


Abstract
Lymphoscintigraphy is performed before sentinel node (SN) biopsy for SN mapping. It is of clinical importance mainly if the tumor is located in body parts with ambiguous lymph node drainage. The purpose of this study was to assess the clinical benefit of fused SPECT/CT images to planar images for SN mapping. Methods: Thirty-four consecutive patients with cutaneous malignant melanoma (n = 28) and squamous cell carcinoma (n = 6) and scheduled for SN biopsy were enrolled. Primary tumors were located in the trunk (n = 12), in the extremities (n = 12), in the head and neck (n = 9), and in the penis (n = 1). Scintigraphy was performed using a hybrid gamma-camera/low-dose CT system. Planar images and fused SPECT/CT images were interpreted separately. Results: SPECT/CT identified multiple draining basins in 6 of 12 patients (50%) with trunk melanoma and in 3 of 9 patients (33%) with head and neck melanoma or mucosal tumor. In 9 of 21 patients (43%) with a primary tumor located in the head and neck or trunk region, SPECT/CT-fused images identified SNs that were missed on planar images, 2 of which were involved with tumor. Three of the 9 nodes were located close to the injection site and were hidden by its scattered radiation, and 2 were in-transit nodes. Another 4 nodes, identified on fused images only, were located in an additional basin to those identified on planar images. Fused images were of no added value either in patients with limb melanoma or in a patient with a penile melanoma. Conclusion: SPECT/CT SN mapping provides additional data that are of clinical relevance to SN biopsy in patients with trunk or head and neck melanoma and in patients with mucosal head and neck tumor.
A sentinel node (SN) is defined as the first lymph node in a lymph node bed to receive lymphatic drainage from a tumor. It is the most likely site of early metastasis. Tumors drain initially to one or several SNs that lie on the direct lymphatic drainage pathway of the individual tumor (1–3). The histopathologic findings in the excised SNs may indicate the need for a further dissection of the nodal basin if metastatic spread or micrometastases are found. Alternatively, if the SN is tumor free, the nodal basin can be regarded as free of disease and an unnecessary dissection can be avoided. Identification and removal of SNs may be followed by a meticulous examination of the latter using step-sectioning and immunohistochemistry staining methodology, thereby improving the accuracy of early metastatic spread diagnosis (4). Even in the era of emerging tumor imaging modalities, such as PET, SN biopsy (SNB) is considered the only reliable method for identifying micrometastatic disease in regional lymphatic nodes (5).
SN mapping has been suggested in the management of various human malignancies, including cutaneous malignant melanoma, squamous cell carcinoma (SCC) of the head and neck region, vulvar and penile malignancies, and breast cancer (2,6–8). At surgery, the search for SNs may be performed either by blue dye injection coloring of the nodes or by injection of labeled particles before surgery and by the use of a hand-held probe during surgery to locate the nodes with the highest counts. The importance of scintigraphic SN mapping before surgery is enhanced in tumors located in body parts with ambiguous lymph node drainage, such as the trunk, shoulder, and the head and neck. Drainage from these regions is unpredictable and is individual for each tumor (9,10). Presurgical lymphoscintigraphic SN mapping may, therefore, assist the surgeon in tailoring the field of surgery and provide guidance at the incision site (2,11,12).
Previous reports have discussed the technical details required for accurate scintigraphic SN mapping. These include the use of various radiopharmaceuticals, acquisition protocols, markers, and transmission images with a 57Co flood source to facilitate localization of lymphatic nodes and also skin marking to reduce operating time for SN identification and minimize the surgical incision (1,3,13−18). The aim of this study was to assess the potential role of fusion of the SPECT lymphoscintigraphy data with CT in the clinical setting of scintigraphic SN mapping using a hybrid gamma-camera/low-dose CT system that allows SPECT and CT to be performed at the same setting without changing the patient’s positioning (19).
MATERIALS AND METHODS
Patient Population
Lymphoscintigraphy using a hybrid SPECT/low-dose CT system was performed in 34 consecutive patients referred for SN mapping. These included 28 patients with cutaneous malignant melanoma and 6 patients with mucosal SCC of the head and neck region. Primary tumors were localized in the limbs in 12 patients (8 in the lower extremities, 4 in the upper extremities), in the trunk in 12 patients, in the head and neck region in 9 patients, and in the penis in 1 patient. There were 20 male and 14 female patients, with a mean age 52 ± 17 y (range, 19–81 y).
