


Abstract
FDG PET has emerged as an important clinical imaging modality for diagnosing and staging cancer. However, the impact of FDG PET on staging and managing patients with breast cancer from the referring physician’s point of view is unknown. Methods: The referring physicians of 160 breast cancer patients received standardized questionnaires inquiring if and how PET findings altered their patient’s stage and their clinical management decisions. Management changes were classified as intermodality if the change was from one modality to another (e.g., medical to surgical, surgical to radiation, medical to no treatment, and vice versa) or as intramodality if the change was within the same modality (e.g., altered medical or radiotherapy approach). Results: Fifty of the 160 surveys were completed (31% response rate). PET changed the clinical stage in 36% of patients (28% upstaged, 8% downstaged) and resulted in intermodality changes in 28% of patients and intramodality changes in 30% of patients. Conclusion: The results of this prospective survey show that FDG PET has a major impact on the management of breast cancer patients, influencing both clinical stage and management in more than 30% of patients.
Although lung cancer has surpassed breast cancer as the leading cause of cancer deaths in American women since 1987, breast cancer alone is expected to account for 182,800, or nearly one third, of all new female cancer cases this year. It is also estimated that breast cancer will account for 15% of cancer mortality among American women (1).
As with other cancers, management decisions are complex and are often affected by the judgment of the physician and by the desires of the patient. Accurate staging is therefore critical to determining the best therapeutic approach for breast cancer patients.
PET with 18F-FDG detects metabolic alterations that occur in malignant tumor cells. Compared with normal tissues, neoplastic cells have an increased glucose metabolism (2–5), the extent of which correlates with the aggressiveness of tumor growth (2,6). Because oxidative metabolism is nearly absent, tumor cells rely on glucose metabolism to meet the energy requirements of rapidly dividing tissues. Markedly accelerated rates of the hexose monophosphate shunt result in large amounts of ribose-6-phosphate, which provides the carbon backbone for DNA and RNA synthesis in tumor cells. These alterations can be imaged and detected with FDG PET (2–5).
Several studies have shown that FDG PET detects and stages breast cancer with a high diagnostic accuracy (7–11). FDG PET has also been used to monitor the effects of treatment in these patients (12,13). However, whether PET findings alter the clinical stage and cause referring physicians to change the management of their patients are unknown. This prospective survey was designed to determine the impact of whole-body FDG PET imaging on the staging and management of breast cancer patients from the referring physician’s perspective.
MATERIALS AND METHODS
Referring Physicians and Patients
The referring physicians of 160 breast cancer patients who underwent whole-body FDG PET at the Ahmanson Biological Imaging Center/Nuclear Medicine Clinic of the University of California, Los Angeles (UCLA) (n = 115; 72%) and the Northern California PET Imaging Center, Sacramento, CA (NCPIC) (n = 45; 28%), between October 1998 and August 2000 were surveyed. Completed questionnaires were received from 32 referring physicians for 50 patients (age range at PET, 30–79 y; mean age ± SD, 57 ± 12 y). Thirty-eight (76%) of these patients were referred to UCLA and 12 (24%) to the NCPIC.
Image Acquisition and Reconstruction
The patients were instructed to fast for at least 6 h before PET imaging (14). Emission scans of the body starting 45 min after intravenous administration of approximately 555 MBq (15 mCi) FDG were acquired for 6–9 bed positions (6 min per bed position) for each patient. Scanning was performed using an EXACT or HR+ system (CTI, Knoxville, TN/Siemens Medical Systems, Inc., Hoffman Estates, IL). The resolution of reconstructed images is approximately 8–12 mm for these devices (15–17). The acquired image sets were displayed in transaxial, coronal, and sagittal planes and were evaluated clinically along with the 3-dimensional projection images on a computer screen. At UCLA, images were reconstructed using standard filtered backprojection without attenuation correction (18). At the NCPIC, iterative image reconstruction algorithms were used and transmission scans were obtained so that attenuation-corrected images were also available for evaluation (19,20).
