


Abstract
Standard application of CT intravenous contrast agents in combined PET/CT may lead to high-density artifacts on CT and attenuation-corrected PET. To avoid associated diagnostic pitfalls, we designed and compared different intravenous contrast injection protocols for routine whole-body PET/CT. Methods: Whole-body PET/CT included a topogram and a single spiral CT scan (2-row) with or without intravenous contrast, followed by an emission scan. The CT scan was used for attenuation correction of the emission data. Four groups of 10 whole-body PET/CT referrals each were investigated: (A) no intravenous contrast agent, (B) biphasic injection (90 and 50 mL at 3 and 1.5 mL/s, respectively) of intravenous contrast (300 mg/mL iodine) and CT in the craniocaudal direction with a 30-s delay, (C) triple-phase injection (90, 40, and 40 mL at 3, 2, and 1.5 mL/s, respectively) in the craniocaudal direction with a 50-s delay, and (D) dual-phase injection (80 and 60 mL at 3 and 1.5 mL/s, respectively) in the caudocranial direction with a 50-s delay. CT image quality was assessed on a scale from 1 to 3, and CT and attenuation-corrected PET images were reviewed separately for contrast-induced artifacts. Results: Average CT image quality was poorest for protocol A (1.0) but improved to 2.8 when using intravenous contrast agents (protocols B–D). Only protocols B and C resulted in contrast-induced image artifacts that were limited to the thorax. The most homogeneous intravenous contrast enhancement without high-density image artifacts on either CT or PET after CT-based attenuation correction was achieved with protocol D. Conclusion: Dual-phase intravenous contrast injection and CT in the caudocranial direction with a 50-s delay yields reproducible high image quality and is now used routinely for combined diagnostic PET/CT at our hospital.
The combination of functional and anatomic images, originally through retrospective software-based image registration (1,2) and, since 1998, through a hardware-based approach (3), was shown to yield a diagnostic benefit in clinical oncology when compared with separate imaging (4,5). A combined PET/CT examination can replace separate CT and PET scans, if both examinations are performed with high standards to obtain a diagnostic image quality, which is equivalent to the image quality of each examination alone. Such a PET/CT scenario, however, includes careful patient preparation according to stand-alone CT and PET and the application of CT contrast media.
Several standardized protocols for intravenous contrast administration have been accepted in CT practice today to yield routinely exquisite CT image quality throughout the body (6–10). However, it has been shown that the unmodified adoption of these intravenous contrast injection protocols into whole-body PET/CT scenarios may lead to artificial tracer uptake patterns on PET after CT-based attenuation correction. Antoch et al. discussed these artifacts for the case of a single-phase bolus injection of intravenous contrast (11). Others have discussed similar-type artifacts for the unmodified use of positive oral contrast agents (12). Thus, alternative, water-based oral contrast agents have been proposed, which were shown to result in artifact-free diagnostic CT and PET images (13).
In the lack of alternative, low-attenuating agents for intravenous contrast enhancement, however, several groups have suggested to correct the CT images retrospectively by segmenting the intravenous contrast-enhanced tissues and replacing the attenuation coefficients with that of water (soft tissue) before using the CT for CT-based attenuation correction (14). Although this approach has been shown to resolve the issue of contrast-induced artifacts on attenuation-corrected PET images from PET/CT scans, it is not available yet; furthermore, it does require a rather significant operator interaction, which perhaps cannot be provided routinely in clinical practice.
Therefore, the aim of our study was to derive an optimized intravenous contrast injection protocol for whole-body PET/CT that prospectively provides both, CT image quality equivalent to separate CT and attenuation-corrected PET images free of contrast-related artifacts as part of the combined dual-modality PET/CT examinations.
MATERIALS AND METHODS
Patients
This study included 40 patients (15 lung cancer, 6 gastrointestinal and 4 colorectal cancer, 3 lymphoma, 3 thyroid cancer, and 9 other malignant diseases) who were referred for a combined PET/CT study with 18F-FDG. All patients signed an informed consent, which details the use of intravenous and oral CT contrast and rare potential side effects. The PET/CT acquisition protocol was performed in accordance with our hospital guidelines for diagnostic procedures.
