


Abstract
Although PET/CT with 68Ga-PSMA-11 in the diagnosis of prostate cancer (PCa) is routinely performed at 1 h after injection, later scans may be beneficial because most lesions present with higher uptake and contrast. This evaluation aimed to investigate the clinical impact of additional late 68Ga-PSMA-11 PET/CT. Methods: Between 2011 and 2016, 112 patients with PCa who underwent early (at 1 h after injection) and late (at 3 h after injection) 68Ga-PSMA-11 PET/CT scans were retrospectively evaluated. The late scans were conducted to clarify unclear findings in early scans or to increase the probability of tumor detection in the case of negative early scans. All patients were asked to drink 1 L of water between early and late scans. In addition, 20 patients received 20 mg of furosemide before late scans. Tumor detection and radioactivity concentration within the urinary bladder were analyzed in both scans. The SUVmax and contrast of 149 tumor lesions were measured in 69 patients with pathologic findings. Results: Overall, 134 lesions characteristic for PCa in 57 patients clearly presented at 1 h after injection and 147 lesions in 68 patients at 3 h after injection. Forty-three patients showed no pathologic findings. Eight patients (7.1%) showed 1 unclear finding in early scans, which could be clarified as characteristic for PCa at 3 h after injection. Four patients (3.6%) presented with 1 lesion characteristic for PCa at 3 h after injection only. Twelve patients (10.7%) presented with 12 possible PCa lesions at 1 h after injection, which, however, could not be confirmed as PCa in late scans. Two patients presented with 1 lesion characteristic for PCa at 1 h after injection, which became invisible at 3 h after injection because of low contrast. At 3 h after injection, 62.4% of the lesions demonstrated a higher SUVmax and 65.1% a higher contrast than at 1 h after injection. Patients with furosemide presented with lower SUV and radioactivity concentration within the urinary bladder. Conclusion: 68Ga-PSMA-11 PET/CT at 3 h after injection showed most lesions characteristic for PCa with a higher uptake and contrast. In addition, the radioactivity signal within the urinary bladder was lower at 3 h after injection, especially when furosemide was applied. Consequently, scans at 3 h after injection detected more tumor lesions than at 1 h after injection.
- prostate cancer
- PET/CT
- positron emission tomography
- PSMA
- prostate-specific membrane antigen
- tumor detection
Prostate cancer (PCa) is the most frequent malignant tumor in men (1,2). After initial curative therapy, mainly by surgery or radiation, biochemical recurrence is frequent in men with high-risk disease. At this stage, searching for tumor lesions is challenging for conventional imaging modalities such as CT and MRI because of frequently unsatisfying sensitivity and specificity. Since the invention and clinical introduction of 68Ga-PSMA-11 (HBED-CC), imaging with PET using 68Ga-PSMA-11 has rapidly spread. 68Ga-PSMA-11 is a small-molecule inhibitor of the prostate-specific membrane antigen (PSMA), a transmembranous enzyme that is significantly overexpressed in most adenocarcinomas of the prostate gland. The first publications indicated that this novel method is significantly superior to other methods used for the detection of recurrent PCa (3–6). Later publications and a meta-analysis confirmed these findings (7–9).
PET/CT with 68Ga-PSMA-11 is routinely conducted 1 h after the injection of the tracer according to its first described clinical setup (3). However, the same article already demonstrated that late images conducted at 3 h after injection show most PCa lesions with higher contrast due to an ongoing decrease of the background signal and increase of tracer uptake in most PCa lesions, which was confirmed by other publications (10,11). All 3 listed publications are based on bi- or multiphasic scans that were planned in advance. However, the impact of additional late scans that were not planned in advance but initiated after the regular scans (1 h after injection) to clarify unclear findings has not yet been investigated.
At our institute, additional late scans have been subsequently used to increase the detection rate of PCa lesions with 68Ga-PSMA-11 PET in men with unclear findings 1 h after injection. This article addresses the issue of what can be expected from late 68Ga-PSMA-11 PET/CT imaging in the case of unclear findings or negative scans conducted at 1 h after injection.
MATERIALS AND METHODS
Of 887 patients with PCa referred for 68Ga-PSMA-11 PET/CT between 2011 and February 2016, 149 patients (16.8%) underwent scans at both 1 and 3 h after injection. In most of the patients (n = 107), recurrent disease was suspected. In 5 cases, PET/CT was conducted before initiation of local therapy to exclude metastases after PCa was confirmed by biopsy.
The first 37 of these 149 patients were part of a previous publication (3) and were excluded from the current analysis because these patients were planned in advance to be scanned at 1 and 3 h after injection. The difference between that publication and the current evaluation is that the late scans of the current evaluation were not planned before the first scan at 1 h after injection but were arranged thereafter to clarify unclear findings or to increase the probability of tumor detection in the case of negative early scans.
