


Visual Abstract

Abstract
For men with prostate cancer who develop biochemical failure after radiotherapy, European guidelines recommend reimaging with 68Ga-PSMA-11 PET/CT and multiparametric MRI (mpMRI). However, the accuracy of 68Ga-PSMA-11 PET/CT for detecting intraprostatic recurrences is unclear, both with and without mpMRI. Methods: A single-center retrospective study of a series of patients investigated for radiorecurrence between 2016 and 2022 is described. All patients underwent 68Ga-PSMA-11 PET/CT, mpMRI, and prostate biopsy. PET/CT images were interpreted independently by 2 expert readers masked to other imaging and clinical data. The primary outcome was the diagnostic accuracy of PET/CT versus mpMRI and of PET/CT with mpMRI together versus mpMRI alone. The secondary outcome was the proportion of cancers missed by mpMRI but detected by PET/CT. Diagnostic accuracy analysis was performed at the prostate hemigland level using cluster bootstrapping. Results: Thirty-five men (70 hemiglands) were included. Cancer was confirmed by biopsy in 43 of 70 hemiglands (61%). PET/CT sensitivity and negative predictive values (NPVs) were 0.89 (95% CI, 0.78–0.98) and 0.79 (95% CI, 0.62–0.95), respectively, which were not significantly different from results by MRI (sensitivity of 0.72; 95% CI, 0.61–0.83; P = 0.1) (NPV of 0.59; 95% CI, 0.41–0.75; P = 0.07). Specificity and positive predictive values were not significantly different. When PET/CT and MRI were used together, the sensitivity was 0.98 (95% CI, 0.92–1.00) and NPV was 0.93 (95% CI, 0.75–1.00), both significantly higher than MRI alone (P = 0.003 and P < 0.001, respectively). Specificity and positive predictive values remained not significantly different. MRI missed 12 of 43 cancers (28%; 95% CI, 17%–43%), of which 11 of 12 (92%; 95% CI, 62%–100%) were detected by PET/CT. Conclusion: For detecting intraprostatic radiorecurrence, 68Ga-PSMA-11 PET/CT has high sensitivity that is not significantly different from mpMRI. When 68Ga-PSMA-11 PET/CT and mpMRI were used together, the results conferred a significantly greater sensitivity and NPV than with mpMRI alone. 68Ga-PSMA-11 PET/CT may therefore be a useful tool in the diagnosis of localized radiorecurrence.
Over 13,000 men with prostate cancer undergo radiotherapy each year in the U.K. alone (1). However, 25% will develop biochemical failure within 10 y (2). Subsequent outcomes are poor; within 5 y, 50% develop metastases and 20%–30% die from their cancer (3). Approximately 10% of biochemical failure patients will develop prostate-confined recurrence, a state independently predictive of metastasis and cancer-specific death (4). Salvage treatments for localized recurrences have shown good medium-term oncologic outcomes and should be considered (5,6). However, patient selection is key, requiring accurate detection of any intraprostatic radiorecurrence (7).
On reaching biochemical failure, European guidelines recommend reimaging with prostate multiparametric MRI (mpMRI) and prostate-specific membrane antigen (PSMA) PET/CT (8). Although mpMRI is highly accurate in the untreated prostate, its interpretation after radiotherapy is challenging because of glandular atrophy, reduced zonal differentiation, and diffuse T2 hypointensity (9). Our group recently published the FORECAST U.K. prospective multicenter trial, which concluded that MRI and MRI-targeted biopsy had high sensitivity for radiorecurrent cancer detection, but systematic biopsies were also needed to identify MRI-invisible disease (6,10).
68Ga-PSMA-11 PET/CT is increasingly used for whole-body imaging after previous treatment, with excellent specificity for identifying extraprostatic disease (11). However, data regarding detection of intraprostatic recurrences are fewer and less robust, with most studies omitting verification of findings against a histologic reference (12). This contrasts with the primary diagnostic setting; the recently published PRIMARY trial identified that 68Ga-PSMA-11 PET/CT and mpMRI used together significantly improve sensitivity and negative predictive values (NPVs) versus mpMRI alone for detecting clinically significant disease (13). We therefore hypothesized that 68Ga-PSMA-11 PET/CT, both with and without mpMRI, may be useful for detecting local failures after radiotherapy and identifying candidates for local salvage. We sought to address this using a robust biopsy reference standard.
