


Abstract
18F-PSMA-1007 is a novel prostate-specific membrane antigen (PSMA)–based radiopharmaceutical for imaging prostate cancer (PCa). The aim of this study was to compare the diagnostic accuracy of 18F-PSMA-1007 with 68Ga-PSMA-11 PET/CT in the same patients presenting with newly diagnosed intermediate- or high-risk PCa. Methods: Sixteen patients with intermediate- or high-risk PCa underwent 18F-PSMA-1007 and 68Ga-PSMA-11 PET/CT within 15 d. PET findings were compared between the 2 radiotracers and with reference-standard pathologic specimens obtained from radical prostatectomy. The Cohen κ-coefficient was used to assess the concordance between 18F-PSMA-1007 and 68Ga-PSMA-11 for detection of intraprostatic lesions. The McNemar test was used to assess agreement between intraprostatic PET/CT findings and histopathologic findings. Sensitivity, specificity, positive predictive value, and negative predictive value were reported for each radiotracer. SUVmax was measured for all lesions, and tumor-to-background activity was calculated. Areas under receiver-operating-characteristic curves were calculated for discriminating diseased from nondiseased prostate segments, and optimal SUV cutoffs were calculated using the Youden index for each radiotracer. Results: PSMA-avid lesions in the prostate were identified in all 16 patients with an almost perfect concordance between the 2 tracers (κ ranged from 0.871 to 1). Aside from the dominant intraprostatic lesion, similarly detected by both radiotracers, a second less intense positive focus was detected in 4 patients only with 18F-PSMA-1007. Three of these secondary foci were confirmed as Gleason grade 3 lesions, whereas the fourth was shown on pathologic examination to represent chronic prostatitis. Conclusion: This pilot study showed that both 18F-PSMA-1007 and 68Ga-PSMA-11 identify all dominant prostatic lesions in patients with intermediate- or high-risk PCa at staging. 18F-PSMA-1007, however, may detect additional low-grade lesions of limited clinical relevance.
Prostate-specific membrane antigen (PSMA) is a transmembrane glycoprotein overexpressed in prostate cancer (PCa) cells. Several radiolabeled PSMA probes have been developed, including that most widely used: 68Ga-PSMA-11. It is well established that 68Ga-PSMA-11 PET/CT is superior to conventional imaging and to choline-based PET/CT for evaluating PCa patients, primarily in the context of biochemical failure but also for staging purposes (1–13). 18F-PSMA-1007 is a novel PSMA-based radiopharmaceutical that has several advantages over 68Ga-PSMA-11. 18F-labeled agents enable large-scale radiosynthesis, allowing for a larger number of patient studies, as compared with the limited quantity obtained from the generator-produced 68Ga. In addition, the longer physical half-life of the 18F radioisotope (half-life, 109 min) allows for central production and distribution to satellite centers. 18F-PSMA-1007 may also offer images of higher spatial resolution than are possible with 68Ga because of the relatively low positron energy of 18F (average β+ energy, 250 keV) (14,15).
Another clear advantage of 18F-PSMA-1007 over 68Ga-PSMA-11, 68Ga-PSMA-617, and the available fluorinated PSMA derivative, 18F-DCFPyL, is the lack of renal excretion and the low urinary activity, which can benefit clinical decision making in cases of local recurrence and unclear lesions near the ureter or urinary bladder (16). 18F-PSMA-1007 has a structural scaffold similar to that of 68Ga-PSMA-617, resulting in similar distribution kinetics. This similarity makes 18F-PSMA-1007 optimal for stratifying patients according to their suitability for therapy with 177Lu-PSMA-617 (17). Recently, 18F-PSMA-1007 was shown to have detection rates comparable to or higher than 68Ga-labeled PSMA ligands in biochemical failure (18,19).
The aim of this study was to compare the findings of 18F-PSMA-1007 PET/CT and 68Ga-PSMA-11 PET/CT in the same patients presenting with newly diagnosed intermediate- or high-risk PCa using histopathology and immunohistochemical staining as reference standards.
