


Abstract
The objective of this study was to assess the impact of 68Ga-prostate-specific membrane antigen (68Ga-PSMA) PET/CT on the management of prostate cancer in patients with biochemical recurrence (BCR). Methods: Documented management plans before and after 68Ga-PSMA PET/CT in 100 patients with BCR were retrospectively reviewed, and changes in plans were recorded. Results: Management changed after 68Ga-PSMA PET/CT in 39 patients (39%). The management changes occurred in 23 (33.8%) of 68 patients with radical prostatectomy and 16 (50%) of 32 patients previously treated with radical radiotherapy. Positive scan results (P < 0.001) and higher prostate-specific antigen (PSA) levels (P = 0.024) were associated with management changes. No significant association with management change was found for Gleason grade, stage, presence of metastatic disease, PSA velocity, or PSA doubling time. Conclusion: 68Ga-PSMA PET/CT altered management in 39% of patients with BCR, and changes occurred more often in patients with radical radiotherapy treatment, positive 68Ga-PSMA scan results, and higher PSA levels.
The management of biochemical recurrence (BCR) of cancer depends on the location and extent of disease (1). Nomograms can be used to distinguish local and distant relapses with good sensitivity but cannot localize disease and have a limited role in patient-specific therapy planning (2). Early disease detection may allow curative treatment to be offered.
68Ga-prostate-specific membrane antigen (68Ga-PSMA) PET/CT has been rapidly adopted into clinical use. However, few studies have evaluated the influence of 68Ga-PSMA PET/CT on the management of prostate cancer. It is important to evaluate the role of 68Ga-PSMA PET/CT in management changes for the acceptance of this technology by referring physicians for clinical implementation and health care providers for reimbursement.
The purpose of this study was to evaluate the observed changes in the management of prostate cancer in patients with BCR after 68Ga-PSMA PET/CT.
MATERIALS AND METHODS
Summary of Study Design
This study was approved by the local institutional review board, and the need for written informed consent was waived. At a large tertiary referral center (University College London Hospital), consecutive patients who had prostate cancer, BCR, a recordable management plan, and 68Ga-PSMA PET/CT during the period from June 2015 to February 2017 were retrospectively identified.
Radiopharmaceutical and Imaging Protocol
A conjugate of the 68Ga-PSMA–specific pharmacophore Glu-NH-CONH-Lys (68Ga-PSMA-HBED-CC) was synthesized using a method similar to that described by Eder et al. (3).
68Ga-PSMA was administered intravenously by bolus injection. The injected dose (mean ± SD) was 159 ± 42 MBq (range, 77–295 MBq). Variation in the injected dose was due to the short half-life of the tracer.
In line with published guidelines, studies were performed with 60 min of tracer uptake time before PET imaging and the acquisition of noncontrast CT from the vertex to the midthighs (4).
Image Analysis
PET/CT images were reviewed on Advantage Workstations 4.4 (GE Healthcare). A nuclear medicine physician who had more than 15 y of experience in PET imaging recorded disease status (positive was defined as uptake that was greater than the background and did not correspond to physiologic uptake).
Disease was recorded as being located within the prostate or prostatectomy bed or within pelvic lymph nodes or as metastatic disease.
Validation Criteria
Positive findings on PET could be validated only in the setting of salvage prostatectomy or when targeted or template biopsy was subsequently performed. Pathologic validation was available in 11 cases (3 prostatectomy and 8 biopsy). The findings in 10 of these cases were concordant with the 68Ga-PSMA findings. In 1 patient, template prostate biopsy did not reveal tumor, but the patient continued to have a rise in prostate-specific antigen (PSA) levels, suggesting that the biopsy may not have identified disease. Avid lesions were considered positive for disease even if they had not been positive on any recent bone scan or 18F-choline PET/CT study.
Management Changes
From electronic medical records, both the intended management plan before 68Ga-PSMA PET/CT and the actual management plan after 68Ga-PSMA PET/CT were recorded (Tables 1 and 2). Management plans were reviewed with a clinical oncologist who had more than 20 y of experience in the management of prostate cancer.
Management Plans That Were Altered After 68Ga-PSMA PET/CT
Management Plans That Were Not Altered After 68Ga-PSMA PET/CT
PSA Data and Kinetics
Serum PSA data from the electronic medical notes for each patient were recorded and included the value and date of the sample taken closest to the scan as well as all values within a 12-mo period before the scan. Any patient on hormone therapy at the time of the scan or in the 12-mo period before the scan was excluded from the PSA analysis. The PSA values were applied to the Memorial Sloan Kettering Cancer Center PSA doubling time tool (5).
Statistical Analysis
For continuous variables, mean ± SD was calculated. For categoric data, counts and percentages were calculated. Relationships between clinical parameters and management changes were investigated with the Fisher exact test.
RESULTS
All Patients
The study population comprised 100 patients, of whom 85 were not currently on hormone therapy or had not received hormone therapy in the 12 mo before the scan. The median age of the patients was 67.95 ± 7.38 y (range, 47–89 y). The original treatments were radical prostatectomy in 68 patients (68%) and radiotherapy in 32 patients (32%).
