


Abstract
68Ga-PSMA-11 PET is used to stage patients with prostate cancer. We performed an updated metaanalysis that separates imaging at the time of diagnosis and at the time of biochemical recurrence and focuses on pathology correlation in both populations. Methods: We searched the MEDLINE and EMBASE databases using the PRISMA statement. Quality was assessed using the Quality Assessment of Diagnostic Accuracy Studies tool 2. In total, 1,811 studies were screened, 58 were analyzed, 41 were included for qualitative synthesis, and 29 were included for quantitative analysis. A random-effect model and a hierarchical summary receiver-operating-characteristic model were used to summarize the sensitivity, specificity, positive predictive value (PPV), negative predictive value, and accuracy for pelvic lymph nodes in initial staging compared with pathology at prostatectomy and the PPV for lesions with pathologic correlation in those with biochemical recurrence. We also summarized the detection rate of 68Ga-PSMA-11 in those with biochemical recurrence stratified by prostate-specific antigen (PSA) at the time of imaging. Results: The metaanalysis of 68Ga-PSMA-11 at initial staging demonstrated a sensitivity and specificity of 0.74 (95% confidence interval [95% CI], 0.51–0.89) and 0.96 (95% CI, 0.85–0.99), respectively, using nodal pathology at prostatectomy as a gold standard. At biochemical recurrence, the PPV was 0.99 (95% CI, 0.96–1.00). The detection rate was 0.63 (95% CI, 0.55–0.70), with a PSA of less than 2.0 and 0.94 (95% CI, 0.91–0.96) with a PSA of more than 2.0. Conclusion: 68Ga-PSMA-11 performed well for the localization of metastatic prostate cancer at initial staging and at the time of biochemical recurrence.
Staging of patients with prostate cancer using conventional imaging, typically MRI, CT, and bone scans, is limited by a low sensitivity for metastatic disease. Imaging using small molecules targeting the prostate-specific membrane antigen (PSMA) has demonstrated higher detection sensitivity than conventional imaging and other radiotracers such a choline-based agents (1–3). Although there is a large number of radiotracers that target PSMA, 68Ga-PSMA-11 constitutes most of the literature.
Paralleling its widespread clinical adoption, a large number of publications on 68Ga-PSMA-11 PET emerged over the past 4 y. Several metaanalyses have been performed. However, prior metaanalyses are limited by the heterogeneity of included studies: patients at initial diagnosis and at biochemical recurrence were combined, and the reference standard for lesion validation ranged from clinical experience and imaging without predefined criteria to surgery or biopsy in a few cases (4,5). However, to achieve the approval of PSMA ligands for PET imaging, systematic analysis of categorized evidence using histopathology validation is needed. Additionally, since the publication of initial metaanalyses, nearly 3 times as many patients have been reported in the literature.
We therefore focused on the 2 indications for which 68Ga-PSMA-11 PET is most likely to be used clinically: initial staging of those with intermediate- to high-risk prostate cancer and localization of metastatic disease in those with biochemical recurrence after definitive therapy. We performed an updated metaanalysis, separating such patients and correlating findings with pathologic validation. We specifically focused on lesions with pathologic validation to support the potential approval of this drug.
MATERIALS AND METHODS
Search Strategy
The aim of this systematic review and metaanalysis was to summarize studies of staging and restaging 68Ga-PSMA PET/CT or PET/MRI in patients with either localized or metastatic prostate cancer. A second aim was to determine the imaging test accuracy of the new PET/CT and PET/MRI method using tissue samples obtained through biopsy or surgery as the reference standard. We followed the PRISMA guidelines (6). The protocol for this metaanalysis was registered with PROSPERO (Centre for Reviews and Dissemination temporary identification number 99828).
The scientific literature databases MEDLINE and EMBASE were systematically searched in April 2018. Our systematic review included original research studies of initial staging and biochemical recurrence patients with 68Ga-PSMA-11 PET. The search used several key words, including “prostate” or “prostate cancer” or “prostate neoplasm” or “prostate malignancy”; “positron emission tomography” or “PET”; and “prostate specific membrane antigen” or “PSMA” and “PSMA PET” with “prostate.” The search and article selection were performed by 2 independent evaluators. Each screened the titles and abstracts of the reports and selected appropriate original research articles that were published in English. Papers that were excluded included those published before 2012, studies of laboratory results, studies of neoplasms other than prostate cancer, studies of radiotracers that were not 68Ga-PSMA-11, bioavailability studies, case studies, and studies with small sample sizes (<20 patients). Risk for bias in the studies was assessed using the QUADAS-2 methodology (7).