MATERIALS AND METHODS
This was a prospective study. 18F-PSMA-1007 and 68Ga-PSMA-11 PET/CT were performed within 15 d of each other (median interval, 6 d) in 16 patients with intermediate-risk PCa (prostate-specific antigen [PSA] of 10–20 ng/mL or Gleason score ≥ 7 or ≥ cT2b) or high-risk PCa (PSA > 20 ng/mL or GS ≥ 8 or cT3) (20) scheduled to undergo radical prostatectomy. The study was approved by the institutional ethical committee (reference number, 0765-17-TLV). This study was also registered with the Israeli Ministry of Health (reference number, MOH_2018-01-11_002026) and with the National Institutes of Health (reference number TASMC-17-ES-0765-CTIL). The study protocol is available as supplemental data (supplemental materials are available at http://jnm.snmjournals.org). All patients gave written informed consent to have 2 consecutive labeled PSMA PET/CT studies.
Findings with the 2 PET tracers were compared with histopathologic findings obtained from radical prostatectomy specimens, considered the reference standard.
Intraprostatic pathologic lesions on PET/CT were drawn on a customized scheme of the prostate (Supplemental Fig. 1) divided into upper, middle, and lower thirds; left or right lobes; central or peripheral regions; and anterior or posterior regions. The same scheme of the prostate gland was used by the uropathologist to specify the location of malignant lesions found on prostatectomy specimens. The nuclear medicine physicians and uropathologists were masked to one another’s results. For the purpose of analysis, the prostate was divided into 6 distinct segments, namely base right/left, mid right/left, and apex right/left.
18F-PSMA-1007 and 68Ga-HBED-CC Synthesis
68Ga-PSMA-11
The 68Ga-PSMA-11 was synthesized using an Isotope Technologies Garching GmBH 68Ge/68Ga generator and a semiautomated module in a good-manufacturing-practice–compliant process (21). The radiolabeling was performed over 5 min using a disposable cassette, labeling kit, and 10 μg of PSMA-HBED-CC (ABX GmBH) precursor dissolved in 1 mL of sodium acetate buffer (0.25 M). The final product identity and purity were confirmed using analytic high-performance liquid chromatography, and radiochemical purity was routinely over 99%. The final product was subjected to quality control analyses in compliance with the European Pharmacopoeia.
18F-PSMA-1007
The 18F-PSMA-1007 was synthesized by a fully automated process as was previously described (22). In brief, after trapping the (18F)/H218O from the target, it was loaded onto an anion exchange column (30PS-HCO3; Macherey Nagel), eluted using 0.65 mL of thiobarbituric acid solution (0.075 M; ABX GmBH), and transferred to the reactor followed by addition of 1.5 mL of acetonitrile (Across Organics) and azeotropic removal of water. PSMA-1007 precursor (1 mg) dissolved in 1 mL of anhydrous dimethyl sulfoxide was then added, and radiolabeling was performed at 90°C for 3 min. The reaction crud was then diluted with 15 mL of 10% ethanol and loaded onto consecutive solid-phase extraction cartridges (PSH+ and C18ec; Macherey Nagel) followed by an additional 10 mL of 15% ethanol. The final product was eluted using 3.5 mL of 40% ethanol, diluted with 16.5 mL of 0.9% NaCl solution, supplemented with 100 mg of sodium ascorbate, and filter-sterilized using a 0.22-μm filter (Cathivex-GV). Identification of the 18F-PSMA-1007 was confirmed by coelution with the reference standard using analytic high-performance liquid chromatography, and the radiochemical purity was 96.3% ± 0.5% (n = 24). The final product quality control was in compliance with previously described acceptance criteria (23).
Imaging Procedure
PET/CT studies were performed on separate days using the Discovery 690 PET/CT system (GE Healthcare). All patients were examined on the same scanner. Patients were instructed to drink 500 mL of water during a 2-h period before acquisition and to void immediately before the start of acquisition. Imaging was done from the tip of the skull to the mid thigh. 68Ga-PSMA-11 was injected 45–80 min before acquisition started (24), and 18F-PSMA-1007 was injected as a bolus 60 min before acquisition.
