


Abstract
Axillary node status is a major prognostic factor in early breast cancer. Staging with sentinel node biopsy (SNB) leads to a substantial reduction in surgical morbidity. Recent multiinstitutional studies revealed SNB false-negative rates ranging from 5.5% to 16.7%, higher than the target (<5%) set by the 2005 guidelines of the American Society of Clinical Oncology. These alarming data point to the necessity of optimization. Dual mapping with radiotracer and blue dye, combining 2 different injection sites, and routinely using lymphoscintigraphy may improve accuracy. Factors associated with decreased sensitivity, such as prior excisional biopsy or neoadjuvant chemotherapy, should be recognized. The use of SNB in situations with a high prevalence of node positivity (large tumor, multifocality) is controversial. The risk of missed disease after negative SNB ranges from 1% to 4% in patients with T1 tumor and up to 15% in patients with T3. With peritumoral injection, internal mammary drainage is seen in about 20% of cases. Patients combining internal mammary drainage with a positive axillary sentinel node have close to a 50% probability of internal mammary involvement. Lymphoscintigraphy might thus be helpful in selecting patients for whom internal mammary radiation has a high benefit-to-risk ratio.
- sentinel node biopsy
- breast cancer
- micrometastases
- lymphoscintigraphy
- internal mammary node
- radiation therapy
- neoadjuvant chemotherapy
Breast cancer is the most common class of cancer diagnosed in women worldwide. Estimates for 2010 in the United States were 209,060 new cases of invasive breast cancer and 40,203 deaths (1). Axillary node status is a major prognostic factor in early-stage disease, and this information is important for tailoring of treatment (2,3).
Because imaging techniques have limited sensitivity, the axilla must be explored surgically. Traditional staging requires levels I and II axillary lymph node dissection (ALND) with 10 or more removed nodes (3). Axillary involvement is found in 10%–30% of patients with T1 (≤2 cm) tumors, depending on size. This rate reaches 45% for small T2 tumors (2.1–3 cm) and 55%–70% for larger tumors (2,4). However, routine ALND carries the risk of lymphedema, sensory disturbances, and chronic pain.
Sentinel node biopsy (SNB) is a less invasive method of checking for nodal involvement (5). SNB is based on the assumption of an orderly progression of lymph node invasion by malignant cells from a tumor site. The implication is that the entire basin is free of involvement if the first relay node is uninvolved (6). Patients with metastasis to a sentinel node would undergo either immediate or delayed completion ALND.
On a size basis, a metastasis in a sentinel node is designated a macrometastasis when larger than 2 mm, a micrometastasis (pN1mi) when larger than 0.2 mm but no more than 2 mm, and isolated tumor cell clusters (pN0i+) when 0.2 mm or smaller and having no more than 200 tumor cells in a single cross section. This terminology stands whatever the detection method, whether classic staining or immunohistochemistry (7).
The SNB procedure uses a radiotracer, a blue dye, or both (8,9). Radiopharmaceuticals for SNB are colloids labeled with 99mTc (10–12). They enter the lymphatic system and are engulfed by histiomonocytic cells of the sentinel node. They allow sentinel node visualization with a γ-camera before surgery and intraoperative detection with a hand-held γ-ray probe. Individual sentinel nodes take up about 1% of the locally injected activity. Dyes bind weakly to interstitial proteins, mostly albumin, and cause the blue coloring as they pass slowly through the sentinel node. Despite a risk of allergic reactions to blue dye, most teams favor the dual-mapping procedure (8,9).
Which women can be offered SNB is a highly debated issue. Some centers use SNB only in patients with a unifocal tumor smaller than 2–3 cm, whereas others have extended the application to patients with large T2 or T3 (>5 cm) tumors or multiple ipsilateral carcinomas (multifocal/multicentric) or to patients who have received neoadjuvant chemotherapy.
Here, we present a critical analysis of SNB in breast cancer in light of recent data that have been published mostly in the last 5 years.
SNB STRATEGY AND SURGICAL MORBIDITY
Randomized trials in which the primary aim was assessment of morbidity conclusively demonstrated a marked diminution of complications associated with the SNB strategy, when compared with routine ALND (13,14). In the ALMANAC trial, 1,031 patients were randomized to undergo either ALND or SNB. Twelve months after surgery, the risk of lymphedema was 13% in the ALND group and 5% in the SNB group. The risk of sensory loss was, respectively, 31% and 11%. Overall, patient-recorded scores for quality of life and arm functioning were significantly better in the SNB group (14). No specific analysis was performed, however, to see whether the morbidity advantage also applies to the small subset of patients with T2 tumor, in whom the risk of completion ALND is higher.
LOCOREGIONAL RECURRENCE AND SURVIVAL
Few randomized trials have investigated the impact of SNB strategy on recurrence and survival (15–17). All these trials compared SNB to SNB + ALND but not SNB to ALND.
The single-institution trial from Milano included 516 patients with tumors no larger than 2 cm. The mean follow-up was 95 mo (15). The axillary relapse rate among patients with a negative sentinel node in the SNB group was as low as 1.2% (2/167). Interestingly, a rate of 4.6% would have been expected from the findings for the group SNB + routine ALND. The authors suggest that many small metastases might stay dormant if devoid of cancer stem cells. Although these data are fully reassuring, the wide exclusion criteria adopted might limit the generalization of these conclusions. The authors excluded patients with tumors that were larger than 2 cm or multicentric, patients with prior excisional biopsy or younger than 40 y, and patients for whom a sentinel node was not found at lymphoscintigraphy or on preoperative probe-guided inspection. Patients were also excluded after surgery if final pathologic examination revealed a tumor that was larger than 2 cm or multifocal (15).
