


Abstract
With the largest high-risk prostate cancer (PCa) cohort to date undergoing 68Ga-prostate-specific membrane antigen (PSMA) PET/CT primary staging, we aimed to, first, characterize the metastatic spread of PCa in relation to tumor 68Ga-PSMA uptake and the D’Amico classification and, second, compare 68Ga-PSMA PET/CT findings with radical prostatectomy and pelvic lymph node dissection (PLND) histopathology findings. Methods: The study included 691 consecutive newly diagnosed, biopsy-proven, treatment-naïve, D’Amico high-risk PCa patients primary-staged by 68Ga-PSMA PET/CT. PSMA SUVmax and metastatic findings were compared with prostate-specific antigen level, International Society of Urological Pathology (ISUP) grade, and clinical stage as traditional risk stratification parameters. Moreover, 68Ga-PSMA PET/CT findings were compared with histology findings in radical prostatectomy patients undergoing PLND. Undetected lymph node metastases (LNMs) underwent immunohistochemical PSMA staining. Results: Advanced disease (N1/M1) was observed in 35.3% of patients (244/691) and was associated with increasing prostate-specific antigen level, ISUP grade, and clinical stage. LNMs (N1/M1a) were detected in 31.4% (217/691) and bone metastases (M1b) in 16.8% (116/691). Advanced disease frequencies in patients with ISUP grades 2 and 3 were 10.8% (11/102) and 37.1% (33/89), respectively. Risk of advanced disease for cT2a, cT2b, and cT2c tumors was almost equal (24.2%, 27.9%, and 22.4%, respectively). We observed a weak correlation between SUVmax and biopsy ISUP grade (ρ = 0.21; P < 0.001) and a modest correlation between SUVmax and postprostatectomy ISUP grade (ρ = 0.38; P < 0.001). Sensitivity, specificity, positive and negative predictive value, and accuracy for LNM detection on 68Ga-PSMA PET/CT in the PLND cohort were 30.6%, 96.5%, 68.8%, 84.5%, and 83.1%, respectively. Undetected LNMs either were micrometastases located in the lymph node border or were without PSMA expression. Conclusion: In this high-risk PCa cohort, we identified advanced disease in about one third at diagnosis. ISUP grade was the superior predictor for advanced disease at diagnosis. We found a significant difference in frequency of advanced disease between ISUP grades 2 and 3, as supports the Gleason score 7 subdivision. Interestingly, we observed no significant differences in risk of advanced disease when comparing the different cT2 stages. The undetected LNMs were either PSMA-negative or micrometastases.
Prostate cancer (PCa) is the second most frequently diagnosed cancer and the fifth leading cause of cancer death among men worldwide (1). Accurate primary staging is one of the most important issues for clinical management of PCa patients (2). Prostate-specific membrane antigen (PSMA) is a promising target for personalized medicine in PCa. PSMA is a type II transmembrane glycoprotein upregulated in almost all PCa cells (97.6%) compared with its sparse distribution in benign prostate tissue (3). Thus, PSMA is a very attractive target for imaging and therapy with radionuclides (4). 68Ga-PSMA PET/CT has been demonstrated to outperform conventional imaging modalities for detection of metastasis and recurrent disease (5,6). Detection of biochemical recurrence is the focus of most studies with 68Ga-PSMA PET/CT (7), and the advantage of 68Ga-PSMA PET/CT is especially evident in patients with low prostate-specific antigen (PSA) levels (<1 ng/mL) (8). However, 68Ga-PSMA PET/CT is increasingly used for primary staging of intermediate- and high-risk PCa (6). In a recent review by Koschel et al. (9), 11 studies using 68Ga-PSMA PET/CT for primary staging were included; only a single study, by Yaxley et al. (10) with 1,253 patients, including 597 at high risk, has achieved a cohort of over 200 men.
68Ga-PSMA PET/CT has been used in clinical routine in PCa patients at our department since April 2016, with a high proportion of primary staging. The aim of the present, retrospective, study was to characterize the metastatic spread of PCa on 68Ga-PSMA PET/CT for primary staging of high-risk PCa in relation to tumor 68Ga-PSMA uptake and the D’Amico classification. Additionally, a correlative analysis of 68Ga-PSMA PET/CT findings with histopathology findings was performed on the subgroup of patients undergoing radical prostatectomy (RP) with pelvic lymph node dissection (PLND). Finally, we described undetected lymph nodes (LNs) through immunohistochemical PSMA staining.
