


Abstract
Given the high frequency of liver metastases in neuroendocrine tumor patients, we aimed to determine whether hepatic intraarterial administration of 90Y-DOTATOC peptide receptor radionuclide therapy (PRRT) would increase treatment efficacy while reducing systemic toxicity compared with systemic toxicity from intravenous administration as previously reported in the literature. Methods: PRRT-naïve adult neuroendocrine tumor patients with liver-dominant metastases were enrolled in a prospective single-center, open-label pilot study. The patients underwent baseline PET/CT using intravenous 68Ga-DOTATOC. Then, 3.5 ± 0.2 GBq (94.7 ± 5.4 mCi) of 90Y-DOTATOC were administered into the proper hepatic artery over 30 min. The first 5 patients also received intraarterial 68Ga-DOTATOC and underwent PET/CT. All patients were followed for response (RECIST, version 1.1) (primary aim 2, safety) and toxicity (Common Terminology Criteria for Adverse Events, version 4.0) (primary aim 1, efficacy) for at least 6 mo, with optional follow-up for up to 1 y. In the subset of 5 patients who underwent both intravenous and intraarterial 68Ga-DOTATOC PET/CT, tumor SUVmax was compared between intravenous and intraarterial administration for hepatic tumors, intrahepatic tumors, and uninvolved background organs (secondary aim, intravenous vs. intraarterial uptake). Results: The study was terminated after a planned analysis of the first 10 patients because of lack of efficacy. The best response was stable disease in 90% (9/10 patients) and progressive disease in 10% (1/10 patients) at 3 mo, and stable disease in 8 of 10 patients and progressive disease in 2 of 10 patients at 6 mo. One additional patient developed progressive disease after the 6-mo follow-up period but within the optional 1-y follow-up period. No partial response or complete response was observed. The 2 patients with the highest liver tumor burden died within 6 mo of treatment, with treatment considered a possible contributor. Patients who received intraarterial administration failed to demonstrate higher uptake by hepatic metastases than patients who received intravenous administration, with a median intraarterial-to-intravenous SUVmax ratio of 0.81 (range, 0.36–2.09) on a lesion level. Conclusion: Our study found that administration of PRRT via the proper hepatic artery did not reproduce the increase in hepatic tumor uptake that was previously reported. In addition, the single treatment using 90Y-DOTATOC did not induce tumor shrinkage, indicating that more treatment cycles may be required. Possible safety concerns in patients with a high liver tumor burden should inform patient selection for future studies.
- gastrointestinal oncology
- radionuclide therapy
- liver-directed therapy
- neuroendocrine tumors
- somatostatin receptor PET
- targeted radionuclide therapy
Peptides targeting the somatostatin receptor (SSTR), which is commonly overexpressed in gastroenteropancreatic neuroendocrine tumors (NETs) but not in normal tissues, can be radiolabeled to deliver targeted radiation therapy (1). Peptide receptor radionuclide therapy (PRRT) carries radioactivity inside tumor cells by triggering internalization of the SSTR-radiolabeled analog complex. In patients with metastatic midgut grade 1 or 2 NETs, PRRT prolongs radiographic progression-free survival and improves quality of life compared with high-dose octreotide alone (2–4); a trend toward improved overall survival was also noted (5–8).
Toxicity from intravenous PRRT is due to off-target exposure, primarily to bone marrow and kidneys (2), as demonstrated on dosimetry studies (9). The radiation dose in PRRT is due to β-particles emitted by the radionuclide, typically either 177Lu or 90Y. 90Y has a higher-energy β-particle than 177Lu and thus may be more effective for treating bulky tumors, but intravenous administration of 90Y-based PRRT has been associated with increased rates of marrow toxicity compared with 177Lu-based PRRT (10).
Liver is the most common site of gastroenteropancreatic NET metastases, affecting up to 75% of patients at diagnosis (11). Directly targeting the liver with intraarterial 90Y-based PRRT is appealing as it has potential to increase the dose to hepatic metastases while decreasing systemic toxicity. Preliminary work with 68Ga-DOTATOC in Heidelberg demonstrated increased hepatic tumor uptake when administered intraarterially compared with intravenously, hypothesized to be due to increased first-pass extraction (12). A study using small doses (<172 MBq [4.6 mCi]) of the SSTR analog 111In-DTPAOC also demonstrated increased (though variable) hepatic tumor uptake with intraarterial administration compared with intravenous (13).
Given these promising findings, the current study was undertaken to determine whether a single intraarterial administration of 90Y-DOTATOC into the proper hepatic artery would achieve higher hepatic intratumoral concentrations of radionuclide (measured by SUVmax) and provide more effective treatment of hepatic metastases while possibly reducing marrow and renal toxicity.
MATERIALS AND METHODS
Patient Selection
This was a prospective single-center, open-label pilot study (NCT03197012) approved by the local Institutional Review Board for patients with biopsy-proven well-differentiated NET liver metastases from any site of origin, and of any World Health Organization grade and any Ki-67, and with either functional or nonfunctional status. The presence of tumoral SSTR positivity was required as demonstrated on prior SSTR PET, with 10%–70% of the liver parenchyma replaced by tumor. Patients were required to have liver-dominant disease, which was defined as a qualitatively greater volume of receptor-positive tumor in the liver than outside the liver as determined by a nuclear radiologist. Disease progression within the past 12 mo as defined by RECIST, version 1.1, was also required (14). The presence of low-volume extrahepatic disease was not considered a disqualifier. Other inclusion criteria were unresectable liver metastases, Eastern Cooperative Oncology Group performance status 0–2, and age greater than 18 y.
Exclusion criteria were serious intercurrent illness, impaired renal function (glomerular filtration rate < 60 mL/min), impaired liver function (including total bilirubin > 1.8 mg/dL and serum albumin < 3.0 g/dL), impaired bone marrow reserve (hemoglobin concentration < 6.0 g/dL, white blood cell count < 3.0 × 109/L, or platelets < 100,000/μL), portal vein thrombosis, prior PRRT, a contraindication to hepatic arteriography, prior external-beam radiation treatment to the liver or to more than 25% of the bone marrow, intracranial metastases, systemic therapies other than SSTR agonists (SSAs) (e.g., mammalian-target-of-rapamycin inhibitors or sunitinib) within 4 wk before enrollment, liver-directed therapy within 12 wk before enrollment, and an inability to withhold short-acting SSAs for 48 h before enrollment or long-acting SSAs for 4 wk before enrollment. All patients provided written informed consent before participation.
