


The estimated absorbed doses from a bolus intravenous administration of 18F-FDG are given in Table 1. The data and assumptions used in these calculations are presented as follows.
Estimated Absorbed Doses from Intravenous Administration of 18F-FDG (Mean ± SD)
RADIOPHARMACEUTICAL
18F-FDG is formed through radiochemical synthesis from cyclotron-produced 18F (K. Breslow, written communication, June 2000). Production of 18F is through proton bombardment of enriched 18O-water. 18F-fluoride is bound to 1,3,4,6-tetra-O-acetyl-2-O-trifluoromethanesulfonyl-β-d-mannopyranose (mannose triflate) under conditions of a stereospecific second-order nucleophilic substitution reaction, which produces no-carrier-added 18F-FDG. The 18F-FDG is injected intravenously as an isotonic, sterile, pyrogen-free, clear, colorless solution.
NUCLEAR DATA
18F decays to stable 18O by positron emission with a half-life of 109.77 min. Physical data are given in Table 2 (1).
Nuclear Data
BIOLOGIC DATA
Residence time (τ), as used here, refers to the area under the time–activity curve for the organ of interest, divided by the activity injected as an intravenous bolus at time zero. The residence times that form the basis for the calculations in this report were derived from the 4 sources described below.
Published Residence Times for 18F-FDG Calculated Using Mathematical Model for Distribution in Healthy Humans
For this study (2) conducted at the VA Medical Center in Palo Alto, CA, all patients recruited (6 men, 1 woman; age range, 55–74 y; 13 studies) had previously undergone cardiac stress studies, requested for the usual clinical indications, that had been interpreted as normal. Heart, liver, lung, whole blood, and plasma time–activity data were acquired for 90 min after intravenous 18F-FDG administration. Accumulated 18F-FDG activity in the urine was assayed at 100 min. Cardiac uptake of 18F-FDG had been expected to be enhanced by glucose loading. However, paired sessions in 5 of these subjects comparing the fasting state with the glucose-loaded state showed no significant differences; therefore, studies are included in this summary regardless of the subject’s glucose status. Three studies on 2 subjects are included here that were omitted from the analysis presented in the study of Hays and Segall (2) because they did not meet the criteria for paired samples required in that analysis.
The observed time–activity data (corrected for physical decay) for 18F activity in the heart, liver, lungs, plasma, erythrocytes, and urine were fitted simultaneously to a multicompartmental model using the SAAM 30 program and methodology as described in Hays and Segall (2). The physiologic model was solved, and the kinetic parameters were calculated for each study. Model-generated time–activity curves (incorporating physical decay) were used to determine the residence time for each source organ.
Brain time–activity data were not directly observed in this study. Instead, brain residence times were calculated using the observed plasma data, incorporating published model parameters for brain 18F-FDG transport (3) into this model. Because direct observational data were unavailable for red marrow, the residence time for this organ was calculated assuming that its 18F-FDG concentration and kinetics are the same as those of whole blood.
Time–activity curves projected from this model using mean parameter values derived from the individual studies are shown in Figure 1 for brain, heart, lungs, liver, and urine. In addition, urine data from the SAAM 30 output were used to provide biologic parameters for input into the MIRD dynamic bladder model (4) for calculation of the dose to the surface of the urinary bladder wall under a variety of circumstances. The results of this calculation were validated against the traditional (static 200 mL) MIRD bladder dose calculations. Table 3 presents the radiation dose per administered activity to the surface of the urinary bladder wall (mean and range) as provided by the dynamic bladder model for the 13 studies from the investigation of Hays and Segall (2).