Outcome Measures
We looked at several outcome measurements from the papers reviewed. We calculated imaging test characteristics (sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy) for the detection of lesions in the prostate and pelvic lymph nodes and compared those values with the results of histopathologic biopsy or radical prostatectomy lymph node dissection. Sensitivity is defined as true-positives divided by true-positives plus false-negatives. Specificity is defined as true-negatives divided by true-negatives plus false-positives. PPV is defined as true-positives divided by true-positives plus false-positives. NPV is defined as true-negatives divided by true-negatives plus false-negatives. Accuracy is defined as true-positives plus false-positives divided by the population. We also calculated detection rate in patients by prostate-specific antigen (PSA) cutoffs that had positive imaging results by 68Ga-PSMA-11. Detection rate is defined as the percentage of patients who have focal uptake on 68Ga-PSMA-11 PET that is interpreted as being consistent with cancer.
Data Collection
Two reviewers independently extracted from the studies the radiation dose and uptake time for 68Ga-PSMA PET/CT and PET/MRI. The reviewers also extracted the number of patients in each study, their age (median and mean), PSA (median and range), Gleason score, and initial treatment (androgen deprivation therapy, radiation therapy, or radical prostatectomy). The number of patients detected with PET imaging and the location of the metastases were also extracted.
Metaanalytic Methods
In our metaanalysis, we used a random-effect model (8) and a hierarchical summary receiver-operating-characteristic model (Stata, version 14.0; StataCorp). We summarized the sensitivity, specificity, PPV, NPV, and accuracy for pelvic lymph nodes in initial staging using pathology at prostatectomy as a gold standard, and for any lesion with pathologic correlation in biochemical recurrence patients. We also summarized the detection rate of 68Ga-PSMA-11 in those with biochemical recurrence stratified by PSA at the time of imaging. All point estimates from the metaanalysis regression are reported as the mean and 95% confidence interval (95% CI).
RESULTS
