


Abstract
18F-DCFPyL (2-(3-{1-carboxy-5-[(6-18F-fluoropyridine-3-carbonyl)-amino]-pentyl}-ureido)-pentanedioic acid) is a promising PET radiopharmaceutical targeting prostate-specific membrane antigen (PSMA). We present our experience with this single-academic-center prospective study evaluating the positivity rate of 18F-DCFPyL PET/CT in patients with biochemical recurrence (BCR) of prostate cancer (PC). Methods: We prospectively enrolled 72 men (52–91 y old; mean ± SD, 71.5 ± 7.2) with BCR after primary definitive treatment with prostatectomy (n = 42) or radiotherapy (n = 30). The presence of lesions compatible with PC was evaluated by 2 independent readers. Fifty-nine patients had scans concurrent with at least one other conventional scan: bone scanning (24), CT (21), MR (20), 18F-fluciclovine PET/CT (18), or 18F-NaF PET (14). Findings from 18F-DCFPyL PET/CT were compared with those from other modalities. Impact on patient management based on 18F-DCFPyL PET/CT was recorded from clinical chart review. Results: 18F-DCFPyL PET/CT had an overall positivity rate of 85%, which increased with higher prostate-specific antigen (PSA) levels (ng/mL): 50% (PSA < 0.5), 69% (0.5 ≤ PSA < 1), 100% (1 ≤ PSA < 2), 91% (2 ≤ PSA < 5), and 96% (PSA ≥ 5). 18F-DCFPyL PET detected more lesions than conventional imaging. For anatomic imaging, 20 of 41 (49%) CT or MRI scans had findings congruent with 18F-DCFPyL, whereas 18F-DCFPyL PET was positive in 17 of 41 (41%) cases with negative CT or MRI findings. For bone imaging, 26 of 38 (68%) bone or 18F-NaF PET scans were congruent with 18F-DCFPyL PET, whereas 18F-DCFPyL PET localized bone lesions in 8 of 38 (21%) patients with negative results on bone or 18F-NaF PET scans. In 8 of 18 (44%) patients, 18F-fluciclovine PET had located the same lesions as did 18F-DCFPyL PET, whereas 5 of 18 (28%) patients with negative 18F-fluciclovine findings had positive 18F-DCFPyL PET findings and 1 of 18 (6%) patients with negative 18F-DCFPyL findings had uptake in the prostate bed on 18F-fluciclovine PET. In the remaining 4 of 18 (22%) patients, 18F-DCFPyL and 18F-fluciclovine scans showed different lesions. Lastly, 43 of 72 (60%) patients had treatment changes after 18F-DCFPyL PET and, most noticeably, 17 of these patients (24% total) had lesion localization only on 18F-DCFPyL PET, despite negative results on conventional imaging. Conclusion: 18F-DCFPyL PET/CT is a promising diagnostic tool in the work-up of biochemically recurrent PC, given the high positivity rate as compared with Food and Drug Administration–approved currently available imaging modalities and its impact on clinical management in 60% of patients.
Patients with localized prostate cancer (PC) who underwent primary definitive treatment may subsequently experience a rise in prostate-specific antigen (PSA) levels, known as biochemical recurrence (BCR). Approximately 20%–40% of patients treated with radical prostatectomy (1), and 30%–50% patients who undergo radiation therapy (2), will experience BCR within 10 y (3). Although rising PSA levels can predict recurrent disease or metastasis, not all BCR patients have the same prognosis based on PSA level alone.
Oncologists thus need to balance rising PSA level with the efficacy and side effects of subsequent treatment options. Common clinical decisions made by oncologists include active surveillance; androgen deprivation therapy (ADT); and salvage radiation therapy, salvage prostatectomy, or both. However, there is no uniform guideline regarding treatment choice and its timing (4).
Therefore, effective imaging that is able to localize recurrence or distant metastasis in BCR patients with high sensitivity and specificity is critical for selection of different treatments.
Imaging such as CT, MR, or bone scintigraphy generally has low sensitivity in detecting sites of recurrent disease (5). The Food and Drug Administration approved 11C-choline in 2012 and 18F-fluciclovine (Blue Earth Diagnostics Ltd.) in 2016 for use in patients with BCR. Recent prospective trials have shown 18F-fluciclovine PET to have a significant impact on clinical decision making in BCR (6). However, a common criticism is that the detection rate of 18F-fluciclovine is relatively lower in patients with a PSA level of less than 2.0 ng/mL (7).
PSMA expression is upregulated in PC and is associated with high-grade PC and androgen deprivation (8). Several PSMA-based radiopharmaceuticals, including 68Ga-PSMA-11 (9–11) and 18F-PSMA-1007 (12), have better rates of detection than 11C- or 18F-choline. 18F-DCFPyL (2-(3-{1-carboxy-5-[(6-18F-fluoropyridine-3-carbonyl)-amino]-pentyl}-ureido)-pentanedioic acid) is a PSMA-targeting PET radiopharmaceutical with greater affinity than the previous generation (13–15). A direct comparison of 18F-DCFPyL with 68Ga-PSMA-11 showed that 18F-DCFPyL is noninferior and may even have higher sensitivity (16). A recent prospective study also showed that 18F-DCFPyL PET/CT is safe and sensitive for detection of BCR and changed clinical management in most patients (17). Here, we report our experience in an academic-center prospective evaluation of 18F-DCFPyL PET/CT in patients with BCR PC.
MATERIALS AND METHODS
This study was approved by the Stanford Institutional Review Board and the Stanford Cancer Institute Scientific Review Committee. All subjects gave written informed consent. The study was registered on clinicaltrials.gov (NCT03501940).
All participants had BCR after primary definitive treatment with radical prostatectomy with or without adjuvant pelvic radiation or radiation therapy alone. A rising PSA level after definitive therapy with prostatectomy or radiation therapy (external beam or brachytherapy) was defined as follows. After radical prostatectomy, the American Urological Association recommendation was used (18): PSA greater than or equal to 0.2 ng/mL measured after at least 6 wk after radical prostatectomy or confirmatory persistent PSA greater than or equal to 0.2 ng/mL (total of 2 PSA measurements > 0.2 ng/mL). After radiation therapy, the American Society for Radiation Oncology–Phoenix consensus definition was used (19): a rise of PSA measurement of 2 ng/mL or more over the nadir. Time to first BCR was calculated from the date of primary definitive treatment to the date of the first BCR.