MATERIALS AND METHODS
Patient Population
Between April 2016 and March 2019, 1,101 68Ga-PSMA PET/CT scans were performed at the Department of Nuclear Medicine and PET Centre, Aarhus University Hospital, Denmark. The inclusion criteria were newly diagnosed, biopsy-proven, treatment-naïve, high-risk (D’Amico classification (11)) PCa patients referred for primary 68Ga-PSMA PET/CT staging. All 691 high-risk patients were included (Fig. 1). 68Ga-PSMA PET/CT scans with extraprostatic extension or metastasis were discussed at multidisciplinary team conferences with board-certified oncologists, radiologists, urologists, pathologists, and nuclear medicine physicians. PSA level and clinical stage based on digital rectal examination were available for all men. International Society of Urological Pathology (ISUP) grade group (12) evaluation of biopsies was available for 99.9% of patients (690/691). In total, 247 patients underwent RP, with 177 patients having a PLND within the standard template of resection according to the European Association of Urology criteria (13). Seventy patients did not undergo PLND because they had a low preoperative risk of LN involvement (<7%) as assessed by the nomogram of Briganti et al. (14). The number of LNs resected and the number of malignant LNs on histopathology examinations were available for all 177 patients. 68Ga-PSMA PET/CT findings were compared with histopathology findings. Pathology reports were gathered through medical records. The Central Denmark Region Committees on Health Research Ethics approved this retrospective study, and the requirement to obtain informed consent was waived.

Study flow for 68Ga-PSMA PET/CT primary staging of high-risk PCa patients.
68Ga-PSMA PET/CT
All 68Ga-PSMA PET/CT scans were performed approximately 60 min after intravenous injection of 2.14 MBq of 68Ga-PSMA (68Ga-Glu-CO-Lys(Ahx)-HBED-CC) per kilogram of body weight, with low-dose CT for anatomic localization and attenuation correction. All patients were scanned on a Biograph TruePoint PET/CT scanner (Siemens). Images were reconstructed with all available corrections applied (attenuation, scatter, and point-spread function) using the TrueX reconstruction algorithm (4 iterations and 21 subsets; Siemens), a 3-mm gaussian postprocessing filter (xyz), and a voxel size of 2 × 2 × 2 mm.
Image Analysis
All PET/CT scans were analyzed by experienced, board-certified specialists in nuclear medicine, knowing common pitfalls in 68Ga-PSMA PET/CT (15). Image analysis was performed using Hybrid Viewer (Hermes Medical Solutions AB). Images were interpreted according to the PSMA-RADS criteria, version 1.0 (16). SUVmax was measured in primary prostate tumors. Primary tumors were considered avid for 68Ga-PSMA uptake on visual evaluation without a predefined SUV threshold. Regional pelvic LN metastases (LNMs) below the common iliac artery bifurcation taking up 68Ga-PSMA were considered positive as N1 disease according to the PROMISE criteria (17). Similarly, nonregional LNMs above the common iliac artery bifurcation taking up 68Ga-PSMA were considered positive as M1a disease (extrapelvic). PSMA-avid lesions thought to represent bone metastases (BMs) were reported as M1b disease. Lastly, lesions suggesting visceral metastases were considered M1c disease. The number of metastases was recorded along with the SUVmax for each lesion. Advanced disease was defined as having at least 1 extraprostatic PSMA-positive lesion (N1/M1 disease).
Immunohistochemical PSMA Staining
Fourteen formalin-fixed, paraffin-embedded tissue sections (primary tumors and LNs from RP procedures) 4.0 μm thick were used for immunohistochemical staining with monoclonal anti-PSMA (Dako; Agilent Technologies) at a 1:50 dilution. Antigen was retrieved using heat-induced epitope retrieval at pH 8.5 with Cell Conditioner 1 (Ventana), followed by primary antibody incubation. Sections were counterstained with hematoxylin and bluing reagent.
Data Analysis
All variables were summarized using descriptive statistics; values without a normal distribution were described as median and range, with log-transformation and 95% confidence intervals (CIs) in analyses. Univariate and multivariate logistic regression analyses provided odds ratios. Sensitivity, specificity, positive and negative predictive value, and accuracy were calculated according to standard definitions. The names of the statistical tests are provided in the Results section. P values of less than 0.05 were considered statistically significant.
