


Abstract
Whole-body PET imaging with 18F-FDG has been used successfully to stage colorectal cancer. However, the impact of FDG PET on patient management from the referring physician’s point of view has not been determined. Methods: A questionnaire was sent to referring physicians to determine whether and how PET altered the management of colorectal cancer patients. Management changes, when present, were classified as intermodality (e.g., medical to surgical, surgical to radiation, medical to no treatment) or intramodality (e.g., altered medical, surgical, or radiotherapy approach). Results: Of 60 responses from referring physicians, changes in clinical stage were reported for 25 patients (42%). Among these, the disease was upstaged in 20 patients (80%) and downstaged in 5 patients (20%). The PET findings contributed to intermodality management changes in 22 of the 60 patients (37%), intramodality changes in 11 patients (18%), a combination of management changes in 4 patients (7%), and no change in 19 patients (32%). Two of the 60 patients (3%) had other changes, and no response to this question was received for the remaining 2 patients (3%). As a result of PET findings, physicians avoided major surgery in 41% of patients for whom surgery was the intended treatment. Conclusion: This survey-based study of referring physicians shows that FDG PET had a major impact on the management of colorectal cancer patients and contributed to changes in clinical stage and major management decisions in >40% of patients.
Colorectal cancer is diagnosed in about 155,000 patients per year and accounts for 15% of the malignancies in adults in the United States. Accurate staging of colorectal cancer is important to determine the best therapeutic approach for individual patients (1,2). Before the emergence of clinical whole-body PET, the diagnostic armamentarium for staging and restaging of patients with colon cancer consisted of anatomic imaging modalities such as CT, sonography, and colonoscopy and rectoscopy. These techniques are limited in their ability to discriminate reliably between postsurgical anatomic alterations and scarring after radiation and residual or recurrent disease (3).
Biologic tumor imaging with PET can overcome these limitations. PET using the glucose analog 18F-FDG is applied clinically to detect and stage a variety of cancers (4–6). The use of glucose metabolism to differentiate malignant tumors is based on the biology of neoplastic degeneration, which has been shown to exhibit high rates of glucose consumption in malignant tissue (4,7). This occurs because of a progressive loss of the tricarboxylic cycle to produce adenosine triphosphate (ATP). The production of ATP by glycolysis is amplified dramatically in tumor tissue. Neoplasms further increase their dependence on glucose by activation of the hexose monophosphate shunt to provide a carbon backbone to meet the high DNA and RNA synthesis requirements of cell proliferation (8).
Like glucose, FDG is a substrate for facilitated transport and is phosphorylated by hexokinase in tumor cells. However, FDG-6-PO4 is not catabolized and remains trapped in tumor cells. Therefore, the relative distribution of FDG-6-PO4 can serve as a marker of glucose metabolism in the organ systems of the body, which can then be imaged, with PET.
A high diagnostic accuracy of PET has been shown for staging many kinds of cancers (4–6,9) and specifically for staging and restaging (10) of colorectal cancer and for identifying the sites of metastatic involvement. Furthermore, the cost-effectiveness of PET imaging for managing patients with lung cancer, solitary pulmonary nodules, and colorectal cancer has been established (9,11,12).
To our knowledge, it has not been established previously how and whether referring physicians change their therapeutic approaches on the basis of information provided by PET. Thus, the true impact of whole-body PET on managing patients with colorectal cancer, in the referring physician’s perspective, is unknown. Therefore, the aim of this study was to determine, from the referring physician’s point of view, the impact of whole-body PET imaging on the management of patients with colorectal cancer.
MATERIALS AND METHODS
Patient Population
Physicians referring 146 patients with colorectal cancer were surveyed between October 1998 and January 2000. The survey was conducted at the Ahmanson Biological Imaging Clinic of the University of California, Los Angeles (UCLA), and the Northern California PET Imaging Center (NCPIC). The patient population consisted of 77 women and 69 men (mean age at PET, 61 ± 12 y; age range, 30–88 y). Fifty-nine patients were referred to UCLA and 87 were referred to the NCPIC.