The 68Ga-PSMA PET/CT findings were positive in 47 of the 100 patients (47%). In patients with positive scan results, local disease (involving the prostate or prostatectomy bed) was the most common (n = 17). Pelvic nodal recurrence occurred in 9 patients, and 21 patients had extrapelvic metastatic disease.
Management Changes
Management was changed after 68Ga-PSMA PET/CT in 39 patients. Twenty-three (33.8%) of the 68 patients in the radical prostatectomy group had a management change. Sixteen (50%) of the 32 patients in the radiotherapy group had a management change. Specific changes in management are shown in Table 1, and the plans that remained unchanged are shown in Table 2.
Higher PSA levels were associated with management changes (P = 0.024). The highest proportion of cases in which management changes occurred involved PSA levels that were higher than 1 ng/mL, as shown in Figure 1. Although PSA kinetics did not show any significant association with management changes, there was a trend toward a greater proportion of management changes with higher PSA velocities (P = 0.086) (Fig. 2). Neither Gleason grade nor tumor stage was associated with management changes.

Management changes occurring at different PSA levels. More changes occurred at higher PSA levels, and this finding was significant (P = 0.024).

Higher PSA velocities were associated with more management changes, but this finding did not reach statistical significance (P = 0.086).
When a subgroup analysis was performed for radical prostatectomy and radiotherapy, the significant relationship with higher PSA levels was not maintained. PSA kinetics, Gleason score, T stage, and metastatic versus localized disease were all not significantly associated with management changes in the subgroups.
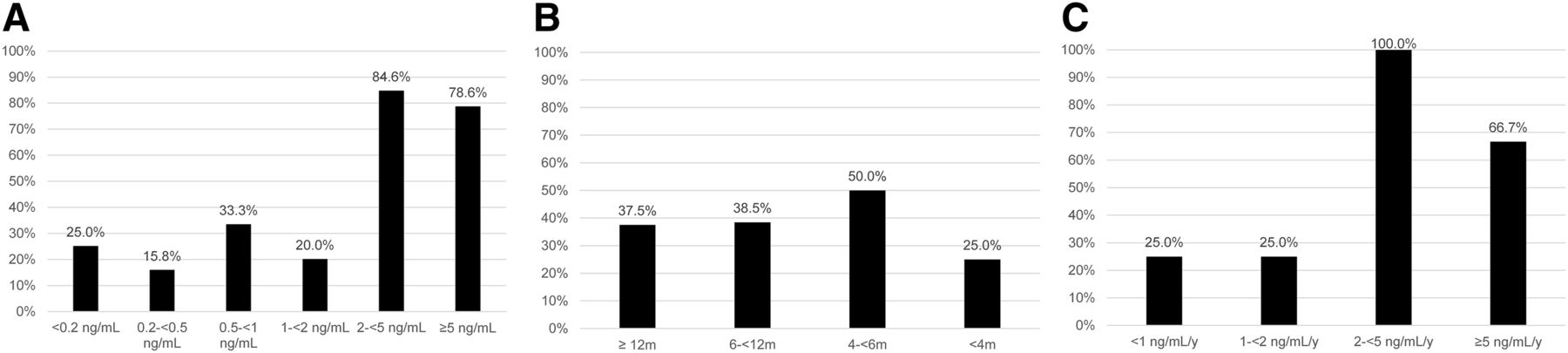
Positive 68Ga-PSMA PET/CT findings were associated with higher serum PSA levels (P < 0.001), but no association was found with doubling times. However, higher velocities were observed in scans with positive results (P = 0.03). The proportions of patients with positive scan results at different PSA levels, PSA doubling times, and PSA velocities are shown in Figure 3.

(A) Proportions of positive 68Ga-PSMA PET/CT results at different PSA levels. Significantly higher rate of positive scan results was seen at high PSA levels (P < 0.001). (B) Proportions of positive 68Ga-PSMA PET/CT results at different PSA doubling times. No significant association was shown (P = 0.946). (C) Proportions of positive 68Ga-PSMA PET/CT results at different PSA velocities. Significantly higher rate of positive scan results was seen at high PSA velocities (P = 0.033).
Positive scan results were associated with higher T stages (P = 0.03), and although higher Gleason scores were found in patients with positive scan results, this finding did not reach significance (P = 0.13).
DISCUSSION
68Ga-PSMA PET/CT led to a change in management plans in 39% of patients with BCR. Changes occurred more often in patients with higher PSA levels and in patients originally treated with radiotherapy rather than radical prostatectomy.
The proportion of changes in management in the present study was lower than that in some other published studies in which management impact was assessed, but the proportion of studies with positive results in our cohort was also relatively lower.
In a retrospective study of 42 patients who had BCR and were scanned for radiotherapy planning, Sterzing et al. reported a change in target volume or dose in 60.5% of patients, with 73.5% of scans having positive results (6). Shakespeare found that an alteration in any aspect of management occurred in 53.7% of cases after 68Ga-PSMA PET/CT, with a change to radiotherapy in 46.3% and a change to androgen deprivation therapy in 33.3% (7).