Image Interpretation
The clinical PET images were interpreted and the corresponding PET reports generated on the basis of all available clinical information. Quantitative or semiquantitative analysis of FDG uptake in lesions, such as region-of-interest analysis or calculation of standardized uptake value, was not performed because such analyses are not part of the protocol for routine interpretation of clinical images at either of the institutions involved.
The impact of PET imaging on patient management was evaluated through pre-PET and post-PET questionnaires (21), which were sent as a single fax to the referring physicians, along with the official interpretive PET report, within 1 wk of the PET study. This simple, straightforward approach was chosen to minimize the administrative burden for referring physicians and to increase the likelihood of response. The pre-PET portion of the questionnaire asked physicians to specify the clinical stage of each patient. The updated scheme of the American Joint Committee on Cancer (22) on TNM staging of breast cancer was attached to the questionnaire. Further, the pre-PET questionnaire asked about the intended management plan before PET. The post-PET questionnaire asked if PET caused any changes in the cancer stage and patient management. Further, the referring physicians were asked to specify the management changes prompted by the PET findings.
When the completed surveys were received, the PET-induced management changes were classified as intermodality changes, intramodality changes, or no change in modality. Intermodality changes refer to alterations from one treatment modality to another, such as from surgery to radiation therapy or from medical treatment to no treatment. Intramodality changes encompass those that were made within a treatment modality, such as from one chemotherapeutic agent to another, and those that involved adding or removing a chemotherapeutic agent.
RESULTS
One hundred sixty patients with breast cancer were referred to the 2 study centers for whole-body PET. Thirty-two different physicians responded to the survey, and 50 completed questionnaires were received, resulting in a response rate of 31% (38/115, or 33%, for patients scanned at UCLA; 12/45, or 27%, for patients scanned at the NCPIC).
The specialties of the responders were as follows: medical oncologists (63%), surgeons (16%), radiation oncologists (6%), and general practitioners (16%). The distribution of specialties did not differ significantly between the physicians who responded and those who did not or between the 2 institutions involved.
Whole-body FDG PET was ordered most frequently for more accurate staging of breast cancer (52%). In fact, all these patients were referred for restaging. In 16% of the patients, PET was ordered for a more accurate diagnosis. Monitoring the course of disease (14%), monitoring therapy (8%), and a combination of 2 or more of the above reasons (8%) accounted for the indications in the remaining patients. The referring physician of 1 patient (2%) did not provide an answer. The clinical indications for PET did not differ significantly between the 2 study centers or between responders and nonresponders.
PET resulted in changes in clinical stage in 36% of the patients. The disease was upstaged for 14 (28%) and downstaged for 4 (8%). PET did not result in changes in clinical stage in 60% of the patients. The referring physicians of the remaining 2 patients (4%) did not respond to this question. The PET-induced changes in stage are listed in Table 1.
Impact of PET on Clinical Stage
PET resulted in intermodality management changes for 14 patients (28%), intramodality changes for 15 (30%), and no change for 13 (26%). One patient (2%) underwent both intermodality and intramodality changes, 3 patients (6%) underwent other unspecified changes, and this question remained unanswered for the remaining 4 patients (8%).
Six (43%) of the 14 patients whose cancer was upstaged by PET underwent intermodality changes, whereas another 6 (43%) underwent intramodality changes. One patient (7%) whose cancer was upstaged had both intermodality and intramodality changes, whereas another patient (7%) whose cancer was upstaged had no management change. Intermodality changes occurred in 2 (50%) of 4 patients whose cancer was downstaged, whereas intramodality changes occurred in the remaining 2 patients.
Clinical management was changed for some of the 30 patients whose stage was not altered by PET: 6 (20%) of these had intermodality changes, 7 (23%) had intramodality changes, and 3 (10%) had other, unspecified changes. Table 2 specifies the management changes for the study group.