Imaging Protocol
18F-DCFPyL was provided by Progenics Pharmaceuticals, Inc., as part of a research access program, for use in an investigator-initiated protocol. 18F-DCFPyL dosage ranged from 270.1 to 370 MBq (mean ± SD, 338.8 ± 25.3 MBq). Imaging started 60 min (mean ± SD, 74.4 ± 10.4 min) after intravenous administration of the radiopharmaceutical. A low-dose CT scan was performed for attenuation correction and anatomic correlation. PET followed immediately afterward, starting from the mid thighs and proceeding to the vertex of the skull. All patients were scanned using a state-of-the-art time-of-flight–enabled, silicon photomultiplier–based Discovery MI PET/CT device (GE Healthcare). PET data underwent block-sequential regularized expectation-maximization penalized-likelihood reconstruction (Q.Clear; GE Healthcare). β, the noise-penalizing determining factor in Q.Clear, was set at 400 per local preference.
Image Analysis and Correlation with Biopsy Results
PET/CT images were reviewed independently by 2 nuclear medicine physicians using MIMvista, version 6.7. Positive lesions (uptake above adjacent background in putative sites of disease) were categorized on the basis of their location in the prostate bed, pelvic lymph nodes, abdominal or retroperitoneal lymph nodes, osseous lesions, or other visceral or soft-tissue lesions (such as hepatic or pulmonary lesions). Imaging findings on other conventional imaging modalities, including CT, MR, bone scanning, 18F-NaF PET/CT, and 18F-fluciclovine PET/CT, were also reviewed and compared with the findings on 18F-DCFPyL PET/CT. Findings were considered congruent if both scans compared were negative or if the same lesions were identified on both scans. Impact on patient management after 18F-DCFPyL PET/CT was recorded from prospective chart review of clinical notes.
Pathologic confirmation of the 18F-DCFPyL findings was available in only a few cases (n = 4). Biopsy was not required by the study design and was often difficult since the lesions detected on 18F-DCFPyL PET were frequently subcentimeter in size.
Statistical Analysis
The positivity rate was defined as the percentage of patients with focal 18F-DCFPyL PET/CT uptake in putative sites of disease. The positivity rates for different PSA levels and doubling times were compared with a χ2 test, with a significant P value set at less than 0.05.
RESULTS
Study Participants
We prospectively enrolled 72 men (52–91 y old; mean ± SD, 71.5 ± 7.2) between May 2018 and July 2019. Primary definitive treatment included radical prostatectomy with or without adjuvant pelvic radiation in 42 participants and radiation therapy in 30 participants. The clinical data are summarized in Table 1. Fifty-nine patients (82%) had at least one of the following conventional imaging scans during the work-up for BCR: bone scan (n = 24), CT (n = 21), MR (n = 20), 18F-fluciclovine PET/CT (n = 18), or 18F-NaF PET (n = 14).
Demographics and Characteristics of Participants
PSA Levels and Positivity Rates on 18F-DCFPyL PET/CT