Scintigraphic Technique
Seventy-four MBq (2 mCi) 99mTc-rhenium colloid (TCK-17, CIS International) divided into 4 equal aliquots of 0.4 mL each were injected at the borders of the primary tumor site using 25-gauge insulin syringes. If the primary tumor had been removed, the injections were performed on either side of the excisional scar. In the case of melanoma, injection was intradermal whereas, in the case of SCC of the mouth and tongue, the injection was submucosal. The rhenium colloid preparation has a particle size of 50–100 nm, larger than the 99mTc-antimony trisulfide colloid and 99mTc-sulfur colloid particles. The rhenium colloid product also contains gelatin. Therefore, it was characterized by a slow migration from the injection site as well as a prolonged accumulation in the SNs. The lymph node level shows binding of 3.06% ± 0.10% of the injected dose at the first hour and 3.83% ± 0.16% at the third hour (manufacturer’s information).
Lymphoscintigraphy was performed 1 d before surgery, and the injected doses at the time of scintigraphy were larger than with other radiopharmaceuticals to allow a probe reading 1 d later.
Planar images—including anterior, lateral, posterior, and, occasionally, oblique projections—were obtained within minutes after injection and continued until the SNs were identified, up to 24 h after injection if necessary. Most SNs are detected 1–3 h after injection. The more delayed images also include areas remote from the primary lesion. A 57Co flood source was placed between the patient and the camera to define the body contour. A SPECT/CT emission/transmission study was performed using a hybrid system composed of a dual-head gamma camera with a low-dose x-ray tube installed in its gantry (Discovery VH consisting of a VG8 gamma camera and a Hawkeye x-ray system [General Electric Medical Systems]). This system allows both transmission and emission acquisitions to be performed without changing the patient’s position, and fused images overlying the transmission (CT) and emission (SPECT) data are generated. SPECT acquisition parameters for SN detection include a matrix size of 128 × 128, 180° in the anterior L-mode rotation, and a 3° angle step with a 20- to 25-s time frame. The CT detector consists of 384 crystals and photodiodes mounted on the gantry rotating module. For transmission of data, a “half-scan” acquisition was performed over 220°, 16 s for each transaxial slice. Multiple slices are obtained by moving the table by a slice step before acquiring the next slice. The full field of view consisting of 40 slices is completed in 10 min. Transmission data of the patient are corrected and reconstructed using a filtered backprojection to produce cross-sectional attenuation images in which each pixel represents the attenuation of the imaged tissue. Fusion of the SPECT and CT images is performed on the eNTEGRA workstation (General Electric Medical Systems). On the basis of the scintigraphic findings on both planar and SPECT/CT images, the skin is marked to guide the surgeon to the location of the SNs.
Scintigraphic Interpretation
SN localization was interpreted separately on planar images with and without a 57Co flood source and on fused SPECT/CT images. The location of lymph nodes of the neck was categorized as submental, submandibular, preauricular, jugular chain, occipital, posterior cervical, retroauricular, jugulodigastric, or supraclavicular. Nodes in the axilla nodes were categorized as anterior (pectoral), central, or posterior (prescapular) (20,21).
In the analysis of the results, fused SPECT/CT images data were concluded to be clinically relevant to SNB if it identified SNs that were missed on planar images, if it excluded a SN suspected on planar images, or if it localized the SNs in additional or different basins than those suggested by planar images.
SN Identification at Surgery
The surgeon is notified of the findings on both the planar and SPECT/CT images. The patient is taken to the operating room the next day after lymphoscintigraphy. Skin marking done at the Department of Nuclear Medicine are the first guide to the supposed location of an SN. An intraoperative hand-held probe (Neoprobe 2000; Neoprobe Corp.) is used before incision to identify the site with the highest counts along the lymphatic basin. The direction of incision is chosen, keeping in mind that a lymph node dissection might be indicated. A patent blue dye (2.5% in aqueous solution containing 0.6% sodium chloride and 0.05% disodium hydrogen phosphate; Laboratoire Guerbet) is injected similarly to the earlier colloid injection. Dye is injected immediately before surgery because the dye fades quickly after injection. At this point, a blue duct or even a blue node can direct the probe in identifying the SN and assist in its dissection. After excision of the node, ex vivo counting is performed followed by probing of the lymphatic basin in search of additional nodes with high counts. Dissection is considered complete only after all “hot” nodes have been removed.
