


Abstract
Overweight has been reported as a cause for the nonvisualization of sentinel nodes (SNs) on preoperative planar lymphoscintigraphy in patients with breast cancer. The purpose of this study was to assess whether SPECT/CT may improve SN identification in overweight patients. Methods: Lymphoscintigraphy was performed in 220 consecutive patients with breast cancer. Body mass index (BMI) was calculated for each. A total of 122 patients were overweight or obese (BMI, ≥25). Planar images and SPECT/CT images were interpreted separately, and SN identification on each of the modalities was related to BMI and to findings at surgery. Results: Planar imaging identified SNs in 171 patients (78%) with a BMI (mean ± SD) of 25.2 ± 4 kg/m2 and failed to do so in 49 patients (22%) with a BMI of 28 ± 8 kg/m2. In 29 of the latter patients (59%), SNs were identified on SPECT/CT. SPECT/CT detected “hot” nodes in 200 patients (91%) and failed to do so in 20 patients with a BMI of 29.2 ± 6.6 kg/m2. For the 122 overweight or obese patients, planar assessment failed to identify SNs in 34 patients (28%) and SPECT/CT failed to do so in 13 patients (11%) (P < 0.001). For 116 patients, surgery took place in our hospital (Tel-Aviv Sourasky Medical Center). An intraoperative blue dye technique failed to detect SNs in 48 patients (41%) with a BMI of 28.2 ± 7 kg/m2. SPECT/CT localized hot nodes in 36 (75%) of the latter patients, and planar imaging did so in 22 (46%) of those patients. Of 19 patients for whom scintigraphy failed, 6 (32%) had nodal metastatic involvement. Conclusion: The addition of SPECT/CT to lymphoscintigraphy improved SN identification in overweight patients with breast cancer. Moreover, SPECT/CT accurately identified SNs in 75% of patients for whom the identification of SNs by the intraoperative blue dye technique failed.
Negative axillary sentinel node (SN) biopsy (SNB) offers patients with breast cancer minimally invasive surgery with reduced postsurgery morbidity. The incidence of lymphedema after axillary lymph node (LN) dissection (ALND) ranges between 6% and 30% (1). Overweight is a major risk factor for the development of severe lymphedema after ALND (2). Intraoperative identification of SNs with the blue dye technique has been reported to be less successful in overweight patients (3). Using multivariate analysis, Nos et al. reported that body mass index (BMI) and breast size are the most significant factors affecting the rate of intraoperative SN identification (4). Nonobese patients and patients with small or medium breast sizes show better detection rates than do obese patients with large breast sizes and voluminous or fatty axillae. It is presumed that the decrease in the capacity of nodes to retain blue dye in obese patients is attributable to replacement of the normal nodal tissue by adipose tissue (4). In patients referred for SNB, particularly those for whom intraoperative techniques are suboptimal, the preoperative identification of SNs by lymphoscintigraphy is of clinical relevance. However, an increased BMI is associated with a high rate of failure of lymphoscintigraphic SN identification (5).
We previously reported that the addition of SPECT/CT to planar imaging may improve the preoperative scintigraphic localization of draining nodes. SPECT/CT data allow the detection of “hot” nodes missed by planar imaging, exclude sites of false-positive nonnodal uptake, and accurately localize axillary and extraaxillary hot nodes (6,7).
The purpose of this study was to assess whether the performance of SPECT/CT may improve SN identification in overweight patients with breast cancer. Our hypothesis was that the improved spatial resolution of SPECT and the better image quality achieved with the use of CT data for attenuation correction may improve the diagnostic accuracy of SN mapping in general and specifically in overweight patients.
MATERIALS AND METHODS
Patients
Planar lymphoscintigraphy and SPECT/CT lymphoscintigraphy were performed in 220 consecutive women with invasive breast cancer (T0−T2), with no clinical evidence of axillary LN metastases (N0), and with no remote metastases (M0). Their age (mean ± SD) was 59 ± 12 y (range, 23−83). These patients included 140 women with a palpable mass, 69 women with a nonpalpable mass, and 11 women after lumpectomy.
Patients were interviewed by department nurses, and then height and weight measurements were obtained for BMI calculations. The BMI was calculated as the body weight in kilograms divided by the height in squared meters (kg/m2). Patients with BMI values of 18.4 kg/m2 and lower were considered to be underweight, those with BMI values of 18.5−24.9 kg/m2 were considered to be normal weight, those with BMI values of 25−29.9 kg/m2 were considered to be overweight, and those with BMI values of 30 kg/m2 and over were considered obese. Of the study population, 122 patients were overweight or obese.