The PSA level at the time of 18F-DCFPyL PET/CT ranged from 0.23 to 698.4 ng/mL (median, 3.0 ng/mL; mean ± SD, 15.8 ± 83.2 ng/mL). Twenty-one patients (29%) had a PSA level of less than 1.0 ng/mL at the time of 18F-DCFPyL PET/CT. The median PSA level for patients treated with radical prostatectomy or radiation therapy was 1.4 ng/mL (range, 0.2–18.3 ng/mL) and 5.4 ng/mL (range, 0.4–698.4 ng/mL), respectively.
18F-DCFPyL PET showed focal uptake in putative sites of disease in 61 patients (85%). This positivity rate increased significantly with PSA level. 18F-DCFPyL PET was positive in 62% of participants with a PSA level of less than 1.0 ng/mL and in 94% of participants with a PSA level of 1.0 ng/mL or higher (P < 0.001). The positivity rates for the various PSA levels (ng/mL) were 50% (PSA < 0.5), 69% (0.5 ≤ PSA < 1), 100% (1 ≤ PSA < 2), 91% (2 ≤ PSA < 5), and 96% (PSA ≥ 5). These findings are summarized in Table 2. The 18F-DCFPyL PET positivity rate for different PSA doubling times was 87%, 85%, 92%, and 79% for doubling times of 0–3 mo, 3–6 mo, 6–12 mo, and greater than 12 mo, respectively (P > 0.05). Four biopsies were performed, all of which confirmed prostate adenocarcinoma at the sites of 18F-DCFPyL uptake. Three of the biopsy sites evaluated uptake in the prostate gland, and one biopsy targeted the left pubic bone.
Positivity Rates of 18F-DCFPyL PET/CT Based on PSA Level and PSA Doubling Time
The 18F-DCFPyL PET positivity rate was 89% for the 28 patients with prior BCR and treatment, compared with 82% for the 44 patients evaluated at first BCR (P < 0.01). This difference may be partially explained by the fact that a prescan PSA level of less than 1.0 occurred in fewer patients with prior BCR (7 of 28 patients, 25%) than in patients at first BCR (13 of 44, 30%) because the overall positivity rate is lower in patients with a prescan PSA level of less than 1.0.
Sites of Disease Detected with 18F-DCFPyL PET/CT
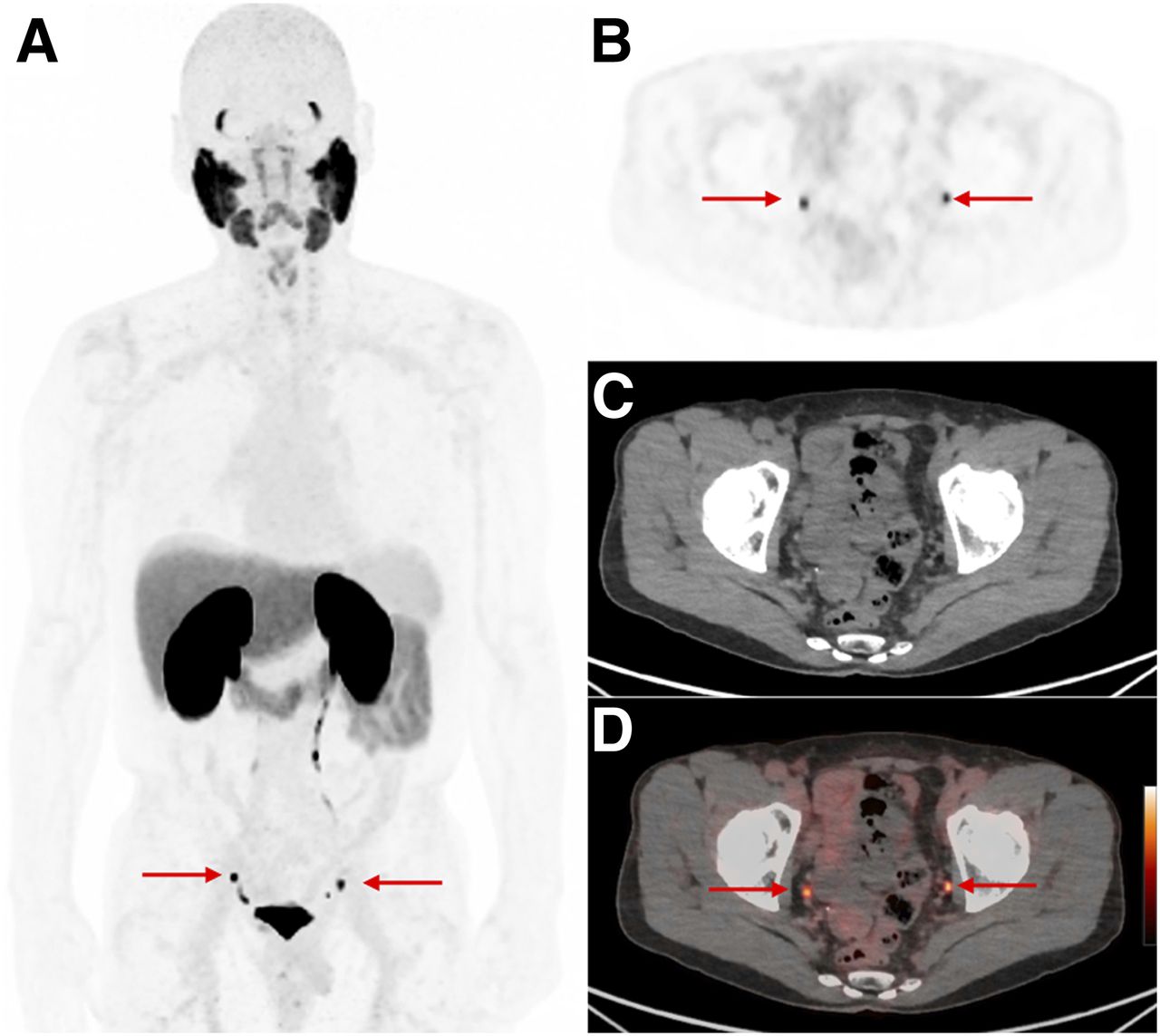
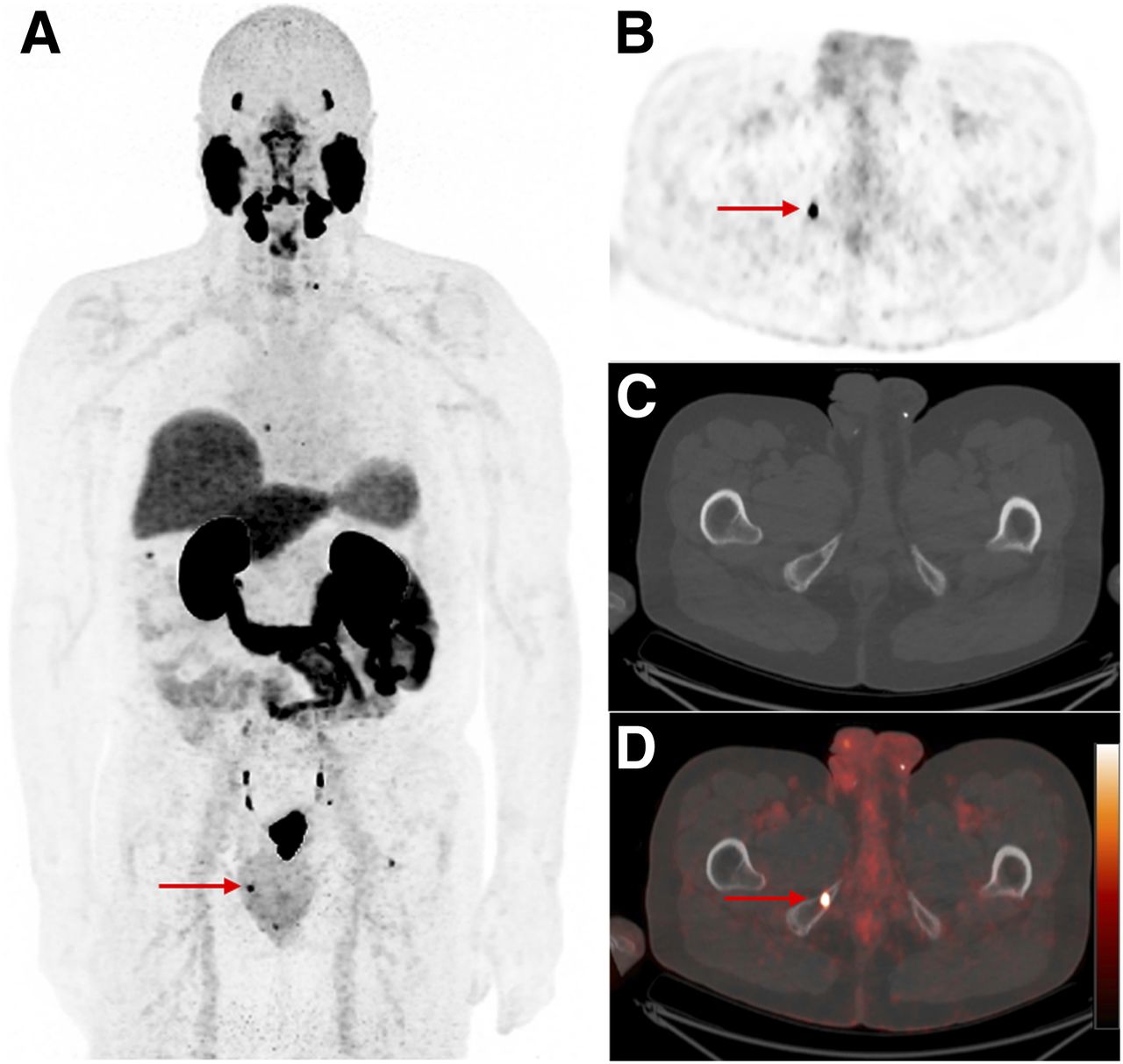
The disease sites most commonly detected by 18F-DCFPyL PET/CT included prostate bed (31% of positive scans) and pelvic lymph nodes (48% of positive scans). In addition, a high percentage of patients had extrapelvic findings on 18F-DCFPyL PET/CT, including 46% with bone lesions, 28% with abdominal and retroperitoneal lymph nodes, and 16% with soft-tissue lesions in other organs such as liver and lungs. Figure 1 shows pelvic lymph nodes as sites of recurrent disease, whereas Figure 2 shows a small osseous lesion. As expected, more lesions were detected in the prostate bed when patients were treated with radiation therapy (15/30 patients, 50%) than when patients were treated with radical prostatectomy (4/42 patients, 10%) (P < 0.001). No significant difference in percentage of detected extrapelvic disease (abdominal or retroperitoneal lymph node lesions, bone, or other sites, including lungs and liver) was seen between prostatectomy and radiation therapy (P > 0.05).