Intravenous 68Ga-DOTATOC Imaging
68Ga-DOTATOC was produced as previously described using 25 μg of precursor (15). Patients underwent 68Ga-DOTATOC PET/CT up to 4 wk before treatment. A 207 ± 33 MBq (5.6 ± 0.9 mCi) dose of 68Ga-DOTATOC was injected intravenously. PET/CT was performed 63 ± 7 min after injection on either a Biograph 16 (Siemens Healthcare) or a Discovery VCT (GE Healthcare). PET was then performed with ten 3-min bed positions, extending from the vertex to the mid thighs with the arms overhead. PET data were reconstructed using 4 iterations, 14 subsets, and a matrix of 168 × 168. The PET transaxial field of view was 620 mm, and the axial slice thickness was 5.0 mm.
90Y-DOTATOC Administration
Long-acting octreotide was withheld 4 wk before treatment, and short-acting octreotide was withheld 24 h before treatment. For renal protection, 2 L of Aminosyn II, 8.5% (amino acid solution, 920 mOsmol/L; Abbott Laboratories), were infused intravenously over a minimum of 4 h, beginning 30 min before administration of the 90Y-DOTATOC dose (2). Compounded solutions containing only positively charged amino acids were not yet available for use at the time of this study.
90Y-DOTATOC was produced in-house using good manufacturing practices. A maximum of 115 μg of precursor was applied per synthesis using the ModularLab PharmTracer (Eckert and Ziegler). The precursor was obtained from ABX Advanced Biochemical Compounds, and 90Y-chloride solution was purchased from PerkinElmer. Under fluoroscopic guidance, 3.5 ± 0.3 GBq (94.7 ± 7.5 mCi) of 90Y-DOTATOC were administered through a proper hepatic artery catheter over 30 min. One patient with variant hepatic artery anatomy (replaced left hepatic artery) received 90Y-DOTATOC to the predominantly involved right liver lobe via the right hepatic artery. The first 5 patients also received intraarterial 68Ga-DOTATOC via the hepatic artery catheter over 30 min concurrently with the therapeutic dose. Those 5 patients underwent subsequent posttreatment PET/CT (same imaging protocol as above) approximately 90 ± 20 min from the midpoint of the intraarterial infusion.
Analysis Plan
The study had 2 primary endpoints. The first was response rate for treated liver lesions at 3 and 6 mo, based on a change in lesion size meeting the threshold for complete response or partial response by RECIST 1.1 (14). Baseline and follow-up liver MRI was evaluated by a fellowship-trained abdominal radiologist for changes in the size of hepatic metastases using RECIST 1.1 (14). The second primary endpoint was safety based on laboratory values and clinical evaluation, using the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 4.0 (16).
The secondary endpoint, evaluable in only the subset of patients who received posttreatment 68Ga-DOTATOC PET/CT, was a change in the SUVmax for target liver lesions, extrahepatic lesions, and an uninvolved organ (spleen, or left kidney if spleen was not present) between intravenous and intraarterial administrations. From pre- and posttreatment 68Ga-DOTATOC PET/CT, changes in SUVmax were determined for up to 5 hepatic metastases and up to 5 extrahepatic metastases (if present). For uninvolved-organ measurements, a volume of interest at least 20 mm in diameter was used. Comparisons between intraarterial and intravenous SUVmax for hepatic tumors, intrahepatic tumors, and the uninvolved organ were performed using a Wilcoxon signed-rank test.
All patients underwent follow-up laboratory tests, symptom inventories, and liver-protocol MRI every 12 wk for a minimum 24 wk or until disease progression.
For the primary endpoint, the study was powered to compare an expected objective response rate of 19% with a comparator objective response rate of 4% (based on everolimus and sunitinib estimates). The NETTER-1 trial (2) was selected as a comparator given that it was the only randomized data for PRRT to date. Assuming a type 1 error of 0.05 and power of 80%, we determined that 32 patients needed to be treated. An interim safety and efficacy analysis was planned after the first 10 patients.
Statistical analysis was performed using R and Excel (version 2016; Microsoft) for Mac (Apple).
RESULTS
Safety
Ten patients were enrolled in the study, with demographics and NET history as summarized in Table 1. The study was terminated after a planned interim analysis before the accrual of additional patients because of evidence of minimal treatment efficacy. During the study, 5 of 10 patients experienced no adverse effects or mild (CTCAE grade 1) adverse effects, 4 of 10 developed moderate (CTCAE grade 2) adverse effects (anorexia, n = 2; elevated alkaline phosphatase, n = 1; elevated total bilirubin and anemia, n = 1; upper respiratory infection deemed to be unrelated to treatment, n = 1), and 3 of 10 developed severe non–life-threatening (CTCAE grade 3) adverse effects, which were deemed unrelated to treatment (cholangitis in a patient who previously had bouts of cholangitis, urinary tract infection, and hyponatremia and pulmonary embolism in a patient with a history of both) (Table 2). Most grade 1 adverse events were considered due to the amino acid administration rather than the treatment drug. There were no adverse effects on renal function. No patient developed CTCAE grade 4 (severe and life-threatening) adverse effects. Two of 10 patients died (CTCAE grade 5) during the study. Though it was not clear that the deaths were related to treatment, the possibility was considered and the deaths were attributed as such.