Lymphoscintigraphic Techniques
On the day before surgery, a dose of 74 MBq (2 mCi) of 99mTc-rhenium colloid (TCK-17; CIS International), divided into 4 equal portions of 0.7 mL each, was injected. Women with palpable masses were injected at 4 peritumoral sites by a nuclear medicine physician, and patients after lumpectomy were injected at 4 sites along the border of the biopsy cavity. Patients with multifocal lesions or subareolar tumors were injected at 4 periareolar sites. All patients with nonpalpable masses were injected under mammographic guidance. After localization of the tumor and insertion of a Kopans wire (Cook), 1 intratumoral injection of 74 MBq (2 mCi) of 99mTc-rhenium colloid in 3 mL of saline solution was administered adjacent to the wire tip. The rhenium colloid preparation is characterized by a particle size of 50–100 nm and contains gelatin. Therefore, it migrates slowly from the injection site and accumulates in SNs for a prolonged period of time. These characteristics permit a 2-d protocol; the scintigraphic study can be performed on the day before surgery, thus offering flexibility in scheduling surgery and a longer scintigraphic study time (8).
Planar images, including anterior and lateral projections, were obtained immediately after injection for palpable masses and up to 60 min after injection during mammography for nonpalpable masses; imaging was continued until hot nodes were identified, up to 24 h after injection, if necessary. Planar images were obtained both before and after SPECT/CT, simulating the posture of the patient during surgery with the arm elevated to 110°. In the anterior view, the patient was asked to remove the breast from the axillary field of view by using her contralateral hand, whereas in the lateral view, the breast was naturally removed from the axillary region. A 57Co flood source was placed between the patient and the camera to define the body contour.
The SPECT/CT study was performed with a hybrid system composed of a dual-head γ-camera with a low-dose x-ray tube installed in the gantry. For 160 patients, we used a Hawkeye SPECT/CT system (GE Healthcare), which has been used and described in detail in earlier reports (6,7); for the other 60 patients, we used a novel SPECT/CT hybrid system, the Infinia/Hawkeye 4 (GE Healthcare). The latter system incorporates the Infinia dual-head camera with integrated low-dose, 4–5-mm-slice-thickness CT. The CT apparatus has a fixed anode oil-cooled x-ray tube and operates at 140 kV and up to 2.5 mA. The x-ray tube and detector array, located on the slip ring gantry of the γ-camera, rotate together in a fixed geometry at 2.0 rpm for 90° L-mode scans. Multiple slices were obtained in the helical mode; 4 slices were acquired simultaneously with a beam coverage of 2 cm in each gantry rotation and reconstructed online to a 512 × 512 image matrix. CT scans were acquired within 4.5 min. The acquisition time added by SPECT/CT was 10−12 min. The radiation dose added to the breast tissue by the low-dose CT was 1.7 × 10−1 mSv/mA (manufacturer data).
Cross-sectional attenuation images in which each pixel represents the attenuation of the imaged tissue were generated. Fusion of the SPECT and CT images was performed on Xeleris workstations (GE Healthcare). On the basis of the scintigraphic findings from both planar imaging and SPECT/CT, the location of hot nodes was marked on the patient's skin. A compact disc with fused SPECT/CT images in 3 planes was given to the surgeon before surgery.
Scintigraphic Interpretation
The interpretation of lymphoscintigraphy data was performed by 2 nuclear medicine physicians in consensus. Planar images with and without the 57Co flood source and SPECT/CT images were interpreted separately and in a masked fashion. The data for planar assessment included the number of hot nodes detected and whether they were axillary or internal mammary nodes. The locations of hot nodes on fused SPECT/CT images were categorized with the classification used by the surgeon into level I nodes, defined as nodes located lateral to the pectoralis minor muscle; level II nodes, defined as nodes located within the medial and lateral margins of the pectoralis minor muscle; and level III nodes, including nodes located in the axilla medial to the pectoralis minor muscle, interpectoral nodes located between the major and minor pectoralis muscles, intramammary nodes located within the breast tissue, internal mammary nodes, and nodes located in the supraclavicular area (9).