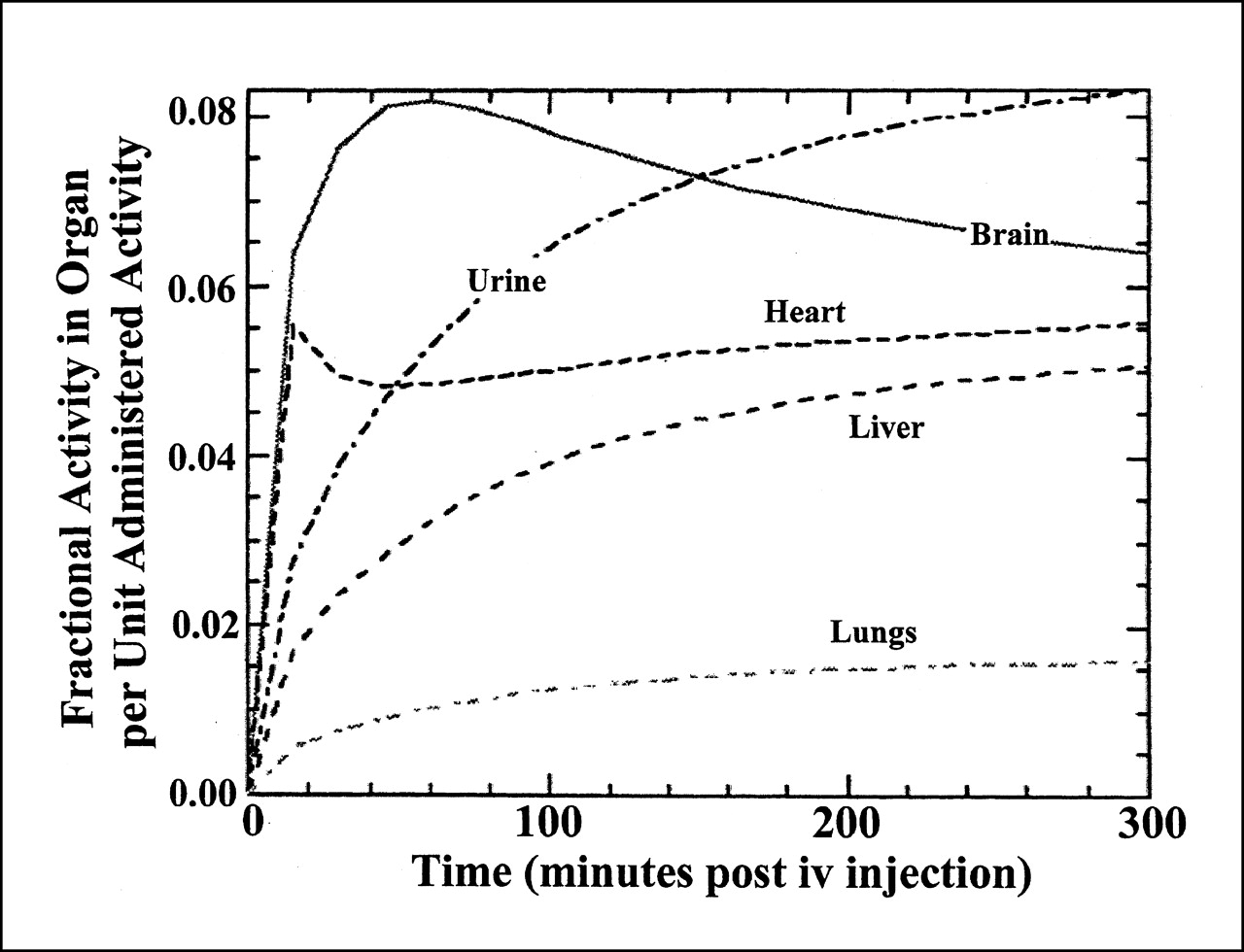
Time–activity curves for decay-corrected FDG activity in normal human brain, heart, lungs, liver, and urine. These curves were projected by model presented in report by Hays and Segall (2), using geometric means of model parameters derived from fits of data from 13 individual studies.
Radiation Dose per Administered Activity to Surface of Urinary Bladder Wall as Provided by Dynamic Bladder Model
Published Residence Times for 18F-FDG in Healthy Japanese Subjects
The results of Mejia et al. (5) were based on analysis of quantitative organ time–activity curves for 1 h after bolus intravenous 18F-FDG injection (2 h in 2 of the brain studies). They also recorded bladder activity for 2 h by external counting, normalized to the activity in the cumulated urine at 2 h. Because of the smaller size of the average Japanese adult, these authors used S tables devised for Japanese subjects (6) based on a model of Japanese reference man (7). To make these data comparable with the American data, values for residence times from this study were normalized to the standard MIRD model by multiplying by the ratio of the organ weight in the MIRD reference man to that in the Japanese reference man. (The logic of this adjustment is that tissue concentrations as a function of blood concentration would be expected to be the same regardless of body size or relative organ size. Thus, adjusting for the differences in sizes in the MIRD and the Japanese standard man models would make the Japanese data usable for dose calculations with the MIRD standard man.) Adjusted residence times for brain (6 subjects), heart (5 subjects), liver (4 subjects), pancreas (3 subjects), spleen (3 subjects), kidneys (4 subjects), and lungs (6 subjects) were used in the dose estimates presented here. Bladder residence times (8 subjects) using the static MIRD model in this study were comparable with those calculated by Hays and Segall (2).