Eligible Studies
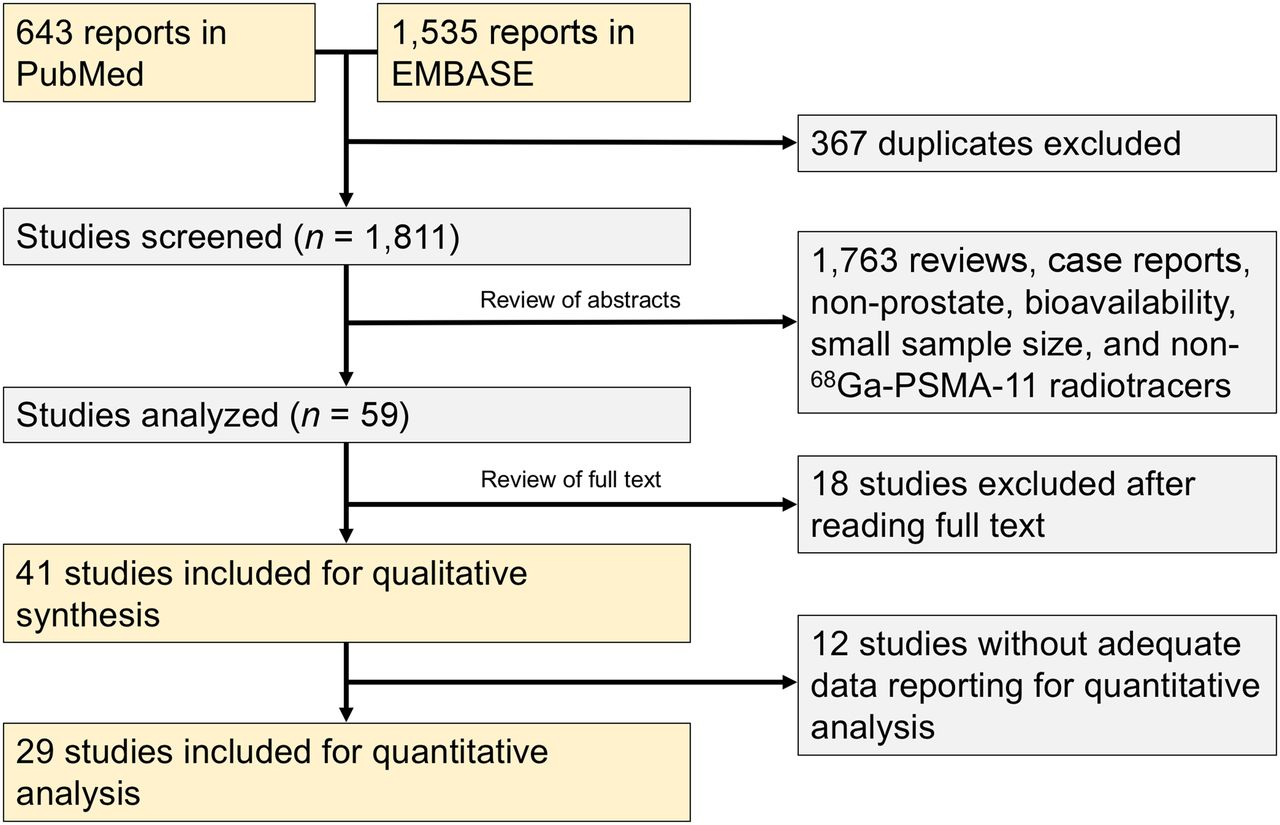
Electronic searching of PubMed and EMBASE resulted in 2,178 articles (Fig. 1). Of these, 367 were duplicates, and 1,811 were reviewed at the abstract level, of which 1,763 were excluded. Subsequently, 59 papers were reviewed in full text, and 18 studies were excluded. Forty-one articles were deemed eligible for inclusion in the metaanalysis (Table 1). Nearly all papers imaged patients roughly 60 min after injection with a dose of 120–230 MBq. Risk for bias and applicability were assessed using the QUADAS-2 tool (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). Significant biases existed in most papers reviewed. Bias concerned the selection of patients, as nearly all studies reported retrospective cohorts without predefined inclusion criteria, and lack of a histologic reference standard, with, again, most papers reporting only detection rates and only a few reporting results compared with histology. Overall, the performance of 68Ga-PSMA-11 PET was fairly consistent across papers, with uptake times and doses in similar ranges. Most of the included papers were retrospective studies that had patients not enrolled on the basis of defined inclusion criteria, and only 4 of the studies were prospectively acquired (Table 1).

PRISMA flow diagram depicting process for selecting papers included in this metaanalysis.
Characteristics of Studies Included
Initial Staging
Six studies in the metaanalysis included patients imaged at initial staging, of which 5 papers correlated pelvic nodal disease to pathology at radical prostatectomy, reporting a total of 266 patients between the 5 studies (Table 2). Most of the papers included only patients who were classified as at intermediate to high risk by the D’Amico classification (Table 2). Across the 5 studies, the metaanalysis of the sensitivity, specificity, PPV, NPV, and accuracy was 0.74 (95% CI, 0.51–0.89), 0.96 (95% CI, 0.85–0.99), 0.93 (95% CI, 0.86–0.99), 0.85 (95% CI, 0.75–0.93), and 0.86 (95% CI, 0.79–0.92), respectively (Fig. 1).
Overview of Included Initial Staging in 5 Studies Reporting Total of 266 Patients
Biochemical Recurrence
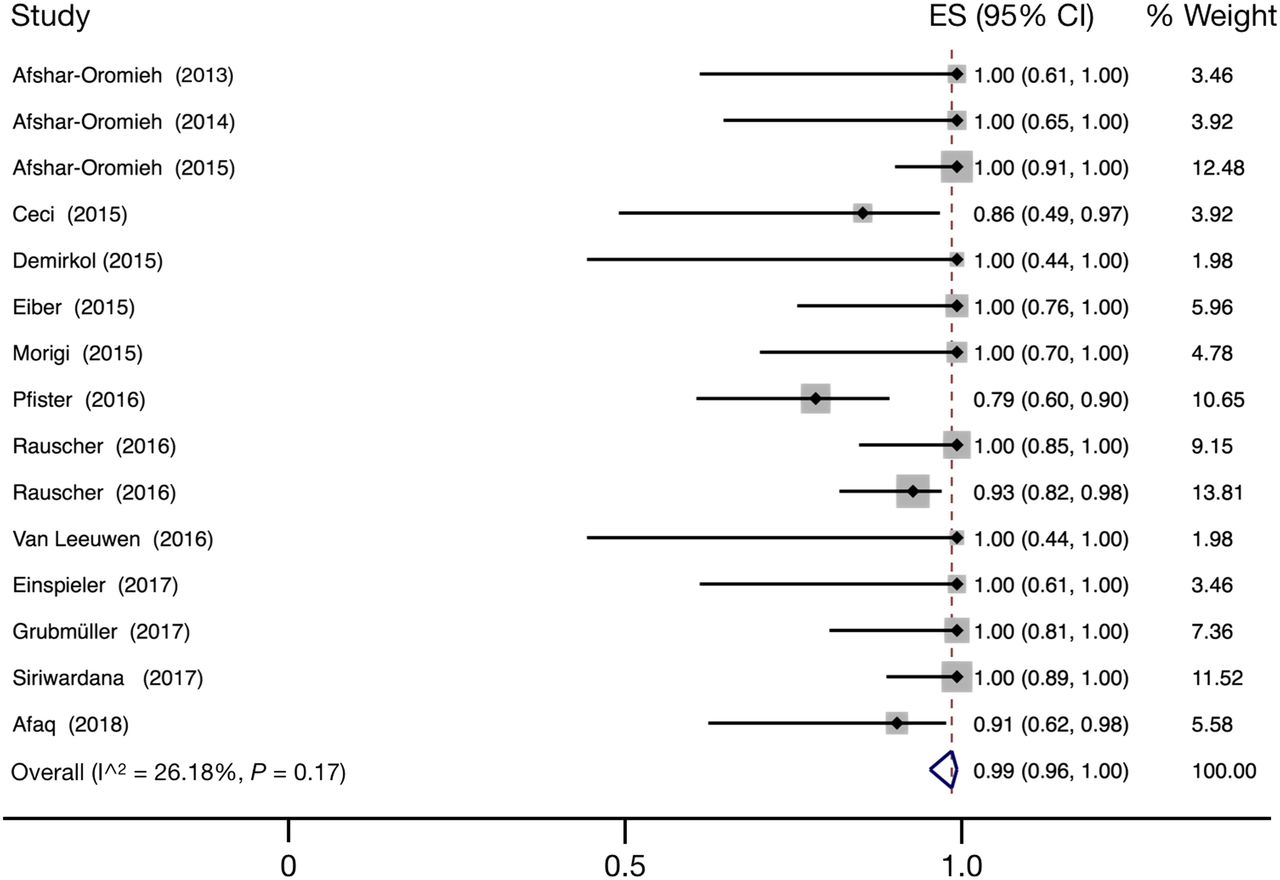