As with other imaging modalities, many cases remain that show no pathologic findings in 68Ga-PSMA-11 PET/CT at 1 h after injection. However, the workload in clinical routine does not allow for additional late scans to be obtained in every one of these cases. As a retrospective analysis, it remains impossible to reconstruct the particular situations in which the decision was made to conduct an additional late scan in 68Ga-PSMA-11 PET/CT.
The patients’ characteristics are presented in Table 1. Thirty-nine patients of the present evaluation have also been part of a previous publication, which, however, exclusively analyzed the regular scans conducted at 1 h after injection (5). We therefore believe that these patients had to be included in the present evaluation instead of being excluded. Their inclusion improved the data quality and significantly strengthened the conclusions.
Characteristics of All Patients Investigated in This Study (n = 112)
All patients signed a written informed consent form for the purpose of anonymized evaluation and publication of their data. All reported investigations were conducted in accordance with the Helsinki Declaration and with our national regulations. This evaluation was approved by the ethics committee of the Heidelberg University (permit S-321/2012).
All patients underwent regular whole-body PET scans (from the head to the upper parts of the legs) at 1 h after injection. Thirty of the scans at 3 h after injection covered the whole body, 17 of them the abdomen and pelvis, and 65 of them the pelvis only.
Both regular scans at 1 h after injection and late scans at 3 h after injection were analyzed with regard to tumor detection. Among all lesions visually considered characteristic for PCa, we selected 149 representative lesions for radiotracer uptake analysis measured as SUVmax. Tumor contrast was measured by subtracting the SUVmean of the background from the SUVmax of tumor lesions. As background, we selected gluteal musculature. Any visible PCa lesion of a patient was counted and analyzed unless they had more than 10 lesions (5 patients). In such a case, a maximum of 10 lesions were analyzed after a random selection. This kind of selection avoids an overestimation of SUVs in the patients’ cohort because otherwise dominant lesions would be preferentially selected.
Radiotracer
68Ga-PSMA-11 was produced as previously described (5,12). Briefly, 68Ga3+ was obtained from a 68Ge/68Ga radionuclide generator and used for radiolabeling of PSMA-11. The 68Ga-PSMA-11 solution was applied to the patients via an intravenous bolus injection (mean ± SD, 207 ± 78 MBq; range, 40–345 MBq). The targeted dose was 2 MBq/kg. Variation of injected radiotracer activity was caused by the short physical half-life of 68Ga (68 min), variable elution efficiencies resulting during the lifetime of the 68Ge/68Ga generator, and unexpected delays in clinical routine. A previous study demonstrated that PCa lesions can present with high contrast at 3 h after injection despite such low amounts of tracer (3). Low amounts of injected tracer cause a high background noise in late images. However, the favorable pharmacokinetics of 68Ga-PSMA-11 (increase of uptake over time in most lesions) compensates for this disadvantage.
Imaging
The patients of this evaluation were investigated with 2 different scanners. A Biograph-6 PET/CT scanner was used until August 2015 and was replaced by a Biograph mCT Flow scanner (both scanners made by Siemens). The 2 different PET/CT scanners were cross-calibrated.
With regard to the Biograph-6 PET/CT, the scan protocol (1 h after injection, whole body; 3 h after injection, whole body or part body) was as described previously (5). For each bed position, a 4-min acquisition time was used for both scans (1 and 3 h after injection). With regard to the Biograph mCT Flow scanner, an unenhanced CT scan was obtained (1 h after injection, whole body; 3 h after injection, whole body or part body) using the following parameters: slice thickness of 5 mm, increment of 3–4 mm, soft-tissue reconstruction kernel, Care Dose (Siemens). Immediately after CT scanning, a PET scan was acquired in 3 dimensions (matrix, 200 × 200) in Flow Motion with 0.7 cm/min (for both scans at 1 and 3 h after injection). The emission data were corrected for randoms, scatter, and decay. Reconstruction was conducted with an ordered-subset expectation maximization algorithm with 2 iterations/21 subsets and was Gauss-filtered to a transaxial resolution of 5 mm in full width at half maximum. Attenuation correction was performed using the low-dose unenhanced CT data. PET and CT were performed using the same protocol for every patient on a Biograph mCT Flow scanner (Siemens).
Between early and late scans, all patients were asked to drink 1 L of water. Twenty patients received additionally 20 mg of furosemide before late scans. None of the patients received furosemide before early scans. Diuretics were given per physician’s choice. As a retrospective analysis, we cannot reconstruct the particular situations in which the decision was made to apply furosemide.