Patient Characteristics
Adverse Events
Both patients who died during the study had extensive hepatic metastatic disease. The first patient was diagnosed with a grade 2 gastric NET (Ki-67, 5%–15%) that progressed on SSAs, with 65%–70% of the liver replaced by metastases. Within a week of treatment, the patient developed abdominal pain, loss of appetite, and transient hyperbilirubinemia (peak total bilirubin, 1.7 mg/dL 6 d after treatment that resolved to 0.6 mg/dL 2 wk later). These effects were considered treatment-related and possibly due to transient biliary obstruction caused by tumor swelling. The patient did not experience other signs of liver failure such as ascites or subsequent elevations in liver function test results. One month after treatment, the patient became dehydrated and developed a deep venous thrombosis, pulmonary embolism, hyponatremia, and herpes zoster. Symptoms improved with supportive care, although the patient continued to have nausea and weight loss (also present at baseline before treatment). Five months after treatment, the patient deteriorated further, was placed on hospice care, and passed away. On review, it remained unclear whether the death was due to intraarterial PRRT, progressive disease, or other causes.
The second patient had a NET of unknown primary with a Ki-67 of less than 1%. Approximately 65% of his liver was replaced by tumor. He had previously been treated with octreotide acetate (Sandostatin; Novartis), everolimus, sunitinib, capecitabine, temozolomide, and 90Y radioembolization to both lobes of the liver. Immediately after treatment, he developed a urinary tract infection, as well as recurrence of lower-extremity edema, which had been intermittently present previously and was treated with furosemide. After treatment, the patient’s alkaline phosphatase increased from 176 IU/L to a peak of 354 IU/L, with a peak total bilirubin of 1.2 IU/L. Six weeks after treatment, the patient was hospitalized with pneumonia and supraventricular tachycardia. Ten weeks after treatment, the patient was admitted to hospice, and he passed away 2 wk later (3 mo after treatment). As with the previous patient, it was unclear whether the death was due to intraarterial treatment, progressive disease, or other causes. However, because a high dose of radiation to the liver could not be entirely excluded as a cause of the patients’ deaths, both were deemed possibly related to treatment. The other 8 patients remained alive at a minimum of 2 y after treatment.
Efficacy
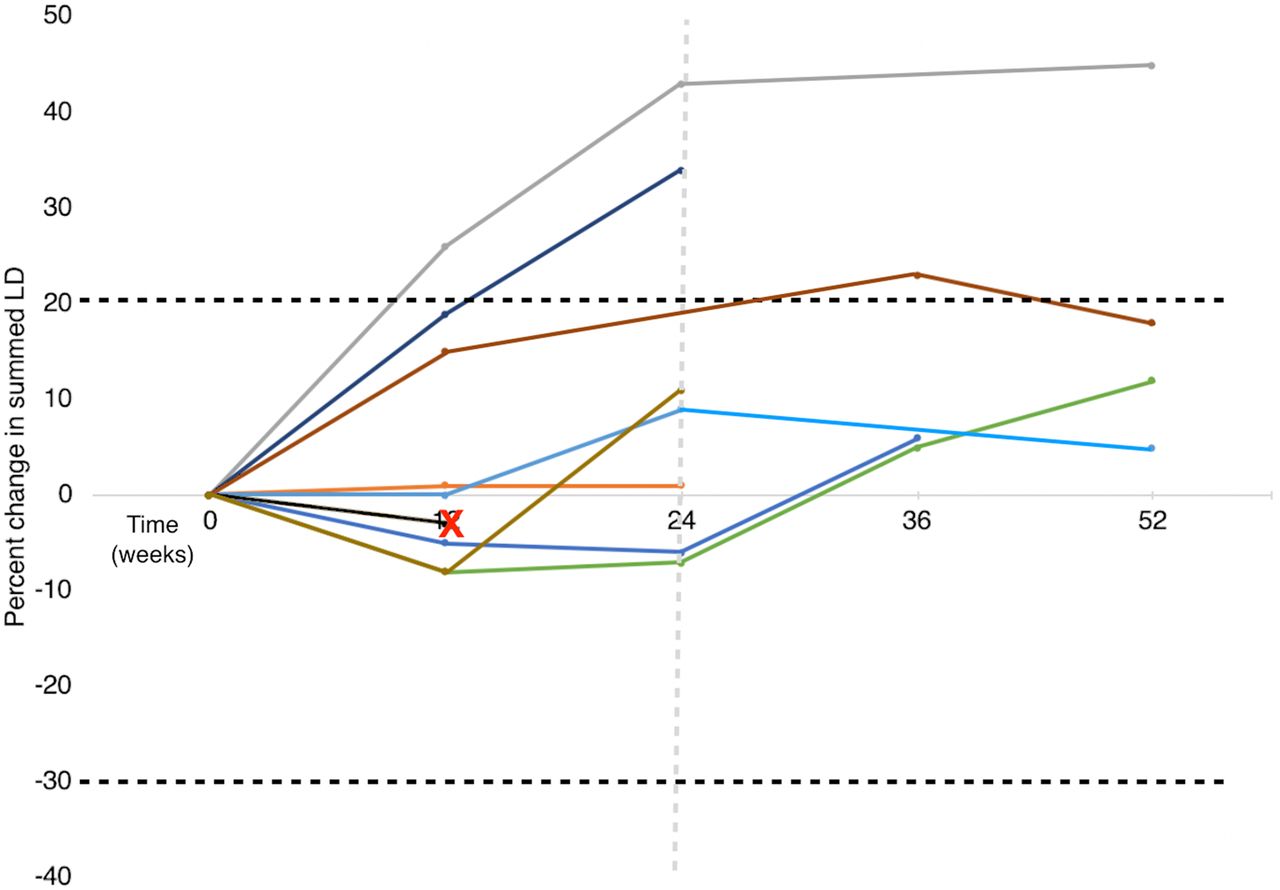
During the follow-up period (24 wk), the best response was stable disease in 70% of subjects (7/10) and progressive disease in 20% (2/10) (Fig. 1). One of the 10 developed progressive disease at 12 wk, and a second patient developed progressive disease at 24 wk. No patients met the criteria for partial response or complete response during the follow-up period. Although 5 patients experienced a slight decline in tumor size from baseline to 12 wk after treatment, the decrease in summed longest dimension (<10% in all cases) was not large enough to meet the criteria for partial response.