Thirty-four studies in the metaanalysis included patients imaged at biochemical recurrence. First, we reviewed all included papers to determine whether results were reported using pathology as a gold standard and selected all patients for whom a pathology correlation was reported. Most papers on patients with biochemical recurrence did not have pathologic correlation for PSMA-avid lesions, and only detection rates were reported. In total, 256 patients were included across 15 studies with pathologic correlation, of which 233 were reported as true-positive lesions (Table 3). The metaanalysis of the sensitivity, specificity, PPV, NPV, and accuracy in all patients with pathology correlation were 0.99 (95% CI, 0.96–1.00), 0.76 (95% CI, 0.02–1.00), 0.99 (95% CI, 0.96–1.00), 0.76 (95% CI, 0.02–1.00), and 0.98 (95% CI, 0.94–1.00), respectively. Given that only PSMA-positive lesions were biopsied and the resultant low number of true- and false-negative lesions, the most relevant measurement in this population is the PPV (Fig. 2).
Overview of Included Biochemical Recurrence Studies Reporting 256 Patients in Total with Pathology Correlation

Summary of sensitivity, specificity, and hierarchical summary receiver-operating-characteristic (HSROC) curve for 68Ga-PSMA-11 for initial staging of intermediate- to high-risk prostate cancer patients before prostatectomy for malignancy in pelvic nodes, with pathology at time of prostatectomy as gold standard. Effect size for sensitivity and specificity was 0.74 (95% CI, 0.51–0.89) and 0.96 (95% CI, 0.85–0.99), respectively. Size of circles represents size of individual studies.
The reporting of detection rate was heterogeneous across PSA levels, and comparisons across all papers is limited within specific PSA ranges. We grouped papers that reported results with a PSA of less than 2.0 ng/dL, between 2.0 and 5.0 ng/dL, and more than 5.0 ng/dL (Table 4). The metaanalysis for the detection rate for PSAs of less than 2.0 was 0.63 95% CI, (0.55–0.70). For PSAs of 2.0–5.0 the estimate was 0.89 (95% CI, 0.85–0.93) (Fig. 4), and for PSAs of more than 5.0 the estimate was 0.95 (95% CI, 0.92–0.97). We grouped papers that reported detection rates above and below PSAs of 2.0 ng/mL, and we provide a Forest plot of the results (Fig. 3).