Image Acquisition and Reconstruction
An EXACT HR or HR+ system (CTI/Siemens, Knoxville, TN) was used to obtain whole-body PET images. The resolution of reconstructed images used in these studies was 8–12 mm for these devices. The characteristics of these scanners have been described (13,14).
No attenuation correction was performed at UCLA, where images were reconstructed using standard filtered backprojection. At the NCPIC, attenuation-corrected images were obtained and iterative image reconstruction algorithms were used (15,16).
After a 6-h fasting period, 555 MBq (15 mCi) FDG were injected. Whole-body imaging was started 45 min later. Images were acquired from six to nine bed positions (6 min per bed position) in each patient. The acquired image sets were displayed on transaxial images and coronal and sagittal views.
The three-dimensional volume was inspected on the monitor.
Image Interpretation
The PET studies were not read blinded but were always interpreted within the context of a clinical readout session (i.e., knowledge of patient history as well as reports of other imaging tests). Thus, PET reports were based on all available clinical information in addition to the PET images. No quantitative or semiquantitative analysis of FDG uptake in lesions, such as by standardized uptake value, was performed because this is not part of the clinical routine image interpretation at our institutions.
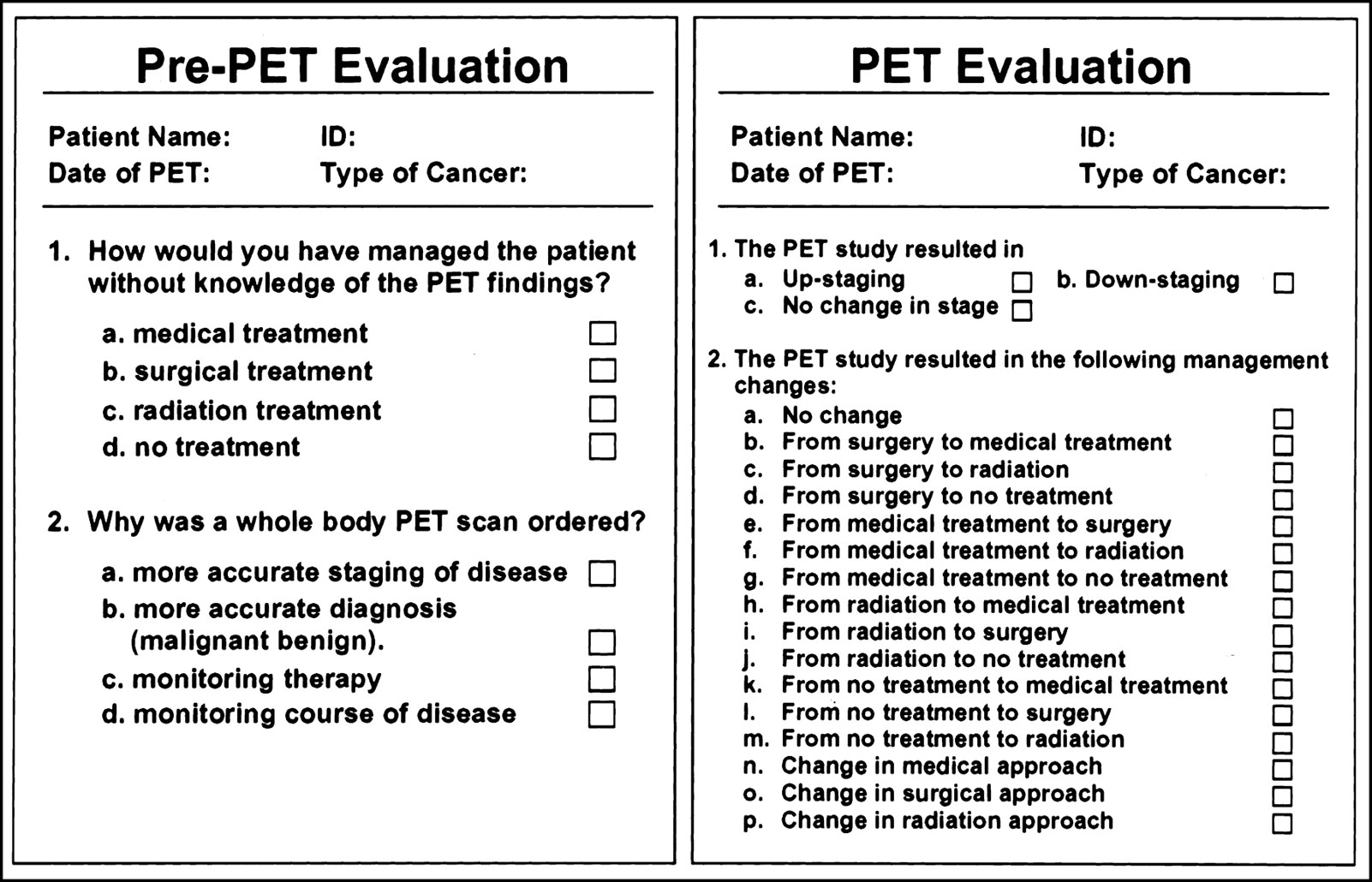