Image Evaluation
Two of the authors, with 11 and 6 y of clinical nuclear medicine experience, read all datasets independently and resolved any disagreements by consensus.
Lesions that were visually considered as suggestive for PCa were counted and analyzed with respect to their localization (local relapses, lymph node [LN], bone and soft-tissue metastases) and to their SUVmax. For calculation of the SUV, circular regions of interest were drawn around areas with focally increased uptake in transaxial slices and automatically adapted to a 3-dimensional volume of interest at a 70% isocontour as previously described (5).
SUVmax in scans at 3 h after injection were compared with those at 1 h after injection and defined as increasing, decreasing, or stable with intensity changes of >10%, < −10%, or between −10% and +10%, respectively.
Furthermore, the SUVmean and SUVmax of the urinary bladders 1 and 3 h after injection were measured as well as the average radioactivity concentration in Bq/mL within the urinary bladder. In addition, the area around the urinary bladder was visually analyzed for the presence (=1) or absence (=0) of the Halo artifact, an artifact caused by extinction of the PET signal as described previously for a hybrid PET/MRI scanner (13).
Statistical Analysis
SUVs of the tumor lesions at 1 and 3 h after injection were compared using a 2-sided Wilcoxon signed-rank test. The same test was also used to evaluate differences concerning the radioactivity signal within the urinary bladder between the groups with and without furosemide. In addition, mathematic differences between 1 h after injection and 3 h after injection were calculated within each group. Thereafter, the results from these calculations were compared between the 2 groups. In this case, a 2-sided Mann–Whitney test was used. A P value of less than 0.05 was considered statistically significant.
RESULTS