Overview of Detection Sensitivity for 68Ga-PSMA-11 PET Stratified by PSA Level at Time of Imaging in 2,616 Patients
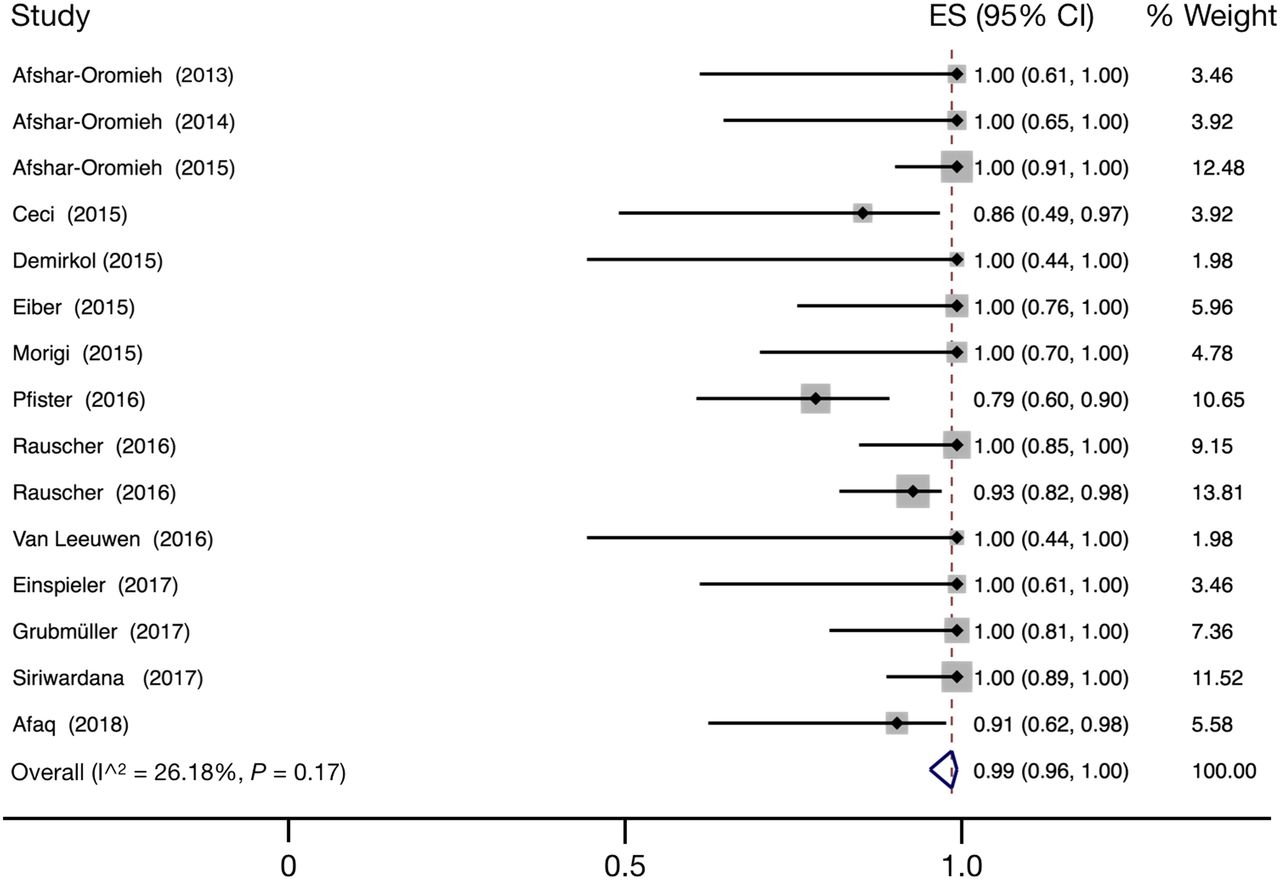
Forest plot of PPV for 68Ga-PSMA-11 in biochemical recurrence patients who have pathologic correlation for gold standard comparison. Overall effect size (ES) for PPV is 0.99 (95% CI, 0.96–1.00). Size of squares represents size of individual studies. Reference numbers are in Table 3.