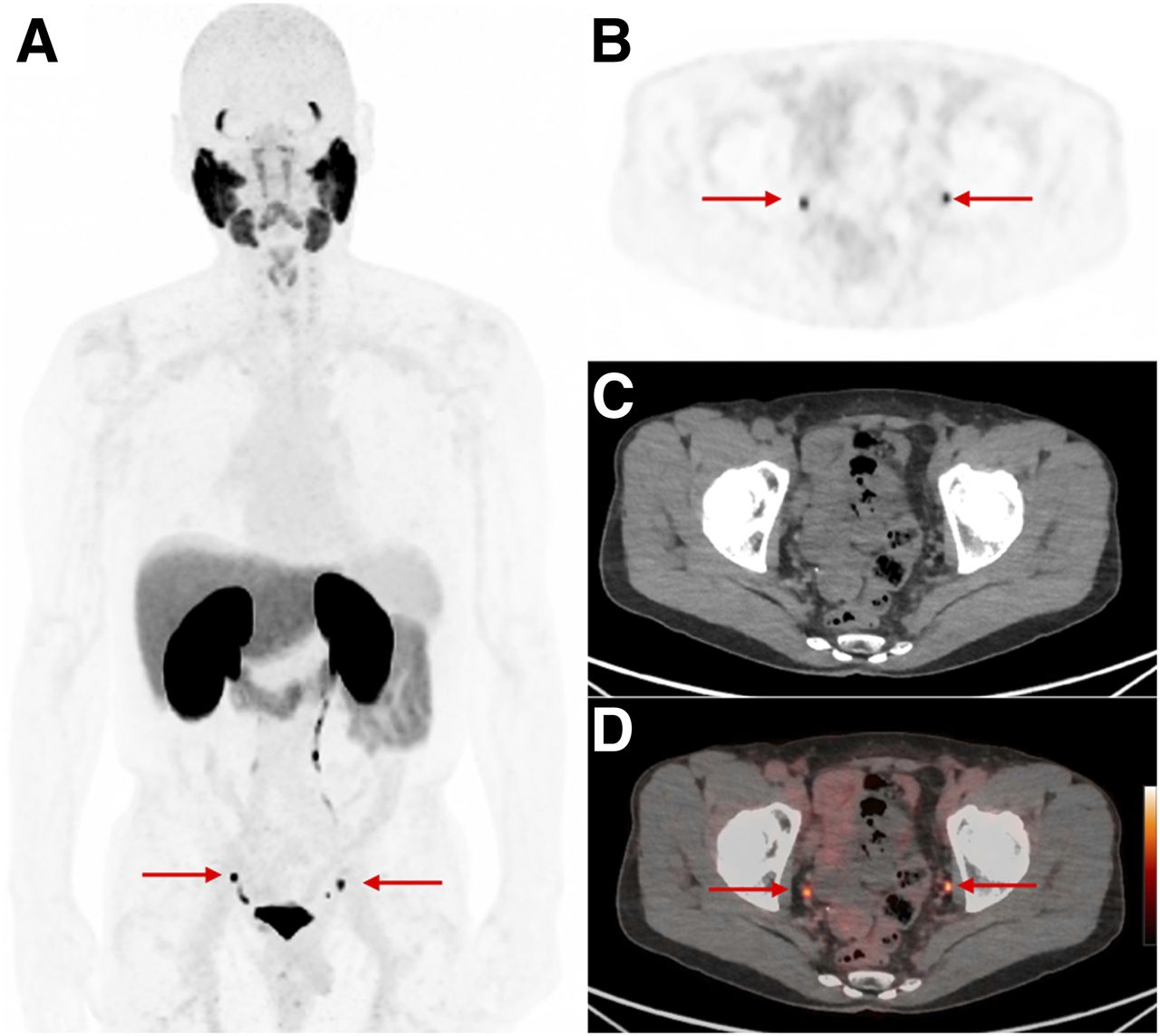
A 68-y-old man with BCR (PSA, 5.4 ng/mL). 18F-DCFPyL PET maximum-intensity projection (A) shows bilateral uptake in pelvic wall lymph nodes (arrows), also seen on axial PET (B), CT (C), and PET/CT (D). These are below CT size threshold for pathology.
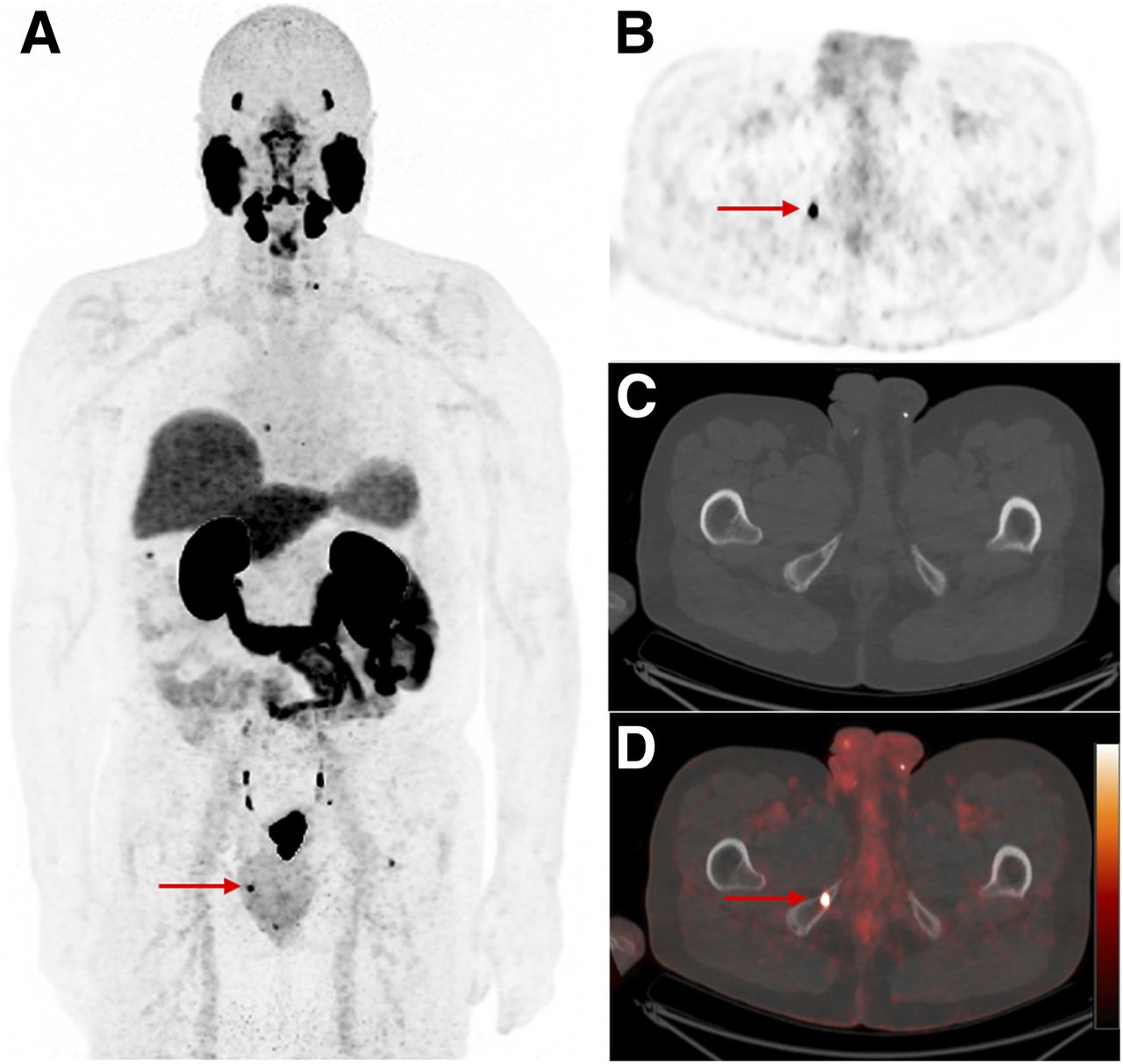
A 69-y-old man with BCR (PSA, 0.4 ng/mL). 18F-DCFPyL PET maximum-intensity projection (A) shows several small bone lesions and pelvic lymph node (arrow); focal 18F-DCFPyL uptake in right ischium (arrows) is seen on axial PET (C), CT (D), and PET/CT (E).