MATERIALS AND METHODS
Study Design
This single-center retrospective study was approved by the local institutional review board, and the requirement to obtain informed consent was waived. All patients who had undergone 68Ga-PSMA-11 PET/CT imaging were reviewed. Patients were included if they underwent both 68Ga-PSMA-11 PET/CT and mpMRI with prostate biopsy to investigate for radiorecurrence. No restrictions were placed on the type of radiotherapy or the use of androgen deprivation therapy. Other local treatment before imaging was prohibited.
Index Tests
All 68Ga-PSMA-11 PET/CT examinations were performed on Siemens Healthineers scanners (Biograph 64 scanner, attenuation-corrected reconstruction, n = 28; Biograph 128 scanner, time-of-flight attenuation-corrected reconstruction, n = 2; Biograph Vision scanner; time-of-flight point-spread function reconstruction with 4.5-mm gaussian filter, n = 5). This comprised standard knees-to-vertex acquisitions (mean, 61 min after injection) and delayed postmicturition pelvic acquisitions (mean, 91 min after injection). Diuretics were not used. The mean activity of the administered radiotracer was 1.9 MBq/kg. Two expert readers, masked to clinical information and previous imaging, independently interpreted images using Hermia software (Hermes Medical Solutions). The prostate was divided into hemiglands (left/right). Suspicion of radiorecurrence within each hemigland was scored with a 5-point Likert system, with a score of 3–5 deemed suspicious (Fig. 1). Where there was a score discrepancy between the readers, the higher score was chosen for analysis. A 5-point Likert score was chosen as it aligned with E-PSMA guidance (14). Furthermore, the PRIMARY score had not been developed at the time of analysis and was designed for use in the untreated prostate (15).

Explanation and examples for 5-point Likert system used for PET/CT interpretation.
MRI was performed per the Prostate Imaging–Reporting and Data System guidelines on a 1.5- or 3.0-T scanner with a multiparametric protocol incorporating T2-weighted images, diffusion-weighted images with apparent diffusion coefficient mapping and at least 1 high b-value acquisition, and dynamic contrast-enhanced images. Examinations were reported by specialist prostate MRI