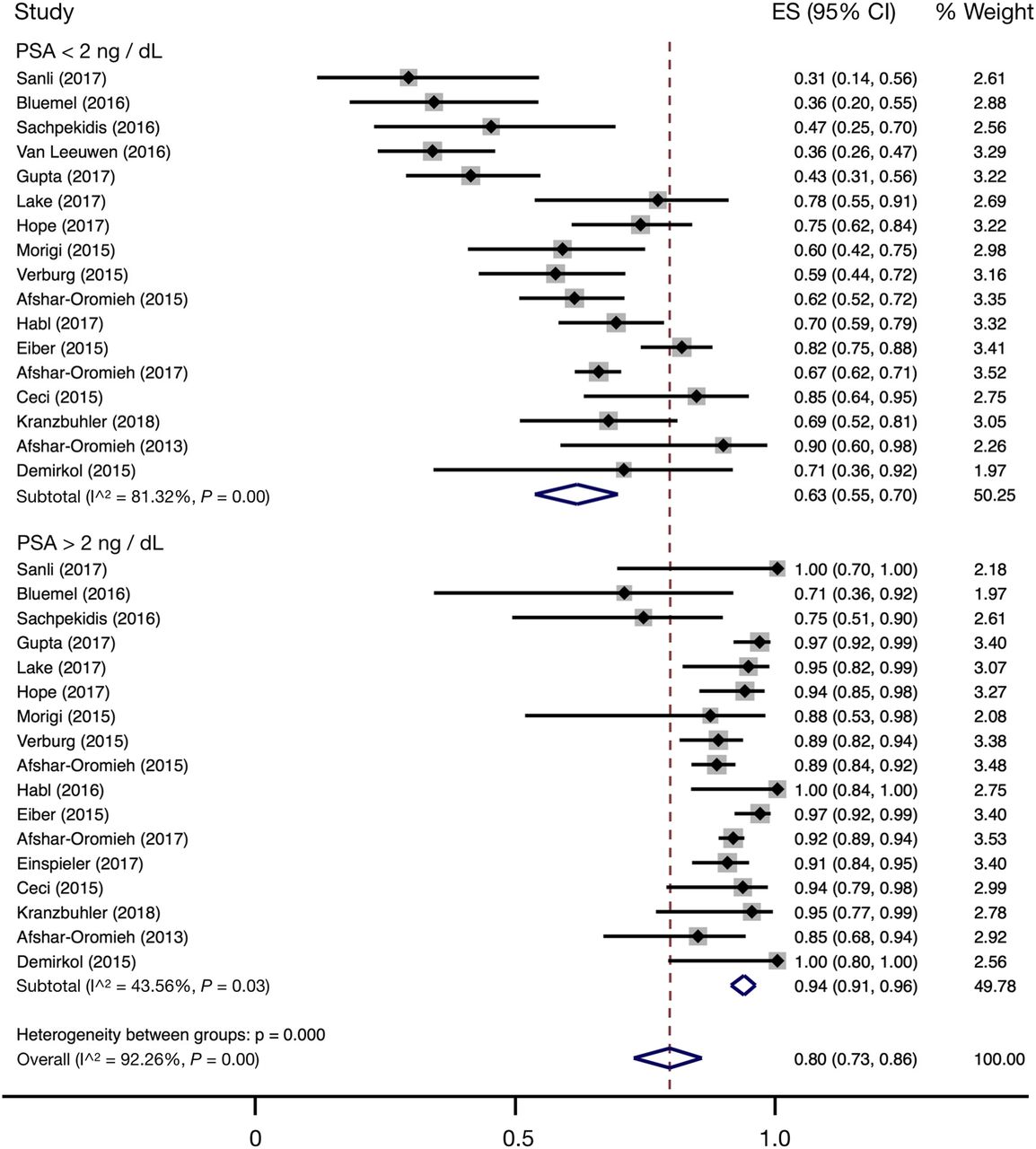
Forest plot of detection rate for 68Ga-PSMA-11 in biochemical recurrence patients. Effect size (ES) for detection rate is 0.63 (95% CI, 0.55–0.70) for PSA < 2.0 ng/dL and 0.94 (95% CI, 0.91–0.96) for PSA > 2.0 ng/dL. Size of squares represents size of individual studies. Reference numbers are in Table 3.
Six papers reported detection sensitivity in patients with a PSA of less than 0.2 ng/mL, although few data were reported on pathology correlation in these papers (9–14). In these papers, 61 of 153 patients were reported as being positive for disease on PSMA PET, and the metaanalysis for the detection rate for PSAs of less than 0.2 was 0.4 (95% CI, 0.24–0.57). The largest study reported 32 of 68 positive for disease when the PSA level was less than 0.2 nd/dL (13).