Assessment of Impact of Attenuation Correction on Identification of Hot Nodes by SPECT/CT
To assess the impact of attenuation correction on SN identification by SPECT/CT in an attempt to determine whether detection by SPECT/CT was attributable to the better spatial resolution of SPECT or to the attenuation correction with the CT maps, SPECT images of patients with negative planar study results and positive SPECT/CT study results were reconstructed twice, with and without attenuation correction. Each reconstructed image set was interpreted separately by 2 nuclear medicine physicians, who were unaware of the reconstruction mode.
Correlation of BMI and Lymphoscintigraphic Findings
The impact of BMI on the rate of detection of hot nodes by scintigraphy was assessed separately for planar images and for SPECT/CT images in the general study population as well as in the subgroup of 122 overweight and obese patients.
Correlation of Intraoperative Blue Dye Detection of SNs, Lymphoscintigraphy, BMI, and Histology
A total of 116 of the patients enrolled in this study underwent surgery at our hospital (Tel-Aviv Sourasky Medical Center), enabling access to surgical and pathologic reports.
The identification of SNs by the intraoperative blue dye technique, preoperative planar imaging, and SPECT/CT was evaluated and was related to BMI and to the histologic diagnosis.
Statistical Analysis
The BMI values (mean ± SD) in patients with positive and negative planar imaging or SPECT/CT SN detection results were calculated and compared. SN detection by planar imaging and SN detection by SPECT/CT were compared for the entire patient population as well as for separate BMI groups by use of the McNemar test. A P value of less than 0.05 was considered statistically significant.
RESULTS
Data for General Study Population
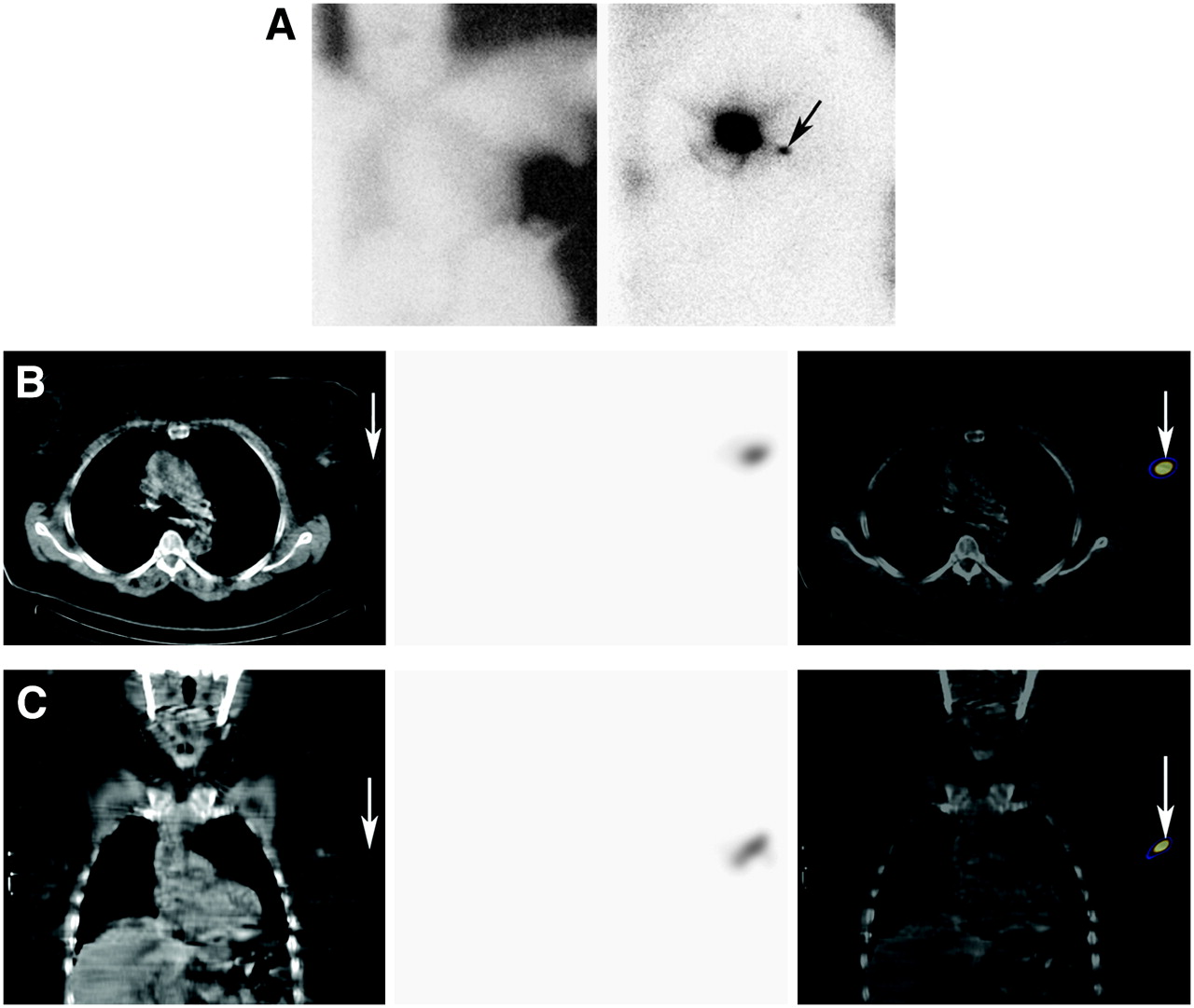