RESULTS
SUVmax Measurements
Patient characteristics are summarized in Table 1. Focal PSMA uptake in the prostate was observed by visual evaluation in 97.3% of men (672/691), whereas 2.7% of men (19/691) had negligible 68Ga-PSMA activity in the primary tumor. Histopathologic assessment of biopsy samples from patients with negligible PSMA uptake revealed adenocarcinomas with no phenotypic deviations from the PSMA-positive patients. Likewise, PSA level, ISUP grade, and clinical stage parameters matched those of PSMA-positive disease. Correlations between SUVmax and biopsy ISUP grade and between SUVmax and postprostatectomy ISUP grade are provided in Figures 2A and 2B, respectively. Area under the receiver-operating-characteristic curve for SUVmax to predict an ISUP grade of 2 or less and an ISUP grade of more than 2 in biopsies was 0.65 (95% CI, 0.56–0.74). With an optimal SUVmax cutoff of 11.4, the sensitivity and specificity were 51.2% and 77.4%, respectively. Primary tumor SUVmax was significantly higher in patients with at least 1 PSMA-positive metastatic lesion than in patients with localized disease only, with a median ratio of 1.62 (95% CI, 1.47–1.80) (Fig. 2C). Median SUVmax with 95% CI for primary tumors in relation to ISUP grades and advanced disease is provided in Table 2. SUVmax and PSA level were moderately positively correlated (Fig. 2D). Median SUVmax for primary tumors and different metastatic sites is accessible in Table 3. A relatively uniform PSMA uptake across different tissues was observed, with lower uptake in visceral metastases as the only exception.
Study Group Characteristics and Odds Ratios (ORs) for Having Advanced Disease Compared with Reference
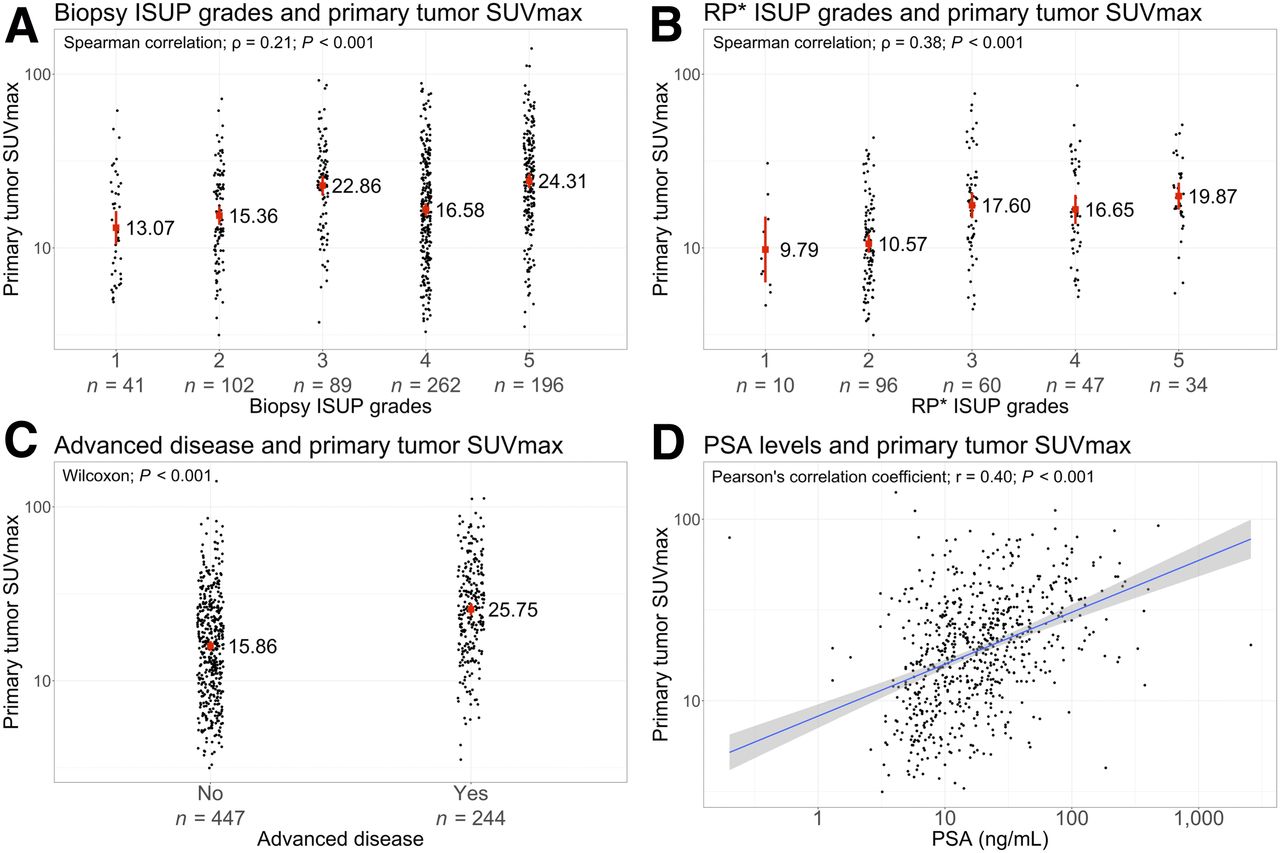
(A) Correlation between SUVmax of primary tumors and ISUP grade from transrectal ultrasound–guided or MRI-guided biopsy. Data are median. (B) Correlation between SUVmax of primary tumors and RP ISUP grade. Data are median. (C) Primary tumor SUVmax in correlation with advanced disease (N1/M1). Data are median. (D) Correlation between SUVmax of primary tumors and PSA at diagnosis. Data are line of best fit with 95% CI. *Radical prostatectomy.