Comparison with Other Imaging Modalities
When 18F-DCFPyL PET was compared with CT, 7 of 21 (33%) CT scans showed findings congruent with 18F-DCFPyL PET, whereas 12 of 21 (57%) patients with negative CT findings had positive 18F-DCFPyL PET findings. In addition, a higher percentage (13/20, 65%) of MR scans had findings congruent with 18F-DCFPyL PET, whereas 5 of 20 (25%) patients with negative MR findings had positive 18F-DCFPyL PET findings. These findings are shown in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). The main explanation for the advantage of 18F-DCFPyL over conventional CT or MR is that 18F-DCFPyL PET often shows uptake in subcentimeter lesions that do not meet size criteria on cross-sectional imaging. Figure 1 shows an example of a patient with DCFPyL uptake in subcentimeter pelvic wall lymph nodes seen on CT but not meeting size criteria. Moreover, 1 of 18 (6%) MR scans showed a single suspected L1 lesion with spinal stenosis confirmed by bone scanning; the patient was initially scheduled for laminectomy. However, 18F-DCFPyL PET showed uptake in additional lesions in L2 and L5; therefore, treatment was changed to ADT. This case demonstrates the advantage of 18F-DCFPyL PET over MR in identifying small marrow lesions.
For dedicated bone imaging, 16 of 24 (67%) 99mTc-MDP bone scans had findings congruent with 18F-DCFPyL PET, whereas 6 of 24 (25%) patients with negative bone scans had bone metastases identified on 18F-DCFPyL PET. Figure 3 shows an 18F-DCFPyL PET scan with extensive bone metastasis, including a left iliac wing lesion that had no uptake on bone scanning. On the other hand, one of the patients had uptake in a sclerotic rib lesion on bone scanning, but no uptake was seen on 18F-DCFPyL PET. This patient continued to receive active surveillance under the assumption that the uptake on the bone scan was nonspecific. In another participant, with focal 99mTc-MDP uptake in an iliac crest lesion, 18F-DCFPyL PET found no uptake in the iliac lesion; instead, there was uptake in a sclerotic rib lesion, as well as in multiple abdominal lymph nodes. This patient received ADT, and the PSA has been down-trending (we are still following participants). Similarly, 10 of 14 (71%) 18F-NaF PET scans had findings congruent with 18F-DCFPyL PET, whereas 2 of 14 (14%) patients with 18F-DCFPyL PET findings positive for bone metastasis had negative results on 18F-NaF PET. In a patient whose findings differed between 18F-NaF and 8F-DCFPyL PET, 18F-NaF PET showed uptake in a left iliac lesion, but no bony uptake was seen on 18F-DCFPyL; instead, 18F-DCFPyL uptake was seen in several abdominal soft-tissue nodules and hepatic lesions. This patient started ADT, and the PSA decreased to undetectable levels.
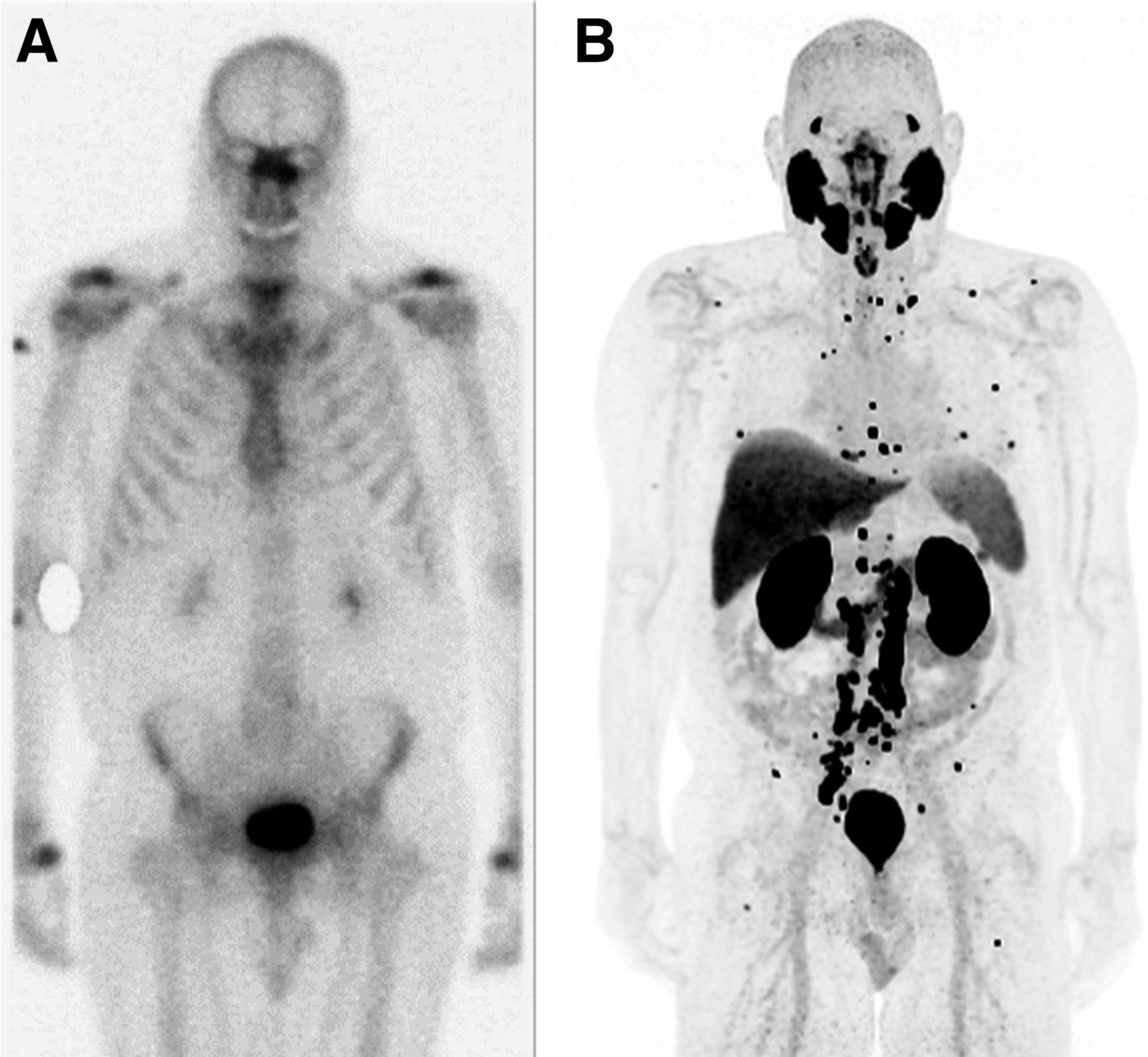
A 69-y-old man with BCR (PSA, 3.3 ng/mL) had bone scan that was negative (A), but 18F-DCFPyL PET maximum-intensity projection (B) showed extensive nodal and skeletal metastases.