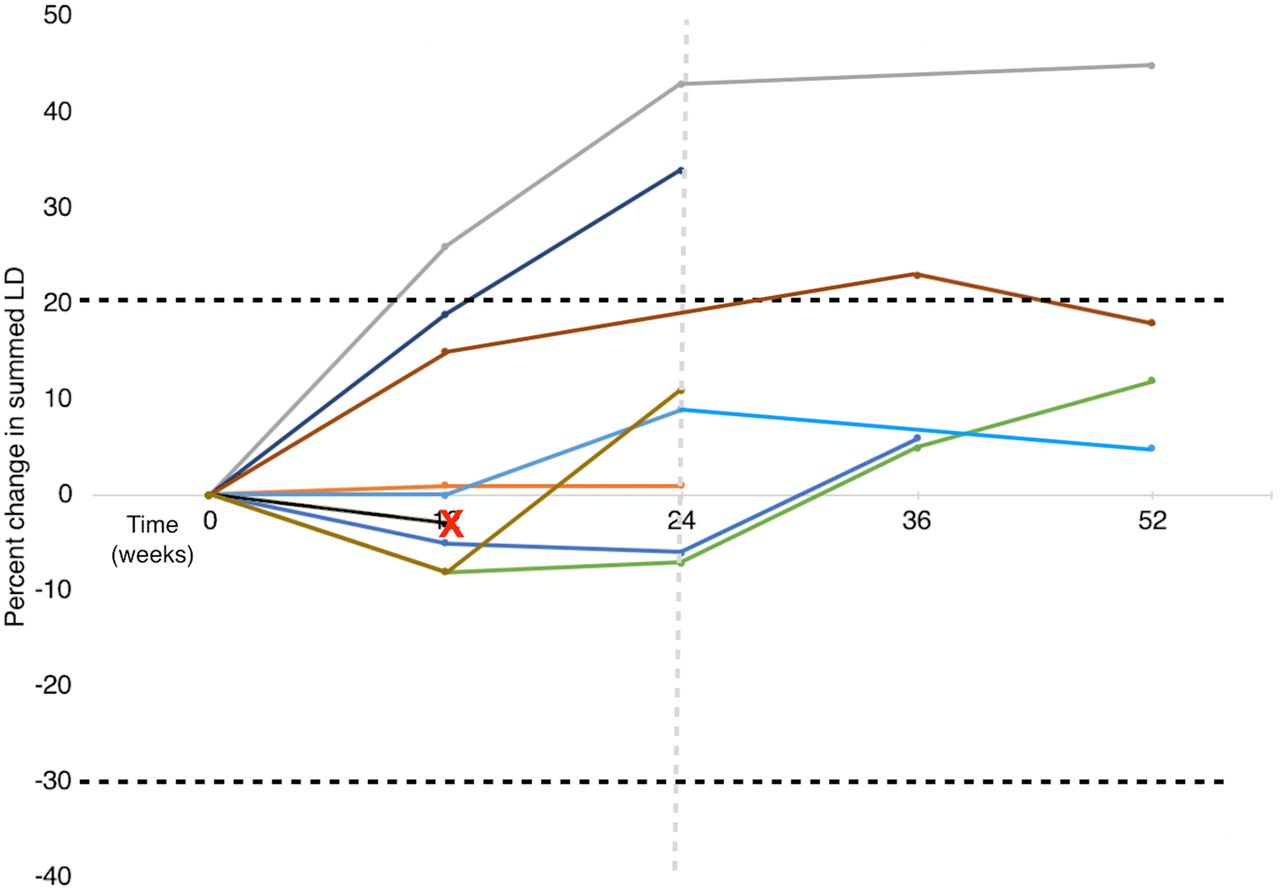
Percentage change in summed longest diameter of target lesions per RECIST 1.1 criteria. Over course of planned follow-up period (24 wk), 2 patients met criteria for progressive disease. Over longer optional 1-y follow-up period, 1 additional patient met criteria for progressive disease. No patients met criteria for partial response during follow-up period. Two patients who ultimately died had identical changes in summed longest diameter of their target lesions at 12 wk, after which both were lost to imaging follow-up (black line with red X). Black dotted lines = thresholds for progressive disease and partial response per RECIST 1.1 criteria; gray dotted line = planned follow-up period in study protocol. LD = longest diameter.
Over the optional longer follow-up period of 1 y, all remaining patients experienced an increase in tumor size from baseline, with 1 additional patient meeting the criteria for progressive disease (Fig. 1).