Hot nodes were detected by lymphoscintigraphy in 200 of the 220 study patients (91%). Planar imaging identified 337 hot sites suspected of being hot nodes. A total of 317 sites indeed represented nodal uptake in 171 patients (78% of the study cohort). The remaining 20 foci of uptake interpreted on planar images as hot nodes were found to be sites of false-positive nonnodal uptake when further assessed on SPECT/CT images and validated by surgery. Those sites represented contamination (n = 4), skin folds (n = 3), propagation from the injection site (n = 4), leakage from the wire tract (n = 5) (Fig. 1), sternoclavicular joint uptake (n = 1), and mediastinal uptake in blood vessels (n = 3). Eleven (3.5%) of the 317 hot nodes detected on planar images were masked when a cobalt flood was used to render the body contour.
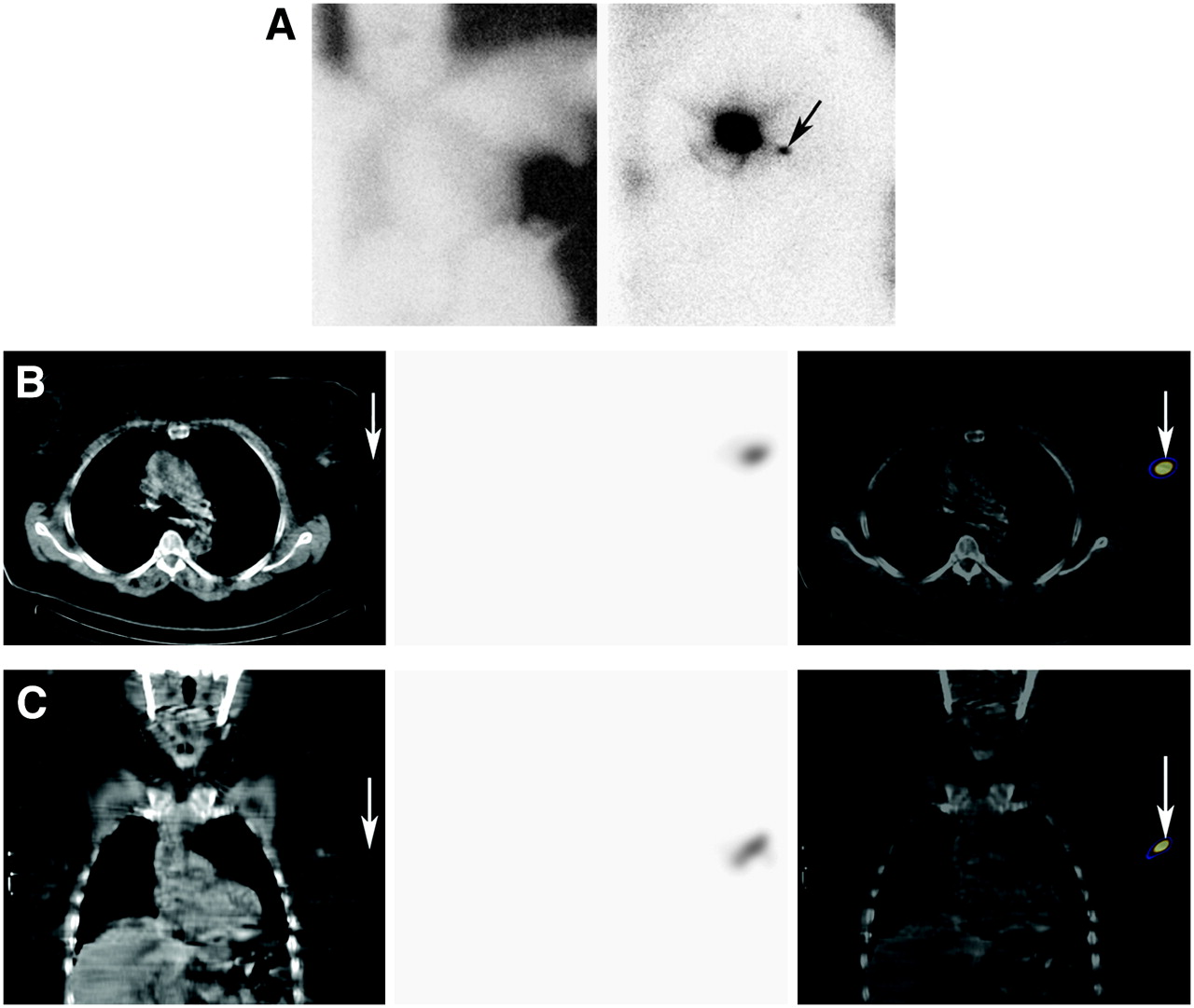
SPECT/CT identification of site of nonnodal uptake misinterpreted as hot node on planar images in 57-y-old obese patient (BMI, 33.2 kg/m2) with nonpalpable mass. Labeled colloid injection was performed after insertion of guide wire during mammography. (A) Anterior and left lateral planar images of chest obtained with 57Co flood. These images were interpreted as identifying hot node in left axilla (arrow). (B and C) Transaxial (B) and coronal (C) SPECT/CT images. CT, SPECT, and fused images are shown from left to right. Hot spot was found to be tip of guide wire and not node (arrows). No other hot nodes were detected, and lymphoscintigraphy results were interpreted as negative. Intraoperative techniques also failed to identify SN, and patient underwent ALND; results of ALND were negative for malignancy.
On SPECT/CT images, 402 hot nodes were detected in 200 patients (91%). In the remaining 20 patients (9%), SPECT/CT results were negative. In 29 of 49 patients with negative planar imaging results (59%), SPECT/CT identified hot nodes. No patients had negative SPECT/CT results and true hot nodes on planar assessment. The 85 hot nodes detected only by SPECT/CT included LNs obscured by the injection site (n = 21), separated adjacent nodes (n = 29), and nodes revealed by the better spatial resolution of SPECT images (n = 35). For the 220 study patients, the rates of SN detection by planar imaging and by SPECT/CT were 78% and 91%, respectively (P < 0.001).