The CT acquisition was performed using automatic current modulation and 120 kV, and the images were reconstructed to a slice thickness of 2.5 mm. The PET acquisition was performed at 3 min per bed position in 3-dimensional mode, and the images were reconstructed in a 128 × 128 matrix with a pixel size of 5.5 mm and a slice thickness of 3.3 mm. The reconstruction method was VUE Point FX (GE Healthcare), which uses time-of-flight information and includes a fully 3-dimensional ordered-subsets expectation maximization algorithm with 2 iterations, 24 subsets, and a filter cutoff of 6.4 mm. The VUE Point FX algorithm also includes normalization and image corrections for attenuation, scatter, randoms, and dead time. A standard Z-filter was applied to smooth between transaxial slices. The same reconstruction parameters were used for both radiotracers.
Image Analysis
All scans were reviewed by nuclear medicine physicians experienced in interpretation of labeled PSMA PET studies, on a computer-assisted reading application (AW Server, version 3.2; GE Healthcare), which allowed the review of PET, CT, and fused imaging data in axial, coronal, and sagittal slices. Intraprostatic lesions were judged as positive when radiotracer uptake was focal and higher than that of surrounding prostate tissue, as previously described (25,26). Outside the prostate, a pathologic lesion was considered as any soft-tissue or skeletal lesion showing increased uptake above normal surroundings (8,27). Typical pitfalls in PSMA ligand PET imaging were considered (25,28). For calculation of the SUVmax of the primary tumor, volumes of interest were segmented automatically with a manually adapted isocontour threshold centered on lesions with focally increased uptake, as previously described (25).
SUVmax in each segment of the prostate was measured using a 1-cm spheric volume of interest.
Tumor-to-background SUVmax ratio was calculated for each lesion. For background activity, 2-dimensional 2 ± 0.03 cm2 (median ± SD) ROIs were semiautomatically drawn on the normal prostate, left gluteal maximus muscle, and mediastinal blood pool. These areas were chosen as background in accordance with previous studies (13,25). SUVmax was chosen because it is considered more operator-independent and more suitable for smaller lesions (1). SUVmean in the urinary bladder was automatically calculated from volumes of interest that were segmented automatically with a manually adapted isocontour threshold based on physiologic urine uptake and verified using anatomic CT data. SUVmean was chosen because it is more suitable for measuring uptake in a large homogeneous structure such as the bladder.
Surgery
Fifteen patients underwent robot-assisted laparoscopic radical prostatectomy with pelvic lymph node dissection, including removal of lymphatic packages along the internal and external iliac vessels and obturator fossa. One patient had unanticipated evidence of gross metastatic lesions observed during his preoperative workup, and he declined his surgery.
Histopathology and Immunostaining
Radical prostatectomy specimens were embedded in formalin, and the right and left halves of the gland were inked in 2 different colors to maintain its orientation. After sampling the proximal margin (prostate base), the distal apical margin, and the base of each seminal vesicle separately, we sectioned the remaining prostate serially at 5-mm slices from base to apex perpendicular to the urethral axis. The slices were laid out sequentially and divided into an upper third (slices adjacent to the base), a middle third, and a lower third (slices adjacent to the apex). After overnight fixation, representative sections were taken from all thirds. In the absence of whole-mount processing, each slice was further divided into 4 quadrants (right anterior, left anterior, right posterior, and left posterior). Each quadrant was placed in a cassette labeled with its location (e.g., cassette no. 5—upper third, right posterior). Hematoxylin- and eosin-stained slides were prepared from all samples using standard methods. Histologic evaluation and Gleason grading were performed by a dedicated genitourinary pathologist in accordance with criteria established by the International Society of Uropathologists. Tumor areas were mapped according to the location of the samples containing prostatic malignant tissue.
PSMA immunohistochemical staining was performed on selected samples using monoclonal anti-PSMA antibody (clone 3E6, dilution 1/100; Dako). The stained samples were evaluated by 2 pathologists according to the percentage of positively stained cells and the staining intensity (0, no color; +1, weak; +2, moderate; +3, intense).