The Sentinella/GIVOM trial (Gruppo Interdisciplinare Veneto di Oncologia Mammaria) included 749 women with a palpable tumor no larger than 3 cm. During a median follow-up of 55.6 mo, locoregional recurrence occurred in 16 patients in the SNB group versus 3 in the ALND group. The 5-y relapse-free survival rate was slightly but not significantly lower in the SNB group (87.6% vs. 89.9%). The number of enrolled patients was deemed not sufficient to draw conclusions (16).
The National Surgical Adjuvant Breast and Bowel Project trial B-32 (NSABP B-32) randomized 5,611 women to SNB versus SNB + ALND. The primary endpoint was comparing overall survival in patients with a negative sentinel node in both arms (17). Tumor size was 2 cm or less in 83.8%, 2.1–4 cm in 14.7%, and more than 4 cm in 1.5% of sentinel node–negative patients. During a mean follow-up of 95.6 mo, 169 of 2,011 sentinel node–negative patients in the SNB group and 140 of 1,975 in the SNB + ALND group died (hazard ratio, 1.2 by log-rank comparison; 95% confidence interval, 0.96–1.5; P = 0.12). The 8-y overall survival rate was 90.3% in the SNB arm versus 91.8% in the ALND arm. Follow-up is continuing for longer-term assessment (17).
In total, data from patients with unifocal T1 tumor are fully reassuring, but it still seems premature to draw conclusions on other situations. Specific data from patients with T2 and T3 tumors would clearly be helpful.
ALARMING RESULTS CONCERNING FALSE-NEGATIVE RATE
In 2005, guidelines from the American Society of Clinical Oncology (ASCO) stressed that a multidisciplinary team should aim at a sentinel node identification rate of 85% with a false-negative rate of 5% or less in order to abandon axillary dissection (8). Identification rate is the proportion of patients in whom at least 1 sentinel node is found at operation. False-negative rate is the proportion of axillary node dissection–positive cases with a negative sentinel node at biopsy. Some false-negatives may result from massive involvement of the first relay node, a circumstance that interferes with the uptake of both radiocolloid and dye and diverts lymph flow to a node other than the true sentinel node (6). The false-negative rate is the safety parameter of the SNB procedure (8). However, once SNB has been adopted, the false-negative rate is no longer measurable in clinical practice.
A metaanalysis of 69 early trials with a total of 8,059 patients in whom SNB was systematically followed by axillary dissection showed substantial variability in SNB performance (18). A high identification rate was associated with a low false-negative rate (18). On the basis of this metaanalysis, ASCO experts stated that “The strongest predictor of the false-negative rate across trials appears to be the proportion of patients for whom mapping is successful.” Identification rate may thus “serve as a reasonable quality indicator for the SNB procedure” (8).
However, recent results from large multiinstitutional trials (16,19–21) showed that all have achieved excellent identification rates, ranging from 93.5% to 97.2%, but that none achieved a false-negative rate lower than 5% (Table 1). The false-negative rate was 9.8% in the NSABP B-32 trial (21) and was dramatically high (16.7%) in the Sentinella/GIVOM (16). Identification rate may thus provide false reassurance about the quality of the SNB procedure.
SNB False-Negative Rates: Results of Large Multiinstitutional Trials
The false-negative rates ranged from 5.5% to 16.7%, with a weighted average of 9.2%. The lowest false-negative rates were obtained in the 2 studies in which preoperative lymphoscintigraphy and dual mapping during surgery were required (Table 1). Direct comparison of protocols between different studies is, however, not possible since they refer to different surgeons and different settings.
False-negative SNB results might impair patient outcome for several reasons: missed nodes might lead to axillary recurrence that is difficult to treat, tumoral axillary nodes are a potential source of distant metastases, and understaging affects decisions about systemic therapy and specific radiation therapy to the chest wall and nodal basins (3,22).
OPTIMIZATION OF SNB PROCEDURE
Impact of Prior Excisional Biopsy on False-Negative Rate
Surgical biopsy can change the pattern of lymphatic drainage. In the NSABP B-32 trial (21), previous excisional biopsy did not affect sentinel node identification but was, however, associated with almost a doubling of false-negative rate compared with percutaneous biopsy (15.3% [27/177] vs. 8.1% [48/589]; P = 0.0082).
Importance of Dual Mapping
In the Axillary Lymphatic Mapping Against Nodal Axillary Clearance (ALMANAC) validation study, the false-negative rate was 6.7%. However, if only blue sentinel nodes are considered, the false-negative rate was 9.1%. Likewise, the false-negative rate would have been 10.9% based on isotope alone (20). In the Sentinella/GIVOM trial (16), blue dye was not used and the false-negative rate was higher than in the other trials (Table 1).
Isosulfan blue is in greater use in the United States, and patent blue V, in Europe (23). Data from NSABP B-32 and American College of Surgeons Oncology Group trial Z0010 (ACOSOG-Z0010) with isosulfan, and from ALMANAC with patent blue V, showed that the overall risk of allergic reaction is close to 1% for both dyes, with an approximately 0.1% risk of severe reactions (grade III).
Mariani et al. suggested that 99mTc-labeled colloids with most of the particles in the 100- to 200-nm size range would be ideal for SNB in breast cancer (10). The choice of tracer is often guided by local availability (23). 99mTc-labeled colloids of human serum albumin are often used in Europe. Among sulfur preparations, 99mTc-sulfur colloid is used in the United States (sometimes after filtration through a 0.1- or 0.2-μm membrane); 99mTc-rhenium sulfide colloid, in Europe; and 99mTc-antimony trisulfide, in Australia. Because the clearing capacity of the macrophages in the sentinel node is limited, a high specific activity can improve sentinel node detection (10). There is no established difference between a 1-d protocol (same-day imaging and surgery) and a 2-d protocol. Injected activity needs to be adapted.
Resection of All Hot or Blue Nodes
Differentiating a true sentinel node from a secondary echelon node is difficult. Also, lymphatics of a tumor site can drain simultaneously to more than 1 sentinel node.