radiologists, who were not masked, and were interpreted binarily as either suspicious or nonsuspicious. A binary score was chosen to reflect simplified clinical decision-making on whether to recommend biopsy based on MRI. The new Prostate Imaging–Recurrence Reporting criteria were not used for interpretation as these had not been validated at the time of analysis (16).
Reference Test
All patients underwent biopsy to confirm recurrence with a view to offering salvage local treatment. All had bilateral sampling of the peripheral zone as the minimum via targeted or systematic cores. Of 35 patients, 33 (94%) underwent biopsy via the transperineal route.
Outcomes
Analyses were performed at the prostate hemigland level. The primary outcomes were the diagnostic accuracy metrics of PET/CT versus MRI and of PET/CT with MRI compared with MRI alone. When PET/CT and MRI were used together, if either modality detected a suspicious lesion, the test was deemed positive. Figures 2–4 illustrate comparative examples.

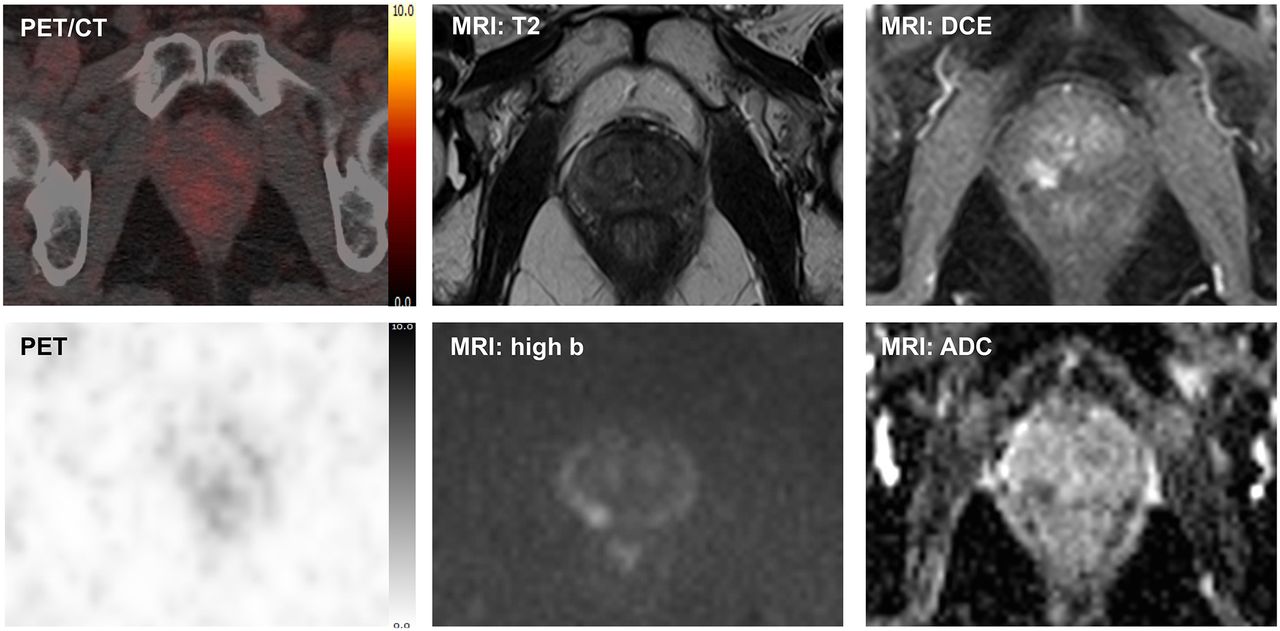
Comparison of 68Ga-PSMA-11 PET/CT (positive) and mpMRI (positive). Patient was reimaged 6.3 y after diagnosis, had current prostate-specific antigen of 3.1 ng/mL, and was previously treated with external-beam radiotherapy and neoadjuvant and adjuvant androgen deprivation therapy. On PET/CT, right apex demonstrated Likert score 5/5 lesion with SUVmax of 11.1. MRI demonstrated corresponding restricted diffusion with intense contrast enhancement. Targeted biopsy revealed grade group 3 cancer with maximum cancer core length of 15 mm. ADC = apparent diffusion coefficient; DCE = dynamic contrast enhancement.

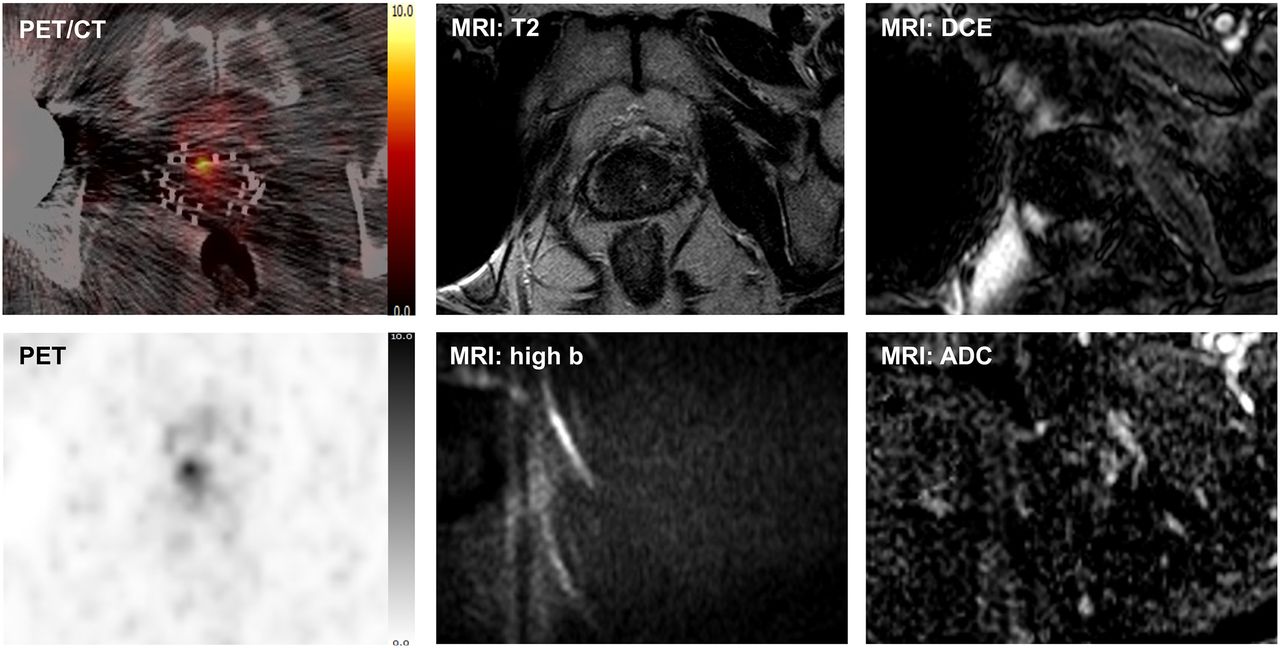
Comparison of 68Ga-PSMA-11 PET/CT (positive) and mpMRI (negative). Patient was reimaged 16.2 y after diagnosis, had current prostate-specific antigen of 4.6 ng/mL, and was previously treated with low–dose-rate brachytherapy. On PET/CT, right mid gland and base demonstrated Likert score 5/5 lesion with SUVmax of 9.1. MRI interpretation was hindered by artifact from right hip replacement and brachytherapy seeds. Targeted biopsy revealed grade group 3 cancer with maximum cancer core length of 1 mm. ADC = apparent diffusion coefficient; DCE = dynamic contrast enhancement.