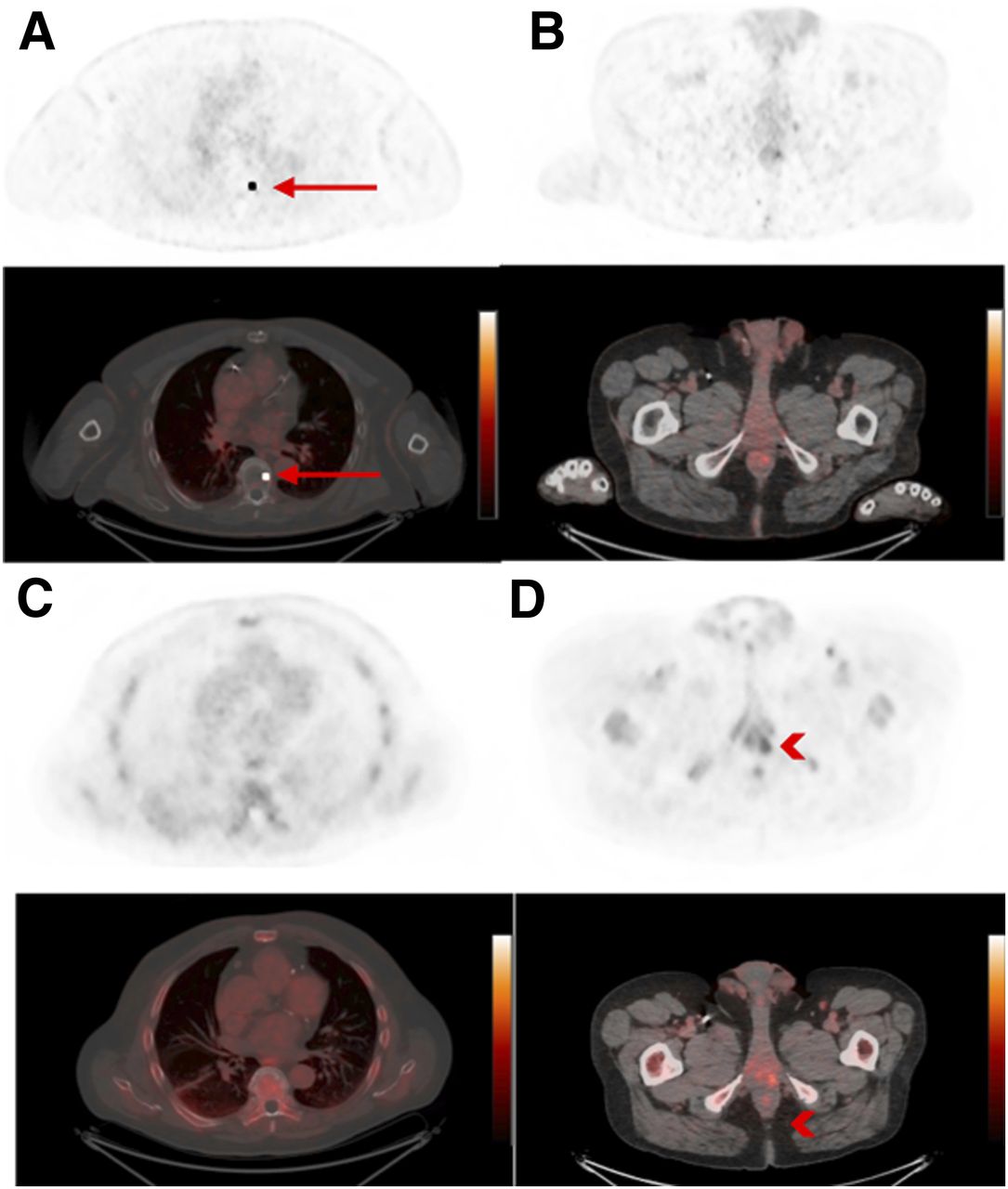
In total, 18 patients had 18F-fluciclovine PET/CT as part of a standard-of-care work-up for BCR. In 8 of the 18 (44%), 18F-fluciclovine PET showed the same lesions as 18F-DCFPyL PET. However, in 5 of the 18 (28%), 18F-fluciclovine PET was negative but 18F-DCFPyL PET identified putative sites of disease, including 3 patients with uptake in pelvic side wall lymph nodes and 2 patients with uptake in multiple sclerotic bone lesions. In comparison, 1 of the 18 (6%), findings were negative with 18F-DCFPyL whereas 18F-fluciclovine showed uptake in the prostate bed. In the remaining 4 of the 18 (22%), 18F-DCFPyL and 18F-fluciclovine scans had different findings. For example, in 1 patient after radical prostatectomy, 18F-DCFPyL PET showed uptake in multiple pelvic and abdominal lymph nodes, focal uptake in the T7 body, and no uptake in the prostate bed, whereas 18F-fluciclovine PET showed uptake in the prostate bed but not in other nodal or bone lesions seen on 18F-DCFPyL PET (Fig. 4). In view of the fact that the patient had high-grade PC at diagnosis and there was a positive margin at prostatectomy, the oncologist took into account findings on both PET scans and treated the patient using ADT and focal radiation to the prostate bed. The patient’s PSA then decreased to undetectable levels.