RESULTS
SPECT/CT images added clinically relevant data in 4 of 9 patients (44%) with head and neck tumor and in 6 of 12 patients (50%) with trunk melanoma. Fused images added no clinically relevant data in patients with limb melanoma and in the single patient with a penile melanoma. Tables 1 and 2 summarize the scintigraphic and histopathologic findings in patients with tumor in the head and neck region and in patients with cutaneous malignant melanoma in the trunk, respectively.
Scintigraphic and Histopathologic Findings in Patients with Tumor Localized in Head and Neck Region
Scintigraphic and Histopathologic Findings in Patients with Malignant Melanoma of Trunk
SPECT/CT identified multiple draining basins in 6 of 12 patients (50%) with trunk melanoma and in 3 of 9 patients (33%) with head and neck tumor.
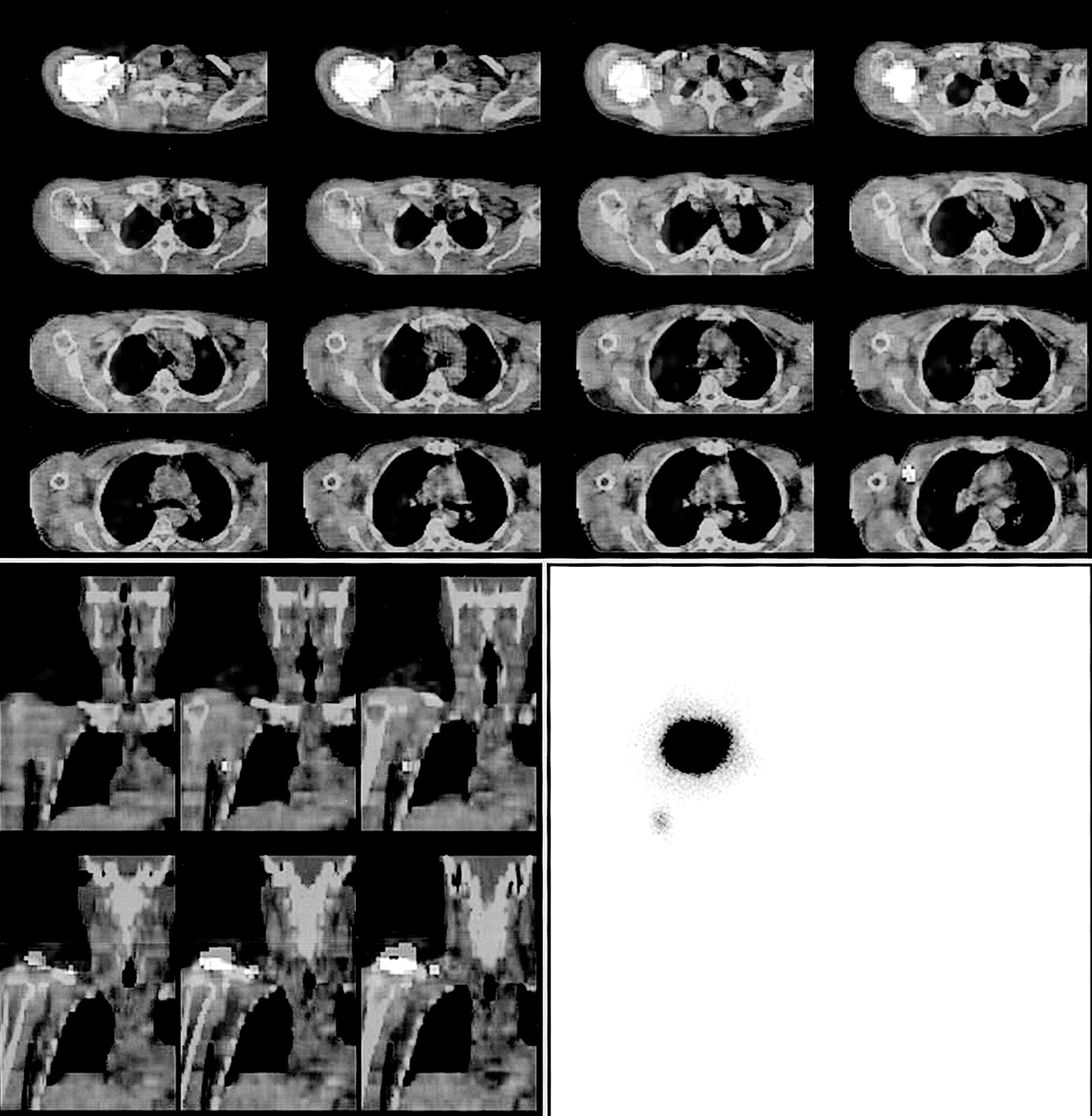
In 9 of the study patients, SPECT/CT fused images identified SNs that were missed on planar images, including 3 nodes that were located close to the injection site and were hidden by its scattered radiation (Fig. 1) and 2 in-transit nodes. The other 4 nodes that had been identified only on fused images were located in basins other than or in addition to the basins identified on planar images (Fig. 2). In 2 patients with head and neck tumor, the SN identified only on fused images was involved with the tumor.