Both the NSABP-B32 trial and the ALMANAC validation study showed the influence of the number of resected nodes on the false-negative rate (20,21). In NSABP B-32, the false-negative rates was 17.7% if only 1 node was resected, 10% if 2, 6.9% if 3, 5.5% if 4, and 1% if 5 or more (21). These results should not translate into routine removal of multiple nodes for an optimal SNB procedure, as this may have a detrimental impact on morbidity. However, all identified hot or blue nodes should be resected. Careful palpation by the surgeon of the operative field is also required to identify any suggestive large, hard nonblue and nonradioactive nodes.
Effect of a Different Injection Site for Radiotracer and Blue Dye on False-Negative Rate
In most early SNB studies, the tracer was injected around the tumor (5). Because the tracer is injected near the same lymph vessels that drain the tumor, such peritumoral injection is considered the gold standard against which all other mapping techniques are tested. Many investigators have reported good results using injection into the breast skin over the tumor, or using a periareolar or subareolar injection (24,25). These approaches exploit the common embryologic origin of the mammary gland and overlying skin and the description by Sappey in the 19th century that breast lymphatics collect in a subareolar plexus before draining to the axilla.
The only clearly established advantage of peritumoral injection is its ability to also reveal extraaxillary drainage. On the other hand, superficial injection techniques entail a faster lymphatic drainage, yield more radioactive counts at the axillary sentinel nodes, and are independent of the palpable or nonpalpable nature of the tumor (25).
In the prospective multiinstitutional randomized French study FRANSENODE, sentinel node identification rate with the γ-probe was 96% after peritumoral injection and 98.2% after periareolar injection (P = 0.16; not statistically significant). When detection by γ-probe plus blue dye was considered, the sentinel node detection rate reached 99.1%, with no difference between peritumoral injection of the 2 tracers and periareolar injections (25). Because ALND was not performed, the impact of injection technique on the false-negative rate is unknown.
Lymphatic drainage of the breast is not completely understood (26). Rather than defending a particular injection site, it might be helpful not to use the same injection site for the radiotracer and blue dye to further enhance the complementary information obtained by combining 2 tracers (9). Anan et al. used 2 dyes: blue dye into the subareolar area and green dye peritumorally. The false-negative rate was 4.9%. However, the false-negative rate was twice higher (10%) if only blue nodes or only green nodes were considered (27). Thus, it might be appropriate to use 2 different injection sites; for example, peritumoral for the radiotracer and subareolar for blue dye (9,28). Peritumoral injection of the radiotracer can evidence extraaxillary drainage (9).
Improvement of SNB Procedure Through Lymphoscintigraphy
By providing the surgeon with a map of sentinel nodes, scintigraphy has the potential to both improve accuracy and reduce morbidity relative to γ-probing alone (10–12,29–32).
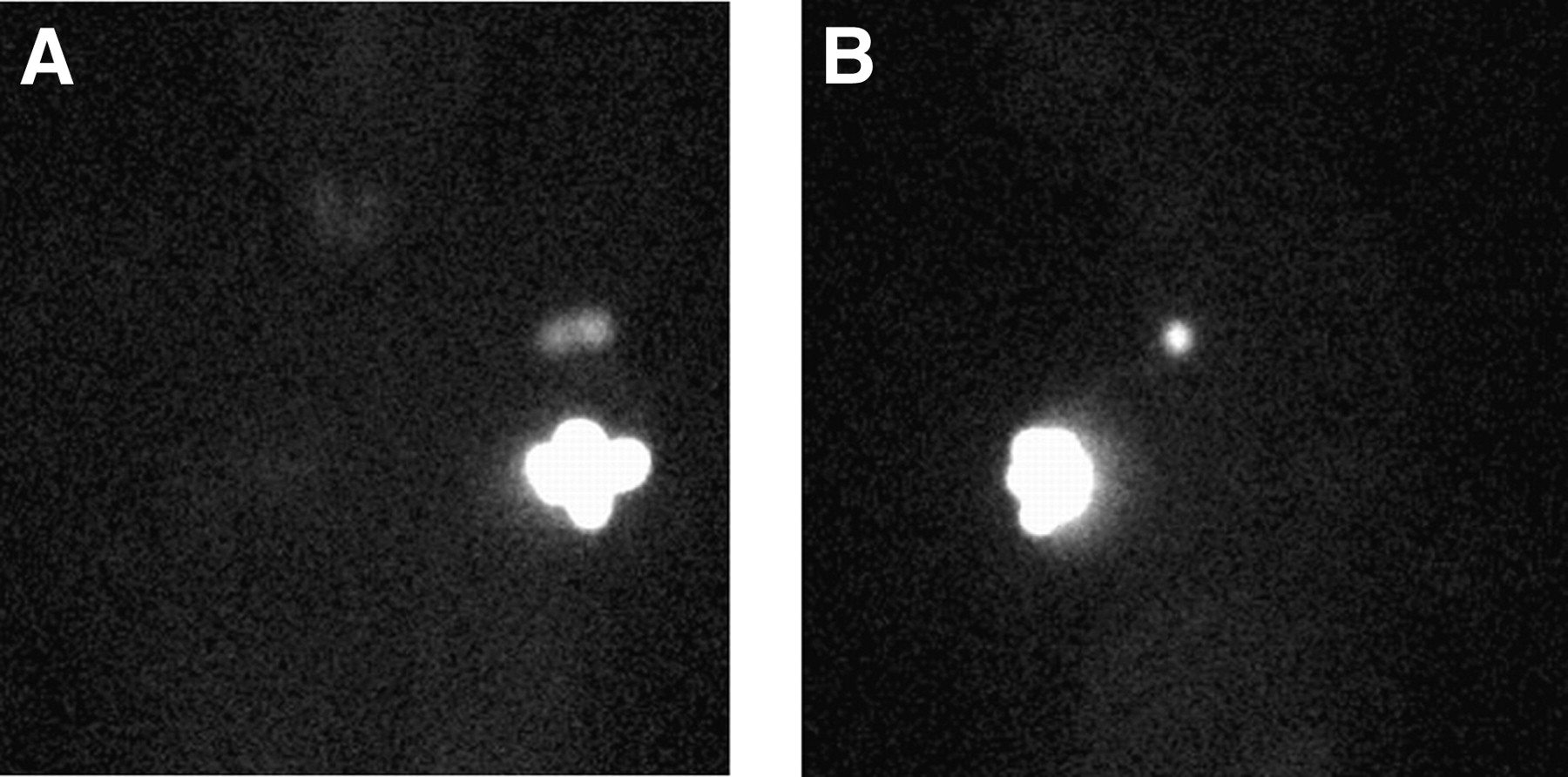
To identify all sentinel nodes and avoid confusion with a stasis in a lymphatic vessel, images are acquired with an adequate delay after injection. This delay may vary with the radiopharmaceutical, injection site, and patient characteristics. Lymphatic drainage can be slower in old or overweight patients. With planar scintigraphy, combining 2 views may help prevent some sentinel nodes from being missed (Fig. 1).
