


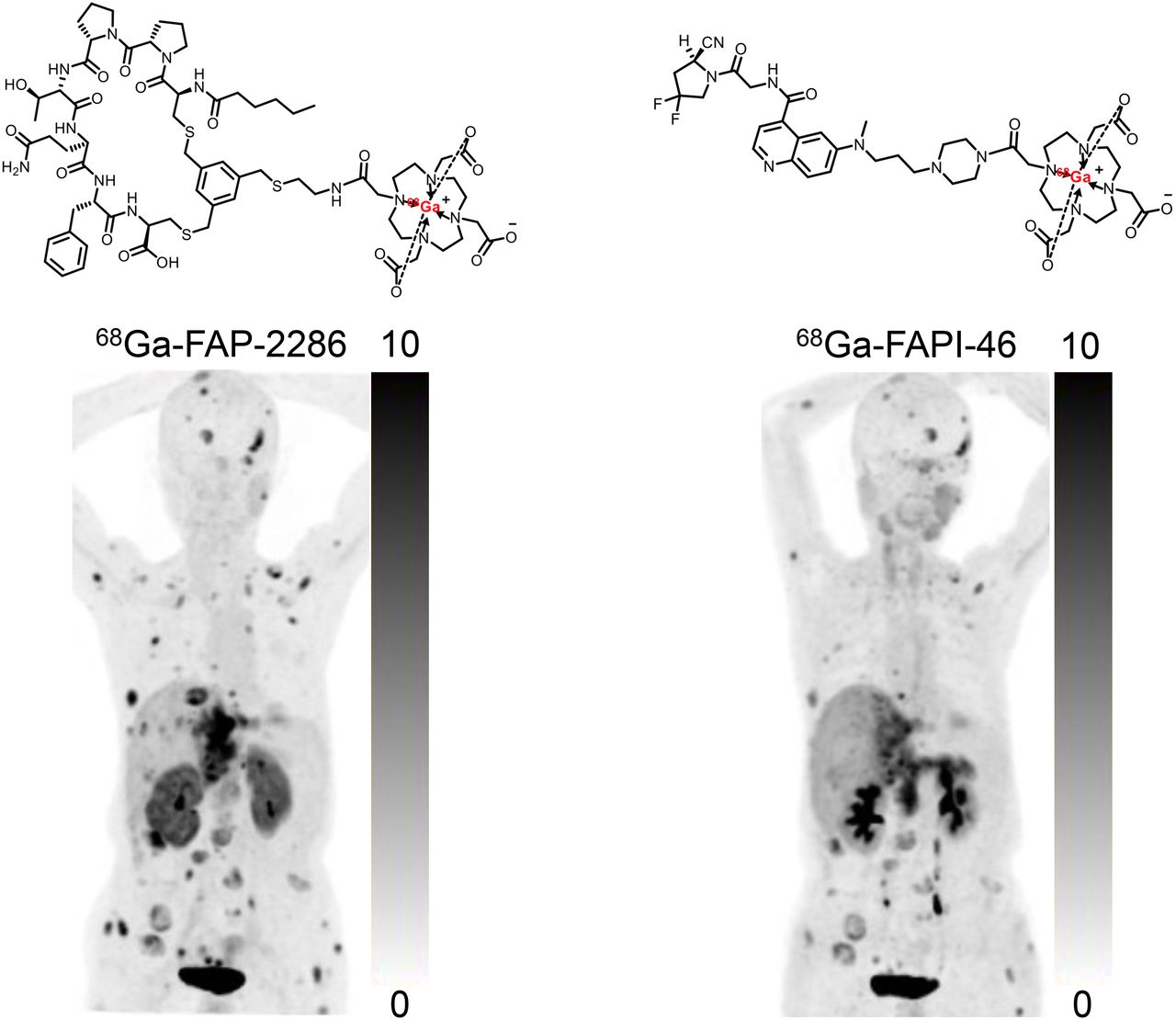
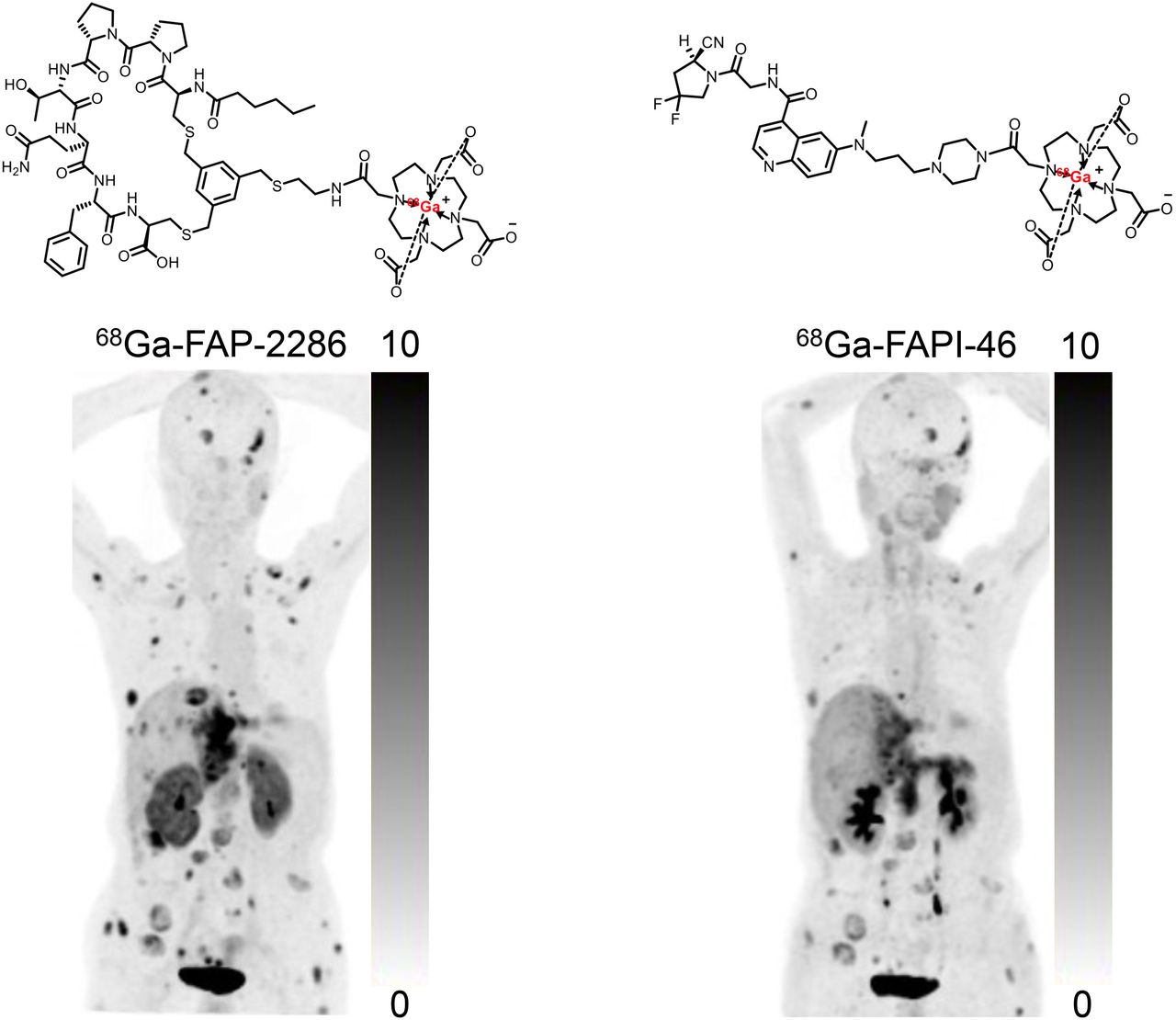
Visual Abstract
Abstract
PET imaging that targets fibroblast activation protein (FAP) on the surface of cancer-associated fibroblasts has yielded promising tumor diagnostic results. FAP-2286 contains cyclic peptides as FAP-binding motifs to optimize tumor retention compared with the small-molecule FAP inhibitor (FAPI) series (FAPI-04/46). The aim of this study was to evaluate the diagnostic accuracy of 68Ga-FAP-2286 to detect primary and metastatic lesions in patients with various types of cancer, compared with 18F-FDG and 68Ga-FAP-2286. Methods: Sixty-four patients with 15 types of cancer underwent 68Ga-FAP-2286 PET/CT for initial assessment or detection of recurrence. For comparison, 63 patients underwent paired 68Ga-FAP-2286 and 18F-FDG PET/CT and 19 patients underwent paired 68Ga-FAP-2286 and 68Ga-FAPI-46 PET/CT. Lesion uptake was quantified as SUVmax and tumor-to-background ratio. The Wilcoxon matched-pairs signed-rank test was used to compare SUVmax between PET modalities, and the McNemar test was used to compare lesion detectability. Results: Uptake of 68Ga-FAP-2286 was significantly higher than that of 18F-FDG in primary tumors (median SUVmax, 11.1 vs. 6.9; P < 0.001), lymph node metastases (median SUVmax, 10.6 vs. 6.2; P < 0.001), and distant metastases, resulting in improved image contrast and lesion detectability. All primary tumors (46/46) were clearly visualized by 68Ga-FAP-2286 PET/CT, whereas 9 of the 46 lesions could not be visualized by 18F-FDG PET/CT. The lesion detection rate of 68Ga-FAP-2286 PET/CT was superior to that of 18F-FDG PET/CT for involved lymph nodes (98% [105/107] vs. 85% [91/107], P = 0.001) and bone and visceral metastases (95% [162/171] vs. 67% [114/171], P < 0.001). 68Ga-FAP-2286 yielded tumor uptake and lesion detection rates similar to those of 68Ga-FAPI-46 in a subcohort of 19 patients. Conclusion: 68Ga-FAP-2286 is a promising FAP-inhibitor derivative for safe cancer diagnosis, staging, and restaging. It may be a better alternative to 18F-FDG for the cancer types that exhibit low-to-moderate uptake of 18F-FDG, which include gastric, pancreatic, and hepatic cancers. In addition, 68Ga-FAP-2286 and 68Ga-FAPI-46 yielded comparable clinical results.