Overall, 134 lesions characteristic for PCa in 57 patients clearly presented at 1 h after injection and 147 lesions in 68 patients at 3 h after injection. Forty-three patients showed no pathologic findings in either scan. As presented by Figures 1 and 2, 8 of the 112 patients (7.1%) showed 1 unclear finding in early scans, which could be clarified as characteristic for PCa at 3 h after injection. Four patients (3.6%) with a nonpathologic scan at 1 h after injection presented with 1 lesion characteristic for PCa at 3 h after injection. Twelve patients (10.7%) presented with 12 possible PCa lesions at 1 h after injection, which, however, could not be confirmed as PCa in late scans (Fig. 3); among them were 7 patients who presented exclusively with 1 of the mentioned lesions. Two patients presented with 1 lesion characteristic for PCa at 1 h after injection, which became invisible at 3 h after injection due to a decrease in uptake and contrast (Fig. 4). No unclear lesions were found when all scans conducted at 3 h after injection were analyzed.
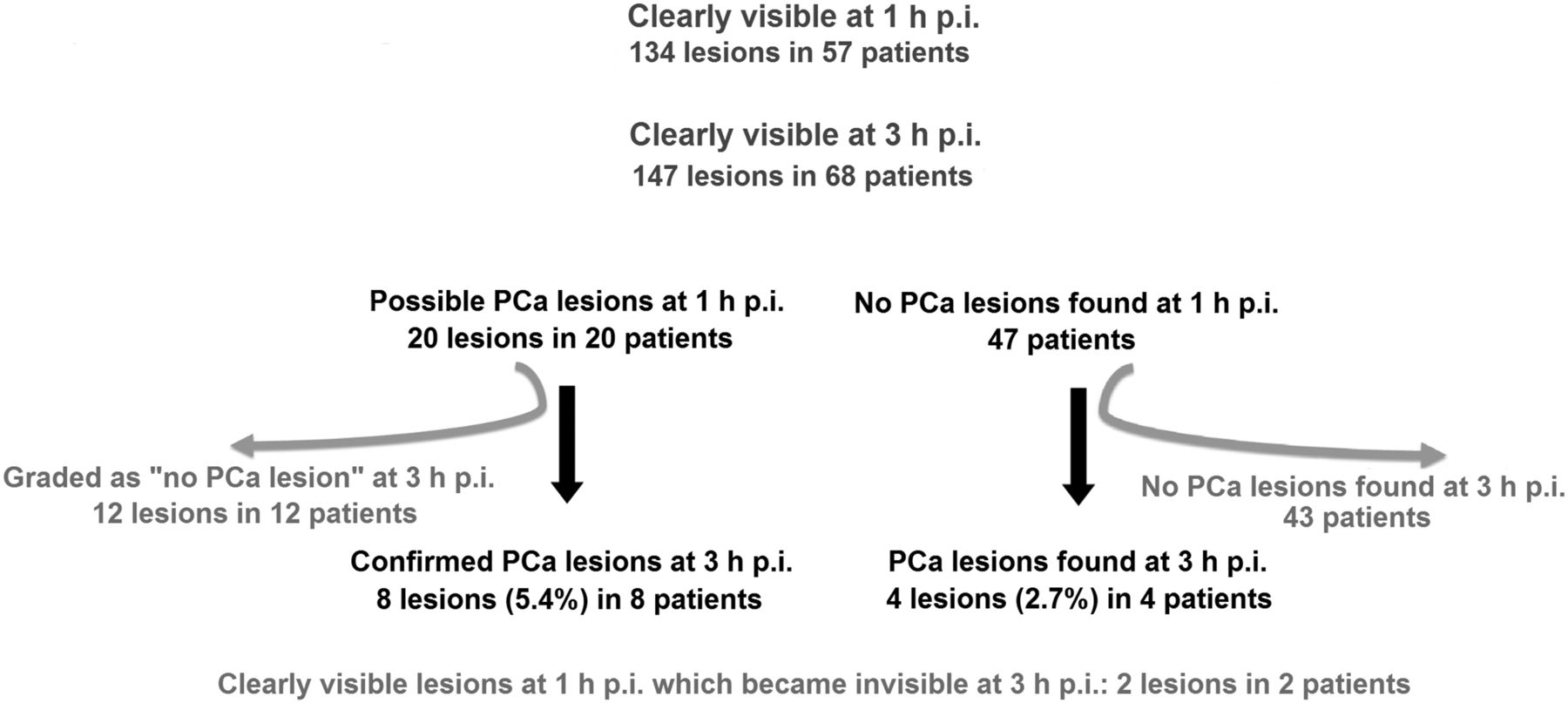
68Ga-PSMA-11 PET/CT at 3 h after injection helped to clarify unclear lesions found at regular scans 1 h after injection and detected new PCa lesions. Included in this figure are 2 lesions characteristic for PCa at 1 h after injection that, however, became invisible at 3 h after injection because of decrease of uptake and contrast. Lesion percentages are related to all lesions characteristic for PCa detected in both scans (n = 149). p.i. = after injection.
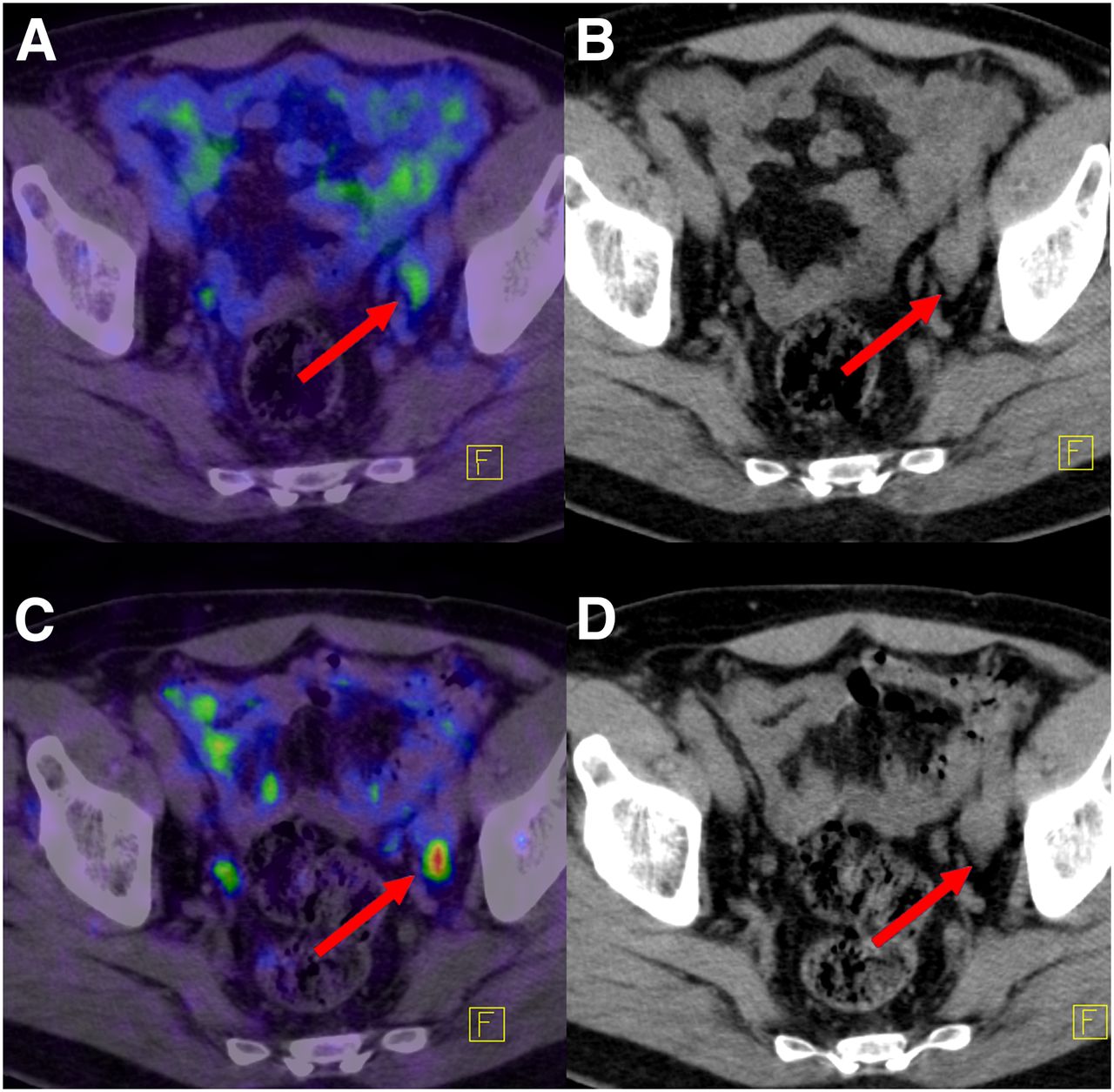
Most PCa lesions present with higher uptake and contrast at 3 h after injection compared with 1 h after injection. Red arrows point to an LN metastasis adjacent to intestines that was clearly visible at 3 h after injection (C [fusion of PET and CT at 3 h after injection] and D [low-dose CT at 3 h after injection]) (SUVmax, 5.7). At 1 h after injection (A [fusion of PET and CT at 1 h after injection] and B [low-dose CT at 1 h after injection]), slight uptake (SUVmax, 2.2) was thought to be related to background signal of intestines as also visible in upper parts of subimage A.