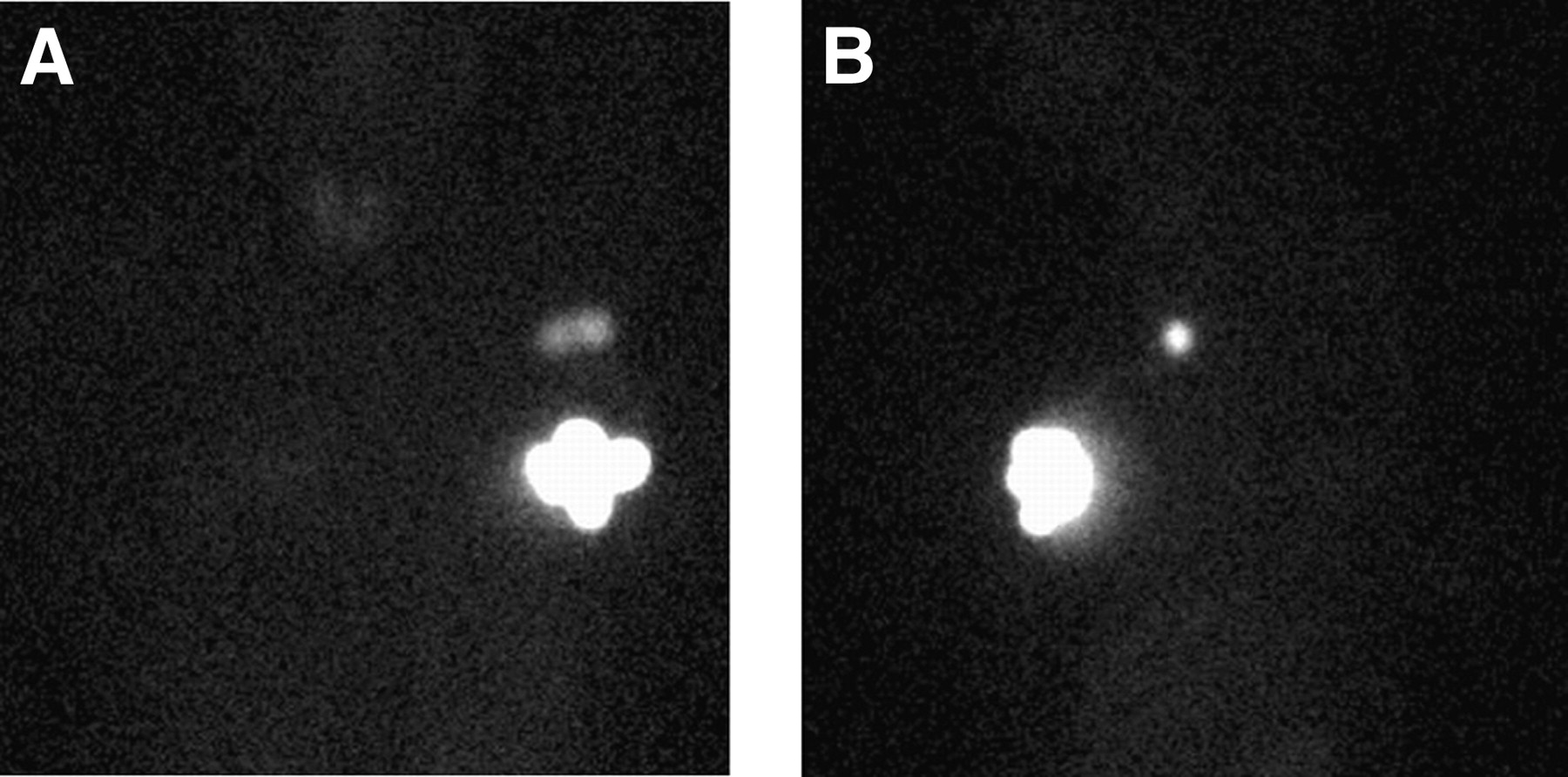
Lymphoscintigraphy of patient with nonpalpable left breast cancer 2 h after periareolar injection of 99mTc-colloidal rhenium sulfide, with the 2 detectors positioned at right angles. (A) Anterior view shows 2 axillary sentinel nodes. (B) On left lateral view, only 1 axillary focus is seen; the 2 sentinel nodes are superimposed.
Lymphoscintigraphy identifies atypical drainage patterns. Drainage to the internal mammary basin occurs in 20% of patients after peritumoral injection (8). Other unusually located sentinel nodes are also seen in a nonnegligible percentage of patients: intramammary (prepectoral) in 6%, interpectoral (Rotter's node) in 2%, and infraclavicular (axilla level III) in 3% (30).