The glucose analog 18F-FDG is extensively used for tumor metabolic imaging. Cancer-associated fibroblasts, one of the most abundant components of the tumor stroma, are alternative targets for the imaging of solid tumors (1). Considering the high expression of fibroblast activation protein (FAP) on the cell surfaces of activated cancer-associated fibroblasts and its limited expression in normal tissue, PET imaging of cancer-associated fibroblasts with radiolabeled FAP inhibitors (FAPIs) is an active field in nuclear medicine (2).
68Ga- and 18F-radiolabeled FAPI variants (including FAPI-04, FAPI-46, and FAPI-74) have yielded promising results in the diagnosis of various cancers (3–5). Furthermore, FAPI has been reported to be superior to 18F-FDG in PET/CT imaging of, for example, hepatic, gastric, and pancreatic cancer, as well as peritoneal carcinomatosis (6–9). However, these FAPI molecules are normally retained in tumors for a relatively short time, potentially limiting their use for radionuclide therapy (10,11).
FAP-2286 is a low-molecular-weight, FAP-targeted polypeptide linked to the chelator DOTA, which allows for the attachment of radionuclides for imaging and therapeutic use. FAP-2286, developed using a cyclic peptide as a binding motif, is reported to be potent, highly selective for FAP, and stable in human plasma (12). In addition, it has a long retention time in tumors, translating to the robust antitumor efficacy of 177Lu-FAP-2286 as demonstrated in a preclinical study (12). In this study, FAP-2286 had a half-maximal effective concentration comparable to that of FAPI-46 (4.9 vs. 1.7 nM), as well as better cellular internalization, longer retention, and higher uptake on PET/CT scans at all time points in human embryonic kidney FAP cells. Moreover, 177Lu-FAP-2286 had a significantly higher tumor retention than 177Lu-FAPI-46 at 24 and 72 h after injection, resulting in excellent antitumor efficacy in human embryonic kidney FAP xenografts. The results of a recent pilot study in which 177Lu-FAP-2286 was used for peptide-targeted radionuclide therapy in patients with diverse advanced adenocarcinomas exhibited acceptable side effects and prolonged retention and activity (13). The preliminary results from the LuMIERE trial (NCT04939610) reported that 177Lu-FAP-2286 demonstrated a manageable safety profile with some promising efficacy in 9 patients with 7 types of cancer (partial response was observed in 1 patient who completed 6 cycles of 177Lu-FAP-2286 in a 3.7-GBq dose cohort) (14). When these results are taken together, FAP-2286 exhibits promising characteristics as a targeting vector, with potent and selective FAP binding that leads to intense tumor accumulation and substantial therapeutic efficacy.
In this study, we aimed to investigate the diagnostic accuracy of the novel imaging agent 68Ga-FAP-2286 for detecting primary and metastatic lesions in patients with various types of cancer, and we compared the results with those of 18F-FDG and 68Ga-FAPI-46.
MATERIALS AND METHODS
Participant Enrollment
This is a preliminary report of an ongoing, single-center, prospective study of the diagnostic accuracy of 68Ga-FAP-2286 for PET/CT imaging of solid tumors. The institutional review board approved the study (approval 2022KY013), and all subjects gave written informed consent. The study was registered at ClinicalTrials.gov (NCT05392205). The inclusion criteria were as follows: adult patients (aged 18 y or older), patients with newly diagnosed or previously treated malignant tumors (to avoid the treatment impact on radiotracer uptake, the interval between the completion of therapy and the PET scan was > 6 mo), and patients who were able to provide informed consent or assent according to the guidelines of the Clinical Research Ethics Committee. Exclusion criteria were as follows: patients with nonmalignant disease; patients who were pregnant; and patients, their parents, or their legal representatives who were unable or unwilling to provide written informed consent.
Radiolabeling
FAP-2286 and FAPI-46 were obtained from Yantai Dongcheng Pharmaceutical Group Co., Ltd., and Jiangsu Huayi Technology Co., Ltd., respectively. Both compounds were used for research purposes. 18F-FDG was manufactured according to the standard method of our laboratory (15,16) using the coincidence 18F-FDG synthesis module (TracerLab FxFN; GE Healthcare). The FAPI-46 ligands were radiolabeled with 68Ga according to a previous protocol (17). Briefly, 925–1,110 MBq of 68GaCl3 eluted from the 68Ge/68Ga generator (ITG) were reacted with 25 μg (28.2 nmol) of FAPI-46 in 1 mL of 0.25 M sodium acetate buffer for 10 min at 100°C and purified before use. FAP-2286 ligands were radiolabeled with 68Ga in a similar protocol (925–1,110 MBq of 68GaCl3 reacted with 25 μg [17.0 nmol] of FAP-2286). The synthesis of the radiopharmaceutical is detailed in the supplemental materials (available at http://jnm.snmjournals.org).