68Ga-PSMA-11 PET/CT of patient at 1 h after injection (A [fusion of PET and CT at 1 h after injection] and B [low-dose CT at 1 h after injection]) and at 3 h after injection (C [fusion of PET and CT at 3 h after injection] and D [low-dose CT at 3 h after injection]). Red arrows point to an unclear finding in scans at 1 h after injection demonstrating slight focal uptake without clear morphologic correlation in CT scan. Late scans demonstrated no pathologic uptake and still no morphologic correlation in CT scan. The slight uptake was therefore thought to be related to background signal of intestines.
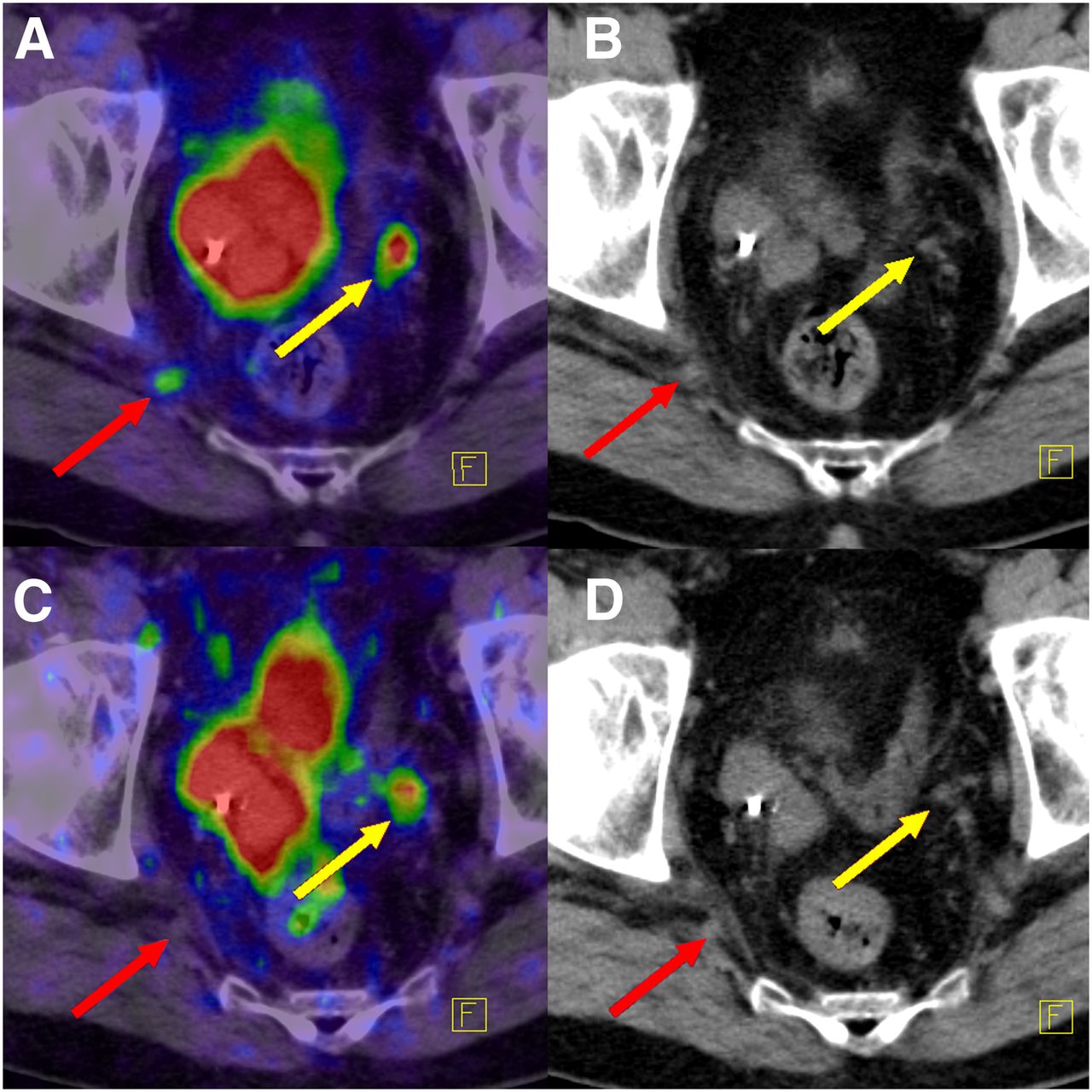
68Ga-PSMA-11 PET/CT of patient at 1 h after injection (A [fusion of PET and CT at 1 h after injection] and B [low-dose CT at 1 h after injection]) and at 3 h after injection (C [fusion of PET and CT at 3 h after injection] and D [low-dose CT at 3 h after injection]). Red arrows point to the lesion (LN) characteristic for PCa in early images that, however, becomes invisible in late scans. Another LN metastasis (yellow arrows) presented also with decreasing uptake and contrast in late scans (SUVmax, 5.0 at 1 h after injection and 3.5 at 3 h after injection; contrast, 4.7 at 1 h after injection and 3.3 at 3 h after injection).
Among all 149 lesions visually considered typical for PCa, 63 were defined as LN metastases, 43 as bone metastases, 16 as primary PCa, 14 as local relapses, and 13 as soft-tissue/organ metastases. Overall, at 3 h after injection 62.4% of the PCa lesions (n = 93) demonstrated higher (> +10%) (Fig. 2), 13.4% (n = 20) lower (< −10%), and 24.2% (n = 36) stable (between −10% and +10%, respectively) SUVmax values compared with at 1 h after injection. The higher SUVmax at 3 h after was statistically significant (P < 0.001).