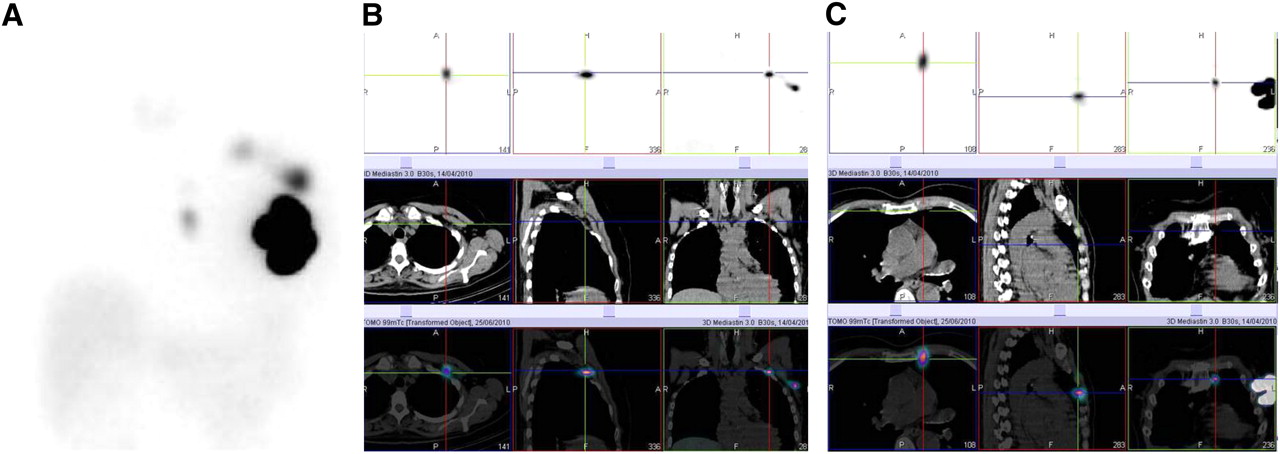
The advent of SPECT/CT reinforces the potential of preoperative scintigraphy (33–35). Low-dose CT is sufficient to pinpoint atypically located sentinel nodes (Fig. 2). SPECT/CT can also detect hot nodes missed by planar imaging because of shine-through from the injection site or in overweight patients (33,34). Thus, SPECT/CT can be useful when planar imaging is negative or ambiguous or shows unexpected drainage.
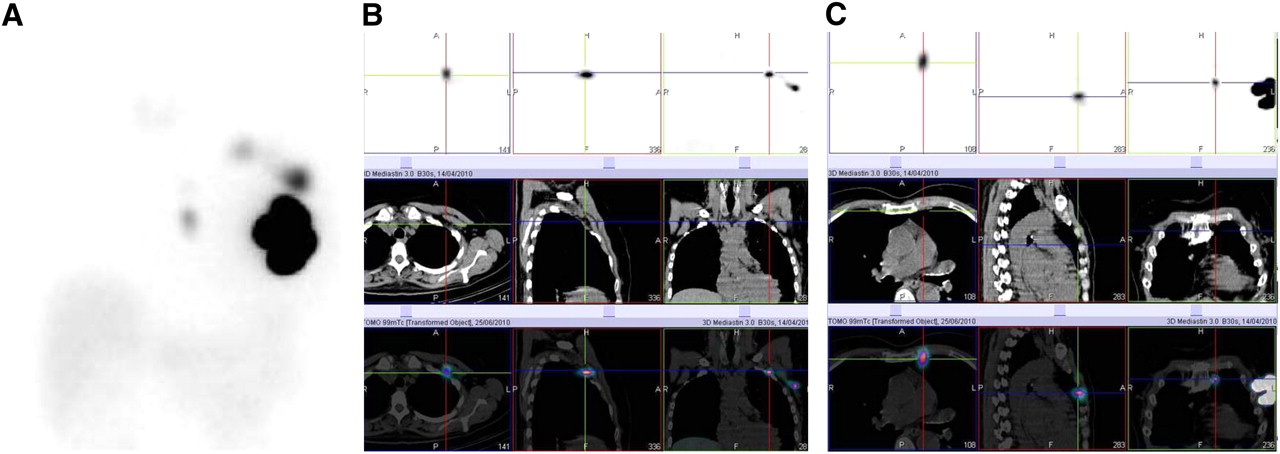
Lymphoscintigraphy of patient with 25-mm invasive lobular carcinoma of left breast. (A) Anterior planar view shows 2 axillary sentinel nodes plus internal mammary drainage. Medium-energy collimator was used to reduce star artifacts. (B) SPECT, CT, and SPECT/CT fusion images of axilla show upper sentinel node at Berg level II (beneath pectoralis minor) and other sentinel node at Berg level I. (C) Internal mammary node is in second intercostal space and did not undergo biopsy. Axillary sentinel nodes were negative.
Failure to visualize a sentinel node is predictive of difficult intervention (31). Negative scintigraphy also heralds a higher risk of axillary involvement (32,35). In a study by Brenot-Rossi et al, node invasion was found in 28.5% of patients with a visualized sentinel node versus 63.3% in cases of negative scintigraphy (32). In cases of nonvisualization after peritumoral injection, some authors reinject superficially. However, sentinel nodes that appeared with rescue injection were associated with a high (24%) false-negative rate (36). Thus, when scintigraphy is negative after an adequate delay, one should check for the presence of macrometastases by ultrasound before surgery. When no sentinel node is identified at surgery, ALND should be performed (3,8).