Published Residence Times for 18F-FDG in Bladder
In the study by Jones et al. (8), bladder residence times were based on continuous external counting of bladder 18F activity in 10 patients, normalized to the activity in the cumulated urine at 2 h.
Published Residence Times for 18F-FDG in Brain
In the study by Niven et al. (9), brain residence times in patients undergoing clinical PET studies were derived from 1-h brain 18F-FDG dynamic studies in which data were acquired at 5-min intervals and integrated numerically using the trapezoidal rule. The authors assumed that no biologic removal occurred after the 1 h of data collection. Eight men and 6 women, aged 53–79 y, were studied, and duplicate studies were done on 6 of the men and all of the women (26 studies total). Because there were no statistically significant sequential differences in residence time, data on each individual study (provided by E. Niven, written communication, July 2001) are considered separately in the current report. The authors found a minor difference (P < 0.05) in residence times between sexes, with residence times for women 4.8% ± 5.2% (mean ± SD) greater than those for men. In pooling data for the current report, this difference has been ignored.
Summary statistics for the residence times used in the dose estimates are presented in Table 4.
Residence Times, in Hours, Used in Absorbed Dose Estimates
ABSORBED DOSE ESTIMATES
Residence times calculated from data from individual subjects were used with S values to calculate radiation absorbed dose estimates for each person. The source organs included brain, heart wall, liver, kidneys, pancreas, spleen, urinary bladder, red marrow, lungs and whole body, the organs for which observed or inferred residence time data were available. Absorbed doses were calculated for these organs and also for the gonads. In this calculation, it was assumed that the gonads had the same 18F-FDG concentration as the remainder of the body. The dose to each target organ was calculated according to the procedures outlined in MIRD Pamphlet No. 1, Revised (10). The dose per unit administered activity for an organ is the sum of the products obtained from multiplying the residence time in the source organ by the appropriate S value. With the exception of brain, the S values were those published in MIRD Pamphlet No. 11 (11). Because the brain is not included in MIRD Pamphlet No. 11, the S value for brain irradiating brain was calculated from the absorbed fractions given in MIRD Pamphlet No. 5 (12). A mass of 1,400 g was assigned to the brain of the adult man. The radiation dose to the brain includes only the dose from activity in the brain because the fraction of radiation emitted from other source organs that would be absorbed in the brain is negligible. The individual dose estimates were averaged, and these averaged results are shown in Table 1. The number of subjects whose data were included in the calculation for each organ is shown in Table 4.
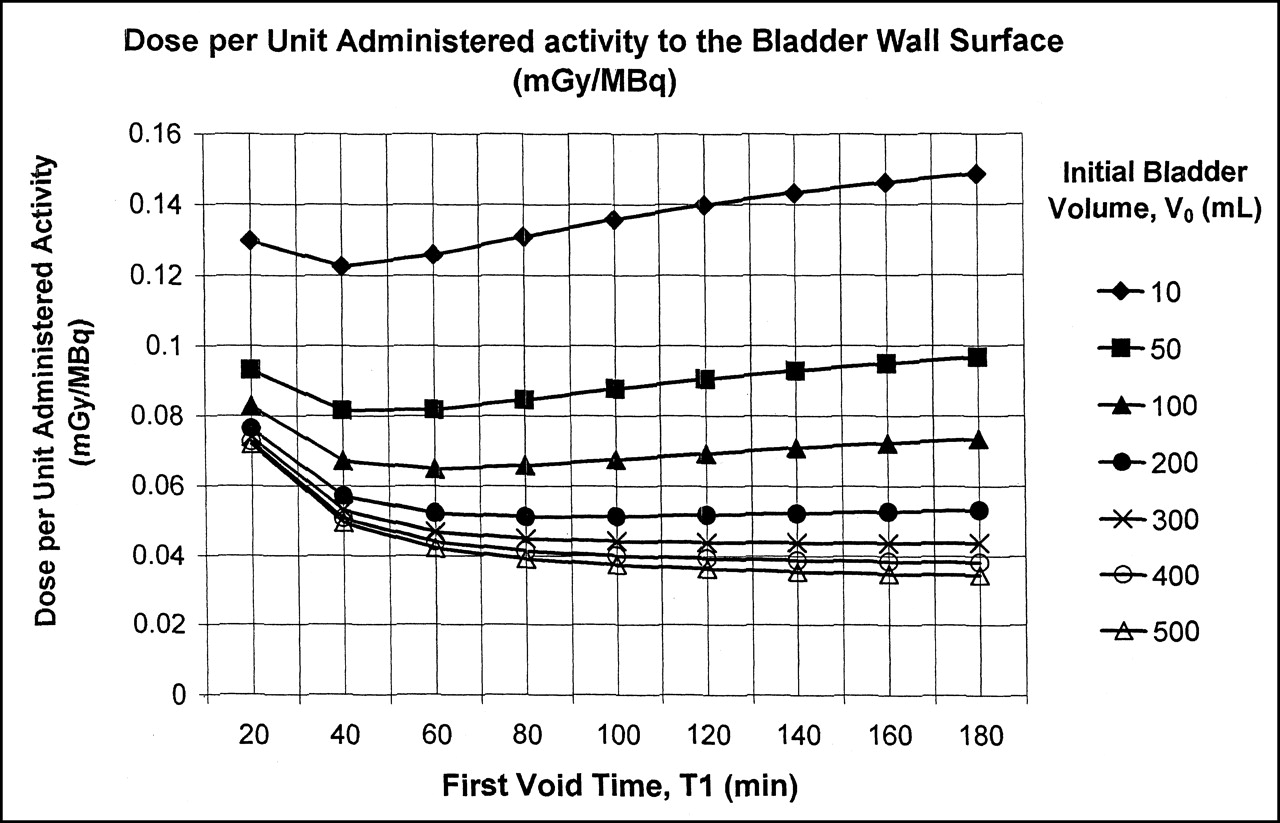