Statistical Analysis
For statistical analysis, 6 major segments of the prostate were used (base right/left, mid right/left, and apex right/left). Categoric variables were reported as frequency and percentage, and continuous variables were reported as median and interquartile range. The Cohen κ-coefficient was used to assess the concordance between 18F-PSMA-1007 and 68Ga-PSMA-11 for detection of intraprostatic lesions. Interpretation of κ-values was according to Landis and Koch (29). The Wilcoxon test was used to compare SUVmax between 18F-PSMA-1007 and 68Ga-PSMA-11 in the prostate lesions and in the bladder.
The Spearman correlation coefficient was used to assess correlation between SUVmax difference and the following patient characteristics: age, body mass index, Gleason score, PSA, and clinical stage. The McNemar test was used to assess agreement between intraprostatic PET/CT findings and histopathologic findings. The areas under receiver-operating-characteristic curves were calculated for each prostate segment and for all segments pooled together in order to describe the overall and per-segment discriminatory ability between diseased and nondiseased areas for each radiotracer.
The Youden index was used to calculate the optimal SUV cutoff for detecting dominant lesions for each segment and for all segments pooled together. On the basis of these cutoffs, we reported sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for each radiotracer for the 15 patients with a histopathologic reference standard. All statistical tests were 2-sided, and a P value of less than 0.05 was considered statistically significant. SPSS was used for all statistical analyses (version 25.0; IBM Corp., for Windows [Microsoft]).
RESULTS
The patients’ characteristics are summarized in Table 1 and Supplemental Table 1. Patients were categorized into risk groups as previously described (30,31). Labeled PSMA-avid lesions in the prostate were identified in all 16 patients, with almost perfect agreement between the 2 tracers (Supplemental Table 2) regarding tumor location (κ = 0.871–1).
Characteristics of Patients
Median SUVmax in the primary dominant intraprostatic tumors was higher for 18F-PSMA-1007 than for 68Ga-PSMA-11, at 8.73 and 6.94, respectively (P = 0.002). The difference in SUVmax between the 2 tracers, both in prostatic lesions and outside the prostate, was not associated with patient age, body mass index, Gleason score, PSA, or clinical stage (Spearman correlation coefficient was used for this analysis). Normal background median SUVmax was also higher for 18F-PSMA-1007 than for 68Ga-PSMA-11 in all regions of interest measured, including normal prostate (2.57 and 1.85, respectively; P = 0.001), left gluteus maximus muscle (0.675 and 0.53, respectively; P = 0.001), and mediastinal blood pool (1.96 and 0.975, respectively; P = 0.001). No significant difference was found in any lesion-to-background SUVmax ratio between the 2 tracers. Urinary excretion was significantly lower for 18F-PSMA-1007 than for 68Ga-PSMA-11. Median urinary bladder SUVmean was 3.66 and 25.35, respectively (P < 0.001). Ureteric activity was viewed in all 68Ga-PSMA-11 scans, as opposed to only one 18F-PSMA-1007 PET/CT scan (Fig. 1; Supplemental Figs. 2–17).

Maximum-intensity projections, transaxial fusion, and PET images of 18F-PSMA-1007 (A–C) and 68Ga-PSMA-11 (D–F) PET/CT scans of 67-y-old patient with GS 8 and PSA 4.9 ng/mL. Marked uptake is seen in urinary bladder and left ureter (arrow) on maximum-intensity projection image of 68Ga-PSMA-11 (D), as opposed to nearly negligible 18F-PSMA-1007 urinary excretion (A). Dominant lesion in left prostatic lobe is evident on both scans (arrowheads). However, second lesion is seen in right lobe only on 18F-PSMA-1007 scan (arrow in C), later verified on pathology as true malignant lesion.
Aside from the dominant intraprostatic lesion, which was detected by both radiotracers, in 4 patients a second positive focus, though less intense, was detected only by 18F-PSMA-1007 PET/CT. Three of these secondary lesions were confirmed as true-positive sites of prostatic adenocarcinoma with Gleason grade 3 and moderate PSMA staining on pathologic specimens. The fourth lesion evident only on 18F-PSMA-1007 PET/CT was shown on pathologic examination to be a false-positive focus of chronic prostatitis associated with weak positive staining for PSMA.