Change in Radiotracer Uptake with Intraarterial Versus Intravenous Administration
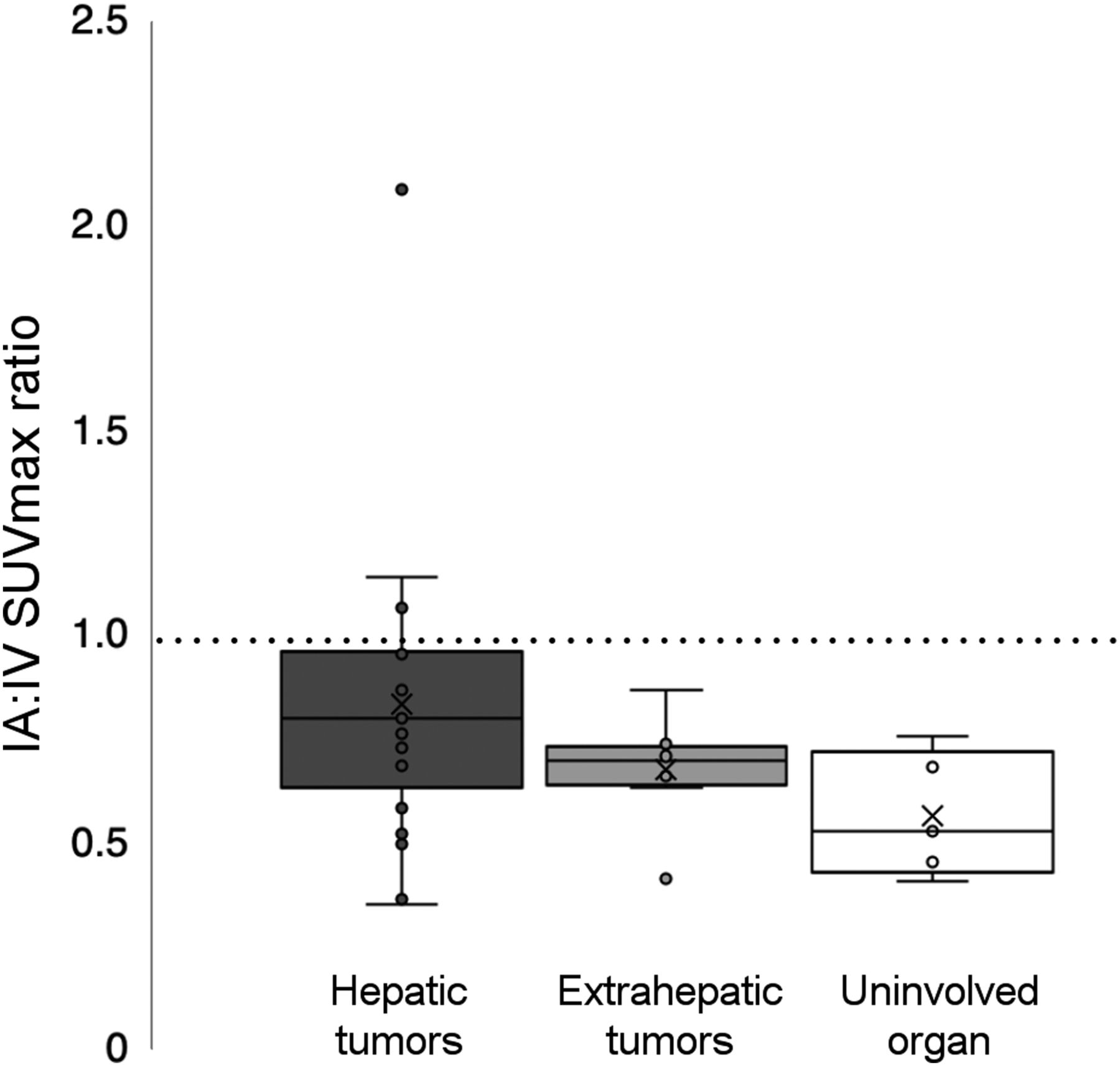
The 5 patients who received intraarterial 68Ga-DOTATOC with 90Y-DOTATOC generally failed to demonstrate an increase in uptake by hepatic metastases over that seen with intravenous administration. The median intraarterial-to-intravenous SUVmax ratio was 0.81 (range, 0.36–2.09) on a per-lesion basis and 0.90 (range, 0.54–0.97) on a per-patient basis (Fig. 2). However, extrahepatic metastases and uninvolved organs demonstrated an expected decreased median uptake between intraarterial and intravenous administration in all patients (ratio of 0.73 and range of 0.42–0.87 for extrahepatic metastases and ratio of 0.53 and range of 0.41–0.76 for uninvolved organs). Uptake in hepatic lesions, extrahepatic lesions, and uninvolved organs as represented by spleen (left kidney in 1 asplenic patient) generally decreased with intraarterial administration compared with intravenous (Fig. 3A), with a trend toward statistical significance for the difference between intravenous and intraarterial SUVmax in liver tumors (P = 0.063) and uninvolved organs (P = 0.063). There was no significant difference between intravenous and intraarterial SUVmax for extrahepatic tumors (P = 0.125).
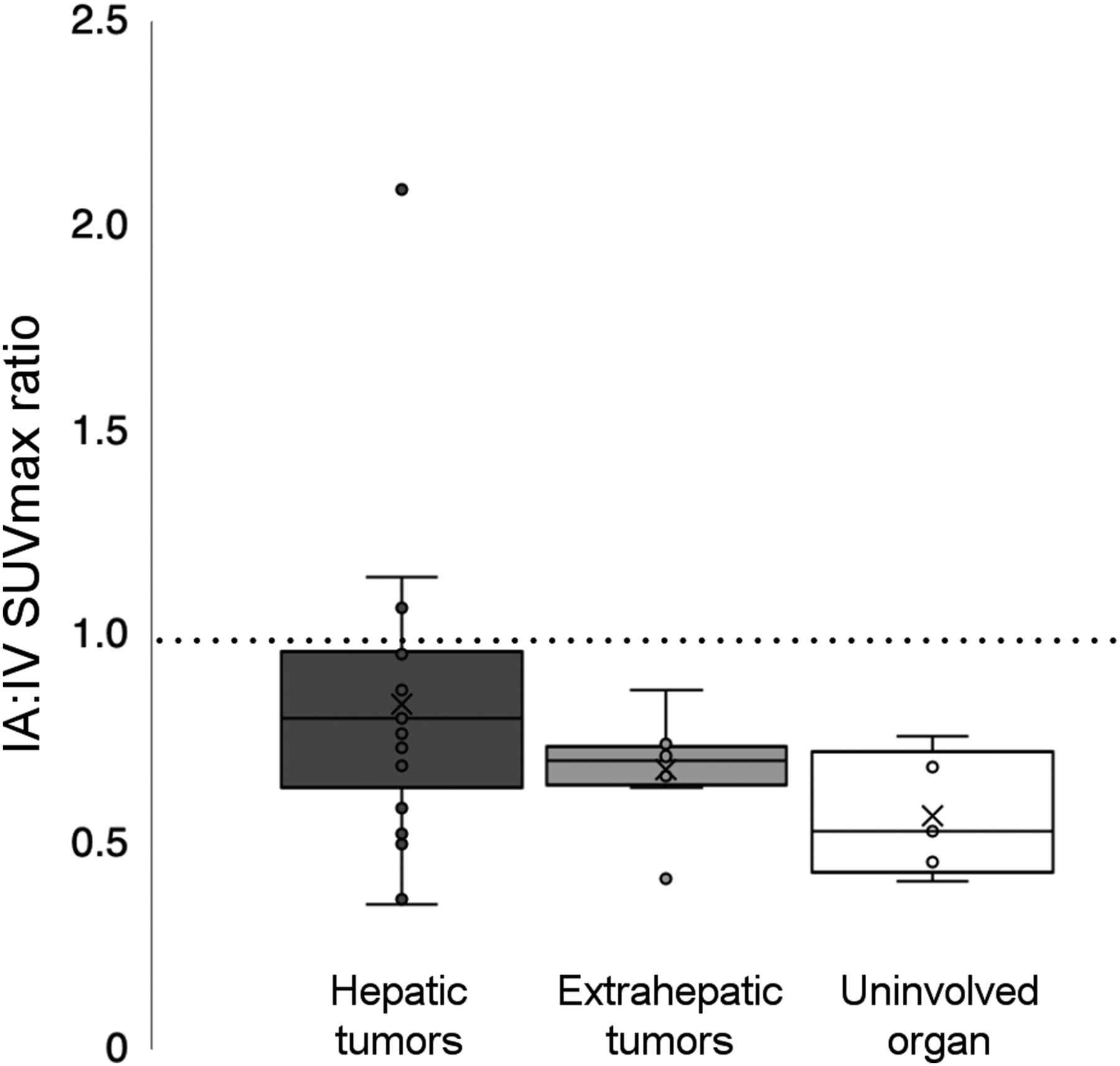
Ratio of median intraarterial-to-intravenous 68Ga-DOTATOC SUVmax for hepatic tumors, extrahepatic tumors, and uninvolved organs. There was trend toward statistical significance for difference in intraarterial-to-intravenous ratios between liver lesions and uninvolved organs (P = 0.063). IA = intraarterial; IV = intravenous.