PET/CT Imaging and Evaluation
The dose of intravenously injected 68Ga-FAP-2286 was calculated according to the participants’ body weight (1.8–2.2 MBq/kg). At 1 h after intravenous administration, the participants underwent PET/CT via a hybrid scanner (Discovery MI; GE Healthcare). All obtained data were transferred to the Advantage Workstation (version AW 4.7; GE Healthcare) and reconstructed using the Bayesian penalized-likelihood reconstruction algorithm (Q.clear; GE Healthcare). For patients with malignant disease, additional 18F-FDG or 68Ga-FAPI-46 PET/CT was performed for comparative purposes, depending on the patients’ willingness. The PET/CT imaging protocols for 18F-FDG and 68Ga-FAPI-46 were the same as those for 68Ga-FAP-2286, except that 6 h of fasting were required before the 18F-FDG PET/CT scan (the supplemental materials provide details) (18).
All PET images were evaluated by 2 board-certified nuclear medicine physicians, each with at least 10 y of experience in PET/CT imaging; the 2 physicians were not masked to the study. Disagreements in opinion were resolved via discussion and consensus. In addition to visual evaluation, lesions were evaluated semiquantitatively by selection of regions of interest. The SUVmax was calculated automatically using the Advantage Workstation. Regions with radiotracer uptake higher than the background activity in primary tumors, lymph nodes, the lungs, the liver, peritoneal surfaces, and other body parts were considered pathologic. Tracer uptake in normal organs (background) was quantified on the basis of SUVmean, which was delineated with a sphere 1 cm in diameter (for the small organs, including thyroid, salivary gland, pancreas) to 2 cm in diameter (for the other organs, including brain, heart, liver, kidney, spleen, muscle, and bone marrow) placed inside the organ parenchyma. The tumor-to-background ratio (TBR) was calculated as the ratio of the tumor SUVmax to the background SUVmean. Physiologic uptake of 68Ga-FAP-2286 and 68Ga-FAPI-46 in normal organs was determined by calculating the SUVmean of the background measurements in the heart, liver, spleen, lungs, kidneys, muscles, prostate, and uterus. Histopathologic results obtained via surgery or biopsy served as the gold standard for the final diagnosis. If tissue-based diagnosis was not possible, comprehensive evaluations of multimodal imaging characteristics were used as the reference standard.
Statistical Analysis
Statistics were analyzed using SPSS, version 22.0 (IBM). The Wilcoxon matched-pairs signed-rank test was used to compare SUVs derived from 68Ga-FAP-2286, 68Ga-FAPI-46, and 18F-FDG PET/CT images. The McNemar test was used to compare the lesion detectability of different PET scans. The paired-sample t test was used to evaluate differences in normal-organ uptake between 68Ga-FAP-2286 and 68Ga-FAPI-46 PET/CT. Statistical significance was defined as a P value of less than 0.05.
RESULTS
Patient Characteristics
From March 1, 2022, to May 31, 2022, 64 patients with malignant disease (38 men; median age, 57.5 y; range, 32–85 y) who underwent 68Ga-FAP-2286 PET/CT were enrolled in this prospective study (Table 1). Among the 64 patients, 44 (9 types of cancer) underwent PET/CT for initial assessment (lesion detection and staging) and the other 20 (9 types of cancer) for detection of tumor recurrence and metastases (restaging). The final diagnosis was based on histopathologic results (n = 58) and diagnostic radiology (comprehensive considerations of imaging findings, n = 6). For comparison, 63 patients underwent paired 68Ga-FAP-2286 and 18F-FDG PET/CT and 19 patients underwent paired 68Ga-FAP-2286 and 68Ga-FAPI-46 PET/CT. Representative images from the 3 types of PET scans are shown in Figure 1.
Patients’ Characteristics (n = 64)

Maximum-intensity projections of 18F-FDG, 68Ga-FAP-2286, and 68Ga-FAPI-46 PET/CT imaging in 7 patients with different types of cancer (histologically confirmed). Tumor lesions are indicated with arrows. Ca = carcinoma; HNCUP = head and neck carcinoma of unknown primary; NPC = nasopharyngeal carcinoma.
Adverse Events and Biodistribution
All patients tolerated the 68Ga-FAP-2286 PET/CT scans. There were no signs of any drug-related pharmacologic effects or other adverse physiologic responses. All observed vital signs (including temperature, blood pressure, and heart rate) were normal at the 4-h follow-up. No abnormal symptoms were reported by the patients.