Primary Tumor SUVmax with 95% CI in Relation to ISUP Grade and Advanced Disease
SUVmax of Different Lesion Sites
Advanced Disease
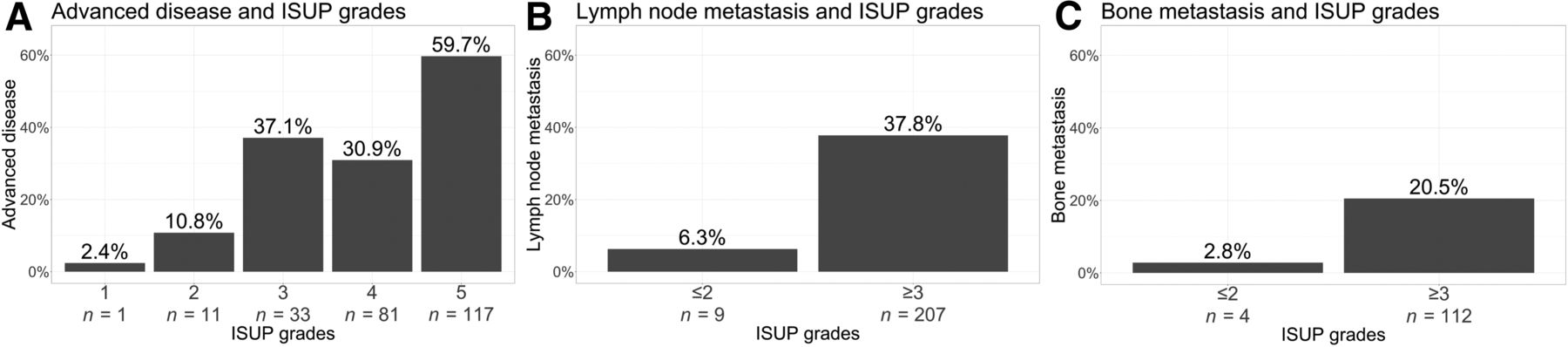
Advanced disease was observed in 35.3% of patients (244/691) and increased greatly with increasing PSA level, ISUP grade, and clinical stage (Figs. 3A, 4A, and 5). Odds ratios (univariate and multivariate logistic regression) for the increasing risk of advanced disease per increase in measurement (PSA level, ISUP grade, and clinical stage) are provided in Table 1.

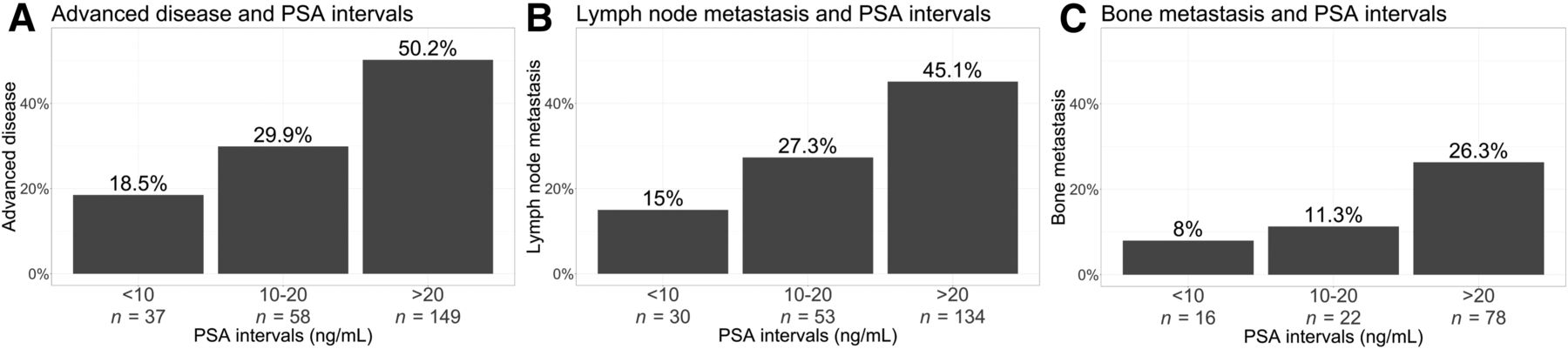
Occurrence of advanced disease (N1/M1) (A), LNMs (N1/M1a) (B), and BMs (M1b) (C) according to PSA interval.