Comparison of 68Ga-PSMA-11 PET/CT (negative) and mpMRI (positive). Patient was reimaged 4.8 y after diagnosis, had current prostate-specific antigen of 2.4 ng/mL, and was previously treated with external-beam radiotherapy and neoadjuvant androgen deprivation therapy. MRI demonstrated restricted diffusion in right mid gland. In this region, PET/CT was scored as Likert 1/5, with SUVmax of 2.1. Targeted biopsy revealed cancer with maximum cancer core length of 6 mm. Gleason grading was not possible because of irradiation effect. ADC = apparent diffusion coefficient; DCE = dynamic contrast enhancement.
Several secondary outcomes were analyzed. First, the proportion of hemiglands correctly classified by each modality, the proportion of cancers missed by each modality, and the number of cancers missed by MRI but detected by PET/CT were compared. Second, the characteristics of cancers detected by PET/CT versus undetected cancers were compared. Third, the optimal SUVmax cut point was determined that would maximize sensitivity and specificity for detecting cancer. The accuracy of other SUVmax cut points in 1.0 increments between 2.0 and 15.0 was also evaluated.
Because the role of Gleason grading after radiotherapy is not well established, analyses focused on detecting cancer of any grade and length (any cancer). Analyses were also performed with clinical significance definitions used in the primary diagnostic setting: a grade group of at least 3 or maximum cancer core length of at least 6 mm (definition 1), and a grade group of at least 2 or maximum cancer core length of at least 4 mm (definition 2) (17). Patients were excluded from calculations if an undeterminable grade or maximum cancer core length meant it was not possible to apply the definition.
As a sensitivity analysis, outcomes were recalculated using a Likert threshold of at least 4 for 68Ga-PSMA-11 PET/CT. Analyses were also performed at the whole-gland level (Appendix 1; Supplemental Tables 7–10; Supplemental Figs. 3 and 4 [supplemental materials are available at http://jnm.snmjournals.org]).
Statistical Analysis
Interreader agreement for Likert scores was determined by calculating Cohen κ. For calculating diagnostic accuracy at the hemigland level, to account for nonindependent data among individual patients, cluster bootstrapping with 1,000 resamples was performed to generate a 95% CI. Sensitivity and specificity were compared between diagnostic tests using the McNemar test (18). Positive predictive values (PPVs) and NPVs were compared using a general estimating equation logistic regression model (19).
For comparison of proportions of hemiglands correctly classified and cancers missed, the Fisher exact test was used. The 95% CIs were calculated using the adjusted Wald method.
To compare characteristics between imaging-detected and -undetected cancers, the Fisher exact test was used for categoric variables, the Wilcoxon rank-sum test for continuous variables, and the χ2 test for trends in ordinal variables.
For determining optimal SUVmax cut points, receiver-operating-characteristic curve analyses were performed and the curves plotted. Cluster bootstrapping was used to generate a 95% CI. Smoothed receiver-operating-characteristic curves were plotted from bootstrapped samples. SUVmax here referred to the highest value of the standard and delayed acquisitions.
All analyses were performed with R version 4.2.2. Statistical significance was set as a P value of less than 0.05.
RESULTS
Cohort Description
Thirty-five men (35 scans; 70 hemiglands) were included in this analysis. Figure 5 gives exclusion reasons. Table 1 describes cohort characteristics.

Flowchart outlining eligibility process. PSA = prostate-specific antigen.
Characteristics of Included Patients (n = 35)
Primary Outcomes
Cancer was confirmed by biopsy in 43 of 70 hemiglands (61%), with 37 of 65 (57%) and 40 of 67 (60%) harboring definition 1 and definition 2 cancer, respectively. Of the 70 (67%) hemiglands, 47 had a suspicious PET/CT (Likert score of 3–5) and 41 of 70 (59%) had a suspicious MRI. When both modalities were used together, 57 of 70 (79%) hemiglands were deemed suspicious.