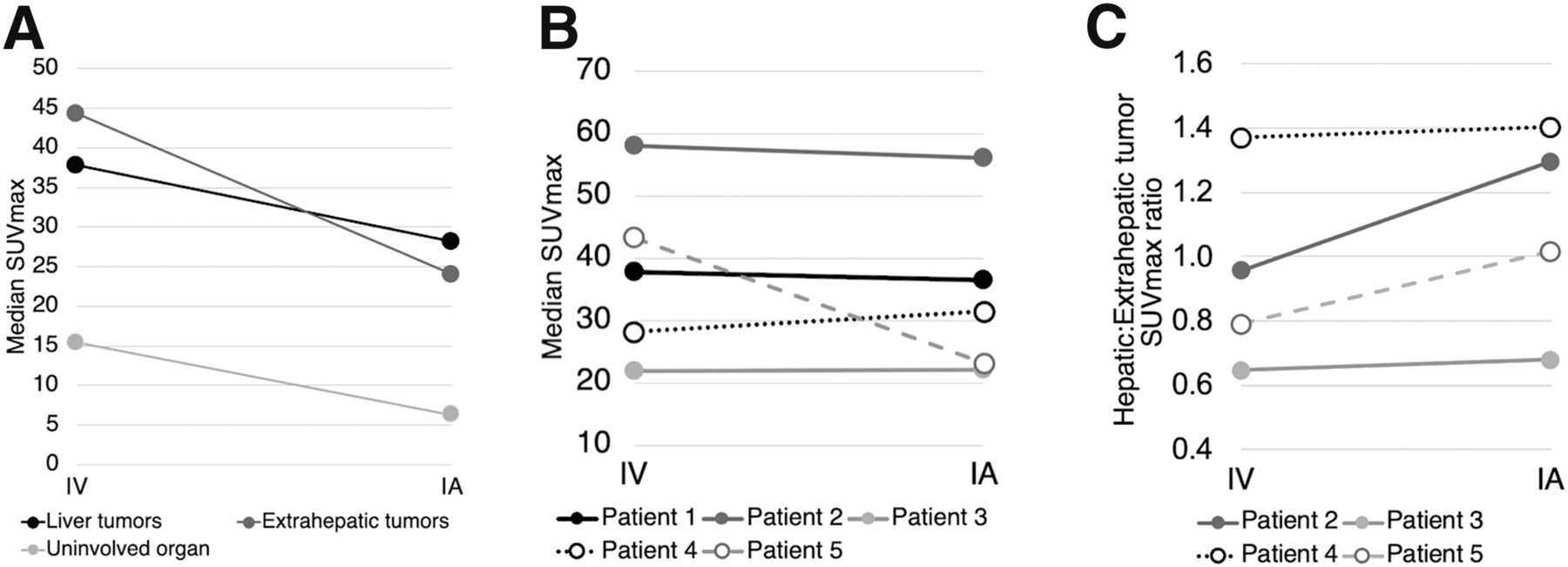
(A) Change in median SUVmax for hepatic tumors, extrahepatic tumors, and uninvolved organs (spleen in 4 patients, left kidney in 1 asplenic patient) from intravenous administration of 68Ga-DOTATOC to intraarterial administration. There was trend toward statistical significance for difference between intravenous and intraarterial SUVmax in liver tumors (P = 0.063) and uninvolved organs (P = 0.063). (B) Change in median hepatic tumor SUVmax from intravenous administration of 68Ga-DOTATOC to intraarterial administration for each patient. Patients 1 and 5 had low hepatic tumor burden (<25% of liver parenchyma), patient 2 had moderate burden (25%–50%), and patients 3 and 4 had high burden (>50%–75%). (C) Change in median ratio of SUVmax for hepatic tumors compared with extrahepatic tumors from intravenous administration of 68Ga-DOTATOC to intraarterial administration. All extrahepatic tumors had decreased uptake with intraarterial compared with intravenous administration. Patient 1 did not have extrahepatic metastatic disease. IA = intraarterial; IV = intravenous.
At the individual-patient level (Fig. 3B), liver uptake patterns were not uniform. The patients with the highest burden of hepatic metastatic disease (50%–70% of liver parenchyma involved, patients 3 and 4) experienced stable to slightly increased uptake in liver lesions with intraarterial administration (patient 3, median intravenous SUVmax of 22.0, median intraarterial SUVmax of 22.2; patient 4, median intravenous SUVmax of 28.2, median intraarterial SUVmax of 31.5). The remaining patients demonstrated stable to decreased uptake in liver lesions on intraarterial administration (Fig. 4). However, for individual patients, the ratio of radiotracer uptake in hepatic metastases compared with extrahepatic metastases slightly increased with intraarterial administration (Fig. 3C).