Table 1 summarizes the planar imaging and SPECT/CT results from patient-based and node-based analyses as well as the locations of the SNs determined with assistance from the anatomic landmarks provided by the CT data.
Identification of Hot Nodes by Planar Imaging and SPECT/CT in Patient-Based and Node-Based Analyses
Assessment of Impact of Attenuation Correction on Identification of Hot Nodes by SPECT/CT
To determine whether the better detection of hot nodes by SPECT/CT than by planar imaging was attributable to better lesion detection by SPECT or to the improved image quality achieved with attenuation correction, SPECT images obtained for the 29 patients with positive SPECT and negative planar imaging results were interpreted separately, with and without attenuation correction. Both SPECT and attenuation correction were found to contribute to the better identification of hot nodes by SPECT/CT than by planar imaging (Table 2).
Comparison of Detection of Hot Nodes on Attenuation-Corrected and Non–Attenuation-Corrected SPECT Images Obtained for 29 Patients with Positive SPECT/CT and Negative Planar Imaging Results
Correlation of BMI and Lymphoscintigraphic Findings
The BMI (mean ± SD) of the 220 patients enrolled in this study was 25.2 ± 4.8 kg/m2 (range, 16.6−51.4). Planar imaging detected hot nodes in 171 patients (78%) with a BMI of 25.2 ± 4.0 kg/m2 (range, 16.6−38.6) and failed to do so in 49 patients (22%) with a BMI of 28.8 ± 6.1 kg/m2 (range, 20.3−51.4) (P < 0.001).
SPECT/CT detected hot nodes in 220 patients (91%) with a BMI of 25.7 ± 4.5 kg/m2 (range, 16.6−38.6), including 29 patients (51%) with negative planar imaging results and a BMI of 28.38 ± 6 kg/m2 (range, 20.3−38.3).