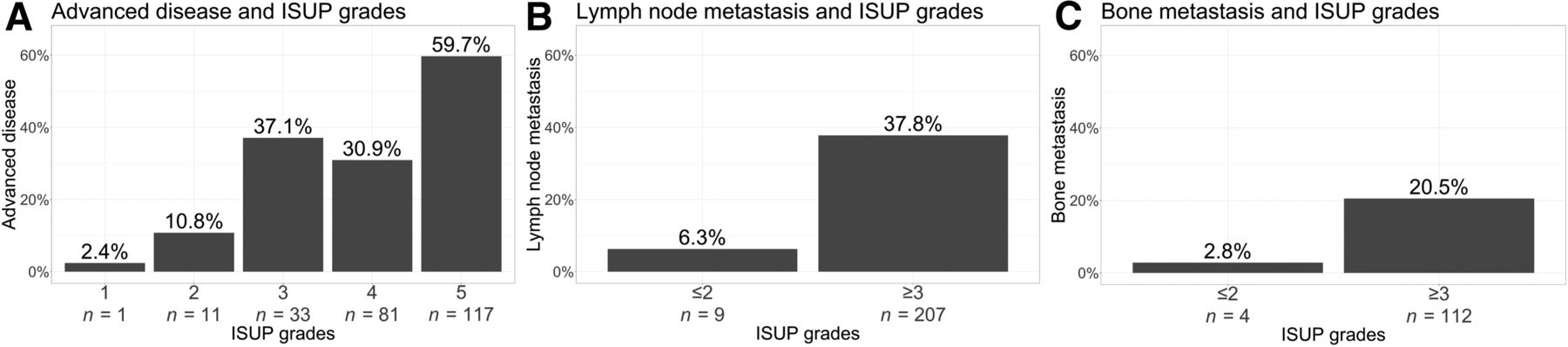
Incidence of advanced disease (N1/M1) (A), LNMs (N1/M1a) (B), and BMs (M1b) (C) according to ISUP grade.

Presence of advanced disease (N1/M1) according to clinical stage.
LNM
Regional and nonregional LNMs were detected in 31.4% of patients (217/691). Of these patients, 50.7% (110/217) presented with regional pelvic LNMs alone (N1, M0) whereas 49.3% (107/217) had nonregional LNMs. Only a single patient (0.5%, 1/217) had nonregional LNMs without having concurrent regional LNMs (N0, M1a). Similar to advanced disease in general, increasing PSA level, ISUP grade, and clinical stage were associated with increased risk of LNMs (Figs. 3B and 4B).
Bone and Visceral Metastasis
BMs (M1b) were identified in 16.8% of men (116/691), and only 22.5% of these men (26/116) presented with BMs exclusively. Most patients (77.6%, 90/116) with BMs had concurrent LNMs. BMs were present to a larger extent in patients with increasing PSA levels, ISUP grades, and clinical stages (Figs. 3C and 4C). Two percent of patients (13/691) presented with visceral metastases (M1c); 12 of these had clinical stage cT3a-cT4, and 10 of these had an ISUP grade of at least 4.
PLND
RP with PLND was performed on 177 patients. All RP specimens confirmed PCa. In terms of preoperative biopsy ISUP grade, 38.1% of patients (94/247) were downgraded after RP, and 18.2% of patients (45/247) were upgraded. More than 2,500 LNs were resected and histologically assessed. The calculated per-patient sensitivity, specificity, positive and negative predictive value, and accuracy for detection of LNMs in this subgroup on 68Ga-PSMA PET/CT are provided in Table 4. The median histologic size of LNMs in the 11 patients identified on PET/CT (7.0 mm; range, 2.0–16.0 mm) was larger than in the 25 patients with no visible 68Ga-PSMA uptake in LNMs (3.0 mm; range, 1.0–11.0 mm), with a median ratio of 2.07 (95% CI, 1.39–3.10) (Wilcoxon Mann–Whitney U test; P = 0.003).