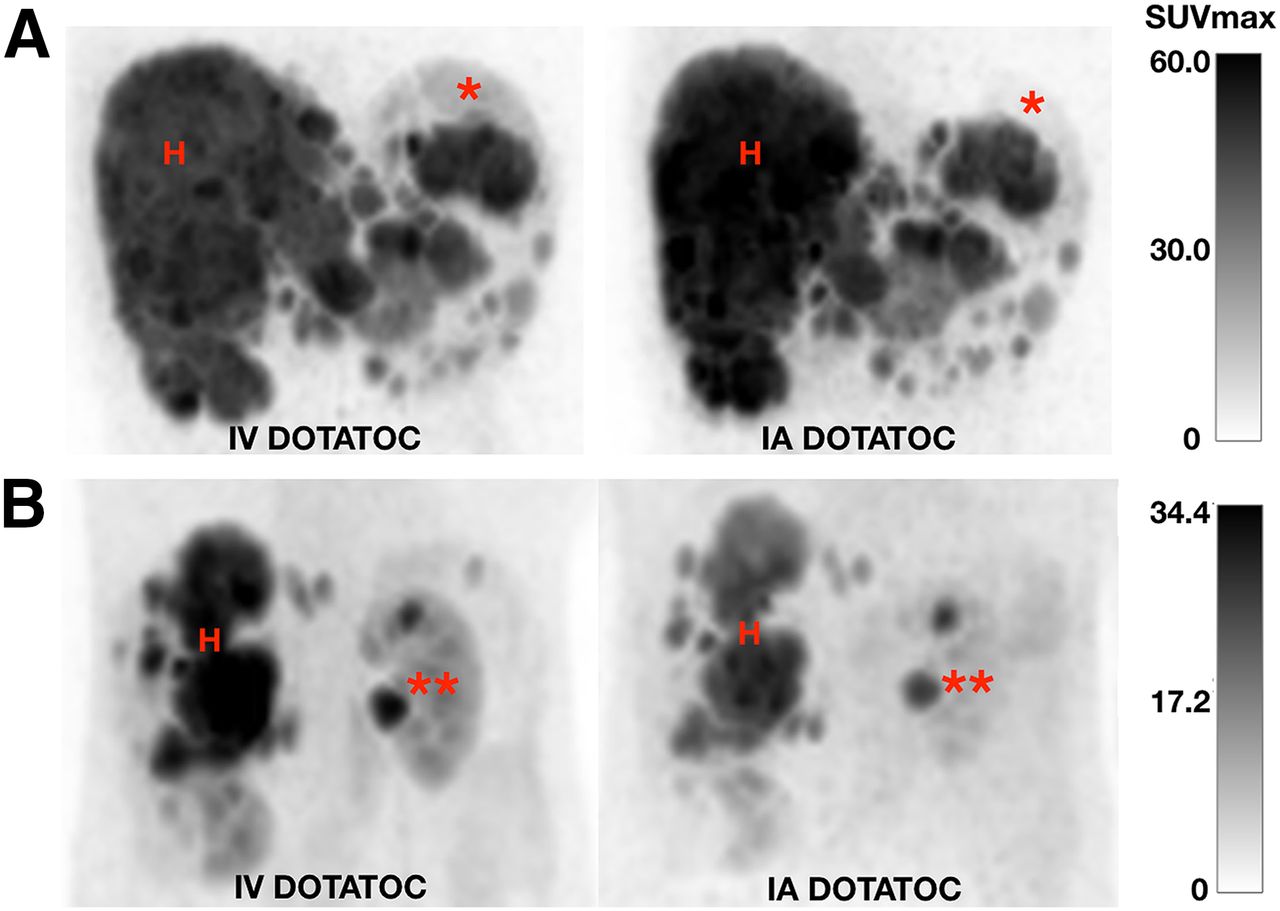
Examples of changes in uptake with intravenous versus intraarterial administration of 68Ga-DOTATOC. (A) Maximum-intensity projections through abdomen in patient with high (50%–70%) degree of liver involvement, showing that uptake in hepatic metastases is slightly higher with intraarterial than intravenous administration. (B) Maximum-intensity projections through abdomen in patient with low (<25%) degree of liver involvement, showing that uptake in hepatic metastases is slightly lower with intraarterial than intravenous administration. For all patients, uninvolved-organ uptake decreased as expected on intraarterial administration (e.g., in spleen [*] and left kidney [**]). H = hepatic metastases; IA = intraarterial; IV = intravenous.
DISCUSSION
Our study demonstrated that a single treatment using 90Y-DOTATOC resulted in minimal radiographic disease response. Additionally, administration of PRRT via the hepatic artery does not clearly recapitulate the increased hepatic uptake seen in previous studies (12,13). Also, although some patients tolerated the therapy well, others experienced severe adverse events, which were possibly attributable to 90Y-DOTATOC.
Previous studies have shown therapeutic efficacy with multiple intraarterial administrations of PRRT: Kratochwil et al., in 2011 (17), demonstrated a complete response in 7% of patients and a partial response in 53% of patients treated with up to 5 intraarterial administrations of 90Y- or 177Lu-PRRT, and Limouris et al., in 2012 (19), demonstrated a partial response in 66.7% of patients treated with up to 6 intraarterial administrations of 177Lu-PRRT. However, the efficacy of a single treatment remains to be determined, as does the minimum number of doses of intraarterial PRRT required for effective treatment. Because Kratochwil et al. demonstrated a mean 3.75-fold increase in hepatic tumor uptake with intraarterial compared with intravenous administration (12), and intravenous 90Y-based PRRT is typically delivered over 2–3 cycles, we hypothesized that efficacy equivalent to multiple intravenous cycles could be achieved in a single intraarterial cycle. Another reason for opting for a single treatment was that NET patients have long lifespans, and it is important to limit cumulative radiation dose, especially if the efficacy of a single treatment is noninferior to that of multiple treatments. However, the lack of efficacy we observed with a single intraarterial treatment suggests that multiple treatments are necessary to achieve a therapeutic effect, though exactly how many remains to be determined.