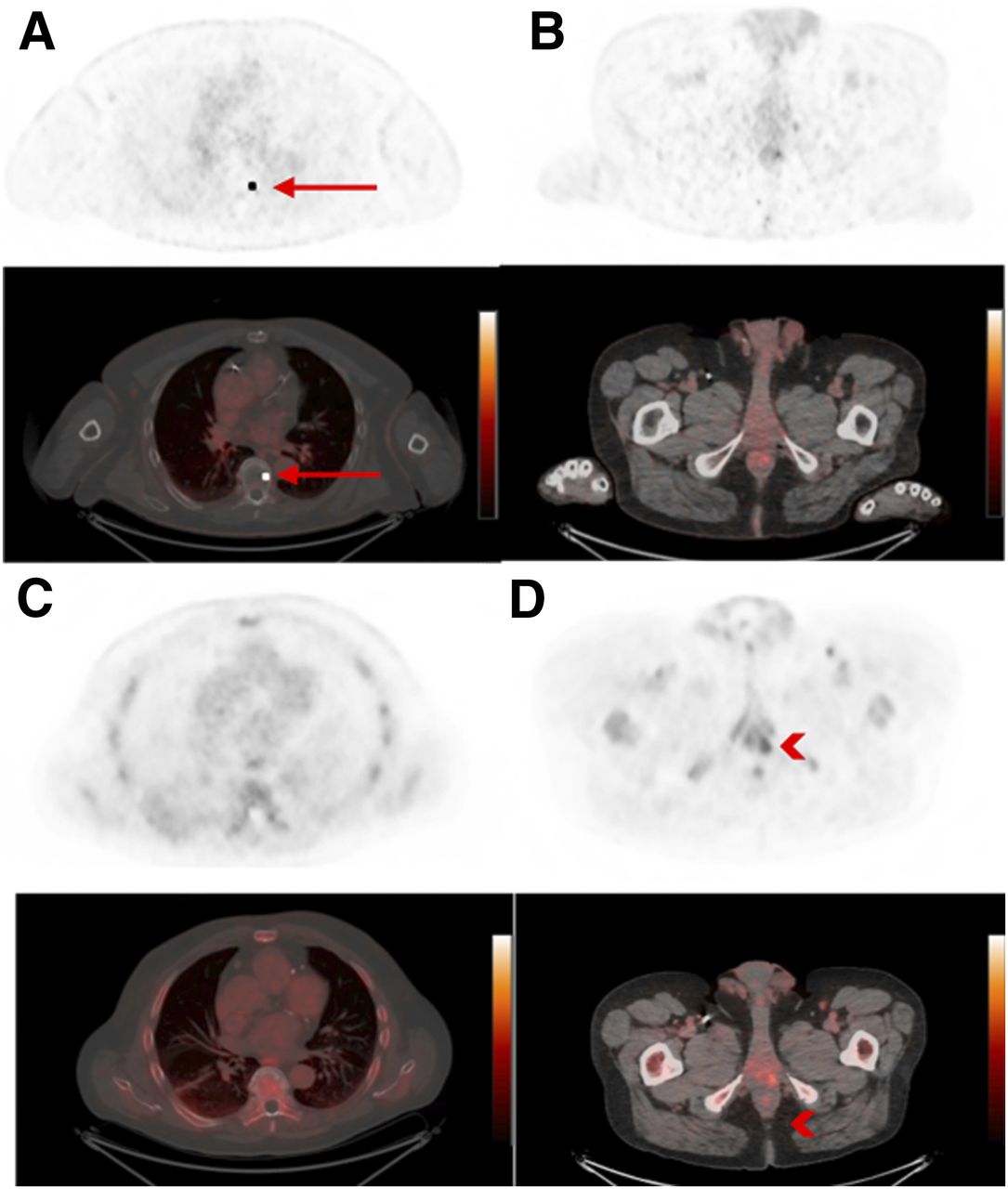
A 64-y-old man with BCR (PSA, 3.1 ng/mL) had different findings on 18F-DCFPyL and 18F-fluciclovine PET. (A and B) Axial 18F-DCFPyL PET/CT (A, bottom) and 18F-DCFPyL PET (A, top) show focal uptake in T7 body (arrows) but no uptake in prostate bed (B, bottom: PET/CT; B, top: PET). (C and D) In comparison, axial 18F-fluciclovine PET/CT (C, bottom) and 18F-fluciclovine PET (C, top) show no uptake in T7 body but focal uptake (arrowhead) in left aspect of prostate bed (D, bottom: PET/CT; D, top: PET).
Impact of 18F-DCFPyL PET/CT on Patient Management
In total, 43 (60%) patients started new treatment after 18F-DCFPyL PET. These included 20 patients (47%) referred for radiation therapy with or without concurrent ADT and 23 patients (53%) who started ADT without radiation therapy. These data are summarized in Supplemental Table 2. Among the 20 patients who received radiation therapy, 7 had targeted extrapelvic lesions (including ribs, vertebral bodies, retroperitoneal lymph nodes, sternum, and calvaria) and 13 had targeted pelvic lesions (6 prostate bed and 7 pelvic lymph nodes). At the time that the manuscript for this article was being prepared, 9 patients had a confirmed PSA decrease after radiation therapy.
18F-DCFPyL PET identified lesions in 26 patients (36%) who had no findings on conventional imaging modalities. This new information led to changes in clinical management in 17 patients (24% of total participants), including 6 patients who received targeted radiotherapy and 11 patients who started ADT. Despite positive findings on 18F-DCFPyL PET, 3 of the 26 patients remained under active surveillance because they had relatively low PSA levels at time of imaging (0.38 and 0.59 ng/mL) or preferred not to receive treatment. Four recently scanned patients had no documented clinical decision after 18F-DCFPyL PET.
DISCUSSION
Compared with 68Ga-labeled tracers, 18F-labeled PSMA-targeting PET radiopharmaceuticals have the advantages of higher spatial resolution due to a shorter positron range and potentially improved commercial availability due to a longer half-life. In the current study, 18F-DCFPyL PET had a high overall positivity rate of 85%. 18F-DCFPyL PET detected more lesions than conventional imaging, ranging from 25% on bone imaging to 57% on CT. Overall, 26 patients (36%) had lesion localization only on 18F-DCFPyL PET, with no findings on other conventional imaging. A similar diagnostic advantage was shown previously in a study in which 138 lesions were detected on 18F-DCFPyL PET whereas only 30 lesions were detected on conventional imaging (14). One reason for this advantage over anatomic imaging is that 18F-DCFPyL uptake is detected in lesions (e.g., lymph nodes) before anatomic diagnostic criteria are met. Moreover, for bone lesions, 18F-DCFPyL PET may be able to detect small marrow lesions that have not caused detectable reactive bony changes typically seen on bone scintigraphy.