SNB IN PATIENTS AT HIGH RISK OF NODAL INVOLVEMENT
SNB in Various Categories of Tumor Size
In the ALMANAC validation study, the false-negative rate was 7.7% for patients with T2 tumors, not significantly different from that (5.2%) for T1 tumors (20). Higher tumor grade was, however, associated with higher false-negative rate (0% in grade 1, 4.7% in grade 2, and 9.6% in grade 3 tumors; P = 0.022). In the NSABP B-32 study (21), the false-negative rate was 8.9% for patients with tumors 2.1–4 cm and 10.3% for T1 tumors.
However, even assuming a constant false-negative rate, the negative predictive value decreases when the prevalence of lymph-node positivity in a population increases. A larger fraction of those patients with negative SNB results will harbor axillary disease.
Using technical data from the ALMANAC validation study (20) and from the group SNB + ALND of the NSABP B-32 trial (21), we assessed the risks of completion ALND and the risks of missed involvement. Our estimates based on ALMANAC data show that the need for completion ALND due to a positive sentinel node is almost twice higher for patients with T2 tumors (2.1–5 cm) than for patients with T1 tumors (51% vs. 28%). The risk of missed axillary disease after a negative SNB is 4 times higher (9.3% vs. 2.2%) (Table 2). In the NSABP B-32, the tumor size category (2.1–4 cm) would correspond to small-to-medium T2 tumors. When the SNB procedure is applied to these patients, the need for completion ALND would be 41% (vs. 24% for T1); the risk of residual disease after negative SNB is also higher (6.2% vs. 3.2%) (Table 2).
Risk of Completion ALND and Risk of Missed Axillary Disease After Negative Sentinel Node in Different Clinical Settings
There were too few patients with a T3 tumor in the ALMANAC, or a tumor larger than 4 cm in the NSABP B-32, to allow any conclusion to be drawn.
Taking into account node-positivity prevalence by tumor size category (2,4) and assuming a false-negative rate of 10% (as found in the NSABP B-32), simple theoretic calculations would show that the risk of completion ALND increases progressively from 10% to 30% in patients with T1, to reach 60% in unselected patients with T3 tumor. Also, the risk of missed axillary disease after negative SNB would progressively increase from 1% to 4% in patients with T1 tumor, depending on tumor size, to about 15% in patients with T3 tumor.
SNB in Patients with Multiple Simultaneous Ipsilateral Carcinomas
In the ALMANAC validation study, the false-negative rate of SNB in 75 patients with multifocal tumors was 8.8% (20). In the prospective multiinstitutional French study IGASSU, with 211 evaluable patients in whom multifocality was diagnosed before SNB and breast surgery, the false-negative rate was 13.6% (37).
Pooled data from these 2 studies show that the risk of completion ALND is close to 50% and the estimated risk of missed axillary involvement after a negative SNB is 7.5%–12.9% (Table 2).
SNB After Neoadjuvant Chemotherapy
Patients with tumors larger than 3 cm are often offered neoadjuvant chemotherapy to increase the probability of breast-conserving surgery. Performing SNB after neoadjuvant chemotherapy is a highly controversial topic (3,8,38). Chemotherapy may increase the chance of false-negative findings due to lymphatic changes, fibrosis, and patchy killing (6,8,38). SNB before neoadjuvant chemotherapy is more accurate (39) but means separate surgery and a possible delay in the start of chemotherapy.
A French study, “Ganglion Sentinelle et Chimiothérapie Néoadjuvante,” prospectively assessed the accuracy of SNB after neoadjuvant chemotherapy (40). A sentinel node was identified in 90% of patients. The false-negative rate was 11.5%. The data led to an estimate of missed axillary disease after negative SNB of 4.6% (Table 2). This risk cannot be neglected, as it occurs in patients who already received chemotherapy and might not receive adequate radiation because of false-negative SNB results.
The position of the National Comprehensive Cancer Network is to perform SNB before neoadjuvant chemotherapy and to base decisions about ALND and adjuvant treatment on the node status before chemotherapy (3).
Safety Measures in Patients with High Probability of Axillary Involvement
Ultrasound, coupled with fine-needle biopsy of suggestive nodes, can spare some patients with macrometastases an unnecessary SNB and the risk of false-negative results (41). Baruah et al. reported a sensitivity of 28.5% (39/137 node-positive patients were identified) and a specificity of 100% (41).
In a study by Heusner et al., the sensitivity of 18F-FDG-PET/CT (with contrast-enhanced CT) was 58%. The positive predictive value was 82% (42). It would be difficult to justify the use of this technique solely for patient selection before SNB. However, baseline 18F-FDG-PET/CT in patients with large tumors might influence management by identifying distant metastases or extraaxillary nodes (43). 18F-FDG-PET/CT is also being investigated as a tool for early assessment of response to neoadjuvant chemotherapy (44).
Practices concerning intraoperative pathologic assessment of sentinel nodes vary (14,16,19–21). However, intraoperative assessment would seem desirable when the prior probability of nodal involvement is high. Recall for completion ALND causes distress to patients, exposes them to the risks of a second anesthesia and operation, and increases total hospital stay. In the Sentinella/GIVOM trial, frozen-section examination offered a sensitivity of 75.3% (16). Imprint or touch-preparation cytology is less time-consuming but requires experience in cytology reading. In the NSAPB B-32 trial, intraoperative cytology had 61.4% sensitivity and 99.5% specificity (21).
Intraoperative molecular techniques have also been developed. One assay analyzes fresh homogenized tissue from sentinel nodes using reverse transcription–polymerase chain reaction to detect cytokeratin-19 and mammaglobin messenger RNAs and is calibrated to detect sentinel node metastases larger than 0.2 mm (45). In 1 study, sensitivity was 87.6%, specificity 94.2%, and positive predictive value 86.2% (45). Because specificity is still suboptimal, molecular tests might be better adapted to a population with a high probability of axillary involvement. Also, because alternate tissue slices analyzed with the assay are lost for postoperative histology, there is a potential risk of loss of information on small metastases.