The major adverse effects associated with intravenous PRRT are bone marrow toxicity and renal toxicity. The largest study regarding toxicity, from Bodei et al. in 2015 (18), involved 807 patients treated with either 90Y- or 177Lu-based intravenous PRRT. In that study, 14% of patients developed CTCAE grade 3 (severe) or 4 (life-threatening) bone marrow toxicity. In addition, 2.8% of patients developed grade 3 or 4 renal toxicity, primarily in patients receiving 90Y. In the NETTER-1 trial, at least 9% of patients developed acute bone marrow toxicity (2). In our study using a single dose of intraarterial PRRT, no patient developed grade 3 or 4 bone marrow or renal toxicity. It remains unclear if systemic toxicity can be decreased with intraarterial administration compared with intravenous.
In terms of hepatic toxicity, neither the NETTER-1 study nor the study by Bodei et al. reported grade 3 or 4 hepatic toxicity with intravenous therapy (2,18), nor did prior studies of intraarterial PRRT. However, although our study did not clearly demonstrate hepatotoxicity (e.g., through sustained laboratory evidence of liver failure), the death of two of the patients with a high liver burden was concerning. It is possible that patients with a higher liver burden and more advanced disease were more likely to have a poor outcome independent of intraarterial PRRT-related toxicity (17,19). The question about hepatotoxicity remains unanswered and may be related to the use of higher-energy 90Y rather than 177Lu.
The 2 patients who died had markedly different treatment histories (one received SSA therapy only, and one received multiple prior liver-directed therapies, chemotherapy, and targeted therapy). However, they shared a characteristic: the largest hepatic tumor burden of all study patients (65%–70% of liver involved). Radiation-induced liver toxicity has been described as a clinical syndrome that includes weight gain, increased abdominal girth, ascites, and alkaline phosphatase elevation out of proportion to other liver enzymes (20). One of the 2 patients did demonstrate an elevated alkaline phosphatase level after therapy, but neither patient displayed other significant signs of this clinical entity. In addition, they did not meet the criteria for nonclassic radiation-induced liver toxicity, including jaundice or markedly elevated transaminases (20). Although several factors unrelated to intraarterial PRRT may have contributed to the patients’ deaths and there was no definitive evidence of radiation-induced liver toxicity, there was concern that the high dose of radiation to the liver could have played some role. The potential treatment-related toxicity suggests that future studies using intraarterial 90Y-DOTATOC should set a lower limit for liver involvement than the 70% threshold used in our study.
Most surprisingly, and in contrast to previous reports, we did not reproduce a significant increase in uptake of 90Y-DOTATOC in hepatic metastases when delivered intraarterially compared with intravenously (12,13). Kratochwil et al., in 2010 (12), demonstrated a leveling off of the time–activity curve with intraarterial administration of 250 MBq (6.8 mCi) of 111In-DOTATOC within 10 min of a 20-min administration period. By contrast, the intravenous time–activity curve demonstrated a nearly linear slope, and uptake continued to increase after administration had concluded. This observation was attributed to receptor saturation. In our study, the fact that the imaged 68Ga-DOTATOC was administered alongside a larger mass dose of 90Y-DOTATOC (25 vs. 115 μg) may have resulted in rapid SSTR saturation. Future studies should be undertaken with an aim to overcome receptor saturation, with possible approaches including decreasing the mass dose or increasing the specific activity, prolonging the administration time, and fractionating the dose. Additionally, work is needed to determine the minimum number of intraarterial treatments needed.
One limitation of our study was the small number of patients, as the study was stopped after accrual of 10 patients because of lack of efficacy. Combined with the heterogeneous prior-treatment histories, this small sample size limited the reliability of statistical conclusions and the generalizability of the findings. Unlike prior studies, patients received 1 treatment session of intraarterial PRRT, thus limiting our ability to compare our findings with prior work. Another possible limitation was the inclusion of patients with a history of liver-directed therapy. These patients may have possessed altered tumor vascularity and altered liver perfusion, which may in turn have altered the distribution of intraarterial PRRT. Lastly, intravenous and intraarterial SUVmax measurements may be less comparable because of differences in median uptake times, with intraarterial PET acquisition occurring after a longer median delay than intravenous PET due to logistic factors related to the therapeutic interventional procedure.
CONCLUSION
Our study found that administration of PRRT via the proper hepatic artery did not reproduce the increase in hepatic tumor uptake that was previously reported. One possible reason for the decreased uptake with intraarterial versus intravenous administration is receptor saturation, as the imaged 68Ga-DOTATOC was coadministered with a larger mass dose of 90Y-DOTATOC. In addition, the single treatment using 90Y-DOTATOC did not induce tumor shrinkage, indicating that more treatment cycles may be required. Possible safety concerns in patients with a high liver tumor burden should inform patient selection for future studies.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does direct administration of PRRT to the proper hepatic artery result in increased uptake in hepatic NET metastases compared with traditional intravenous administration, and is it safe and efficacious?
PERTINENT FINDINGS: In a prospective pilot study, patients underwent baseline PET/CT using intravenous 68Ga-DOTATOC, followed by 3.5 ± 0.3 GBq (94.7 ± 5.4 mCi) of 90Y-DOTATOC into the proper hepatic artery at a second visit. Uptake in hepatic metastases was not significantly increased with arterial administration compared with intravenous, and the study was stopped early because of evidence of lack of efficacy of a single treatment, as well as possible safety concerns.
IMPLICATIONS FOR PATIENT CARE: More than a single intraarterial PRRT treatment is likely required to show treatment efficacy, and possible safety concerns in patients with a high liver tumor burden should inform patient selection for future studies.
Footnotes
Published online Jun. 8, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 22, 2020.
- Accepted for publication May 5, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}