To evaluate the impact of PET imaging on patient management, pre-PET and post-PET questionnaires were sent to the referring physicians (Fig. 1). This was done as a single faxed protocol. This simple straightforward approach was chosen to increase the likelihood of receiving a response from referring physicians. A letter explaining the purpose of the study was attached to the survey. However, to avoid bias, the participating physicians did not receive any additional reminder or any other information related to the study. The pre-PET questionnaire asked to specify the patient stage and management plan before PET, whereas the post-PET questionnaire inquired about PET-induced changes. Two parameters were analyzed: changes in patient stage and changes in patient management. Management changes were classified into two categories: Intermodality changes were defined as changes between treatment modalities (from surgery to radiation therapy), and intramodality changes were defined as changes within one treatment modality (e.g., from one chemotherapeutic agent to another).
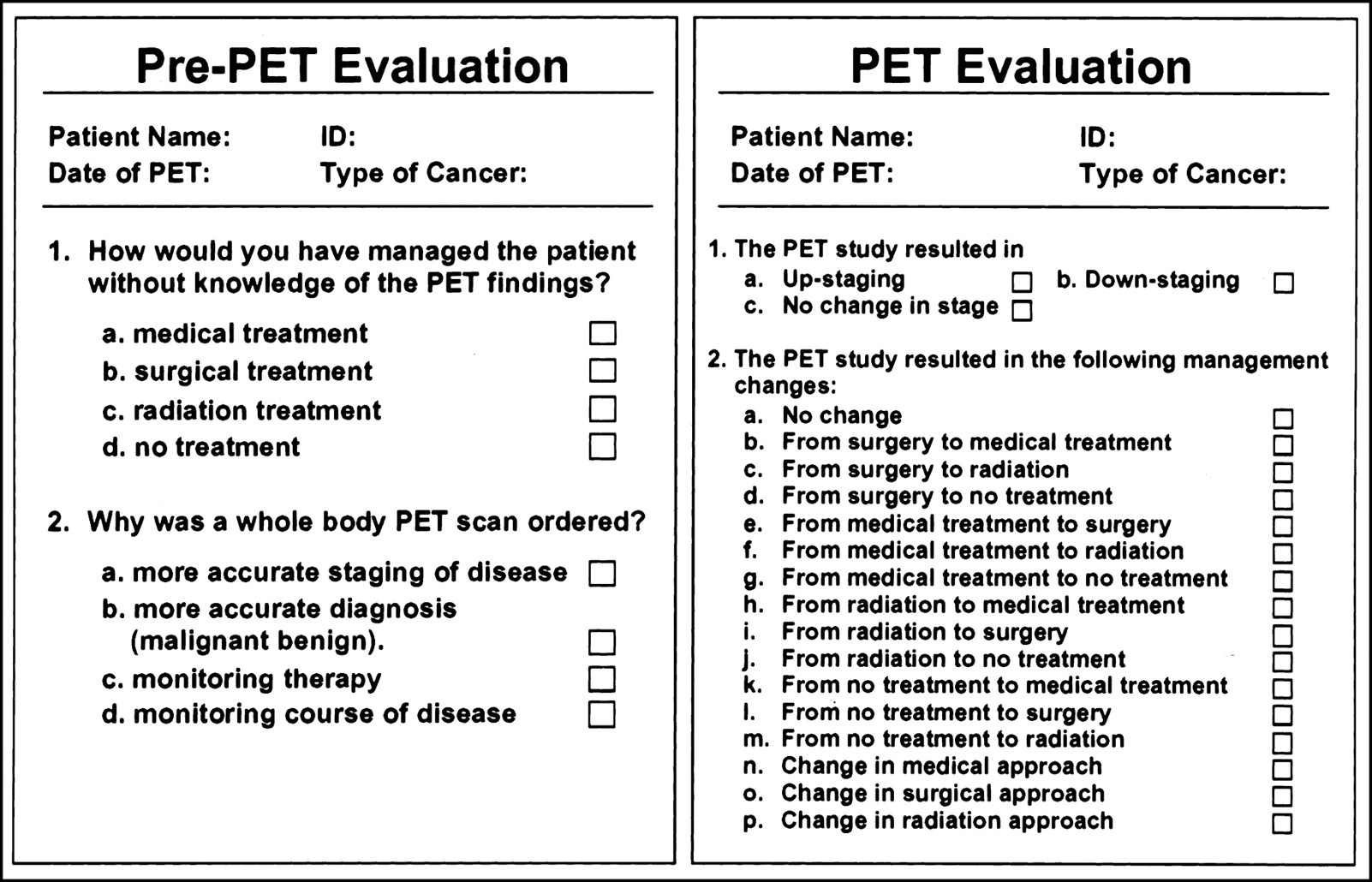
Sample questionnaire sent to referring physicians.
RESULTS
Characteristics of Referring Physicians
During the study period, 95 physicians referred 146 patients with colorectal cancer for whole-body FDG PET. Sixty of the 146 questionnaires were received by the time of publication, resulting in a response rate of 41% (37% for patients scanned at UCLA and 44% for those scanned at the NCPIC).