Histopathologic Coherence Between PSMA-Positive or -Negative LNs and Pathologic Verification in Patients with PLND
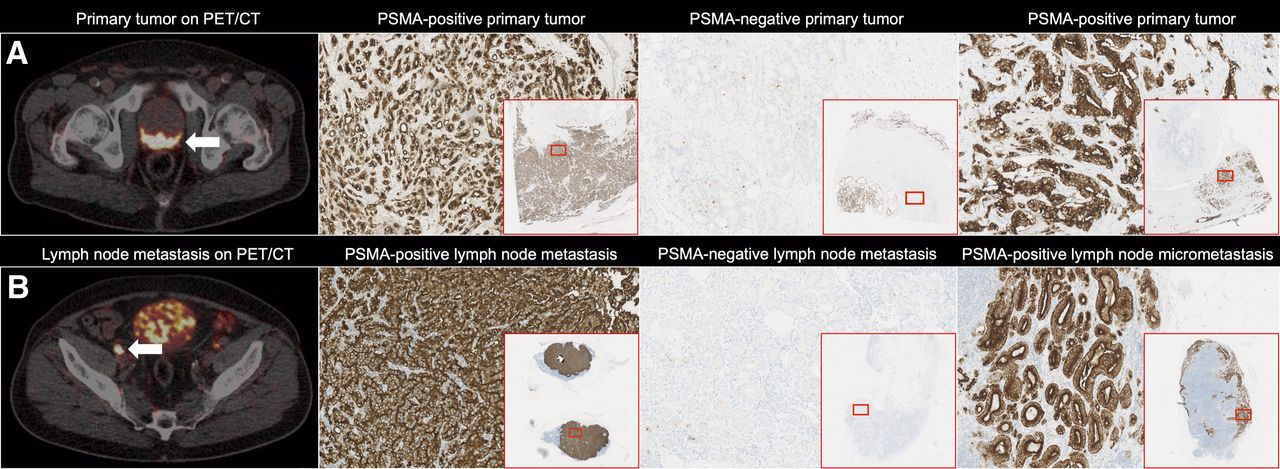
An LNM true-positive for 68Ga-PSMA uptake and its corresponding primary tumor on PET/CT (Fig. 6) was immunohistochemically stained for PSMA expression. In addition, this was also performed on the 6 histopathologically verified LNMs larger than 5.0 mm that went undetected on 68Ga-PSMA PET/CT and their corresponding primary tumors. One undetected cancer was PSMA-negative in both primary tumor and metastasis, and the remaining undetected LNMs were micrometastases characteristically located in the border of the LN cortex.
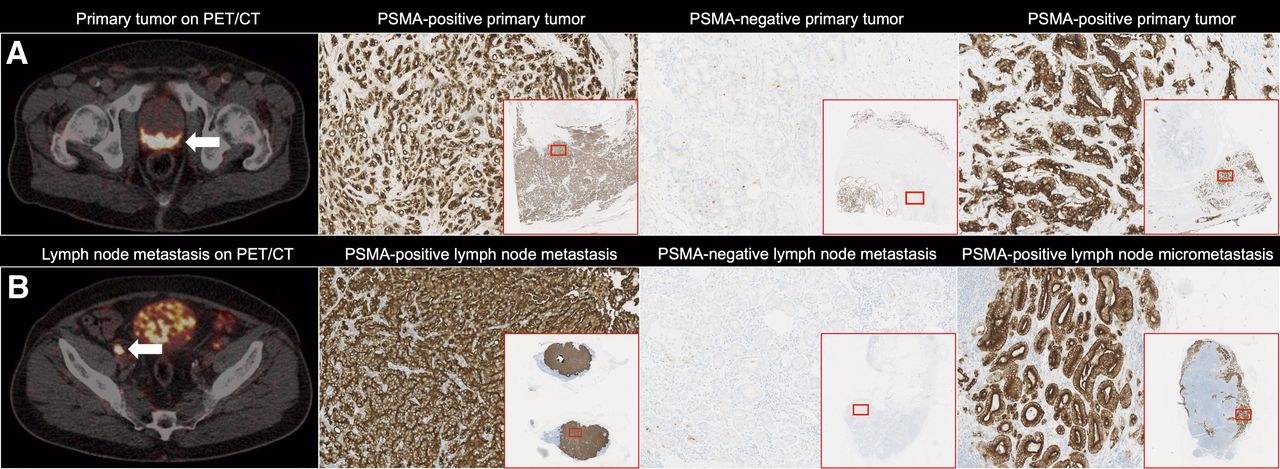
(A) Primary prostate tumors. From left: 68Ga-PSMA PET/CT (arrow), PSMA-positive immunohistochemical staining of primary tumor from previous image, PSMA-negative immunohistochemical staining of primary tumor, and PSMA-positive immunohistochemical staining of primary tumor. (B) LNMs from corresponding primary tumors in A. From left: LNMs on 68Ga-PSMA PET/CT (arrow), PSMA-positive immunohistochemical staining of true-positive LNMs from previous image, PSMA-negative immunohistochemical staining of undetected LNMs, and PSMA-positive immunohistochemical staining of undetected LN micrometastasis, characteristically located in the border of the LN cortex.