On categorizing Likert scores as 1–2 versus 3–5, there was substantial interrater agreement (κ = 0.65; 95% CI, 0.48–0.83). Table 2 details the diagnostic accuracy metrics. For detection of any cancer, PET/CT sensitivity was 0.89 (95% CI, 0.78–0.98), which was not significantly different from MRI (0.72; 95% CI, 0.61–0.83; P = 0.1). Specificity was not significantly different between PET/CT (0.67; 95% CI, 0.48–0.86) and MRI (0.64; 95% CI, 0.44–0.83; P = 0.8). Furthermore, neither PPV nor NPV was significantly different between modalities.
Diagnostic Metrics for Imaging Modalities
When both modalities were used together, sensitivity was 0.98 (95% CI, 0.92–1.00) and the NPV was 0.93 (95% CI, 0.75–1.00), both significantly higher than with MRI alone (P = 0.003 and P < 0.001, respectively). Specificity was 0.45 (95% CI, 0.27–0.67), and PPV was 0.74 (95% CI, 0.61–0.87), which were not significantly different from the results with MRI alone (P = 0.07 and 0.6, respectively).
For definition 1 and definition 2 cancers, the diagnostic metrics for each modality used alone were comparable to detection of any cancer, with no significant differences detected (Table 2). When modalities were used together, sensitivity and NPV were again significantly higher than with MRI alone. For definition 1 only, the specificity of the combined modalities (0.44; 95% CI, 0.27–0.63) was significantly reduced versus MRI (0.65; 95% CI, 0.46–0.84; P = 0.04). PPV estimates were not significantly different for either definition.
Supplemental Table 1 details the diagnostic accuracy metrics when the Likert score threshold was increased to at least 4. Substantial interrater agreement remained when categorizing Likert scores here as 1–3 versus 4–5 (κ = 0.72; 95% CI, 0.55–0.88). With this new threshold, 40 of 70 (57%) and 52 of 70 (74%) hemiglands were suspicious on PET/CT alone and on PET/CT with MRI, respectively. Similar to a Likert threshold of at least 3, diagnostic metrics were not significantly different between PET/CT alone and MRI. However, when used together, sensitivity and NPV were significantly higher than with MRI alone. These patterns were preserved for all cancer definitions.
Secondary Outcomes
MRI missed 12 of 43 cancers (28%; 95% CI, 17%–43%), and PET/CT missed 5 of 43 (12%; 95% CI, 5%–25%), a nonsignificant difference (P = 0.1; Supplemental Table 2). Although 11 of 12 cancers (92%; 95% CI, 62%–100%) were missed by MRI, they were detected by PET/CT. For definition 1 and definition 2, 8 of 9 (89%; 95% CI, 54%–100%) and 9 of 10 (90%; 95% CI, 57%–100%) tumors undetected by MRI were detected by PET/CT. With a Likert threshold of at least 4, PET/CT detected 75%–80% of MRI-missed cancers (Supplemental Table 3).
Aside from SUVmax, there were no significant differences observed with regard to tumor characteristics for cancers detected and undetected by PET/CT (Supplemental Table 4). These results were consistent when a Likert threshold of at least 4 was used (Supplemental Table 5).
Supplemental Figure 1 details the characteristics of the 5 tumors undetected by PET/CT. All PET/CT examinations were performed on a Biograph 64 scanner. Three of these had cancer detected in the contralateral hemigland both on PET/CT and on biopsy, with 1 of these likely reflecting midline extension of a medial tumor contralaterally. All 5 undetected tumors fulfilled definition 1 criteria (grade group ≥ 3 or maximum cancer core length ≥ 6 mm), the most stringent clinical significance definition used. One patient had received adjuvant androgen deprivation therapy at the time of the PET/CT imaging; 2 patients had not, and for 2 patients, these data were not available. No tumor displayed neuroendocrine differentiation.