The in vivo distribution pattern of 68Ga-FAP-2286 was evaluated and compared with that of 68Ga-FAPI-46 in 19 patients who underwent both scans. 68Ga-FAP-2286 exhibited an in vivo distribution pattern similar to that of 68Ga-FAPI-46, except for a slightly higher physiologic uptake in the liver and kidneys (Fig. 2). Semiquantitative analysis demonstrated that 68Ga-FAP-2286 uptake in the kidneys (5.3 ± 1.5 vs. 2.3 ± 1.2, t = 8.959, P < 0.001), liver (2.8 ± 1.0 vs. 1.5 ± 0.9, t = 8.582, P < 0.001), and heart (1.9 ± 0.4 vs. 1.4 ± 0.3, t = 6.557, P < 0.001) were higher than that of 68Ga-FAPI-46. In contrast, background uptake of 68Ga-FAP-2286 in the thyroid (1.6 ± 0.5 vs. 1.9 ± 0.5, t = −3.537, P = 0.01), pancreas (1.8 ± 0.3 vs. 2.1 ± 0.5, t = −2.559, P = 0.038), muscles (1.3 ± 0.5 vs. 1.5 ± 0.5, t = −2.515, P = 0.04), and salivary glands (2.5 ± 0.6 vs. 3.6 ± 1.0, t = −3.356, P = 0.012) were lower than that of 68Ga-FAPI-46 (Fig. 2).

PET-based biodistribution analysis of 68Ga-FAP-2286 and 68Ga-FAPI-46 in normal organs at 1 h after injection. Results are shown as means and SDs from 19 patients. *P < 0.05. ***P < 0.001. ns = not statistically significant.
68Ga-FAP-2286 and 18F-FDG Uptake in Cancer Patients
Among the 44 patients who underwent paired 68Ga-FAP-2286 and 18F-FDG PET/CT for initial diagnosis, 1 was diagnosed with a synchronous double cancer (esophageal cancer and lung adenocarcinoma) and 1 was diagnosed with multifocal breast cancer (4 primary tumors in the same breast). In addition, the primary tumors could not be located in 2 patients with head and neck cancers of unknown primary. Thus, in total, 46 primary tumor lesions (all confirmed by histopathology) were evaluated in this study (Table 2). All primary tumors were clearly visualized with intense radiotracer uptake on 68Ga-FAP-2286 PET/CT, whereas 9 of the 46 lesions could not be visualized via 18F-FDG PET/CT. Primary tumor lesions exhibiting no pathologic uptake on 18F-FDG PET/CT images were gastric cancer (n = 3), hepatic cancer (n = 3), breast cancer (n = 2), and pancreatic cancer (n = 1) (Supplemental Fig. 1). The SUVmax of all primary tumor lesions derived from 68Ga-FAP-2286 PET/CT was significantly higher than that derived from 18F-FDG PET/CT (11.1 vs. 6.9, P < 0.001). Moreover, lesions exhibited a 3-fold higher TBR on 68Ga-FAP-2286 PET/CT images than they did on 18F-FDG PET/CT images (9.2 vs. 3.0, P < 0.001), thus improving the image contrast for tumor detection and delineation. Representative images are shown in Supplemental Figure 2.
Comparison of SUVmax on 68Ga-FAP-2286 and 18F-FDG PET/CT Images in Primary and Metastatic Tumors
We investigated tumor uptake over time by performing 68Ga-FAP-2286 PET at multiple time points (0.5, 1, and 3 h after injection) in patients 33 and 54. The SUVmax in patient 33 (nasopharyngeal carcinoma with lymph node and bone metastases) increased from 0.5 to 3 h in the primary tumor (by 72.1%, from 8.6 to 14.8), involved lymph nodes (by 5.2%–69.1%), and 1 bone metastasis (by 64.4%) (Fig. 3). Similar results were observed in patient 54 (metastatic colon cancer); the hepatic metastases demonstrated stable 68Ga-FAP-2286 uptake but an increased TBR from 1 to 3 h (Supplemental Fig. 3).

A 66-y-old man with nasopharyngeal carcinoma who underwent 68Ga-FAP-2286 PET/CT at different time points after injection. Rapid and stable radiotracer uptake was observed in both primary and metastatic lesions. Semiquantitative analysis demonstrated SUVmax increase at 0.5–3 h in primary tumor (by 72.1% [from 8.6 to 14.8]), involved lymph nodes (by 5.2%–69.1%), and 1 bone metastasis (by 64.4%). BM = bone metastasis; LNM = lymph node metastasis.