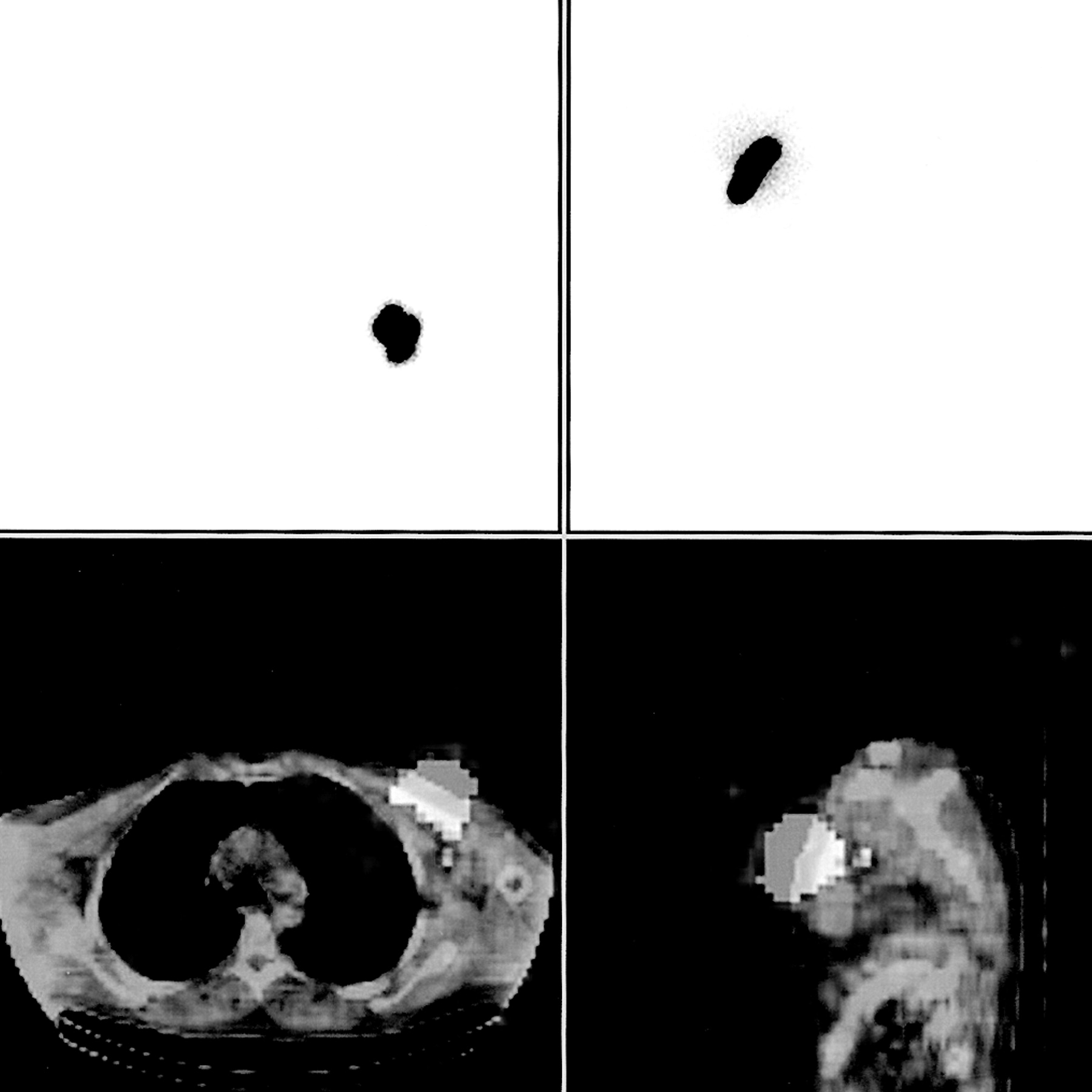
Patient with cutaneous malignant melanoma in chest wall. SN hidden by scattered radiation of injection site. Multiprojection planar lymphoscintigraphy failed to identify SN (top images: selected planar images in anterior and lateral projections). On fused SPECT/CT images, hot node was identified in axilla (bottom images: transaxial and sagittal slices).