In addition, at 3 h after injection 65.1% of the PCa lesions (n = 97) demonstrated higher (> +10%), 14.1% (n = 21) lower (< −10%), and 20.8% (n = 31) stable (between −10% and +10%, respectively) contrast compared with at 1 h after injection. The higher contrast at 3 h after injection was also statistically significant (P < 0.001).
In 8 of all 69 patients with pathologic PET/CT (11.6%), lesions with decreasing uptake between 1 and 3 h after injection were simultaneously present with lesions demonstrating an increasing uptake. In 6 patients (8.7%), lesions with decreasing uptake were present exclusively.
Supplemental Figure 1 (supplemental materials are available at http://jnm.snmjournals.org) is representative for the advantages of a lower radioactivity signal within the urinary bladder. The average radioactivity within the urinary bladder at 1 and 3 h is presented in Table 2. In addition, mathematic differences between 1 h after injection and 3 h after injection were calculated within each group (with and without furosemide). Thereafter, the results from these calculations were compared between the group with hydration only and that with hydration + furosemide. The results were as follows: P = 0.014 for SUVmean, P = 0.031 for SUVmax, and P = 0.092 for Bq/mL.
SUV and Radioactivity Concentration Within Urinary Bladder at 1 and 3 Hours After Injection and Associated P Values
In none of the 112 patients was a Halo artifact observed around the urinary bladder, neither at 1 nor at 3 h after injection.
DISCUSSION
In the first 68Ga-PSMA-11 PET/CT study, the uptake of PCa lesions was analyzed at 1 and 3 h after injection in 37 patients, revealing that in most PCa metastases the uptake and contrast were more intense at 3 h after injection (3). However, because all tumor lesions presented with good contrast already at 1 h after injection, 68Ga-PSMA-11 PET/CT is routinely performed at 1 h after injection. In small patient cohorts, PSMA-11 and different other PSMA ligands demonstrated to be taken up in PCa lesions increasingly over time (14–16). The current analysis in a larger patient cohort confirmed this observation.