Impact of PET on Clinical Management
DISCUSSION
This prospective survey showed PET to have a considerable impact on staging and managing breast cancer patients. PET altered the clinical stage in 36% of patients and the clinical management in 60%. This study also supports the notion that referring physicians accept FDG PET as an important diagnostic staging modality for the care of their patients.
The results are in keeping with a previous report suggesting that FDG PET added information on the extent of disease in 29% of the 41 patients studied (23), mainly through detection of additional lymph node involvement. Importantly, in the current study PET uncovered unknown lymph node metastases (n = 5) and unknown distant metastases (n = 8) (Fig. 1 shows a case example) in 10 patients (20% of the entire population; both unknown lymph node metastases and unknown distant metastases were found in 3 of these patients).
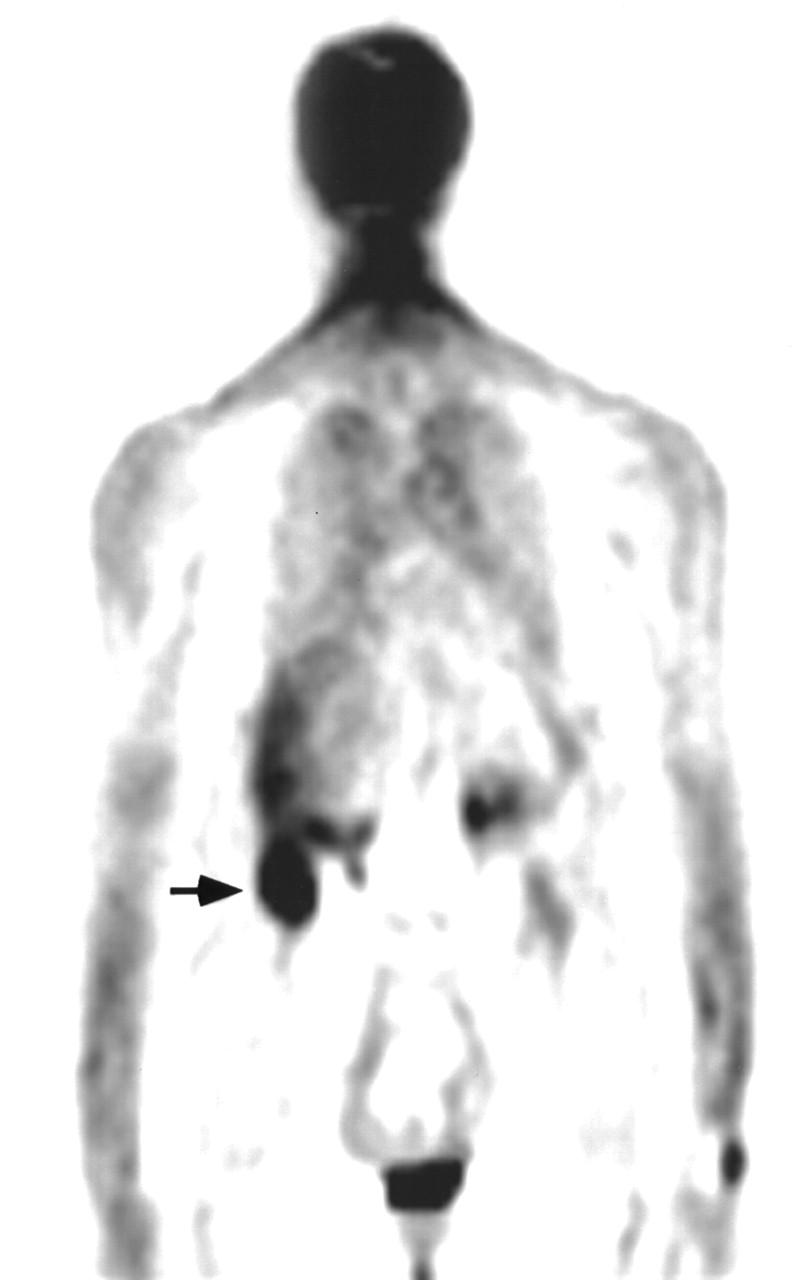
A 73-y-old woman with history of mastectomy for cancer of right breast. She was examined with PET because of rising tumor markers. Anterior coronal cut showed intense hypermetabolic focus (arrow) at inferior tip of right liver lobe, consistent with large, solitary liver metastasis. Cancer was upstaged, and clinical management was changed from medical treatment to surgery.