Patient with cutaneous malignant melanoma in right upper back. SNs in multiple basins. Multiprojection planar images identified hot node in axilla (bottom right image: anterior projection). Fused SPECT/CT images identified additional supraclavicular and low jugular nodes (top: transaxial slices; bottom left: coronal slices).
DISCUSSION
The SNB technique is used for staging lymph node involvement in patients with melanoma, breast cancer, and mucosal tumors of the head and neck (6–8,22). The results of SNB play an important role in selection of both the appropriate surgical procedure and the nonsurgical adjuvant therapy and are a major prognostic factor. In patients with cutaneous melanoma, in particular, the SN status has been found to be strongly prognostic. Jansen et al. assessed 200 consecutive melanoma patients with a Breslow thickness of at least 1.0 mm and reported a 3-y survival of 93% in negative SN patients compared with 67% in patients with a positive node (23). SNB is of importance in patients with mucosal SCC of the head and neck, particularly at early site disease without clinical or radiologic evidence of metastatic spread. Occult cervical nodal metastases may be present in >20% of the latter patients (24,25). The SNB approach is multidisciplinary, combining 3 complementary modes of SN identification: preoperative scintigraphic SN mapping, use in the operating room of a hand-held gamma probe for guiding the dissection toward the SN, and use of patent blue dye at surgery, which enhances the anatomic configuration of the lymphatic structures giving a clear picture of the lymphatic channels, confirming the location of the SN (26). The aim of all 3 modes of SN identification is to reduce the chance of false-negative biopsies.
Preoperative lymphoscintigraphy provides the road map for the surgeon by defining the drainage basins and the SN localization of an individual tumor site. This preoperative mapping is particularly important if the tumor is located in body regions with ambiguous lymph node drainage, such as the head and neck and the trunk. Lymphatic drainage in the head and neck region is especially complex. There are >350 lymph nodes and a rich lymphatic network as well as a wide variability in the patterns of lymphatic drainage (27). In a study conducted on 30 patients with head and neck melanoma, only 53% of the nodes were found to be both dyed blue and radioactive (10). Determination of the accurate number of draining basins is of major importance. A group of lymph nodes that belong to a single basin must be differentiated from multiple lymph nodes of several basins. In the latter case, each of the nodes may be an SN. Identifying >1 draining basin indicates the need to identify, remove, and examine the SN of each of the basins separately (3).
An effort should be made to accurately define all draining basins before surgery and to localize all SNs. Aberrant SNs outside the recognized lymphatic fields have been reported in up to 21% of the patients. These aberrant SNs may be sites of metastasis (21,28,29). In-transit lymph nodes located between the tumor site and the basin may also be recognized (Fig. 3). These nodes are equally at risk for metastatic disease and are, by definition, SNs.

Patient with melanoma in back. Anterior (bottom left) and lateral (bottom right) planar images detect multiple nodes. Transaxial SPECT/CT images (top) localize nodes in anterior axilla and in aberrant superficial location.
SNs are not necessarily the nodes with the highest intensity uptake. Therefore, it is important to record all detected lymph nodes even if they show a less intense uptake. If only the hottest nodes in each basin had been removed, 13% of the basins with positive lymph nodes would have been missed (16,17).