Bladder doses for a typical subject under various conditions of initial urine volume and void times are presented in Figure 2. These were calculated using the MIRD dynamic bladder model (4), incorporating data from a subject reported by Hays and Segall (2). Table 3 presents the means and ranges of the results of these calculations in the 13 studies from the data of Hays and Segall (2), with the bladder fill rate taken to be 1 mL/min during waking hours and 0.5 mL/min during sleeping hours.

Dose per unit administered activity to bladder-wall surface as calculated by MIRD dynamic bladder model (4) for typical subject from study of Hays and Segall (2) for 1.0/0.5 mL/min (daytime/nighttime) bladder filling rate. Dose depends on initial bladder (urine) volume, V0, and time of first void, T1.
DISCUSSION
As a MIRD dose estimate report, this study incorporates only data from well-documented human studies of 18F-FDG kinetics done independently in more than one laboratory and providing time–activity data with sufficient time points to project cumulated activities. In particular, the brain data from the study by Jones et al. (8) were not incorporated in this report because they were based on a single observation. Similarly, the data from a 1998 study by Deloar et al. (13) were not included because their residence times were projected from only 3 time points.
Although 18F-FDG is widely used clinically and scientifically, there have been few studies that provide the type of human kinetic data needed for dosimetry calculations. The International Commission on Radiological Protection (ICRP), in its publications 53 (14) and 80 (15), presents tables of 18F-FDG doses derived from a model assuming specific uptake of 18F-FDG by the brain and heart with the further assumption that all other activity is distributed uniformly in the body. The ICRP authors used the kinetic data on urinary excretion from the study of Jones et al. (8) to calculate the kinetics of total-body 18F-FDG retention and assumed that 4% and 6% of the administered tracer were taken up by the myocardium and brain, respectively. They were not specific about the source of those figures. The radiation dose values for 18F-FDG presented in ICRP 80 differ from those in ICRP 53, but the database for the calculations presented in ICRP 80 appears to be the same as that used for the ICRP 53 report.
Several differences exist between the results provided in ICRP 80 (15) and those presented here. Although the whole-body residence time in the ICRP publication (2.13 h) is similar to that reported here (2.38 h), residence times for some source organs are notably different. This MIRD report finds a brain residence time of 0.23 h, which is higher than the ICRP value of 0.15 h, resulting in a correspondingly greater dose to the brain (0.046 mGy/MBq vs. 0.028 mGy/MBq). For the liver, ICRP 80 gives the dose as 0.011 mGy/MBq, whereas this report lists the mean liver dose as 0.034 mGy/MBq. This difference reflects the observed specific liver uptake found in the human studies that form the basis of this MIRD dose-estimate report, whereas the ICRP authors assumed that the human liver had no specific 18F-FDG uptake (12).