The fact that 53% of those patients whose stage was not altered by PET nevertheless were managed differently after PET is noteworthy and suggests that PET provided the referring physicians with additional pertinent staging information. For instance, in patients with stage IV disease, additional nodal or distant metastatic disease detected by PET may not result in a stage change but may result in different management plans.
The current study has several limitations. First, whether all the management changes that were intended really took place is unknown. A study addressing this issue and further evaluating the outcome of these patients is currently under way. Second, the 31% response rate likely introduced a “responder bias.” Only those referring physicians who believed PET had provided useful information for the management of their patients might have responded to the survey. Those who did not respond might have believed that PET did not add useful information. However, even in the unlikely event that all nonresponders believed PET had no effect on stage or management, 11% and 21% of the entire population of 160 patients would have incurred a change in stage and management, respectively, because of the PET findings.
The issue of responder bias was addressed by a recent study by Sjöström et al. (24), who reported that questionnaire studies tend to have a bias caused by both nonresponse and incorrect answers and that this bias can be substantial. Although such factors should not be dismissed, one should be aware that those authors conducted a parallel survey to validate their findings and found that even higher response rates of 60%–70% (their actual response rate was 43%) would not have altered their findings.
The low response rate of the current study can be accounted for by several factors, such as varying degrees of interest among referring physicians in the subject of the survey, the length of the questionnaires, and their 2-component (pre- and post-PET) aspect. The response rate was slightly higher at UCLA (33%) than at the NCPIC (27%); however, this difference was not statistically significant. Also, the impact of PET on stage and clinical management did not differ between the 2 study sites. An important finding is that the clinical specialty and level of training did not vary between the responders and nonresponders (25); hence, the possibility of a bias based on specialty can be ruled out.
The breast cancer in this study was classified as stage IV in 36% of patients before PET but in 52% after PET. Thus, PET revealed unknown distant metastases in 8 patients. This finding shows the value of PET, as a whole-body imaging technique, in providing additional information about the extent of metastatic involvement, which in turn affects clinical management in many patients.
CONCLUSION
The current survey of referring physicians showed that whole-body FDG PET affected clinical stage and management in 36% and 58%, respectively, of their breast cancer patients.
Footnotes
Received Dec. 12, 2000; revision accepted Apr. 9, 2001.
For correspondence or reprints contact: Johannes Czernin, MD, Ahmanson Biological Imaging Center/Nuclear Medicine Clinic, Department of Molecular and Medical Pharmacology, UCLA School of Medicine, AR-259 CHS, Los Angeles, CA 90095-6948.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- [18F]Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography in Breast Cancer: When... and When Not?
- The Effects of Estrogen, Progesterone, and C-erbB-2 Receptor States on 18F-FDG Uptake of Primary Breast Cancer Lesions
- FDG-PET/CT in restaging of patients with recurrent breast cancer: possible impact on staging and therapy
- Potential of Dual-Time-Point Imaging to Improve Breast Cancer Diagnosis with 18F-FDG PET
- Clinical Decisions Associated With Positron Emission Tomography in a Prospective Cohort of Patients With Suspected or Known Cancer at One United States Center
- 18F-2-Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography in Staging of Locally Advanced Breast Cancer
- Impact of Whole-Body 18F-FDG PET on Staging and Managing Patients for Radiation Therapy
- The Impact of PET on the Management of Lung Cancer: The Referring Physician's Perspective