Median SUVmax was significantly higher in the primary dominant lesion than in secondary lesions detected by 18F-PSMA-1007 (8.73 and 4.2, respectively; P = 0.043). Intraprostatic findings on PET/CT and histopathology are summarized in Supplemental Table 3. Both radiotracers were able to discriminate well between dominant lesions and nondiseased segments of the prostate (Supplemental Table 4). Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for detecting dominant lesions were 100, 90.9, 87.5, 100, and 94.5, respectively, for 18F-PSMA-1007 and 85.7, 98.2, 96.8, 91.5, and 93.3, respectively, for 68Ga-PSMA-11 (Supplemental Table 5). Regarding nondominant lesions, the areas under the curve per segment and for all segments pooled together did not significantly differ from 0.5; therefore, optimal SUV cutoffs were not calculated.
PSMA Immunohistochemical Staining
PSMA immunohistochemical staining of areas with chronic prostatitis and no evidence of carcinoma was weak (+1) in approximately 30% of the cells (Fig. 2A). Compared with these areas, segments with prostatic adenocarcinoma showed stronger staining in a greater percentage of cells. The adenocarcinoma with the higher Gleason grade had more intense staining. The tumor area with Gleason grade 3 showed moderate staining (+2) in 80% of the tumor cells (Fig. 2B), and the adenocarcinoma with Gleason grade 4 had intense staining (+3) in over 90% of the tumor cells (Fig. 2C).
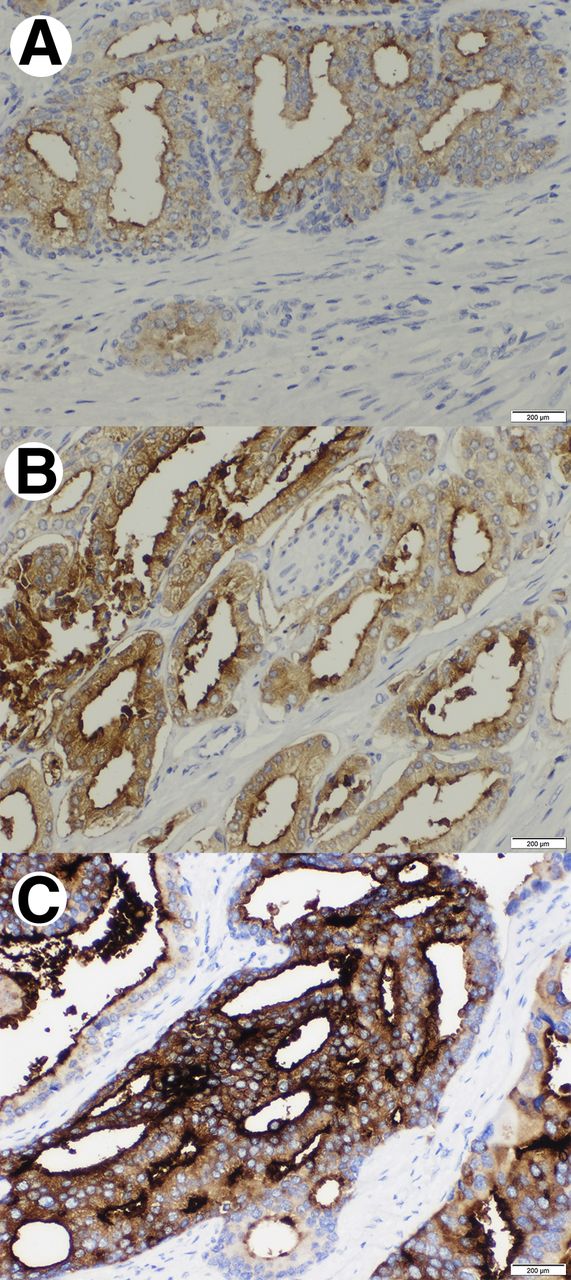
PSMA immunohistochemical stains in 3 different segments. (A) Area with chronic prostatitis showing weak staining (+1) in less than half of cells. (B) Area of prostatic adenocarcinoma, Gleason grade 3, with moderate staining (+2) of most tumor cells. (C) Area of prostatic adenocarcinoma, Gleason grade 4, showing intense staining (+3) in over 90% of tumor cells.