Specialties of all referring physicians (responders and nonresponders) included medical oncologists (54%), surgeons (23%), general practitioners (19%), radiation oncologists (3%), and pulmonologists (1%). The distribution of specialties of the 60 responding physicians included 53% medical oncologists, 27% surgeons, 15% general practitioners, 2% radiation oncologists, and 3% other specialties. Similarly, the distribution of specialties of the 86 nonresponding physicians included 53.5% medical oncologists, 21% surgeons, 21% general practitioners, 3.5% radiation oncologists, and 1% pulmonary specialists. The distribution of specialties did not differ significantly between UCLA and the NCPIC.
Clinical Indications for PET Study
FDG PET was ordered for more accurate staging in 55% of the cases, for monitoring the course of the disease in 23%, for more accurate diagnosis in 12%, for monitoring therapy in 2%, and for a combination of these reasons in 5% of the cases. The remaining 3% reported other reasons for ordering the scan. The clinical indications for the PET study did not differ between the study centers.
Pre-PET Clinical Management Plan
The intended treatment before PET was surgery in 36.5%, medical treatment in 27%, radiation in 3%, and a combination of treatments in 5%. No further treatment was planned in 27%, whereas the remaining 1.5% of the respondents stated other treatments.
Impact of PET on Clinical Stage
Changes in clinical stage were reported for 25 patients (42%): 20 (33%) were upstaged and 5 (8%) were downstaged. Thirty-two patients (53%) had no change in clinical stage. No response to this question was received for the remaining 5% (Table 1).
