metaanalysis, concordance of SLN biopsy with axillary lymph node dissection did not vary significantly among these techniques (17). To understand how these techniques have yielded similar results, it is essential to gain a thorough knowledge of the lymphatic drainage pattern of the breast. Sappey (18) described the lymphatic flow in the breast in 1834 as traveling centripetally to the SA plexus and then to the axilla via lymphatic collecting channels. In the 1950s, Turner-Warwick showed that lymph flows from the superficial to the deep layers and then toward the regional (axillary) lymph nodes through lymph channels that originate in the interlobular spaces and along the lactiferous ducts (9).
Although slightly different, each of these findings is consistent with the existence of a common afferent lymphatic channel system to a common axillary SLN. This would explain the accuracy of breast SLN biopsy when using any of the reported techniques, including PT, dermal, SD, and SA/PA injection (17).
To date, few studies have evaluated the feasibility of PA and SA injection. In 1999, Klimberg et al. (6) compared the SA injection of labeled sulfur colloid with the PT injection of isosulfan blue in 69 cases and concluded that SA injection of 99mTc is as accurate as PT injection of blue dye. In the same year, Kern (5) used blue dye alone, injected subareolarly, to visualize SLNs in 40 patients with operable breast cancers, concluding that this technique had demonstrated a high SLN identification rate, no false-negatives, and a rapid learning curve.
In 2000, Borgstein et al. (10) compared PT with intradermal PA injection of blue dye and concluded that the PA technique appeared ideal in identifying the principal (axillary) route of metastasis in early breast cancer.
In 2002, Shimazu et al. (4) found that PA injection of radiolabeled tin colloid in 52 patients was superior to PT injection because of the former method’s simplicity, high success rate in lymphoscintigraphy, and SLN detection. Similar conclusions were reported by Bauer et al. (13), who subareolarly injected blue dye in 249 patients. Moreover, Kern (14) was the first to use and compare SA injections of the same volumes of blue dye and radiocolloid. He found a concordance rate that ranged between 98.9% (“blue hot” concordance) and 95.1% (“hot blue” concordance).
Finally, in 2003, Maza et al. (15) compared detection rates obtained with PT versus SA injections of labeled nanocolloid in terms of SLNs identified and localization. They concluded that a simple SA injection in the clock position is sufficient for SLN detection in breast cancer.
Despite the small number of patients in most of these series, there appears to be a persistent trend, with SA/PA injection offering a higher rate of SLN identification and good concordance with SLNs identified by other injection techniques. The reported advantages of PA injection led us to evaluate this modality in comparison with the SD/PT techniques.
Since 1998, after a 2-mo learning period in our institute, we performed lymphatic mapping in patients with early breast cancer. Our technique included SD injection of labeled tracer in patients with superficial or palpable tumors and PT injection under echographic or stereotactic guidance in patients with tumors located deep within the mammary gland (1). In January 2002, we began PA injection of blue dye. The preliminary results of the PA blue dye injection compared with SD injection of radiolabeled nanocolloid were presented previously (16). In that article, we observed that PA injection of blue dye obtained results that were comparable with those of SD injection and that concordance between the techniques in terms of SLN detection was complete. Therefore, we initiated a second part of the study, in which we injected radiotracer periareolarly, with blue dye injected subdermally. We also initiated a third part in which blue dye and radiotracer were both injected with the PA technique. This study design allowed us to definitively validate the PA technique and to underline its possible advantages in comparison with the SD/PT technique.
In fact, we observed that when both tracers identified an SLN, this turned out to be the same node, even when the injection sites were different, with concordance rates of 98.1% and 100%, respectively, in groups B and C. This finding is in agreement with the hypothesis that the breast functions as a single biologic unit and that the preferential lymph drainage pathway from all quadrants is essentially toward the same axillary SLN (10). This finding led us to validate the PA injection technique.
The PA injection technique was confirmed to have several advantages over the SD/PT technique. When the tracers (labeled nanocolloid or blue dye) were injected periareolarly, the SLN identification rate was significantly higher than with the SD/PT injection (Fig. 3). Also, we noticed at lymphoscintigraphy that the rate of late images necessary to visualize SLNs was significantly reduced (20% when injected with the PA technique; 39.5% with the SD/PT technique). Finally, with the PA injection technique, the need for image-guided injection was eliminated in those patients with nonpalpable tumors.
We did not observe the “shine-through” effect of tumors localized in the outer upper quadrant with SLN mapping using the SD/PT injection of labeled nanocolloid. Therefore, we are unable to address this reported advantage arising from the PA injection technique. The feasibility of identifying the SLN in multifocal/multicentric breast tumors was not considered in our study, because this type of pathology was not included in our population.
The detection rates of IMC lymph nodes obtained with the PA and SD/PT techniques showed great differences. In fact, when radiotracer was injected with the SD/PT technique, 30 of 210 (14.3%) IMC tumors were detected, where 2 of 120 (1.7%) were detected with the PA injection. This finding is in agreement with that reported by several authors (10,15). Even if we cannot ignore the existence of alternative drainage pathways, there is considerable agreement that axillary lymph node status is crucial in the nodal staging of early breast cancer. Moreover, the incidence of isolated IMC metastases in the absence of axillary metastases is low (19). Although the recent interesting findings of Galimberti et al. (20) could change this viewpoint, according to current treatment and staging concepts, the detection of IMC lymph nodes has no therapeutic consequences (21,22). Thus, biopsies are not usually performed, and the lower IMC lymph node detection rate cannot be considered a major disadvantage.
The study had some limitations. The accuracy of the PA technique was not validated, because we did not perform axillary lymph node dissection in those cases in which the SLN biopsy proved negative. Therefore, the true false-negative rate, as in other series (6,12), is not known. Instead, we correlated the results with the standard SD/PT injection of blue dye or radiotracer to determine whether the 2 techniques mapped the same lymph node.
CONCLUSION
In conclusion, we believe that the results of this study strongly validated the PA technique (with a concordance rate between blue dye and radiotracer nearly 100%) and showed its advantages in comparison with the SD/PT injection technique. With the PA injection technique, the identification rate was higher than that with the SD/PT injection technique, fewer late images were necessary to visualize the SLN, and image guiding was not need for injection in patients with a nonpalpable tumor.
Footnotes
Received Jul. 9, 2003; revision accepted Oct. 23, 2003.
For correspondence or reprints contact: Gianni Bisi, MD, PhD, Università di Torino, Medicina Nucleare, Dipartimento di Medicina Interna, Corso Bramante, 88, 10126 Torino, Italy.
E-mail: gianni.bisi{at}unito.it




{kind=link}
{kind=link}
{kind=link}