In 20 patients, both planar and SPECT/CT results were negative. The BMI of this subgroup was 29.5 ± 6.6 kg/m2 (range, 21.1−51.4).
A total of 122 patients (55.5%) in the study population were found to have BMI values equal to or higher than 25 (mean ± SD, 29.2 ± 4.1 kg/m2; range, 25−51.4). Among this subgroup of overweight and obese patients, planar imaging results were positive in 88 patients (72%) with a BMI of 28.2 ± 3.1 kg/m2 (range, 25−38.6) and negative in 34 patients with a BMI of 31.4 ± 5.2 kg/m2 (range, 25−51.4). SPECT/CT detected hot nodes in 109 overweight and obese patients (89%), including 18 of the 34 obese patients with negative planar imaging results (Fig. 2). The difference between SN detection by planar imaging and SN detection by SPECT/CT in overweight and obese patients was statistically significant (P < 0.001). The correlation of BMI and the detection of lymph nodes by planar imaging and by SPECT/CT is summarized in Table 3. This table illustrates the difference in the detection of hot nodes by planar imaging and the detection of hot nodes by SPECT/CT in patients with different BMI values. The superiority of SPECT/CT appears to be enhanced in overweight and obese patients. Although in planar imaging there is a progressively declining rate of detection as the BMI increases, the rate of detection by SPECT/CT is relatively stable.

Negative planar imaging and positive SPECT/CT identification of hot node in 64-y-old overweight patient (BMI, 29.1 kg/m2). (A) Anterior and left lateral planar images of chest obtained with 57Co flood. Except for uptake at injection site, no hot spot was identified. (B) SPECT/CT transaxial images. CT, SPECT, and fused images are shown from left to right. Hot node was detected at level I of left axilla (arrow), in keeping with SN. Increased uptake detected in left mediastinum appears to be nonnodal uptake in blood vessel.
Correlation of BMI and Detection of Hot Nodes in Patient-Based Analysis
Correlation of Intraoperative Blue Dye Detection of SNs, Lymphoscintigraphy, BMI, and Histology
A total of 116 study patients underwent surgery at our hospital. LNs were detected by the intraoperative blue dye technique in 68 patients (59%) with a BMI of 24.8 ± 4.4 kg/m2 (range, 16.6−34.5), and this technique failed in 48 patients with a BMI of 28.2 ± 7 kg/m2 (range, 19.6−51.4) (P < 0.01). Of the patients for whom the blue dye technique failed, SPECT/CT detected SNs in 36 patients (75%). The correlation of the blue dye technique, planar imaging, and SPECT/CT findings and BMI is summarized in Table 4.
Correlation of Scintigraphic Findings, Intraoperative Blue Dye Detection of SNs, and BMI
Lymphoscintigraphy, both planar and SPECT/CT, failed to identify hot nodes in 20 patients, 19 of whom underwent surgery at our hospital. In 12 patients (63%), intraoperative techniques, which included blue dye and γ-probe assessments, also failed to identify SNs, and ALND was performed. On frozen sections from 5 of the latter patients, the SN was associated with metastatic involvement. Metastasis was found in another patient in whom the SN was detected by γ-probe mapping; for this patient, lymphoscintigraphy and blue dye mapping results were negative. Thus, metastatic involvement of SNs was found in 6 of 19 patients (32%) for whom lymphoscintigraphy results were negative. The correlation of intraoperative mapping and histologic results in patients for whom lymphoscintigraphy results were negative is summarized in Table 5.
Correlation of Intraoperative Mapping and Pathology for 19 Patients for Whom Both Planar Imaging and SPECT/CT Failed
DISCUSSION
The assessment of LN involvement is a major prognostic factor in patients with breast cancer. Thus, early and accurate identification of LN involvement enables adequate therapeutic decisions. Incomplete SN resection may result in inaccurate staging and therapy. SNB is an alternative to axillary dissection as a surgical staging approach for patients with breast cancer, offering a minimally invasive surgical procedure with reduced morbidity. Furthermore, histologic sampling error can be reduced if only a few nodes, rather than a large number of excised nodes, are assessed extensively.