Among the 19 patients who underwent paired 68Ga-FAP-2286 and 18F-FDG PET/CT for cancer restaging, 68Ga-FAP-2286 demonstrated significantly higher lesion detection rates than 18F-FDG PET/CT (100% [9/9] vs. 33% [3/9], P = 0.031) in 9 locally recurrent tumors (all confirmed by histopathology) (Supplemental Fig. 2B). Among the 63 patients who underwent paired 68Ga-FAP-2286 and 18F-FDG PET/CT for initial staging or restaging, 107 lymph node metastases and 171 bone and visceral metastases were evaluated. Among these, 66 metastatic lesions (12 lymph nodes and 54 bone and visceral metastases) were confirmed by histopathology, and 212 lesions (95 lymph nodes and 117 bone and visceral metastases) were confirmed by diagnostic radiology. 68Ga-FAP-2286 yielded significantly higher radiotracer uptake (SUVmax, 10.6 vs. 6.2; P < 0.001) and TBR (9.0 vs. 3.7, P < 0.001) than did 18F-FDG in the metastatic lymph nodes. Therefore, 68Ga-FAP-2286 PET/CT had a significantly higher detection rate (98% [105/107] vs. 85% [91/107], P = 0.001) than 18F-FDG PET/CT in the diagnosis of lymph node metastases. Interestingly, the 18F-FDG uptake was positive and the 68Ga-FAP-2286 uptake was negative in the enlarged mediastinal lymph nodes in 1 patient with gastric cancer; these lymph nodes were confirmed to be inflammatory on endobronchial ultrasound-guided transbronchial needle aspiration (Supplemental Fig. 2C). Regarding PET/CT imaging of bone and visceral metastases, 68Ga-FAP-2286 yielded a greater number of positive lesions (95% [162/171] vs. 67% [114/171], P < 0.001) and a higher radiotracer uptake and TBR than 18F-FDG in most lesions (hepatic, peritoneal, subcutaneous, and bone metastases). Interestingly, no significant difference in hepatic metastasis SUVmax was observed between 68Ga-FAP-2286 and 18F-FDG, even though the TBR yielded by 68Ga-FAP-2286 (4.1) was twice that yielded by 18F-FDG in those lesions (2.2, P < 0.001).
With the new lymph node and visceral metastases detected by 68Ga-FAP-2286 PET/CT, TNM staging was upgraded in 3 patients (3/44, 7%), including 1 with gastric cancer (from IIA to IIB), 1 with esophageal cancer (from IIIA to IIIB), and 1 with nasopharyngeal cancer (from IVA to IVB). Compared with 18F-FDG, 68Ga-FAP-2286 PET/CT detected a greater number of metastatic lesions or a larger disease extent in 12 patients (12/44, 27%), including 4 with pancreatic cancer, 2 with hepatic cancer, 2 with nasopharyngeal cancer, 1 with esophageal cancer, 2 with ovarian cancer, and 1 with gastric cancer. Among the other 19 patients in whom recurrence was detected, 68Ga-FAP-2286 PET/CT detected 18F-FDG–negative locally recurrent tumors in 6 patients (6/19, 32%) and 18F-FDG–negative metastatic lesions in 7 patients (7/19, 37%). The patients with new lesions or a larger disease extent detected by 68Ga-FAP-2286 PET/CT are presented in Supplemental Table 1.
68Ga-FAP-2286 and 68Ga-FAPI-46 Uptake in Patients with Cancer
Among the 19 patients who underwent paired 68Ga-FAP-2286 and 68Ga-FAPI-46 PET/CT, 11 did so for initial staging and 8 for restaging. The 68Ga-FAP-2286–derived SUVmax was comparable to that derived from 68Ga-FAPI-46 in 13 primary tumor lesions (13.6 vs. 13.3, P = 0.53; Table 3), 4 recurrent tumors (11.2 vs. 9.6, P = 0.47), and 33 metastatic lymph nodes (8.3 vs. 8.2, P = 0.28). Too few patients with each cancer type underwent paired analyses with these modalities to allow for comparisons of radiotracer uptake per tumor type. Regarding visceral and bone metastases, the quantitative tumor uptake of 68Ga-FAP-2286 was not inferior to that of 68Ga-FAPI-46 in the lung (4.0 vs. 3.9), liver (4.6 vs. 4.4), peritoneum (9.8 vs. 11.4), or bone (6.9 vs. 5.8) (all P > 0.05; Table 3). Interestingly, in 1 patient with metastatic cholangiocarcinoma, the median SUVmax of 68Ga-FAP-2286 was significantly higher than that of 68Ga-FAPI-46 (8.1 vs. 6.0, P = 0.022) in the widespread subcutaneous metastases, and 68Ga-FAP-2286 PET/CT detected a greater number of subcutaneous metastases than 68Ga-FAPI-46 (25 vs. 16). Representative images are shown in Figures 4⇓–6.
Comparison of SUVmax on FAP-2286 and FAPI-46 PET/CT Images in Primary and Metastatic Lesions

A 65-y-old woman with metastatic intrahepatic cholangiocarcinoma who underwent imaging for cancer restaging. 68Ga-FAP-2286 (A) revealed greater number of metastases and higher uptake than 68Ga-FAPI-46 (B) in widespread subcutaneous metastases (arrows).