DISCUSSION
This metaanalysis reaffirms the utility of 68Ga-PSMA-11 PET for imaging of intermediate- to high-risk patients before definitive therapy and those who develop subsequent biochemical recurrence. In initial staging with pathology as a gold standard, 68Ga-PSMA-11 had a sensitivity and specificity of 0.74 (95% CI, 0.51–0.89) and 0.96 (95% CI, 0.85–0.99), respectively, and in biochemical recurrence, the PPV was 0.99 (95% CI, 0.96–1.00). For those patients with biochemical recurrence, the detection rate was 0.63 (95% CI, 0.55–0.70) with a PSA of less than 2.0 and 0.94 (95% CI, 0.91–0.96) with a PSA of more than 2.0.
The sensitivity and specificity results in our study can be difficult to compare with other studies. Perera et al. reported a sensitivity and specificity of 0.86 (95% CI, 0.37–0.98) and 0.86 (95% CI, 0.03–1.00), respectively, but merged data from both biochemical recurrence and initial staging patients (5). A second, more recent, metaanalysis performed only on the initial staging population closely mirrored our results, with estimated sensitivity and specificity of 0.71 (95% CI, 0.59–0.81) and 0.95 (95% CI, 0.87–0.99), respectively (15). von Eyben et al. reported the sensitivity and specificity for initial staging alone—0.70 (95% CI, 0.53–0.83)—and pooled specificity was 0.84 (95% CI, 24–99) (4). The point estimates from von Eyben more closely mirror our results, although our confidence intervals are narrower because of a greater number of patients published since the von Eyben article. von Eyben et al. did not perform a metaanalysis compared with histopathology in the biochemical recurrence setting.
In biochemical recurrence, we chose to report a PPV and not the sensitivity and specificity, as only PSMA-avid lesions are typically biopsied and therefore the subsequent calculated sensitivity and specificity are not relevant. Given that all patients with biochemical recurrence are considered to have disease, the detection rates may be used to approximate the sensitivity for metastatic disease in these patients. It is not possible to biopsy numerous nodes in patients, and therefore the accuracy of 68Ga-PSMA-11 PET outside biopsied lesions is unknown. It is possible that 68Ga-PSMA-11 PET sees only the tip of the iceberg in a large number of patients and that there may be several negative lesions that are not detected and not biopsied.
We chose to limit our analysis to lesions that have a biopsy correlate, because the definition of reference standards varied across the papers that used a composite endpoint of clinical and imaging follow-up. One of the main reasons for the lack of pathology correlation is the difficulty in obtaining a biopsy of lesions in patients with biochemical recurrence at low PSAs. The absence of gold-standard verification makes measurements of accuracy in this population difficult. Given that there is no agreed-upon follow-up composite gold standard, it is not possible to pool data from patients who do not have pathologic validation. Nonetheless, there was a relatively large number of patients (256) reported in the literature with pathologic correlation.
When reporting the results of research radiopharmaceuticals, it is important to consider how the data included may be used to support the subsequent radiopharmaceutical approval. In some cases, literature-based metaanalysis can be used in lieu of a second registration trial, and therefore the quality of studies is critical in support of future approvals. There are several things that are frequently not reported, including safety, inclusion and exclusion criteria, radiopharmaceutical synthesis methods, and quality control method. Using multiple readers and reporting interreader variability is also important in strengthening the value of the results. Dose ranges and uptake times are frequently reported by what is defined in the imaging protocol and not what occurred in individual patients. Another factor that is frequently underdescribed in the literature is the chemistry process (source of the precursor, synthesis module used, generator type, and quality assurance process used), which are important in the registration process so that regulatory bodies know that identical compounds were used across studies. There may be value in developing standard reporting guidelines for studies that evaluate the role of radiopharmaceuticals to ensure high-quality data in the literature moving forward. Furthermore, there may be value in developing harmonized release criteria across sites using the same compound in the research setting to help keep radiopharmaceutical products consistent across sites.
In addition to improved harmonization of reporting in PSMA PET articles, what would greatly strengthen the results in the literature are well-designed prospective studies that include a well-defined gold standard that can be used to measure accuracy. Although this is an optimistic goal, we readily admit that in the setting of biochemical recurrence, this goal may be difficult to achieve given the general frequent inability to obtain histologic verification.