In contrast to other published studies, the current article specifically focuses on additional late scans, which were not planned before the first (regular) scans. This article therefore addresses the issue of what can be expected from late imaging in the case of unclear findings or negative scans conducted at 1 h after injection. As far as the authors know, such data have never been published before.
The results presented here demonstrate that 68Ga-PSMA-11 at 3 h after injection is a powerful method to confirm findings of regular scans at 1 h after injection, to find new PCa lesions or to clarify unclear findings. With regard to detection rates and lesion visibility, 68Ga-PSMA-11 PET/CT at 3 h after injection was shown to be superior to 68Ga-PSMA-11 PET/CT at 1 h after injection. These results confirm the findings of a previous study in which 3 h after injection appeared to be the best imaging timing for 68Ga-PSMA-11 PET/CT (10). In addition, no unclear findings were detected at 3 h after injection. This result, however, needs to be interpreted with caution because the scanned area at 3 h after injection was smaller in most patients than the scan area at 1 h after injection.
Diuretics were given per physician’s choice before the late scans. Because of these possibly biased decisions regarding the administration of diuretics, a statistical lesion-based analysis under consideration of diuretics is not appropriate. However, our results demonstrate that the reduction of SUVs and radioactivity within the urinary bladder between 1 and 3 h after injection was more intense in patients who received diuretics. This fact is known from other imaging modalities such as PET imaging with 18F-FDG or DOTA conjugates. One can assume that the lower the PET signal of the urinary tract, the higher the visibility of adjacent PCa lesions. In this context, hydration and diuretics can help to optimize the visibility of PCa lesions in those regions. The routine administration of diuretics is controversial because of their side effects, though. Recently, an article was published showing the positive effects of diuretics on the assessment of the prostate region when using the PSMA ligand 68Ga-PSMA I&T for PET/CT (17).
Our results demonstrate that in more than 12% of the patients referred to 68Ga-PSMA-11 PET/CT, an additional late scan was conducted by the responsible physicians to clarify unclear findings of regular scans at 1 h after injection. These additional scans were not planned before the arrival of the patients at our PET center. As a consequence, such scans disturb the clinical routine and consume time and further resources. This is an important aspect for a modern health-care system, which continuously pushes the boundaries of efficacy. In addition, reimbursement issues for additional scans raise questions. At least, the patients need to be informed about the additional costs in an appropriate time before the additional scans. Therefore, the question remains whether a procedure exists that provides the best possible information available by 68Ga-PSMA-11 PET/CT at a single time. According to our experiences and the presented results, a 68Ga-PSMA-11 PET/CT scan at 3 h after injection after a sufficient hydration with at least 1 L of water and the administration of diuretics appears to be the best option to increase the probability of a pathologic PET scan. In this context, hydration and diuretics should not be administered too early because both would excrete portions of the tracer before it had enough time to interact with the PSMA receptor. Hydration may be started at 2 h after injection followed by diuretics 20–30 min later. Still, later images, for example, at 4 h after injection, can show an increase of tumor uptake and therefore help to clarify unclear lesions (10). However, with increasing time intervals between tracer administration and imaging, the injected activity and, therefore, the counting rate and image quality become more and more important. Quantification analysis can become unstable for images acquired at 5 h after injection because of low counting rates remaining after 5 half-lives, especially when tracer amounts of 150–200 MBq are administered (10).
Without doubt, the longer waiting time is a disadvantage of the suggested procedure compared with scans conducted at 1 h after injection. The amount of activity after radiolabeling may also be limiting. However, the higher diagnostic outcome may justify the longer waiting time and further actions to reduce the signal of the urinary bladder and ureters, especially for patients with low prostate-specific antigen (PSA) levels and, therefore, expected reduced tumor detection rates. In the case of a negative single scan at 3 h after injection despite a biochemical relapse of PCa, we recommend waiting until a further PSA elevation and plan a biphasic 68Ga-PSMA-11 PET/CT at 1 and 3 h after injection including hydration and furosemide administration as described before.
In accordance with previous publications (3,11), a minority of PCa lesions showed a decreased uptake in late images. Such lesions often occur simultaneously with lesions demonstrating an increasing uptake with time. In a few number of patients, decreasing lesions occur exclusively. With the exception of 2 lesions, all PCa lesions that presented with a lower uptake at 3 h after injection compared with 1 h after injection were still clearly visible at 3 h after injection.
Although the reasons for a decrease of uptake remain unclear, we speculate that some lesions show a reduced internalization rate of the PSMA ligand. Further studies are mandatory to analyze this observation.