A 72-y-old man with newly diagnosed nasopharyngeal carcinoma who underwent PET/CT for tumor staging. 68Ga-FAP-2286 PET/CT (A) showed higher radiotracer uptake in primary tumor (SUVmax, 17.4 vs. 12.2; arrows) than 68Ga-FAPI-46 (B).

A 44-y-old man with glioblastoma who underwent surgical resection 1 y before images were obtained. (A) MRI revealed suggestive recurrent lesions in right frontal lobe adjacent to surgical margin (arrow). (B [axial PET image] and C [fused PET/CT image]) 68Ga-FAP-2286 PET/CT yielded higher radiotracer uptake (SUVmax, 4.2 vs. 2.7; arrows) and TBR (70.0 vs. 45.0) than 68Ga-FAPI-46 in these lesions. (D [intraoperative view] and E [fluorescence-guided surgery]) Patient subsequently underwent surgical resection, and postoperative pathology confirmed diagnosis of recurrent glioblastoma. T1WI+C = T1-weighted imaging with contrast enhancement; T2WI = T2-weighted imaging.
DISCUSSION
In this study, we conducted clinical investigations using 68Ga-FAP-2286 for PET/CT imaging in patients with different types of cancer. We aimed to investigate whether 68Ga-FAP-2286 could be used for cancer imaging, and we compared it with 18F-FDG and 68Ga-FAPI-46.
The encouraging results from a preclinical study and a first-in-humans study (12,13) warranted further clinical evaluation of 68Ga-FAP-2286. Therefore, we are in the process of investigating the diagnostic accuracy of 68Ga-FAP-2286 for the identification of FAP-positive solid tumors via PET/CT. First, we evaluated the in vivo distribution pattern of 68Ga-FAP-2286 and compared it with that of 68Ga-FAPI-46. The physiologic uptake of 68Ga-FAP-2286 was lower than that of 68Ga-FAPI-46 in the muscles, salivary glands, thyroid, and pancreas. However, 68Ga-FAP-2286 uptake in the kidneys, liver, and heart was higher than that of 68Ga-FAPI-46, thus suggesting that the cyclopeptide structure of FAP-2286 may lead to altered in vivo pharmacokinetics. Cyclic peptides may have improved biologic properties compared with the small-molecule FAPI series (19), including stronger receptor selectivity and binding affinity, because of increased plasma stability and conformational rigidity. Indeed, 177Lu-FAP-2286 had a long effective half-life in the first-in-humans study (35 ± 9 h in the entire body and 44 ± 25 h in bone metastases) (13). Moreover, tumor uptake in our study increased in one patient and remained stable in the other from 0.5 to 3 h after injection. In preclinical studies, FAP-2286 demonstrated longer tumor retention than FAPI-46 at later time points (12), and greater antitumor efficacy was observed in tumor xenografts with 177Lu-FAP-2286 than with 177Lu-FAPI-46. When these results are taken together, an increased FAP-binding affinity, improved tumor accumulation, and longer tumor retention are seen to be the main potential advantages of FAP-2286 compared with other FAPI variants. In our study, the results from PET imaging demonstrated that tumor uptake of 68Ga-FAPI-46 and 68Ga-FAP-2286 was comparable at earlier time points, thus indicating that both compounds can be used for imaging of FAP-positive tumors. Further studies with a larger patient population are needed to test the role of 68Ga-FAP-2286 among the existing FAPI derivatives.
Another aim of the present study was to compare tumor uptake and lesion detectability between 68Ga-FAP-2286 and 18F-FDG PET/CT. With respect to primary tumor lesions, the quantitative tumor uptake and TBR were significantly higher with 68Ga-FAP-2286 than with 18F-FDG. This finding corresponds to the results showing that all primary tumors (46/46) were identified with 68Ga-FAP-2286 whereas 9 were missed with 18F-FDG (Supplemental Fig. 1). Consistent with previous FAPI-based imaging studies (7–9), 68Ga-FAP-2286 PET/CT was superior to 18F-FDG PET/CT in gastrointestinal malignancies, including gastric, pancreatic, and hepatic cancer. This result suggests that 68Ga-FAP-2286 PET/CT is promising in the diagnosis of these cancer types for which 18F-FDG PET/CT is inadequate. Regarding the detection of lymph node and visceral metastases, 68Ga-FAP-2286 yielded a higher radiotracer uptake and TBR than 18F-FDG and an improved lesion detectability, particularly of hepatic, bone, and peritoneal metastases. Interestingly, we noted that 1 patient (Supplemental Fig. 2C) with reactive lymph nodes did not exhibit increased 68Ga-FAP-2286 uptake, whereas false-positive 18F-FDG uptake was observed in these nodules. Similar findings have been reported in previous studies (20). Thus, we speculate that 68Ga-FAP-2286 may be more suitable than 18F-FDG for differentiating reactive lymph nodes from tumor metastatic lymph nodes. However, tumor and inflammation differentiation by 68Ga-FAP-2286 PET/CT was not the main aim of this study, although this question should be investigated in future clinical trials.