Extraprostatic Disease
No lymph node involvement was suggested in any of patients’ PET/CT scans. Mild uptake was evident in one pelvic lymph node with both tracers and was interpreted as nonspecific. Pathologic examination of this lymph node showed calcification, but no explanation was found for the mild uptake. Overall, 145 lymph nodes were removed and available for pathologic evaluation; all were negative for carcinoma.
Other Findings
One patient had pathologic uptake in a blastic lesion in a thoracic vertebra, detected by both radiotracers and considered to be bone metastasis. Surgery was declined, and the patient was referred for radiation and hormonal therapy. One patient had mild uptake with both tracers (SUVmax of 3.35 and 1.7 for 18F-PSMA-1007 and 68Ga-PSMA-11, respectively) in a sclerotic lesion in a rib compatible with a healing fracture. This patient had undetectable levels of serum PSA at follow-up 8 mo after surgery.
Follow-up
Clinical follow-up was available for 13 patients, with a median postsurgical interval of 173 d. All patients had undetectable levels of serum PSA except for one patient with positive surgical margins, found to have rising PSA levels 2 mo after surgery (from a 0.05 nadir to 0.2). This patient was referred for early salvage radiation therapy.
DISCUSSION
Imaging of PCa is an ongoing challenge, especially in the setting of staging intermediate- and high-risk patients. Previous reports have shown the usefulness of 68Ga-PSMA-11 PET/CT for imaging PCa, as well as its superiority over morphologic imaging in the preoperative setting (1–6). Others have shown 68Ga-PSMA-11 PET/CT to be superior to several other available radiotracers such as choline-based tracers (7,9) and 18F-fluciclovine (32) in patients with recurrent PCa.
18F-PSMA-1007 is a novel radiotracer emerging as an alternative to the routinely used 68Ga-PSMA-11 for evaluating the extent of disease in PCa patients. Recent retrospective studies by Giesel et al. (18) and Rahbar et al. (19) have shown high detection rates with 18F-PSMA-1007 in biochemical failure—rates comparable or superior to those reported for 68Ga-PSMA-11, even in patients with low PSA levels (≤0.5 ng/mL). This finding may have a significant impact on the further management of the disease.
The present study was a prospective head-to-head comparison of the performance of 68Ga-PSMA-11 and 18F-PSMA-1007 in staging intermediate- and high-risk PCa in the same patients using histopathologic and immunohistochemical analysis as the reference standard. The results of this study show good concordance between the radiotracers; both performed equally well and showed high accuracy in detection of the dominant intraprostatic lesion. In view of the near-equal performance of the 2 tracers, this preliminary study suggests the routine use of 18F-PSMA-1007 in lieu of 68Ga-PSMA-11 for staging PCa patients, and clinicians can use either radiotracer based on availability. The present study also provides further validation as to the role of labeled PSMA in the staging of newly diagnosed PCa patients, an indication that has not been studied as extensively as in the biochemical-failure setting.
On the basis of visual analysis, 18F-PSMA-1007 may identify additional low-intensity small intraprostatic lesions, which can result in an increased false-negative rate or detection of clinically irrelevant low-grade tumors. The clinical relevance, if any, of the latter may be limited in the context of treatment of patients with higher-grade dominant lesions.
In view of the almost negligible urinary excretion, 18F-PSMA-1007 may enable a more accurate interpretation of tumor lesions located near physiologic urine uptake. However, this possible advantage was not clearly demonstrated in the present study and should be further explored.
None of the patients included in this study had lymph node involvement, despite the fact that more than half the patients in this small cohort had either high-risk or unfavorable intermediate-risk PCa. Thus, a comparison of the ability of the 2 tracers to detect lymph node involvement could not be done.