No statistically significant higher positivity rate was found for 18F-DCFPyL PET in patients with shorter PSA doubling times, although a trend was observed. This lack of significance may be attributed to the relatively small cohort size. Other PET radiotracers targeting PC have shown increased positivity rates with shorter PSA doubling times. In a metaanalysis of 1,309 patients, 68Ga-PSMA PET positivity was found to be associated with shorter PSA doubling time (20).
18F-DCFPyL PET altered clinical management in 43 patients (60%) treated with targeted radiotherapy or ADT, including 17 patients (24% overall) without findings identified on conventional imaging. This level of impact on clinical management has been observed in other studies using PSMA-targeting radiopharmaceuticals (9,17). One difference in methodology is that several prior studies used a survey of oncologists to determine a change in intended clinical management, whereas we used a review of clinical charts to determine the impact of 18F-DCFPyL PET on clinical management. This approach, although based on actual changes, not intent, makes it difficult to determine whether the decisions of the treating physicians were based on imaging alone or on other contributing factors such as PSA, risks and benefits of treatments, and patient preference. In future prospective trials, we plan to submit prescan and postscan patient-management questionnaires to the treating physicians to help validate these initial findings.
One limitation of our study is that histopathologic confirmation of positive 18F-DCFPyL scans was available for only a few patients. 18F-DCFPyL PET/CT often detects subcentimeter lesions in the setting of BCR, and such lesions are difficulty to biopsy. When multiple lesions are detected on 18F-DCFPyL PET in putative sites for PC recurrence or metastases, treating physicians often rely on posttreatment PSA changes, rather than on biopsy, as an alternative for confirmation of positive DCFPyL lesions. Overall, there are still not enough data in our cohort to evaluate the rate of 18F-DCFPyL false-positive lesions. We previously showed that 68Ga-PSMA-11 had specificity of 87.5% for prostate lesions and 98.4% for metastatic lymph nodes in initial staging using histopathology as the gold standard (11).
Three recently published studies on 18F-DCFPyL showed overall positivity rates of 84.6%, 67.7%, and 86.3% (17,21,22). In comparison with a recent prospective 2-center trial of 68Ga-PSMA11 PET in BCR with a large patient cohort (635 patients) (9), 18F-DCFPyL PET has a better or similar positivity rate of 50% vs. 38% for a PSA level of less than 0.5 ng/mL, 69% vs. 57% for 0.5 ng/mL ≤ PSA < 1.0 ng/mL, 93% vs. 85% for 1.0 ng/mL ≤ PSA < 5.0 ng/mL, and 96% vs. 97% for a PSA level of 5 ng/mL or higher. A similar overall positivity rate of 80.3% was found for 18F-PSMA-1007 in the setting of BCR (12).
In our study, 18F-DCFPyL PET had a higher positivity rate than 18F-fluciclovine PET in a small subgroup who underwent both PET imaging tests (89% vs. 67%, P < 0.01). The overall positivity rate of 18F-fluciclovine PET was 59% in a published study (6). Similarly, higher positivity rates were seen for PSMA-based radiotracers in head-to-head direct comparisons of 68Ga-PSMA-11 to 18F-fluciclovine (23,24). Interestingly, we report 3 patients with prostate bed uptake on 18F-fluciclovine PET who had multiple extrapelvic lesions but no prostate bed lesion identified on 18F-DCFPyL PET. This finding raises the possibility that various radiopharmaceuticals may be complementary in detecting lesions in patients with BCR.
Improved detection of recurrence by 18F-DCFPyL PET is clinically significant only if a subsequently changed clinical management can improve progression-free or overall survival. These long-term benefits have yet to be evaluated. A multicenter phase III trial (SPPORT trial) in patients with BCR showed that the freedom-from-progression rate increased from 71.7% in patients who received prostate bed radiation alone to 89.1% in patients who received prostate bed radiation, pelvic lymph node radiation, and short-term ADT (25). This management decision was based solely on rising PSA and did not consider any imaging findings. Such changes in practice by radiation oncologists could mean that the added value of 18F-DCFPyL PET may be greatest when it detects extrapelvic oligometastatic lesions that may benefit from targeted radiation (26). More clinical trials are needed to evaluate the survival benefits of PSMA-based PET radiotracers in BCR.
A multicenter, multireader prospective trial is currently assessing the accuracy of 18F-DCFPyL PET in localizing disease in patients with BCR and negative baseline imaging results (including 18F-fluciclovine PET), according to an institutional standard-of-care work-up (ClinicalTrials.gov identifier NCT03739684).
CONCLUSION
18F-DCFPyL PET/CT is a promising diagnostic tool in the work-up of patients with biochemically recurrent PC, with an overall positivity rate of 85% in this cohort and an impact on clinical management in 60% of patients, including 24% without abnormal findings on conventional imaging.
DISCLOSURE
18F-DCFPyL was provided by Progenics Pharmaceuticals, Inc., as part of a research access program. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 18F-DCFPyL PET/CT useful in the evaluation of patients with BCR PC?
PERTINENT FINDINGS: In a prospective study of 60 men with BCR after primary definitive treatment, 18F-DCFPyL PET/CT had an overall positivity rate of 83%, which increased with higher PSA levels (ng/mL): 43% (PSA < 0.5), 64% (0.5 ≤ PSA < 1), 100% (1 ≤ PSA < 2), 94% (2 ≤ PSA < 5), and 96% (PSA ≥ 5). In total, 36 of 60 patients (60%) had treatment changes after 18F-DCFPyL PET and, most noticeably, 14 of these patients (23% total) had lesion localization only on 18F-DCFPyL PET, despite negative findings on conventional imaging.
IMPLICATIONS FOR PATIENT CARE: 18F-DCFPyL PET/CT is a promising diagnostic tool in the work-up of BCR patients, given the high positivity rate as compared with other currently Food and Drug Administration–approved imaging modalities and its impact on clinical management.
Footnotes
Published online Oct. 18, 2019.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prospective Comparison of 68Ga-NeoB and 68Ga-PSMA-R2 PET/MRI in Patients with Biochemically Recurrent Prostate Cancer
- Diagnostic Performance of 68Ga-PSMA-11 PET/CT Versus Multiparametric MRI for Detection of Intraprostatic Radiorecurrent Prostate Cancer
- Correlation of 68Ga-RM2 PET with Postsurgery Histopathology Findings in Patients with Newly Diagnosed Intermediate- or High-Risk Prostate Cancer
- 18F-DCFPyL PET Acquisition, Interpretation, and Reporting: Suggestions After Food and Drug Administration Approval
- PSMA- and GRPR-Targeted PET: Results from 50 Patients with Biochemically Recurrent Prostate Cancer
- Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study
- Disparities in PET Imaging of Prostate Cancer at a Tertiary Academic Medical Center