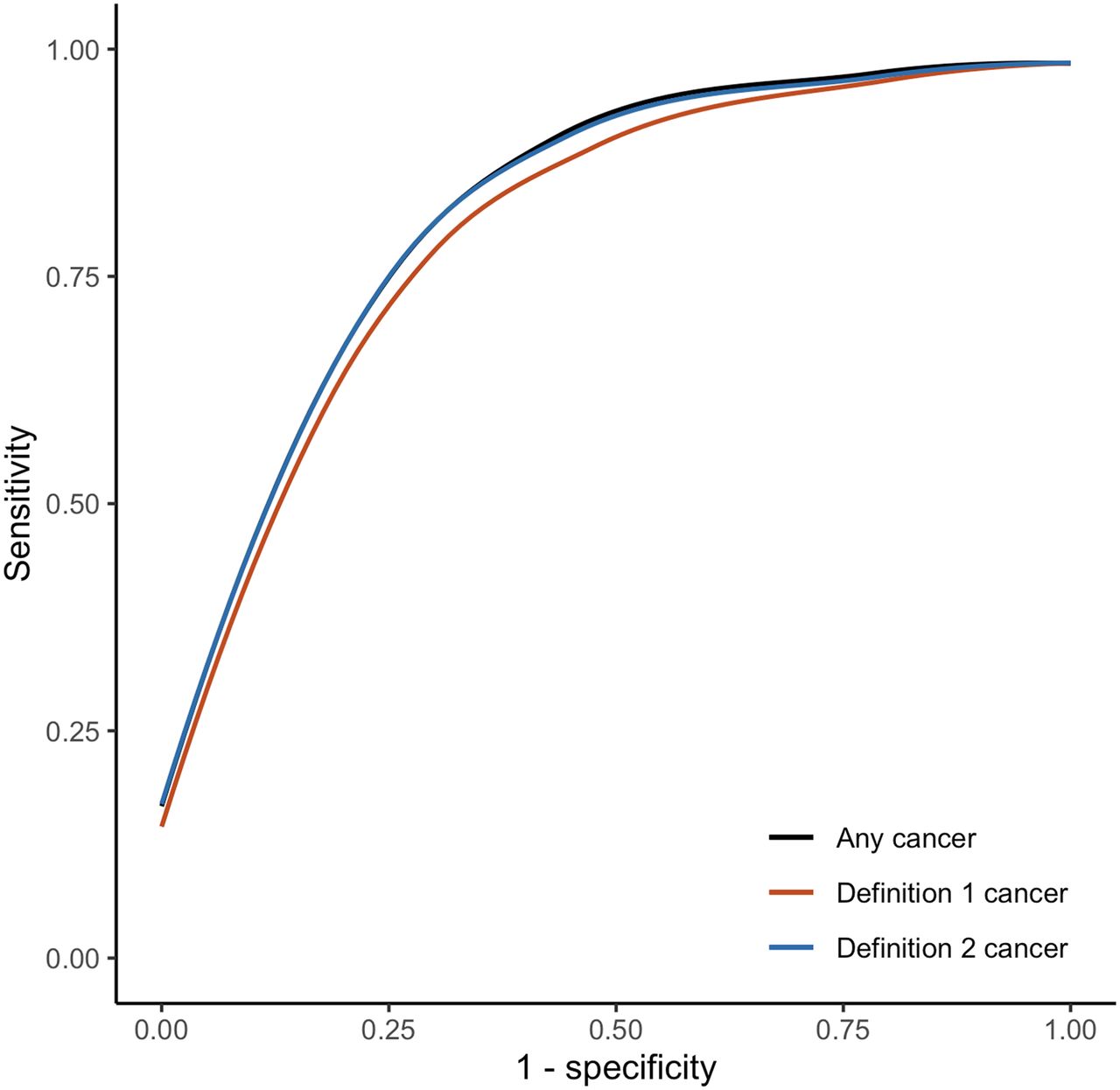
Figure 6 displays the receiver-operating-characteristic analysis to determine optimal SUVmax cut points; Supplemental Table 6 and Supplemental Figure 2 detail the diagnostic accuracy metrics for these cut points. With SUVmax, the area under the curve for any cancer was 0.83 (95% CI, 0.71–0.92); for definition 1, it was 0.81 (95% CI, 0.69–0.90), and for definition 2, it was 0.82 (95% CI, 0.71–0.92). For all definitions, an SUVmax of 4.4 yielded the greatest combination of sensitivity and specificity. With this cut point, across cancer definitions, sensitivity ranged from 0.84 to 0.86, specificity from 0.79 to 0.82, PPV from 0.85 to 0.88, and NPV from 0.48 to 0.78.

Smoothed receiver-operating-characteristic curves plotted for each cancer definition based on SUVmax.
DISCUSSION
Summary
68Ga-PSMA-11 PET/CT has high sensitivity and modest specificity for detecting intraprostatic radiorecurrent cancer measured against biopsy. mpMRI also has good sensitivity with comparatively lower specificity, consistent with FORECAST findings (6). The use of both modalities together, however, conferred a significantly greater sensitivity and NPV than with MRI alone across all cancer definitions. Notably, 89%–92% of cancers missed by MRI were detected by PET/CT imaging. Within the limitations of our small, highly selected cohort, these data suggest that using 68Ga-PSMA-11 PET/CT and mpMRI together could be an excellent tool for ruling out local failure after radiotherapy. An inherent further advantage of 68Ga-PSMA-11 PET/CT is its established utility in detecting extraprostatic spread. A concern raised, in contrast, is that the low specificity across modalities indicates these tests do produce many false-positive results. PPV, however, was fair when both modalities were used together (0.70–0.74).