Impact of PET on Clinical Stage
PET Influence on Patient Management
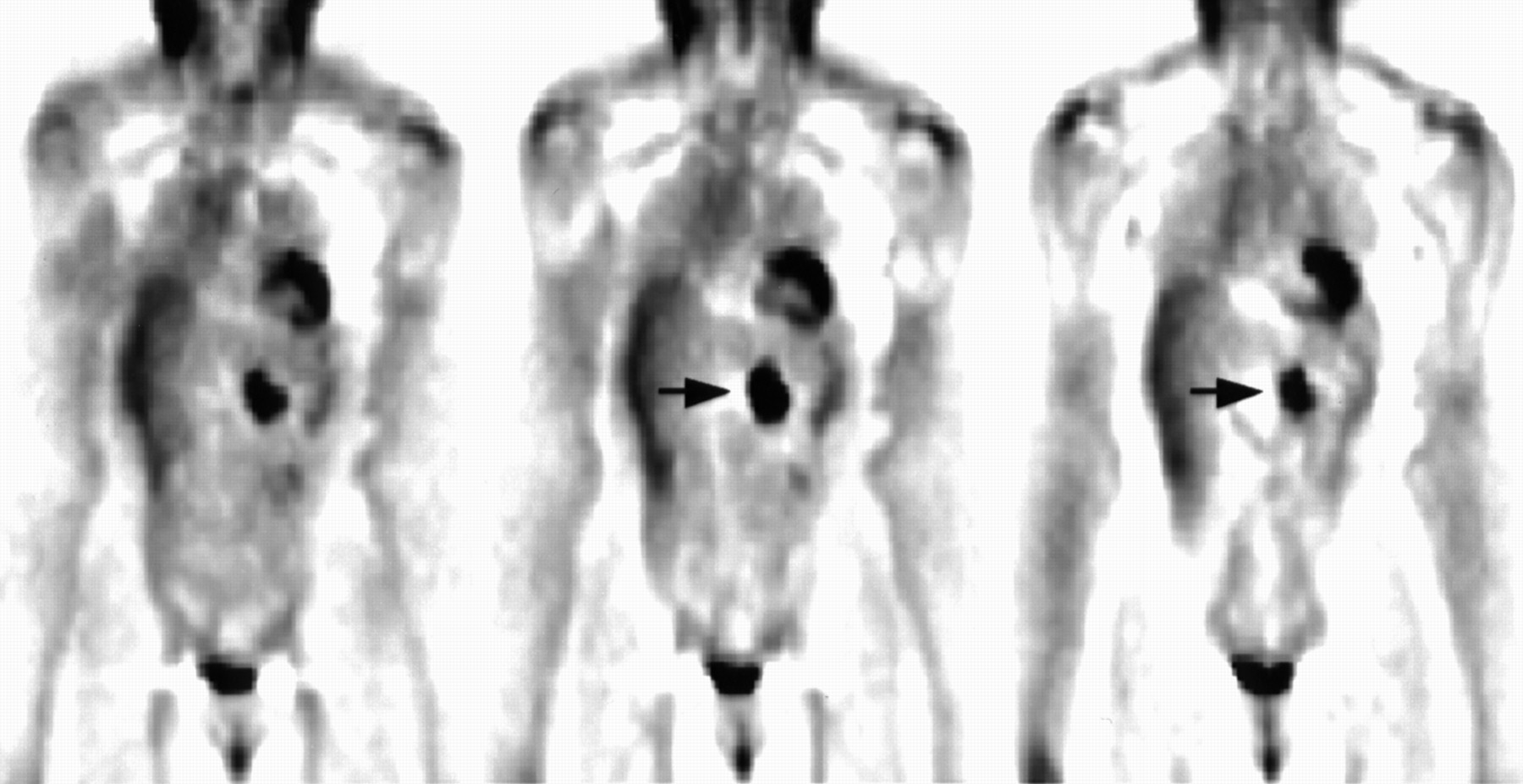
PET findings resulted in intermodality treatment changes in 22 patients (37%) (Fig. 2), intramodality changes in 11 patients (18%), and no change in treatment in 19 patients (32%). Referring physicians changed patient management to a combination of modalities in 4 patients (7%). The question was not answered in 3% of the surveys. Other management changes not specified in the questionnaire occurred in the remaining 3% of patients.