Data on the value of preoperative lymphoscintigraphy for optimizing the SNB procedure are accumulating. During surgery, SN identification is achieved by injection of a blue dye, which makes the lymphatic vessels and the SN visible, and by the identification of the radioactive SN with a hand-held γ-probe (10). Intraoperative failure to identify SNs leads inevitably to ALND, which may be futile. Old age and overweight are reported to be associated with an increased incidence of failed SN identification during surgery. In a study of 1,356 patients, Cox et al. found that an increase of 1 BMI unit decreased the odds of SNB success by approximately 5%n (11). Consequently, patients with high BMI values are more likely to undergo ALND for axillary staging despite the fact that overweight carries a higher risk for postsurgery complications, mainly lymphedema. The identification and accurate localization of SNs in this selective group of patients is of major importance, as lymphedema is the most dreaded, refractory-to-treatment complication of ALND (12).
As indicated by the results of the present study, the addition of SPECT/CT to the acquisition protocol for lymphoscintigraphy may improve the identification of hot nodes in overweight and obese patients. Such improvement is attributable to both the use of SPECT itself and the improved quality of SPECT images gained by use of CT maps for attenuation correction. SPECT data alone are, of course, not interpretable if they are not overlaid on CT anatomic landmarks. SPECT/CT identified hot nodes in 91% of the study cohort, including 29 patients for whom planar imaging failed to detect hot nodes. SPECT/CT detected 85 hot nodes missed by planar images alone, including 14 nodes located in drainage sites, which are not routinely explored during surgery such as intramammary, interpectoral, and supraclavicular regions.
SPECT/CT correctly identified 20 nonnodal hot spots, which were misinterpreted on planar images as SNs. Of note is the uptake at the edge of the wire inserted during mammography in patients with nonpalpable masses. It is valuable to identify the location of such a wire on data from the CT portion of SPECT/CT to avoid false-positive readings (Fig. 1).
The rate of false-negative planar imaging results for 122 overweight and obese patients was 28%, higher than that for the general study population. The rate of false-negative SPECT/CT results for these 122 patients was also higher than that for the general study population, 11%; however, the latter modality identified hot nodes in 18 additional patients (53%) and had a statistically higher rate of detection of hot nodes in overweight patients.
The superiority of SPECT/CT appears to be enhanced in overweight and obese patients. Although in planar imaging there is a progressively declining rate of detection as the BMI increases, the rate of detection by SPECT/CT is relatively stable. The advantage of SPECT/CT was particularly pronounced for 45 obese patients with BMI values of ≥30 kg/m2; SPECT/CT identified hot nodes in 39 of these patients (87%), whereas planar imaging detected hot nodes in only 20 patients (44%).
As previously reported by Nos et al., overweight was associated with a high failure rate for the intraoperative identification of hot nodes in the present study (4). Among 116 patients who underwent surgery at our hospital, the blue dye technique failed to identify draining nodes in 48 patients (41%)—those with higher BMI values. Because SPECT/CT identified hot nodes in 36 (75%) of the latter patients (planar imaging did so in 26 patients), the surgeon actually performed surgery solely on the basis of the scintigraphic findings. In such a clinical scenario, the accurate localization of hot nodes is crucial, and the 3-dimensional data of fused SPECT/CT images have great clinical relevance.
Six of 13 patients (50%) with negative lymphoscintigraphic and intraoperative SN identification had nodal metastatic involvement. It appears that even for overweight patients, in whom the nonvisualization of hot nodes may be a technical limitation, the nonvisualization of SNs by all techniques used for SN identification should raise the possibility of nodal metastatic involvement and should be approached with extreme caution.
CONCLUSION
The addition of SPECT/CT to the acquisition protocol for lymphoscintigraphy in overweight and obese patients with breast cancer improves the identification of hot nodes and avoids false-positive interpretations of sites of nonnodal uptake. It is of a particular value in overweight patients for whom the identification of draining nodes by intraoperative techniques has failed.
Acknowledgments
The authors thank Tamar Geva and Maya Shacham for their contributions to this work.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication August 17, 2006.
- Accepted for publication October 19, 2006.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Sentinel Node Procedure in Breast Cancer: Nuclear Medicine as the Starting Point
- Impact of Obesity on Nuclear Medicine Imaging
- Assessment of Patient Exposure to X-Radiation from SPECT/CT Scanners
- Incremental Value of 131I SPECT/CT in the Management of Patients with Differentiated Thyroid Carcinoma
- SPECT/CT
- Optimal 57Co Flood Source Activity and Acquisition Time for Lymphoscintigraphy Localization Images
- The Additional Value of SPECT/CT in Lymphatic Mapping in Breast Cancer and Melanoma