Pathologic characteristics were not significantly different between PET/CT-detected and -undetected tumors in this small cohort. This remains an area needing investigation in larger studies (10). Nonetheless, all 5 tumors that PET/CT missed satisfied definition 1 criteria and, at least in the primary diagnostic setting, would be deemed aggressive tumors.
An optimal SUVmax cut point of 4.4 across each cancer definition conferred high sensitivity and specificity. This cut point could represent a useful metric for quantitative image assessment.
Comparison to Literature
Our results are comparable to primary diagnostic data. For detection of cancer with a grade group of at least 2, the PRIMARY trial determined 68Ga-PSMA-11 PET/CT to have a sensitivity of 0.90, a specificity of 0.50, a PPV of 0.69, and an NPV of 0.80 (13). When combined with mpMRI, the sensitivity was 0.97, with a specificity of 0.40, a PPV of 0.67, and an NPV of 0.91. Sensitivity and NPV compared between PET/CT and MRI alone were not significantly different; however, the sensitivity and NPV of the combined modalities were significantly greater than with MRI alone.
PSMA PET/CT is increasingly used after radiotherapy and is advocated by the European guidelines (8). However, relevant data are mostly weak as many studies omit a histologic reference standard (12). This is problematic; false positives are common in the irradiated prostate as we also demonstrate in our own data, often due to faint-to-moderate prostatic uptake and inflammation (20). Furthermore, when histologic data are provided, these are frequently and inappropriately amalgamated with histologic data from postprostatectomy patients or extraprostatic sites (12).
A 2022 review by our group identified just 3 studies presenting histology-verified prostatic imaging findings after PSMA PET/CT for radiorecurrence (12). Our findings are concordant, principally in that PSMA PET/CT with or without mpMRI has high sensitivity for detecting radiorecurrent disease. In a German retrospective 68Ga-PSMA-11 series of 50 patients undergoing salvage radical prostatectomy, sensitivity on a hemigland basis was 81% and specificity was 67% (21). The method of PET/CT interpretation, however, was not reported. In an Australian retrospective 68Ga-PSMA-11 series (n = 267), 33 of 90 patients with isolated local recurrence on PET/CT underwent biopsy, conferring a sensitivity of 85% (22). Local recurrence here was defined as a moderately or intensely avid lesion with an SUVmax of at least 3.0. A third, prospective, American 18F-DCFPyL series (n = 30) reported positive intraprostatic lesions in 15 patients, defined as uptake above background. Three of the 15 patients underwent prostate biopsy, with recurrence confirmed in all (sensitivity, 100%) (23). Since this review, a Dutch group has published prospective data from 41 men undergoing biopsy for a suggestive focus on both 68Ga-PSMA-11 PET/CT and mpMRI (24). Using both modalities in conjunction, sensitivity was 100% at the whole-gland level with 1 false-positive reading (PPV, 98%). This study defined a positive intraprostatic lesion as focal increased uptake. Importantly, in all 4 studies, biopsy was performed only in patients with a positive PET/CT image. In contrast, our study included 4 patients with negative PET/CT, and the use of a hemigland analysis also increased the number of units for analysis with negative imaging. Furthermore, only the last study evaluated the performance of mpMRI alongside PET/CT, a central element of our analysis (23).
Implications for Practice
Many patients with radiorecurrence are managed with watchful waiting or androgen deprivation therapy. The latter carries bothersome side effects and potentially serious adverse events, with castration-resistant disease developing after 2–3 y, necessitating expensive second- and third-line treatments (25).
One study of 128 radiorecurrent patients with positive 68Ga-PSMA-11 PET/CT imaging from 3 prospective trials observed that 36% had uptake confined to the prostate only (26). For these patients, some centers offer salvage radical prostatectomy or reirradiation. Though effective, these can have considerable toxicity. This is particularly the case for radical prostatectomy, which can lead to erectile dysfunction in nearly all patients, urinary incontinence in 80% of patients, and rectal injury in 5%–10% of patients (5,27). An emerging alternative is salvage focal ablation, for example, with high-intensity focused ultrasound or cryotherapy, which targets the recurrent lesion or lesions alone. Early data suggest that this approach provides good early disease control comparable to whole-gland treatments but with reduced toxicity (5,6).