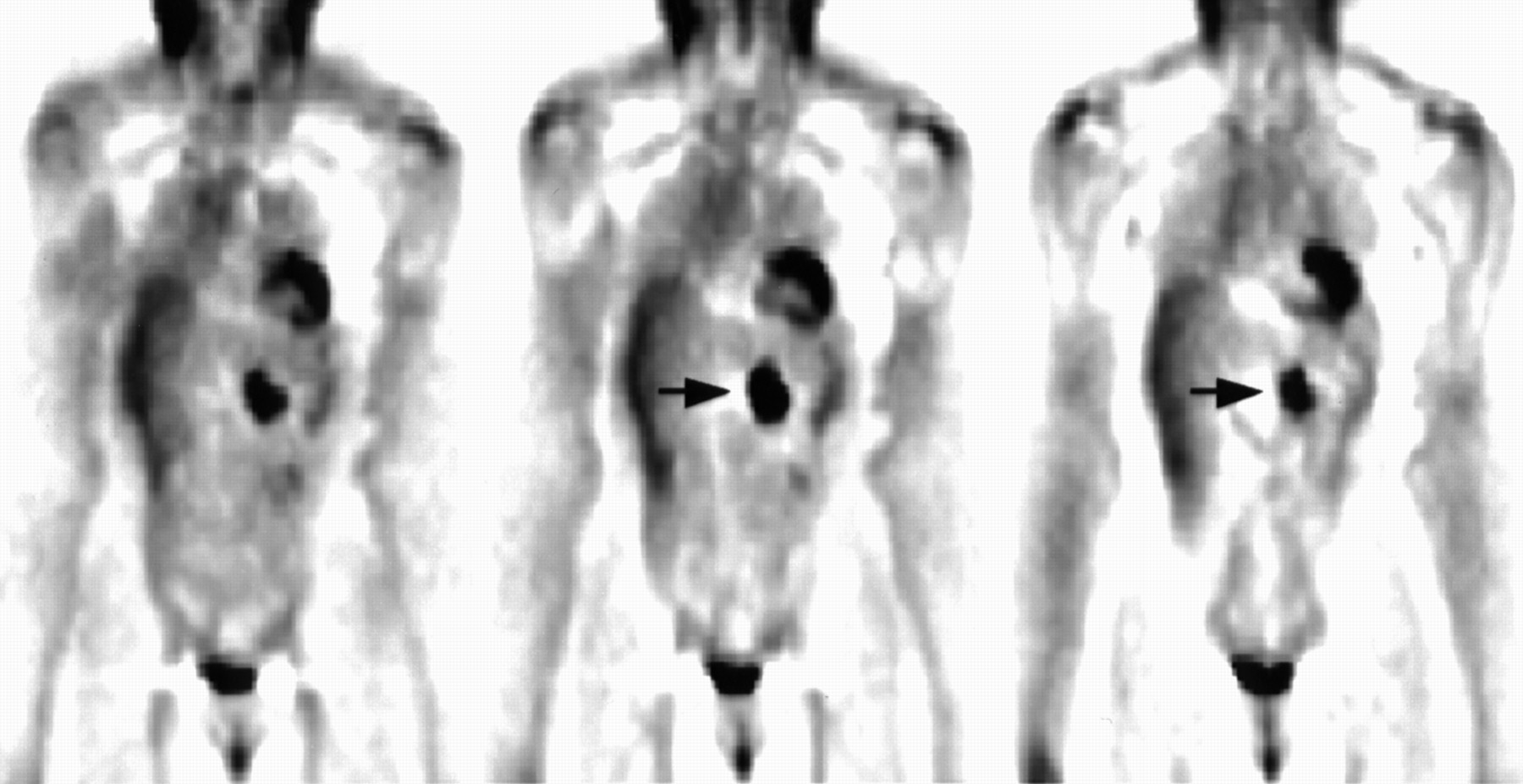
A 64-y-old female patient with colorectal cancer restaged for tumor recurrence 6 mo after chemotherapy. Tumor markers and CT scan were negative for tumor recurrence. FDG PET images show large focus of increased tracer uptake suggesting mesenteric lymph node involvement (arrows). Management was changed from no therapy to chemotherapy.
Intermodality changes occurred in 70% of patients who were upstaged by PET, in 60% of those who were downstaged, and in 13% of patients who had no change in clinical stage by PET. Intramodality changes occurred in 15% of patients who were upstaged, 40% who were downstaged, and 16% who had no change in clinical stage. No change in management occurred in 5% of patients who were upstaged.
Table 2 specifies the management changes for each individual patient.