DISCUSSION
With 691 patients, the present study included the largest—to our knowledge—high-risk cohort reported to date using 68Ga-PSMA PET/CT for primary PCa staging and furthermore had a high proportion of patients with metastatic disease. Hence, the study was able to characterize the metastatic spread of PCa assessed by 68Ga-PSMA PET/CT and the relationship with traditional risk stratification parameters (PSA level, biopsy ISUP grade, and clinical stage).
The SUVmax of the primary tumor in 68Ga-PSMA PET/CT has previously been proposed as a surrogate marker of clinically significant PCa, with higher values in tumors of higher ISUP grade than in tumors of lower ISUP grade (18). In our cohort of high-risk patients only, we found a trend toward an increasing median SUVmax with increasing ISUP grade in both biopsies and RP specimens. However, when plotting all patients, we clearly saw that there was a massive overlap between groups. The fact that even the lowest SUVmax can correspond to ISUP grades of 4 and 5 questions the applicability of 68Ga-PSMA SUVmax as a marker of aggressiveness (Figs. 2A and 2B). Uprimny et al. (19) found a greatly increased SUVmax in patients with ISUP grades of 4 or 5, compared with ISUP grades of 3 or less, with medians of 19.5 (range, 5.3–65) and 6.8 (range, 2.7–35.1), respectively. In accordance with Demirci et al. (18), the natural separation in our cohort would be between ISUP grades 2 and 3, as the SUVmax of ISUP grade 3 was as high as that of ISUP grade 5. Similarly, primary tumor SUVmax was 62% higher in patients with advanced disease than in patients with localized disease in our cohort (Fig. 2C). Furthermore, PSA level correlates greatly with total metastatic burden in the body and is not dependent solely on the activity in the primary tumor as included in our analyses (Fig. 2D). This is a potential confounder in the correlation between SUVmax and PSA level.
Approximately 35% (244/691) of patients presented with advanced disease. As seen in Table 1, odds ratio steadily increased for rising ISUP grade and turned out to be the far superior predictor for advanced disease at diagnosis. cT3 and cT4 disease on digital rectal examination was also an apparent predictor of advanced disease. On the other hand, PSA level was clearly inferior to the other 2 stratification parameters in predicting advanced disease in our cohort, because of the relatively high rate of metastasis (18.5%, 37/200) in the reference group, with a PSA level of less than 10 ng/mL.
We observed a striking difference in the rate of advanced disease between patients with ISUP grade 2 (10.8%, 11/102) and patients with ISUP grade 3 (37.1%, 33/89). This difference supports the subdivision of Gleason score 7 into ISUP grades 2 and 3 (Gleason score 3 + 4 and 4 + 3, respectively) (20,21), with ISUP grade 3 potentially needing to be treated as a higher-risk disease. According to the classification of D’Amico et al. (11), the subdivision of cT2 by digital rectal examination stratifies patients into low-risk (cT2a), intermediate-risk (cT2b), and high-risk (cT2c) groups. Interestingly, we observed no differences in the risk of advanced disease when comparing the different cT2 stages (Fig. 5). This observation indicates that a 3-way subdivision of cT2 may not provide additional information on the risk of advanced disease once high-risk disease has already been established.
We identified LNMs (N1/M1a) in 31.4% of patients (217/691), a markedly higher percentage than in a recent study by Yaxley et al. (10) (8.5%, 107/1,253), yet they included intermediate-risk patients as well. We observed only a single patient (0.5%, 1/217) who had nonregional LNMs without having concurrent regional LNMs (N0, M1a), consistent with the traditional LN spreading pattern from the pelvis and upward via regional lymphatic vessels (22). With 16.8% of patients having BMs (116/691), this was by far the most common site of hematologic spread. In a recent cross-sectional study of 220 patients with newly diagnosed PCa (23), 3.2% of patients (4/124) with a PSA level of less than 10 ng/mL and 9.6% (5/52) of patients with a PSA level of 10–20 ng/mL displayed BMs, compared with 8.0% (16/200) and 11.3% (22/194), respectively, in our high-risk–only cohort.