Some limitations need to be highlighted. First, this was a small pilot study that needs to be corroborated in a larger cohort. Second, long-term follow-up is still unavailable. Third, 2 patients had false-positive small foci of intraprostatic uptake, irrespective of the dominant lesion, that were actually sites of chronic inflammation. These areas showed weak PSMA staining on immunohistochemistry. Rahbar et al. (33) also showed evidence of false-positive uptake in areas of prostatitis. This should be kept in mind as a potential drawback when interpreting less intense foci of intraprostatic uptake. Administration of furosemide concomitant with 68Ga-PSMA-11, as recommended by some authors (34), was not implemented until recently in our local protocol. This is a major drawback to this study, as uptake of 68Ga-PSMA-11 in the urinary tract would have been lower and might resemble that of 18F-PSMA-1007.
Another major limitation of this study is the different uptake time used for the 2 radiotracers. For 68Ga-PSMA-11, the acquisition was performed between 45 and 80 min after injection, whereas 18F-PSMA-1007 PET/CT was performed 60 min after injection. These uptake periods were derived from the literature (24,34,35). Theoretically, a longer uptake may lead to an improved tumor-to-background ratio (34,35) and result in bias in favor of the tracer for which a longer uptake was applied. However, in a busy routine clinical practice, we failed to perfectly match the uptake time for the 2 tracers.
CONCLUSION
This pilot study shows that both 18F-PSMA-1007 and 68Ga-PSMA-11 identify all dominant prostatic lesions in patients with intermediate- and high-risk PCa at staging. 18F-PSMA-1007, however, may detect additional low-grade lesions of limited clinical relevance.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How does 18F-PSMA-1007 PET/CT perform in comparison to 68Ga-PSMA-11 PET/CT in staging PCa?
PERTINENT FINDINGS: A prospective intraindividual comparison was made between 68Ga-PSMA-11 and 18F-PSMA-1007 for staging PCa in 16 patients scheduled to undergo radical prostatectomy. Histopathologic specimens were used as a reference standard. The results of this study show both radiotracers to have comparably high detectability for the dominant intraprostatic lesion.
IMPLICATIONS FOR PATIENT CARE: The results of this study suggest the routine use of either 18F-PSMA-1007 or 68Ga-PSMA-11 for staging PCa.
Acknowledgments
We thank our dedicated technicians for their contribution to this work.
Footnotes
Published online Sep. 27, 2019.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 18, 2019.
- Accepted for publication August 26, 2019.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Limitations of Retrospective Study Design and Potential Bias in the PRECISE-MDT Study
- Diagnostic Performance of [18F]AlF-Thretide PET/CT in Patients with Newly Diagnosed Prostate Cancer Using Histopathology as Reference Standard
- Protocol for SNOTOB study: radical prostatectomy without prostate biopsy following 18F-PSMA-1007 PET/CT based on a diagnostic model: a single-centre, single-arm, open-label study
- Identification of alternative protein targets of glutamate-ureido-lysine associated with PSMA tracer uptake in prostate cancer cells
- Appropriate Use Criteria for Prostate-Specific Membrane Antigen PET Imaging
- Prostate-specific membrane antigen positron emission tomography compared to multiparametric MRI for prostate cancer diagnosis: a protocol for a systematic review and meta-analysis
- Tumor Detection of 18F-PSMA-1007 in the Prostate Gland in Patients with Prostate Cancer Using Prostatectomy Specimens as Reference Method
- Combination of Forced Diuresis with Additional Late Imaging in 68Ga-PSMA-11 PET/CT: Effects on Lesion Visibility and Radiotracer Uptake
- Matched-Pair Comparison of 68Ga-PSMA-11 and 18F-rhPSMA-7 PET/CT in Patients with Primary and Biochemical Recurrence of Prostate Cancer: Frequency of Non-Tumor-Related Uptake and Tumor Positivity
- Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study
- Intraprostatic Tumor Segmentation on PSMA PET Images in Patients with Primary Prostate Cancer with a Convolutional Neural Network
- Diagnostic Accuracy of 18F-PSMA-1007 PET/CT Imaging for Lymph Node Staging of Prostate Carcinoma in Primary and Biochemical Recurrence
- Factors Predicting Metastatic Disease in 68Ga-PSMA-11 PET-Positive Osseous Lesions in Prostate Cancer