Previous reports have discussed the methodologic details for optimizing lymphoscintigraphy, recommending acquisition of early images, the use of high-resolution collimation, multiple projections, and the use of markers and transmission images with a 57Co flood source to facilitate anatomic localization (1,3,13–18). Even then, there was a discrepancy between the lymphoscintigraphic and the actual number and location of SNs in 23% of the patients. Lymphoscintigraphy has been found to accurately predict the number of nodes in only 81% of the basins, overlooking nodes that were superimposed and could not be separated from other nodes or from the injection site or lymphatic channels and nodes that were beyond the resolution of the planar images (30). In patients with mucosal SCC or melanoma of the head and neck, the distance between the primary tumor injection site and the lymphatic basin is usually short. This proximity may result in obscuring of the SN by the scatter radiation arising from the injection site (27,30,31).
The better anatomic definition and improved resolution that characterize SPECT images may overcome the above limitations of planar images. Localization of hot lymph nodes on SPECT images without anatomic landmarks is not possible. However, in this study it became possible by fusing the SPECT image with the anatomic data obtained by performing low-dose CT at the same setting as with the SPECT acquisition. SPECT/CT images were found to add data that were clinically relevant in patients with a tumor in the head and neck region and in the trunk. Multiple drainage basins were found in 33% of patients with a head and neck tumor and in 50% of patients with melanoma in the trunk. In patients with melanoma in the extremities, SPECT/CT did not add to planar images. Unpredicted SNs were found, including anterior nodes in patients with cutaneous melanoma in the back and a deep supraclavicular SN in a patient with SCC of the tongue. SPECT/CT clarified the number of draining basins in 4 of 5 patients in whom the accurate number of basins could not be determined on planar images. In 9 patients, SPECT/CT identified nodes that were overlooked by planar images: 3 nodes were obscured by the injection site, 2 were in-transit nodes, and 4 nodes belonged to additional basins or were located in unexpected sites. Two of the nodes detected only by SPECT/CT images were positive on histopathologic examination. Potential explanations for identification of additional nodes by SPECT/CT could have been the effect of time, inadequate planar technique, or improved tomographic imaging technology. Planar images were obtained immediately before or after SPECT acquisition and as long as 24 h after injection. The planar imaging protocol was not altered by the addition of SPECT/CT but, rather, was identical to the multiprojection, multiple time-points protocol that has been used in our institution for many years. It appears, therefore, that the improved lesion detectability of tomographic images and the anatomic landmarks of CT would be the more likely explanation for the additional data provided by SPECT/CT. It should be borne in mind that SPECT/CT is not without disadvantages, as it involves a higher radiation dose because of the addition of CT and requires a longer acquisition time.
CONCLUSION
SPECT/CT SN mapping adds data that are of clinical relevance to SNB in patients with trunk or head and neck melanoma and in patients with mucosal head and neck tumor.
Acknowledgments
We thank Esther Eshkol for editorial assistance.
Footnotes
Received Dec. 10, 2002; revision accepted Apr. 2, 2003.
For correspondence or reprints contact: Einat Even-Sapir, MD, PhD, Department of Nuclear Medicine, Tel-Aviv Sourasky Medical Center, 6 Weizman St., Tel-Aviv, 64239 Israel.
E-mail: evensap{at}tasmc.health.gov.il
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Radioguided Surgery
- 89Zr-Nanocolloidal Albumin-Based PET/CT Lymphoscintigraphy for Sentinel Node Detection in Head and Neck Cancer: Preclinical Results
- Sentinel lymph node biopsy using dynamic lymphoscintigraphy combined with ultrasound-guided fine needle aspiration in penile carcinoma
- SPECT/CT
- Optimal 57Co Flood Source Activity and Acquisition Time for Lymphoscintigraphy Localization Images
- Multimodality Molecular Imaging of Tumor Angiogenesis
- The Additional Value of SPECT/CT in Lymphatic Mapping in Breast Cancer and Melanoma
- Evaluation and Localization of Lymphatic Drainage and Sentinel Lymph Nodes in Patients with Head and Neck Melanomas by Hybrid SPECT/CT Lymphoscintigraphic Imaging
- Improved Sentinel Node Identification by SPECT/CT in Overweight Patients with Breast Cancer
- Procedure Guideline for SPECT/CT Imaging 1.0
- Role of Nuclear Medicine in the Management of Cutaneous Malignant Melanoma
- Fusion of SPECT and Multidetector CT Images for Accurate Localization of Pelvic Sentinel Lymph Nodes in Prostate Cancer Patients