Dewes et al. observed that 68Ga-PSMA PET/CT led to a change in staging classification in 53.3% of analyzed patients; revisions to the radiotherapy concept occurred in 33.3% of patients, with relevant changes in the planned target volume (8).
Albisinni et al. (9) evaluated 131 patients and found positive scan results in 75% and an impact on management in 76%. Although PSA levels were studied in relation to the positivity of scan results, the authors did not differentiate cases into the key groups of prostatectomy and radiotherapy, as was done in the present study. The fact that a larger proportion of patients was treated with radical prostatectomy in the present study may have accounted for the different results, as patients who had undergone prostatectomy had a lower rate of management changes. In addition, the smaller number of positive study results in our patient population would have influenced the proportion of management changes. However, in a prospective study with predominantly radical prostatectomy patients, Morigi et al. found an impact on management after 68Ga-PSMA PET/CT in 24 (63%) of 38 patients, and 68% of the scans had positive results (10).
The proportion of PET/CT scans with positive results in the present study (47%) was significantly lower than the proportions described by Afshar-Oromieh et al. (82.8%) (11) and Ceci et al. (74.2%) (12) for recurrent prostate cancer. The large number of patients with very low PSA levels in our patient population (in view of the large proportion of patients treated with prostatectomy, after which PSA relapse occurs at significantly lower PSA levels) and the large number of patients with low PSA levels referred to our center may have accounted for the different results.
Positive study results were associated with higher PSA levels, higher PSA velocities, and higher T stages. No significant association was demonstrated with PSA doubling times. There was a trend toward higher Gleason scores in patients with positive scan results, but this finding did not reach significance.
It is possible that the smaller proportion of patients for whom data were available to calculate kinetics may have led to the masking of an association with PSA doubling times. In a recent metaanalysis, PSMA positivity was 64% for PSA doubling times of greater than 6 mo and 92% for PSA doubling times of less than 6 mo. High heterogeneity between subgroups was noted and, in the subgroup with long PSA doubling times, there was evidence of a small-study effect (13).
The relationship between PSA and positive scan results has also been investigated by others (11,14,15). The proportion of scans with positive results at each PSA threshold was lower in the present study than in previous reports. For example, 15.8% of studies had positive results at PSA levels of 0.2–<0.5 ng/mL, compared with 57.89% in the study by Eiber et al. (15) and 50% in the study by Afshar-Oromieh et al. (11), and 20% of studies had positive results at PSA levels of 1–<2 ng/mL, compared with 93.06% (15) and 71.8% (11). A possible explanation is that the exclusion of patients on androgen deprivation therapy from our study would have reduced PSA levels at the time when scans with positive results were obtained in other studies, from which such patients were not excluded. In addition, patients may have been referred at earlier time points within the biochemical recurrence pathway in the present study, as 68Ga-PSMA for early investigation has become more routine practice since older studies were performed.
Limitations of the present study include a retrospective design, which prevented the collection of data on how 68Ga-PSMA PET/CT may have affected confidence in management decisions. Only a small number of patients had pathology as validation, in common with other studies on BCR. However, good sensitivity and specificity of 68Ga-PSMA PET/CT for disease detection have already been described in multiple reports (13), and this information is part of the rationale for its accelerated acceptance into clinical practice.
CONCLUSION
68Ga-PSMA PET/CT altered management in 39% patients with BCR. Changes occurred more often in patients with radical radiotherapy treatment, positive scan results, and higher PSA levels. Gleason score, T stage, PSA kinetics, and disease distribution were not associated with management changes after 68Ga-PSMA PET/CT.
DISCLOSURE
Financial support for Asim Afaq was received from the UCLH NIHR BRC, the UCL Experimental Cancer Medicine Centre, and the London North West Healthcare Charitable Fund. Heather Payne’s work was supported by the UCLH/UCL Comprehensive Biomedical Research Centre. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 26, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 1, 2017.
- Accepted for publication June 26, 2017.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Changes in Management After 18F-DCFPyL PSMA PET in Patients Undergoing Postprostatectomy Radiotherapy, with Early Biochemical Response Outcomes
- A Phase II, Open-Label Study to Assess Safety and Management Change Using 68Ga-THP PSMA PET/CT in Patients with High-Risk Primary Prostate Cancer or Biochemical Recurrence After Radical Treatment: The PRONOUNCED Study
- Impact of 68Ga-PSMA-11 PET/CT on Staging and Management of Prostate Cancer Patients in Various Clinical Settings: A Prospective Single-Center Study
- A Prospective Study on 18F-DCFPyL PSMA PET/CT Imaging in Biochemical Recurrence of Prostate Cancer
- Intention-to-Treat Analysis of 68Ga-PSMA and 11C-Choline PET/CT Versus CT for Prostate Cancer Recurrence After Surgery
- Metaanalysis of 68Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology
- 68Ga-PSMA-11 PET/CT in Primary and Recurrent Prostate Carcinoma: Implications for Radiotherapeutic Management in 121 Patients
- Impact of 68Ga-PSMA-11 PET/CT on the Management of Prostate Cancer Patients with Biochemical Recurrence