INTERNAL MAMMARY DRAINAGE: POTENTIAL IMPACT ON DECISIONS ABOUT RADIOTHERAPY
In the last few years, there has been renewed interest in internal mammary treatment (46). A metaanalysis showed that postmastectomy radiotherapy to chest wall and nodal basins (including internal mammary) improves the survival of axilla-positive patients (22). Internal mammary radiation techniques have also improved, and cardiovascular side effects are less common (22,46). However, internal mammary radiation remains controversial, mainly because of the difficulty of selecting patients at risk of occult internal mammary involvement (46). Difficulty in establishing guidelines was acknowledged by the National Comprehensive Cancer Network Panel (3). In some institutions, patients are selected on the basis of tumor location (medial/central), as is the case for the European Organisation for Research and Treatment of Cancer trial 22922 (EORTC 22922) assessing the impact of internal mammary radiation on survival.
Lymphoscintigraphy is an objective means of identifying cases of drainage to the internal mammary basin and thus with an anatomic substratum for occult internal mammary invasion.
Probability of Internal Mammary Involvement in Patients with Internal Mammary Drainage According to Axilla Sentinel Node Status
We reviewed studies in which internal mammary nodes identified on lymphoscintigraphy underwent biopsy. We selected 6 studies that fulfilled the following criteria: a large number of patients, peritumoral or intratumoral tracer injection, internal mammary biopsy successfully achieved in most patients with internal mammary drainage, and axilla staged routinely independent of internal mammary status (47–52).
These studies included a total of 3,876 patients (Table 3). Internal mammary drainage was present in 20.4%. When internal mammary biopsy could be performed, it was positive in 17.2% of patients. A major difference was found according to axillary sentinel node status. In patients with a negative axilla, internal mammary biopsy was positive in 7.8%, whereas in patients with positive axilla, internal mammary biopsy was positive in 41% (Table 3). Because it is difficult to perform multiple biopsies on patients with multiple internal mammary hot nodes, the true rate of invasion should be even higher, close to 50%. This high risk of occult internal mammary involvement in cases of a positive axillary sentinel node and internal mammary drainage suggests that these patients can be offered internal mammary radiotherapy with no need for internal mammary biopsy.
Internal Mammary Visualization Rate and Biopsy Results: Data from 6 Prospective Studies
Patients with Internal Mammary Drainage and Negative Axillary Sentinel Node
Internal mammary biopsy may identify a few candidates for internal mammary radiation (Table 3). However, internal mammary biopsy is linked to a small percentage of complications (due to the proximity of internal mammary vessels and pleura), which makes the procedure controversial.
In a patient with a small tumor, finding internal mammary invasion would also lead to chemotherapy. In the 2 studies that included only tumors smaller than 2–3 cm (48,52), internal mammary positivity in cases of internal mammary drainage and a negative axillary sentinel node was 5% (Table 3).
SNB AND SOME CONTROVERSIAL ISSUES
Prognostic Significance of Micrometastases and Isolated Tumor Cell Clusters
The advent of SNB resulted in upstaging of approximately 10% of breast cancer patients, an increase mainly due to micrometastases (53).
Some retrospective studies found that patients with micrometastases pN1mi or with isolated tumor cell clusters pN0(i+) do not have worse disease-free survival than do sentinel node-negative patients (54). It was also found that completion ALND was associated with improved outcome in cases of sentinel node macrometastases (>2 mm) but not in cases of microscopic involvement (55). Bleiweiss suggested that some “tumor deposits” detected solely by anticytokeratin immunostaining could be benign epithelial cells transported to the sentinel node after breast biopsy (6).
Other retrospective studies found microscopic nodal disease that was clinically relevant (56–58). At completion ALND, Cox et al. found additional invasion in 15.5% of women with sentinel node micrometastasis. Survival was shorter in patients with micrometastases than in node-negative patients (56). Tan et al. reexamined paraffin blocks from 368 patients who underwent surgery long before and whose ALND was negative. The review procedure, with a technique similar to that used for sentinel nodes, revealed occult metastases in 83 patients (23%). Death by cancer was significantly more frequent in these patients (57). De Boer used The Netherlands Cancer Registry to compare outcomes. After adjustment for other prognostic factors, the hazard ratio for disease events was 1.56 for patients with micrometastases and no systemic therapy, as compared with node-negative patients. The hazard ratio was 1.5 in cases of isolated tumor cell clusters (58). Outcome was improved with adjuvant therapy. For patients with micrometastases, 5-y disease-free survivals were 87.9% and 75.9%, respectively, with and without systemic therapy (P < 0.001) (58). The prognostic relevance of microscopic nodal disease is thus an area of continuing controversy. Results of prospective trials (ACOSOG-Z0010, NSABP B-32, and International Breast Cancer Study Group trial 23-01 [IBCSG 23-01]) are eagerly awaited.
In the new edition of the AJCC Cancer Staging Manual (7), stage I breast cancer has been divided into stage IA and stage IB. Stage IB includes patients with a T1 tumor with only micrometastases (N1mi). These patients are thus excluded from stage IIA.
Alternatives to Routine ALND in Patients with Positive Sentinel Node
AMAROS is a trial of completion ALND versus axillary radiotherapy in patients with a positive sentinel node. IBCSG 23-01 is a trial of ALND versus no ALND for patients with sentinel node micrometastases. Until results are available, the current recommendations are to perform ALND in patients with a positive sentinel node (3).
The risk of additional node involvement depends on such factors as the number of positive and total sentinel nodes, size of sentinel node metastases, size of primary tumor, nuclear grade, and presence of lymphovascular invasion. Several models have thus been developed to help predict additional involvement (59). Some aim more specifically at patients with sentinel node micrometastases (60).