The MIRD Committee reports the “total-body” dose (based on the total energy deposited in the body divided by its total mass), whereas the ICRP reports “effective dose” (a value estimated by applying risk-based weighting factors to individual organ doses, to estimate a uniform whole-body dose that in theory gives the same risk as the nonuniform dose pattern that actually occurred). These values are not directly comparable, being based on different concepts. It has been shown that effective dose for many diagnostic radiopharmaceuticals is generally higher than total-body dose by a factor of 1.5–10 (16). For 18F-FDG, using the same kinetic data as input, effective dose is estimated to be higher than total-body dose by approximately a factor of 2.
CONCLUSION
This dose estimate report presents estimated radiation doses to human organs after a bolus intravenous injection of 18F-FDG, based on review of the published literature as interpreted by members of the MIRD Committee. The absorbed dose estimates are summarized in Table 1.
Acknowledgments
The members of the MIRD Committee of the Society of Nuclear Medicine are Wesley E. Bolch, A. Bertrand Brill, N. David Charkes, Darrel R. Fisher, Marguerite T. Hays, Ruby F. Meredith, George Sgouros, Jeffry A. Siegel, Stephen R. Thomas, and Evelyn E. Watson (chair). The activities of the MIRD Committee are partially supported by the Society of Nuclear Medicine.
Footnotes
Received Mar. 20, 2001; revision accepted Oct. 24, 2001. For correspondence contact: Marguerite T. Hays, MD, 270 Campesino Ave., Palo Alto, CA 94306.
E-mail: ritahays19{at}yahoo.com
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A metabolically stable PET tracer for imaging synaptic vesicle protein 2A: Synthesis and preclinical characterization of [18F]SDM-16
- Establishment of National DRL for CT in Hybrid Imaging Studies (The Second Phase of the National NM CT (PET) Dose Audit for Kuwait Population -2019)
- Human Radiation Dosimetry for Orally and Intravenously Administered 18F-FDG
- Biodistribution, Tumor Detection, and Radiation Dosimetry of 18F-5-Fluoro-2'-Deoxycytidine with Tetrahydrouridine in Solid Tumors
- A Microdose PET Study of the Safety, Immunogenicity, Biodistribution, and Radiation Dosimetry of 18F-FB-A20FMDV2 for Imaging the Integrin {alpha}v{beta}6
- Update on 18F-Fluciclovine PET for Prostate Cancer Imaging
- Assessment of Tryptophan Uptake and Kinetics Using 1-(2-18F-Fluoroethyl)-L-Tryptophan and {alpha}-11C-Methyl-L-Tryptophan PET Imaging in Mice Implanted with Patient-Derived Brain Tumor Xenografts
- Radiation Dosimetry of Whole-Body Dual-Tracer 18F-FDG and 11C-Acetate PET/CT for Hepatocellular Carcinoma
- Determining the Minimal Required Radioactivity of 18F-FDG for Reliable Semiquantification in PET/CT Imaging: A Phantom Study
- Diagnostic Reference Levels of CT Radiation Dose in Whole-Body PET/CT
- Uncertainty Quantification in Internal Dose Calculations for Seven Selected Radiopharmaceuticals
- Radiation Dosimetry of the Fibrin-Binding Probe 64Cu-FBP8 and Its Feasibility for PET Imaging of Deep Vein Thrombosis and Pulmonary Embolism in Rats
- Absorbed 18F-FDG Dose to the Fetus During Early Pregnancy
- The Effect of Renal Failure on 18F-FDG Uptake: A Theoretic Assessment
- Radiopharmaceuticals for Nuclear Cardiology: Radiation Dosimetry, Uncertainties, and Risk
- Dual-Modality Imaging: Combining Anatomy and Function
- Estimation of the {beta}+ Dose to the Embryo Resulting from 18F-FDG Administration During Early Pregnancy
- Proposed Addendum to Previously Published Fetal Dose Estimate Tables for 18F-FDG
- 18F-Fluorothymidine Radiation Dosimetry in Human PET Imaging Studies
- 18F-Fluoroerythronitroimidazole Radiation Dosimetry in Cancer Studies