The main limitation of our study is the heterogeneity that exists within the included studies. For example, patients are grouped by varying PSA ranges in the literature, which makes determining the reported sensitivities within various PSA ranges difficult to pool across articles. Additionally, most studies assessing imaging in those with biochemical recurrence did not include pathology correlation and simply reported detection sensitivities. Finally, the interpretive criteria are not defined in all papers, and in the past year reporting standards have been proposed that may limit variability in readings (16,17). One of the main reasons for the heterogeneity across studies using 68Ga-PSMA-11 is that most reports are from institutions using the compound under a compassionate-use setting, and so no formal prospective protocols were developed or followed.
CONCLUSION
68Ga-PSMA-11 performed well for the localization of metastatic prostate cancer. In initial staging, with pathology as a gold standard, 68Ga-PSMA-11 had a sensitivity and specificity of 0.74 (95% CI, 0.51–0.89) and 0.96 (95% CI, 0.85–0.99). In biochemical recurrence, with pathology as a gold standard, the PPV was 0.99 (95% CI, 0.96–1.00). The detection rate was 0.63 (95% CI, 0.55–0.70) with a PSA less than 2.0 and 0.94 (95% CI, 0.91–0.96) with a PSA greater than 2.0.
DISCLOSURE
Thomas Hope receives grant support from the 2017 Jonathan Kovler Young Investigator Award from the Prostate Cancer Foundation, and the National Institutes of Health (R01CA212148). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 7, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication August 21, 2018.
- Accepted for publication November 1, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic Performance of [18F]AlF-Thretide PET/CT in Patients with Newly Diagnosed Prostate Cancer Using Histopathology as Reference Standard
- The Value of 68Ga-PSMA PET/MRI for Classifying Patients with PI-RADS 3 Lesions on Multiparametric MRI: A Prospective Single-Center Study
- The Impact of Baseline PSMA PET/CT Versus CT on Outcomes of 223Ra Therapy in Metastatic Castration-Resistant Prostate Cancer Patients
- Lesion Dosimetry for [177Lu]Lu-PSMA-617 Radiopharmaceutical Therapy Combined with Stereotactic Body Radiotherapy in Patients with Oligometastatic Castration-Sensitive Prostate Cancer
- An Analysis of the Distribution of PSMA PET/CT-Positive Lymph Nodes and Their Coverage by Different Elective Nodal Radiation Volumes in Postoperative Prostate Cancer Patients
- Head-to-Head Comparison of 68Ga-PSMA-11 PET/CT and mpMRI with a Histopathology Gold Standard in the Detection, Intraprostatic Localization, and Determination of Local Extension of Primary Prostate Cancer: Results from a Prospective Single-Center Imaging Trial
- A Comprehensive Assessment of 68Ga-PSMA-11 PET in Biochemically Recurrent Prostate Cancer: Results from a Prospective Multicenter Study on 2,005 Patients
- The European Association of Urology Biochemical Recurrence Risk Groups Predict Findings on PSMA PET in Patients with Biochemically Recurrent Prostate Cancer After Radical Prostatectomy
- Detection Efficacy of 18F-rhPSMA-7.3 PET/CT and Impact on Management in Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy and Before Potential Salvage Treatment
- Positive Predictive Value and Correct Detection Rate of 18F-rhPSMA-7 PET in Biochemically Recurrent Prostate Cancer Validated by Composite Reference Standard
- The PSMA-targeting Half-life Extended BiTE Therapy AMG 160 has Potent Antitumor Activity in Preclinical Models of Metastatic Castration-resistant Prostate Cancer
- Diagnostic Accuracy of 18F-PSMA-1007 PET/CT Imaging for Lymph Node Staging of Prostate Carcinoma in Primary and Biochemical Recurrence
- Impact of 68Ga-PSMA-11 PET/CT on Staging and Management of Prostate Cancer Patients in Various Clinical Settings: A Prospective Single-Center Study
- 11C-Choline PET/CT in Recurrent Prostate Cancer: Retrospective Analysis in a Large U.S. Patient Series
- Differential Expression of Glucose Transporters and Hexokinases in Prostate Cancer with a Neuroendocrine Gene Signature: A Mechanistic Perspective for 18F-FDG Imaging of PSMA-Suppressed Tumors
- Histologically Confirmed Diagnostic Efficacy of 18F-rhPSMA-7 PET for N-Staging of Patients with Primary High-Risk Prostate Cancer
- Appropriate Use Criteria for Imaging Evaluation of Biochemical Recurrence of Prostate Cancer After Definitive Primary Treatment
- The Future of Nuclear Medicine as an Independent Specialty