SNB After Aesthetic Breast Surgery
Although SNB is technically feasible in patients with a history of aesthetic breast surgery (61), the impact on false-negative rate has not been studied.
SNB and Pregnancy
Blue dyes are contraindicated (8). Considering radiocolloids, the guidelines of ASCO did not validate their use in pregnancy (8). The European Association of Nuclear Medicine considered the isotopic technique safe, both in breast cancer and in melanoma, and the radiation dose potentially delivered to the fetus very low (12,23). Gentilini et al. recommend using a low activity (≤10 MBq), with imaging and surgery the same day (62).
SNB in Ductal Carcinoma in Situ
Core-needle biopsy may be affected by sampling error; in about 15% of patients with ductal carcinoma in situ, invasive disease is found at surgery (63). However, routine use of SNB in ductal carcinoma in situ is not recommended. SNB was positive in only 1.4% of unselected cases (64). SNB should be considered, however, when a mastectomy is planned, because SNB could not be performed afterward if invasive disease is diagnosed (3,65). SNB can also be an option with breast-conserving surgery when there is a high risk of invasive cancer at final diagnosis (e.g., large clinical or mammographic mass or high nuclear grade).
RESEARCH AREAS IN LYMPHATIC MAPPING
Axillary Reverse Mapping (ARM)
A radiotracer is used to identify the breast sentinel node, and a blue tracer is injected in the inner part of the arm to visualize lymphatics and nodes draining the upper extremity and allow their preservation (66). Early reports have suggested that ARM lymph nodes do not contain metastatic disease and that the technique can reduce the incidence of lymphedema in cases of completion ALND (66). Other authors have used the technique during ALND in node-positive patients and found a nonnegligible prevalence (10%–20%) of disease involving ARM nodes (67). Thus, further research is needed to determine the appropriate population for this new procedure in order to preserve oncologic safety.
SNB and Concomitant Probe-Guided Excision of Nonpalpable Breast Cancer
Currently, nonpalpable breast lesions benefit from presurgical wire localization. ROLL (radioguided occult lesion localization) is a more patient-friendly technique that consists of injecting a radiotracer into the lesion under ultrasound or stereotactic guidance, followed by intraoperative γ-probing. In 1 study, complete tumor excision with tumor-free margins was achieved in 89.4% of patients undergoing ROLL versus 82.4% undergoing wire-guided lumpectomy (68).
The radiotracer can serve for concomitant SNB (68,69). Van Rijk et al. applied this combined procedure (also called SNOLL) to 368 patients after intratumoral injection of 99mTc-nanocolloid. Tumor-free margins were obtained in 89%. The sentinel node could be identified in 97% of patients and was involved in 19% (69). Thus, ROLL with concomitant SNB is a strategy that deserves further investigation.
Intraoperative Imaging
Intraoperative real-time imaging using a portable γ-camera is being investigated in situations with difficult-to-localize sentinel nodes (70). Its role in breast cancer remains to be clarified.
CONCLUSION
In a woman with a unifocal T1 tumor, most data suggest that the SNB procedure offers safe (and possibly improved) staging with reduced morbidity. This is the case for most newly diagnosed breast cancer patients. In patients with large (>3 cm) or multiple ipsilateral tumors, SNB is still debated. More effort should be spent on improving patient selection (through such techniques as ultrasonography with fine-needle biopsy or 19F-FDG PET/CT) before SNB in high-risk patients.
Some recent multiinstitutional trials revealed high false-negative rates. Reducing the false-negative rate of SNB is an important and difficult challenge. We highlighted some causes of failure and discussed several points that should help in optimizing the procedure.
Documentation of internal mammary drainage on lymphoscintigraphy might be helpful in the choice of locoregional treatment. If this information is to be fully appreciated, the peritumoral injection technique needs to be better standardized.
SNB is a team procedure. Interaction between nuclear physicians and clinicians is more necessary than ever.
Acknowledgments
Prof. Jean-Luc Moretti, a member of the Editorial Board of JNM, died on December 21, 2010, in Paris at the age of 64, after a long illness. His death is a painful loss to his family and friends and to the international community of nuclear medicine.
Footnotes
↵† Deceased.
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the factors influencing the false-negative rate of SNB in breast cancer; (2) the risks associated with the use of the technique in specific situations such as large tumors, multiple ipsilateral tumors, or the setting of neoadjuvant chemotherapy; and (3) the meaning of internal mammary drainage on lymphoscintigraphy in terms of risk of occult internal mammary involvement.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNM is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNM designates each JNM continuing education article for a maximum of 1.0 AMA PRA Category 1 Credit. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For CE credit, participants can access this activity through the SNM Web site (http://www.snm.org/ce_online) through March 2012.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication July 27, 2010.
- Accepted for publication December 8, 2010.





{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- SNB STRATEGY AND SURGICAL MORBIDITY
- LOCOREGIONAL RECURRENCE AND SURVIVAL
- ALARMING RESULTS CONCERNING FALSE-NEGATIVE RATE
- OPTIMIZATION OF SNB PROCEDURE
- SNB IN PATIENTS AT HIGH RISK OF NODAL INVOLVEMENT
- INTERNAL MAMMARY DRAINAGE: POTENTIAL IMPACT ON DECISIONS ABOUT RADIOTHERAPY
- SNB AND SOME CONTROVERSIAL ISSUES
- RESEARCH AREAS IN LYMPHATIC MAPPING
- CONCLUSION
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Predicting Axillary Lymph Node Metastasis in Early Breast Cancer Using Deep Learning on Primary Tumor Biopsy Slides
- Internal Mammary Node Irradiation in Breast Cancer: The Issue of Patient Selection
- Lymphoscintigraphy and Sentinel Nodes
- The Yield of 18F-FDG PET/CT in Patients with Clinical Stage IIA, IIB, or IIIA Breast Cancer: A Prospective Study