In none of the patients was an artifact caused by extinction of the PET signal around the urinary bladder (called Halo artifact by the authors) observed. This artifact was reported when using 68Ga-PSMA-11 in a PET/MRI hybrid system (13). The Halo artifact can cause reduced tumor visibility, thereby leading to false-negative results (13). The scatter correction of the PET/MRI hybrid system is suggested to cause or influence the mentioned artifact. After the first description of this artifact, some colleagues argued that an extinction artifact around the urinary bladder is also present in PET/CT. However, as described above, we could not observe such an artifact when using the above-mentioned scanners. Further improvements of the manufacturers are mandatory to reduce the Halo artifact in PET/CT or PET/MRI scanners.
Our retrospective analysis shows typical limitations compared with prospective studies: probably biased decisions regarding the conduction and area of additional late scans as well as the administration of diuretics. However, our data reflect the daily clinical routine and every center conducting PSMA ligand PET/CT faces similar conditions. Regarding the area of the late scans, most were conducted from the pelvis or abdomen and pelvis. Therefore, additional PCa lesions outside these areas cannot be excluded. On the other hand, it is unlikely that PCa lesions exist outside these areas without the existence of lesions in the pelvis or abdomen, especially in patient cohorts with low PSA values such as the current cohort. We therefore believe that—in the case of a negative whole-body PET scan result—additional late scans can be focused on the pelvis and abdomen, especially in patients with low PSA values.
One additional limitation of the analysis presented here is the lack of a standard reference in terms of systematic histopathologic investigations of PET-positive lesions. However, since 68Ga-PSMA-11 PET/CT was introduced, the results prove the excellent specificity of this compound, indicating that any uptake of 68Ga-PSMA-11 above local background in CT- or MR-morphologic visible lesions of PCa patients should be regarded as highly suspicious for PCa (5,6,18,19).
CONCLUSION
PET/CT with 68Ga-PSMA-11 at 3 h after injection is a valuable method to clarify unclear findings of regular scans conducted at 1 h after injection or to find new PCa lesions because most PCa lesions present with a higher uptake and contrast in late scans. With regard to detection rates and lesion visibility, 68Ga-PSMA-11 PET/CT at 3 h after injection was superior to 68Ga-PSMA-11 PET/CT at 1 h after injection. Hydration and diuretics shortly before the scans at 3 h after injection are recommended because they can help to better distinguish between urinary bladder and adjacent PCa lesions.
Footnotes
Published online Jan. 6, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 1, 2016.
- Accepted for publication December 8, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 61Cu-PSMA-Targeted PET for Prostate Cancer: From Radiotracer Development to First-in-Human Imaging
- 61Cu-Labeled Radiotracers: Alternative or Choice?
- Early Injection of Furosemide Increases Detection Rate of Local Recurrence in Prostate Cancer Patients with Biochemical Recurrence Referred for 68Ga-PSMA-11 PET/CT
- Combination of Forced Diuresis with Additional Late Imaging in 68Ga-PSMA-11 PET/CT: Effects on Lesion Visibility and Radiotracer Uptake
- Matched-Pair Comparison of 68Ga-PSMA-11 and 18F-rhPSMA-7 PET/CT in Patients with Primary and Biochemical Recurrence of Prostate Cancer: Frequency of Non-Tumor-Related Uptake and Tumor Positivity
- Quantitative and Qualitative Analyses of Biodistribution and PET Image Quality of a Novel Radiohybrid PSMA, 18F-rhPSMA-7, in Patients with Prostate Cancer
- Comparison of 3 Interpretation Criteria for 68Ga-PSMA11 PET Based on Inter- and Intrareader Agreement
- An 18F-Labeled PSMA Ligand for PET/CT of Prostate Cancer: First-in-Humans Observational Study and Clinical Experience with 18F-JK-PSMA-7 During the First Year of Application
- Preclinical Evaluation and Pilot Clinical Study of Al18F-PSMA-BCH for Prostate Cancer PET Imaging
- Impact of 68Ga-PSMA PET/CT on the Radiotherapeutic Approach to Prostate Cancer in Comparison to CT: A Retrospective Analysis
- Metaanalysis of 68Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology
- Seduction by Sensitivity: Reality, Illusion, or Delusion? The Challenge of Assessing Outcomes after PSMA Imaging Selection of Patients for Treatment
- Treatment Outcomes from 68Ga-PSMA PET/CT-Informed Salvage Radiation Treatment in Men with Rising PSA After Radical Prostatectomy: Prognostic Value of a Negative PSMA PET
- 18F-DCFPyL PET/CT in the Detection of Prostate Cancer at 60 and 120 Minutes: Detection Rate, Image Quality, Activity Kinetics, and Biodistribution
- PSMA Ligands for PET Imaging of Prostate Cancer