Impact of PET on Clinical Management
DISCUSSION
To our knowledge, this study is the first to address the impact of whole-body PET on managing patients with colorectal cancer from the referring physician’s point of view. This study shows that PET alters the clinical stage in 42% and changes the clinical management in >60% of the patients with colorectal cancer. The study also indicates that referring physicians accept the findings and use the information provided by PET to change the clinical management in a large proportion of patients with colorectal cancer. Table 3 illustrates how PET affected management in the 22 patients whose pre-PET intended treatment was surgery. Specifically, it shows that 15% of the entire study population, or 41% of those patients for whom surgery was listed as the initial treatment, had a reported treatment change from surgery to radiation, medical treatment, or no treatment. On the other hand, surgery was chosen as the treatment of choice in 12% of the patients because of PET findings.
Patients for Whom Surgery Was Intended Pre-PET Treatment
These results are in keeping with previous studies, which reported that PET changed patient management or the clinical stage in 20%–50% of patients with colorectal cancer (10,17–20). Valk et al. (21) analyzed the potential impact of PET on patient management. This analysis was based on discussions with referring physicians and on the assumption that patients with more than one metastatic lesion were no longer surgical candidates. The costs of surgical procedures that were avoided because of PET were then compared with the cost of PET imaging. The authors reported that unnecessary surgery would have been avoided in 32% of the patients with recurrent colorectal cancer and concluded that $3,000 per patient could have been saved if PET would have been included in the management algorithm (21). Similar estimates regarding the potential impact of PET were provided by Delbeke et al. (10), who investigated retrospectively the effect of PET on surgical management of these patients. These authors found that PET changed patient management in 28% of patients with colorectal cancer. Surgery planning was facilitated in 6 patients and unnecessary surgery was avoided in 11 patients.
This survey-based study has several limitations. Fifty-nine percent of the surveys were not returned by the referring physicians, which likely introduced a “responder” bias. As a worst-case scenario, only supporters of PET might have responded, whereas those who believed that PET imaging was not useful for patient management might have refrained from participating in this study. However, assuming this scenario, PET would have affected the clinical stage and management in 17% and 21% of all patients, respectively. However, the response rate in one of the two study sites (NCPIC) was significantly higher (44%), decreasing the probability that the data were skewed in this direction. More important, the impact of PET on patient stage and clinical management did not differ between the two sites.
The response rate of 41% is likely explained by several factors. Varying interests in the subject of the survey, the length of the questionnaires, and other parameters affect response rates. In addition, less isolated and more “with-it” doctors tend to respond more frequently. A comparison between respondents and nonrespondents to our survey revealed no large bias. Cartwright (22) reported that the level of training and professional specialty did not vary between respondents and nonrespondents. In our survey, 53% of the respondents and 53.5% of the nonrespondents were oncologists, 2% and 3.5% were radiation oncologists, 27% and 21% were surgeons, and 15% and 21% were general practitioners. These differences in specialties between respondents and nonrespondents were not significant. Thus, a bias based on specialty can be ruled out. Furthermore, no significant differences were found between normal and abnormal PET scans for responders and nonresponders (normal and abnormal PET scans were found in 23% and 77% of the responders and in 30% and 70% of nonresponders). A recent study, which had a response rate of 43%, estimated the error introduced by such bias to range from 3% to 10% (23). These authors used a parallel survey to validate their findings and concluded that even response rates of 60%–70% would not have altered their findings.
The accuracy of whole-body PET imaging for the staging of recurrent colorectal cancer has been established. Strauss et al. (24) examined 29 patients with colorectal cancer and found recurrent disease in 21. In the remaining 8 patients, masses that were suggestive of cancer on CT were ruled out by biopsy (n = 7) or surgery (n = 1).
A similar accuracy was reported by Delbeke et al. (10), who used FDG PET on 51 patients with suspected recurrent colorectal cancer. They showed that PET was more accurate than CT for characterizing both intrahepatic and extrahepatic lesions. In most of these patients, histopathology served as the gold standard.