Overall, the results from this study suggest that 68Ga-FAP-2286 is a promising FAPI molecule for cancer diagnosis, staging, and restaging. Therefore, 68Ga-FAP-2286 PET/CT may contribute to the diagnosis of solid tumors, especially in malignant tumors with low-to-moderate uptake on 18F-FDG PET/CT. The specific cancer types that showed 68Ga-FAP-2286 to be superior to 18F-FDG include gastric, pancreatic, and hepatic cancers; the respective findings were in line with those described in previous publications (7). Specifically, pancreatic and hepatic cancers (especially intrahepatic cholangiocarcinoma) are characterized by intense stromal desmoplastic reactions surrounding cancer cells, and cancer-associated fibroblast are the main effector cells in the desmoplastic reaction (21,22). Furthermore, because of the low background uptake in hepatic parenchyma, FAP imaging was able to detect hepatic tumors with favorable tumor-to-background contrast. Gastric cancer evokes the production and deposition of activated fibroblasts in the submucosa wall (23), resulting in increased 68Ga-FAPI uptake in gastric tumor lesions. Unlike 18F-FDG, very low 68Ga-FAPI uptake was observed in the gastric wall and gastrointestinal tract, which further improved the detectability of gastric cancer. Taken together, high FAP expression and low background activity in abdominal organs are the main reasons and explain why 68Ga-FAP-2286 PET/CT is superior to 18F-FDG in terms of tumor detectability in these tumor entities. Improved tumor detectability may lead to changes in clinical staging and optimization of therapeutic strategies. Moreover, the favorable TBR may improve delineation of gross tumors in radiotherapy and evaluation of the effectiveness of therapy (24,25).
Our study was associated with several limitations. First, few patients underwent paired 68Ga-FAP-2286 and 18F-FDG PET/CT, rendering subgroup analysis of radiotracer uptake per tumor type impracticable. Second, as the subcohort of patients who underwent paired 68Ga-FAP-2286 and 68Ga-FAPI-46 PET/CT was also small (n = 19), only a descriptive comparison was possible. Furthermore, as only 2 patients underwent 68Ga-FAP-2286 PET/CT at multiple time points, we could not fully investigate radiotracer retention in tumors. Prospective studies with a larger patient population are warranted to better explore the role of 68Ga-FAP-2286 in cancer diagnosis and the potential superiority of FAP-2286 with respect to other FAPI derivatives.
CONCLUSION
68Ga-FAP-2286 is a promising FAPI derivative for safe cancer diagnosis, staging, and restaging. It may be superior to 18F-FDG in selected cases, especially for cancers that exhibit low-to-moderate uptake of 18F-FDG, including gastric, pancreatic, and hepatic cancers. In addition, 68Ga-FAP-2286 and 68Ga-FAPI-46 yielded comparable clinical results.
DISCLOSURE
This work was funded by the National Natural Science Foundation of China (82071961), the Key Scientific Research Program for Young Scholars in Fujian (2021ZQNZD016), the Fujian Natural Science Foundation for Distinguished Young Scholars (2022D005), Key Medical and Health Projects in Xiamen (3502Z20209002), and National University of Singapore start-up grants (NUHSRO/2020/133/Startup/08, NUHSRO/2021/097/Startup/13). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 68Ga-FAP-2286 an efficacious alternative for the imaging of FAP-positive tumors?
PERTINENT FINDINGS: In this preliminary report of a single-center, prospective study of the diagnostic accuracy of 68Ga-FAP-2286 PET/CT of solid tumors, all 46 primary tumors in 9 types of cancer were identified with 68Ga-FAP-2286, whereas 9 were missed with 18F-FDG. 68Ga-FAP-2286 yielded a higher radiotracer uptake and TBR than 18F-FDG. 68Ga-FAP-2286 and 68Ga-FAPI-46 yielded comparable clinical results.
IMPLICATIONS FOR PATIENT CARE: 68Ga-FAP-2286 is a promising FAP-inhibitor derivative for safe cancer diagnosis, staging, and restaging.
Footnotes
Published online Sep. 2, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 20, 2022.
- Revision received August 30, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SNMMI Procedure Standard/EANM Practice Guideline for Fibroblast Activation Protein (FAP) PET
- 68Ga-FAP-2286 PET of Solid Tumors: Biodistribution, Dosimetry, and Comparison with 18F-FDG
- Initial Experience with 68Ga-FAP-2286 PET Imaging in Patients with Urothelial Cancer
- Clinical Evaluation of 68Ga-FAPI-RGD for Imaging of Fibroblast Activation Protein and Integrin {alpha}v{beta}3 in Various Cancer Types
- Clinical Evaluation of 68Ga-FAPI-RGD for Imaging of Fibroblast Activation Protein and Integrin {alpha}v{beta}3 in Various Cancer Types