In the subcohort of patients who underwent RP with concomitant PLND, we achieved a consistently high per-patient specificity of 96.5%, as reported in most previous papers (>90%) (24). Conversely, 68Ga-PSMA PET/CT detected only 11 of 36 of the histologically confirmed LNMs in our population, revealing a per-patient sensitivity of 30.6%. However, this was a highly selected subpopulation with a massive selection bias, as the patients scheduled for surgery are usually deemed free of metastatic disease by 68Ga-PSMA PET/CT beforehand. Our sensitivity was on a par with comparable studies (RP with PLND) reporting sensitivities spanning from 33% to 42% (25–28). This selection bias is illustrated by the much higher sensitivity found by Hofman et al. in their recent prospective study of 68Ga-PSMA PET/CT in a less preselected group (6). Furthermore, we observed a large difference in median histologic size for the LNMs that were detected (7.0 mm; range, 2.0–16.0) and undetected (3.0 mm; range, 1.0–11.0) by 68Ga-PSMA PET/CT. In a study by Budäus et al. (28), the median size of LNMs detected and undetected by 68Ga-PSMA PET/CT was 13.6 versus 4.3 mm (P < 0.05). On histopathology examination of the undetected LNMs larger than 5.0 mm, we observed 1 PSMA-negative metastasis seeded from a PSMA-negative primary tumor (Fig. 6). Characteristic of the rest of undetected LNMs was the fact that the metastasis infiltrated only the border of the LN cortex (Fig. 6). Even though the pathologic measurement of this particular LNM was 8.0 mm in longitudinal diameter, the actual volume of the metastasis was relatively small and hence apparently under the detection limit of 68Ga-PSMA PET/CT. A recent study by Jilg et al. (29) has also described the importance of the volume of tumor deposits within the LN for 68Ga-PSMA positivity on PET/CT.
There are some limitations to the present study. First, the retrospective nature of the study may infer potential bias. Moreover, our population was high-risk–only, and hence the findings are not valid for all PCa patients. Third, many metastases reported on 68Ga-PSMA PET/CT were without confirmatory biopsies; thus, we relied solely on imaging, with the known pitfalls considered. However, in the subgroup with PLND histology, LNs were available.
CONCLUSION
We identified extraprostatic disease in 35.3% (244/691) of high-risk PCa patients at the time of diagnosis. As expected, the proportion of advanced disease increased with higher PSA level, ISUP grade, and clinical stage. However, ISUP grade turned out to be the far superior predictor for advanced disease at diagnosis. We found a striking difference in the proportion of advanced disease between ISUP grade 2 (3 + 4) and 3 (4 + 3) (10.8%, 11/102, and 37.1%, 33/89, respectively), which supports a subdivision of Gleason score 7. Interestingly, we observed no differences in the risk of advanced disease when comparing the 3 different clinical T2 stages.
DISCLOSURE
This work was financially supported by the Danish Cancer Society. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What characterizes the initial metastatic findings of 68Ga-PSMA PET/CT for primary staging of high-risk PCa, and which traditional risk stratification parameters predict the risk of having advanced disease at diagnosis?
PERTINENT FINDINGS: In a retrospective study comprising 691 newly diagnosed, high-risk PCa patients referred for primary 68Ga-PSMA PET/CT staging, advanced disease was observed in 35% at diagnosis, with ISUP grade being the superior predictor. A significant difference was observed between ISUP grades 2 and 3, yet no significant differences were found when comparing the different cT2 stages.
IMPLICATIONS FOR PATIENT CARE: The present study provided knowledge about risk stratification parameters, which may help improve the future prediction of advanced disease.
Footnotes
Published online May 22, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 21, 2020.
- Accepted for publication May 5, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Considerations Surrounding the Sentinel Lymph Node in Prostate Cancer and Unanswered Questions
- Reply: Considerations Surrounding the Sentinel Lymph Node in Prostate Cancer and Unanswered Questions
- Diagnostic Performance of [18F]AlF-Thretide PET/CT in Patients with Newly Diagnosed Prostate Cancer Using Histopathology as Reference Standard
- 68Ga-PSMA-11 PET/MRI in Patients with Newly Diagnosed Intermediate- or High-Risk Prostate Adenocarcinoma: PET Findings Correlate with Outcomes After Definitive Treatment
- Utility of 18F-rhPSMA-7.3 PET for Imaging of Primary Prostate Cancer and Preoperative Efficacy in N-Staging of Unfavorable Intermediate- to Very High-Risk Patients Validated by Histopathology
- Head-to-Head Comparison of 68Ga-Prostate-Specific Membrane Antigen PET/CT and Ferumoxtran-10-Enhanced MRI for the Diagnosis of Lymph Node Metastases in Prostate Cancer Patients