Similar findings were reported by Schiepers et al. (3). They evaluated the clinical value of FDG PET in 76 patients who presented with or were suspected of having recurrent local or distant colorectal cancer. PET results were compared with those of routine imaging (CT of the pelvis, CT or sonography of the liver, and chest radiography). The accuracy of PET for local disease was 95%, which was superior to CT of the pelvis (accuracy, 65%). PET accuracy for liver metastases (98%) compared favorably with anatomic imaging (93%). Unexpected extrahepatic metastases were detected by PET in 10 patients. These authors concluded that the main value of PET was an improved staging of apparently resectable, local, or distant recurrent disease. Thereby, a more adequate indication of major secondary surgery could be attained (3). In that study, 20% of the patients were upstaged and about 5% were correctly downstaged by PET. These findings were confirmed subsequently in an expanded group of patients from the same institution (25). Valk et al. (21) addressed the diagnostic accuracy and cost-effectiveness of this PET imaging in 155 consecutive patients with recurrent colorectal cancer. In this prospective, blinded study the authors reported similar specificities for PET and CT (98% vs. 96%), yet a significantly higher sensitivity was reported for PET (93% vs. 69%). Specifically, PET proved to be more accurate than CT for detecting liver lesions, pelvic involvement, extrahepatic abdominal metastases, and retroperitoneal disease.
All of these studies provide the justification for including PET in the diagnostic work-up of patients with colorectal cancer. However, none of the studies has evaluated prospectively the impact of PET on the management of patients with colorectal cancer from a referring physician’s point of view.
CONCLUSION
This survey-based study of referring physicians shows that FDG PET has a major impact on the management of colorectal cancer patients, contributing to changes in the clinical stage and major management decisions in >40% of patients.
Acknowledgments
The authors thank Ron Sumida, Larry Pang, Francine Aquilar, Der-Jen Liu, Priscilla Contreras, and Sumon Wongpiya for their excellent technical assistance in performing the clinical PET studies and Diane Martin for assistance with graphics.
Footnotes
Received Jul. 19, 2000; revision accepted Dec. 11, 2000.
For correspondence or reprints contact: Johannes Czernin, MD, Department of Molecular and Medical Pharmacology, Ahmanson Biological Imaging Clinic/Nuclear Medicine, University of California, Los Angeles, School of Medicine, AR-259 Center for the Health Sciences, Los Angeles, CA 90095-6948.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Lack of Evidence for PET or PET/CT Surveillance of Patients with Treated Lymphoma, Colorectal Cancer, and Head and Neck Cancer: A Systematic Review
- 18F-FDG PET and PET/CT in the Evaluation of Cancer Treatment Response
- PET Changes Management and Improves Prognostic Stratification in Patients with Recurrent Colorectal Cancer: Results of a Multicenter Prospective Study
- The National Oncologic PET Registry (NOPR): Design and Analysis Plan
- Recent Chemotherapy Reduces the Sensitivity of [18F]Fluorodeoxyglucose Positron Emission Tomography in the Detection of Colorectal Metastases
- Comparison Between 18F-FDG PET, In-Line PET/CT, and Software Fusion for Restaging of Recurrent Colorectal Cancer
- Metabolic Response After Intraarterial 90Y-Glass Microsphere Treatment for Colorectal Liver Metastases: Comparison of Quantitative and Visual Analyses by 18F-FDG PET
- Clinical Decisions Associated With Positron Emission Tomography in a Prospective Cohort of Patients With Suspected or Known Cancer at One United States Center
- 18F-Fluoro-2-deoxyglucose positron emission tomography in the evaluation of gastrointestinal malignancies
- Impact of Whole-Body 18F-FDG PET on Staging and Managing Patients for Radiation Therapy
- The Role of Positron Emission Tomography in Colorectal Carcinoma
- The Impact of PET on the Management of Lung Cancer: The Referring Physician's Perspective
- Role of 18F-FDG Dual-Head Gamma-Camera Coincidence Imaging in Recurrent or Metastatic Colorectal Carcinoma
- Impact of Whole-Body 18F-FDG PET on Staging and Managing Patients with Breast Cancer: The Referring Physician's Perspective
- Effect of Whole-Body 18F-FDG PET Imaging on Clinical Staging and Management of Patients with Malignant Lymphoma