Patient selection for focal ablation is crucial; beyond establishing the presence of localized recurrence, meticulous mapping of disease is needed for treatment planning (7). In this context, our findings suggest that 68Ga-PSMA-11 PET/CT and mpMRI, if both negative, can convincingly rule out intraprostatic recurrence. Furthermore, the FORECAST trial demonstrated that MRI and MRI-targeted biopsy misses 8% of cancers (6); our results show that 68Ga-PSMA-11 PET/CT does detect most tumors missed by MRI. Given that performing both mpMRI and 68Ga-PSMA-11 PET/CT is advocated by guidelines for restaging men with suspected radiorecurrence, we therefore recommend that intraprostatic findings from each imaging modality should be integrated to improve diagnostics (8).
Limitations
Our study is a small, single-center retrospective cohort. However, our cohort does include patients referred from elsewhere for 68Ga-PSMA-11 PET/CT and salvage focal ablation. Furthermore, our cohort size is comparable to the aforementioned studies, reflecting the paucity of radiorecurrence patients undergoing biopsy and the paucity of patients subsequently undergoing salvage focal ablation (5,12,21–24).
Although we have included patients with negative imaging, in contrast to previous studies, our use of a biopsied cohort does confer some selection bias. Ultimately, this cohort comprises patients in whom extraprostatic disease has been ruled out and who are both fit and willing to undergo salvage intervention, having already undergone radiotherapy several years previously. On a related note, biopsy protocols were not uniform, and therefore, bias may arise from this, although the majority were transperineal and all included bilateral sampling sufficient for prostate mapping.
Further Research
Biopsy verification should be a core element of future studies, which should also be designed to overcome the aforementioned limitations (12). We believe our preliminary data encourage development of a well-designed, paired-cohort, multicenter prospective study that offers template biopsies to patients both with and without a positive PET/CT or MRI, similar to the FORECAST trial (6). This would be vital to establish confidence in PET/CT for ruling out local failures. Although we have included men undergoing biopsy with nonsuspicious PET/CT and MRI, previous studies have offered biopsy only to patients with positive imaging (21–24). Granular histologic data in larger cohorts will also enable better characterization of tumors that are not visible on imaging.
Other considerations also need investigation. First, work into the feasibility of PET/CT-targeted biopsies is needed. Second, 68Ga-PSMA-11 interpretation is not standardized. Validation of the recently published 5-point PRIMARY score in the radiorecurrence setting should be considered (15). Furthermore, small validation studies have shown the potential of the 5-point Prostate Imaging–Recurrence Reporting score in improving MRI interpretation after radiotherapy (16,28). Prostate Imaging–Recurrence Reporting validation was not the focus of our work but certainly warrants future study. Last, although research into hybrid PET/MRI remains at a preliminary stage, future work should aim to compare its performance against PET/CT and MRI in this setting.
CONCLUSION
68Ga-PSMA-11 PET/CT confers high sensitivity for detecting intraprostatic recurrences that are not significantly different from mpMRI when measured against biopsy. However, using 68Ga-PSMA-11 PET/CT and mpMRI together leads to a significantly greater sensitivity and NPV than mpMRI alone. This may be a useful tool for the diagnosis of localized radiorecurrence and thus the selection of patients for salvage focal ablation.
DISCLOSURE
Alexander Light acknowledges research funding from the U.K. National Institute for Heath and Care Research (NIHR) and Imperial Health Charity. Hashim Ahmed, Taimur Shah, and Tara Barwick receive infrastructure support from the NIHR Imperial Biomedical Research Centre. Hashim Ahmed and Taimur Shah also receive infrastructure support from the Imperial College Experimental Cancer Medicine Centre. Hashim Ahmed also receives research funding from Sonablate and Boston Scientific; is a paid scientific advisory board member for Francis Medical; has given lectures for Boston Scientific, Ipsen, and Janssen; and has received funding to attend scientific conferences from Janssen. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the diagnostic performance of 68Ga-PSMA-11 PET/CT compared with mpMRI for detecting intraprostatic radiorecurrent prostate cancer?
PERTINENT FINDINGS: 68Ga-PSMA-11 PET/CT alone had high sensitivity when measured against biopsy. However, combining findings from 68Ga-PSMA-11 PET/CT and mpMRI led to a significantly higher sensitivity and NPV than did mpMRI alone.
IMPLICATIONS FOR PATIENT CARE: Using 68Ga-PSMA-11 PET/CT and mpMRI together may be excellent for ruling out intraprostatic radiorecurrence.
Footnotes
Published online Jan. 11, 2024.
- © 2024 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication August 10, 2023.
- Accepted for publication October 4, 2023.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.