PET/CT Acquisition and Intravenous Contrast Injection
All patients were examined on a dual-modality PET/CT tomograph (biograph BGO duo; Siemens Medical Solutions) (15,16). The CT components of the biograph BGO duo correspond to a Somatom Emotion Duo (Siemens Medical Solutions), a 2-row spiral CT system with a maximum continuous scan time of 100 s and a maximum rotation speed of 75 rpm. The PET components of the combined PET/CT tomograph are based on an ECAT EXACT HR+ (Siemens Medical Solutions), a full-ring bismuth germanate (BGO)-based PET system (17).
PET/CT was performed according to 1 of 4 protocols with or without intravenous contrast, whereby groups of 10 subjects each were investigated (Table 1). Protocol A corresponded to a nonenhanced imaging protocol without intravenous contrast. Protocols B–D corresponded to intravenous contrast injection protocols, which were adapted from clinical practice in our hospital with stand-alone CT (Table 1). Protocol B, referred to as the standard protocol, included a dual-phase injection of 90 and 50 mL (at 3 and 1.5 mL/s, respectively) of intravenous contrast and CT scanning in the craniocaudal direction with a 30-s delay. Protocol C, referred to as the extended protocol, was similar to protocol B, except a third phase of intravenous contrast injection (40 mL at 1.5 mL/s) was added for a continuous enhancement of the abdomen during the whole-body CT scan. Protocol D, referred to as the modified protocol, included a dual-phase injection of 80 and 60 mL (at 3 and 1.5 mL/s, respectively) with both the scan delay increased to 50 s and the CT scan direction reversed to image the abdomen with sufficient contrast enhancement and to avoid high-density artifacts in the subclavian vein (11). All 3 enhanced protocols were based on Xenetix 300 (Guerbet GmbH) with 300 mg of iodine per milliliter as the intravenous contrast material of choice.
Patient Groups for Adapted Intravenous Contrast Injection Protocols and Parameters for Intravenous Contrast Injection
Patients in each group (A–D) fasted for 4 h before the combined PET/CT examinations. The average administered activity of 18F-FDG was 360 ± 30 MBq. During the 18F-FDG uptake phase (90 ± 30 min) all patients were asked to drink 1.5 L of a water-equivalent oral contrast dispersion (13). This dispersion does not contain glucose, or glucose analogs, and is used routinely in PET/CT without known adverse side effects to the accumulation of 18F-FDG (13). Immediately before the PET/CT examination, patients were asked to void and to remove all jewelry and disposable metal implants. Patients were positioned head first supine on the common patient handling system with the arms raised and supported above the head in accordance with standard CT practice.
First, a topogram was acquired over 1,024 mm axially. Coaxial whole-body imaging ranges were defined on the topogram, covering an area from the base of the skull to the upper thighs (6–8 PET bed positions, or 80–100 cm, depending on the size of the patient). Intravenous contrast was administered according to 1 of the 4 protocols (A–D) described (Table 1). CT was performed in spiral mode using a continuous acquisition at 130 kVp, 115 mAs, 4-mm collimation, 5-mm slice width, a table feed of 8 mm per rotation at 0.8-s rotation time, and a 2.4-mm slice spacing. During the CT acquisition a limited breath hold protocol was followed, which required the patients to hold their breath in normal expiration (18).
After completion of the CT, patients were moved automatically to the PET toward the rear of the gantry, where 3-dimensional PET emission scanning subsequently started in the caudocranial direction with the bladder/pelvis region being scanned first. An emission scan time of 3.5 min per bed position was used for all patients, which resulted in a total emission scan time of no more than 28 min (8 bed positions) and a total PET/CT examination time, including the CT, of about 30 min. The CT transmission images were used for attenuation correction of the PET emission data, as described in detail by Kinahan et al. (19). After scatter and attenuation correction, PET emission data were reconstructed using an attenuation-weighted ordered-subsets maximization expectation approach (20) with 2 iterations and 8 subsets on 128 × 128 matrices and with a 5-mm gaussian postreconstruction filtering.
Image Review and Analysis
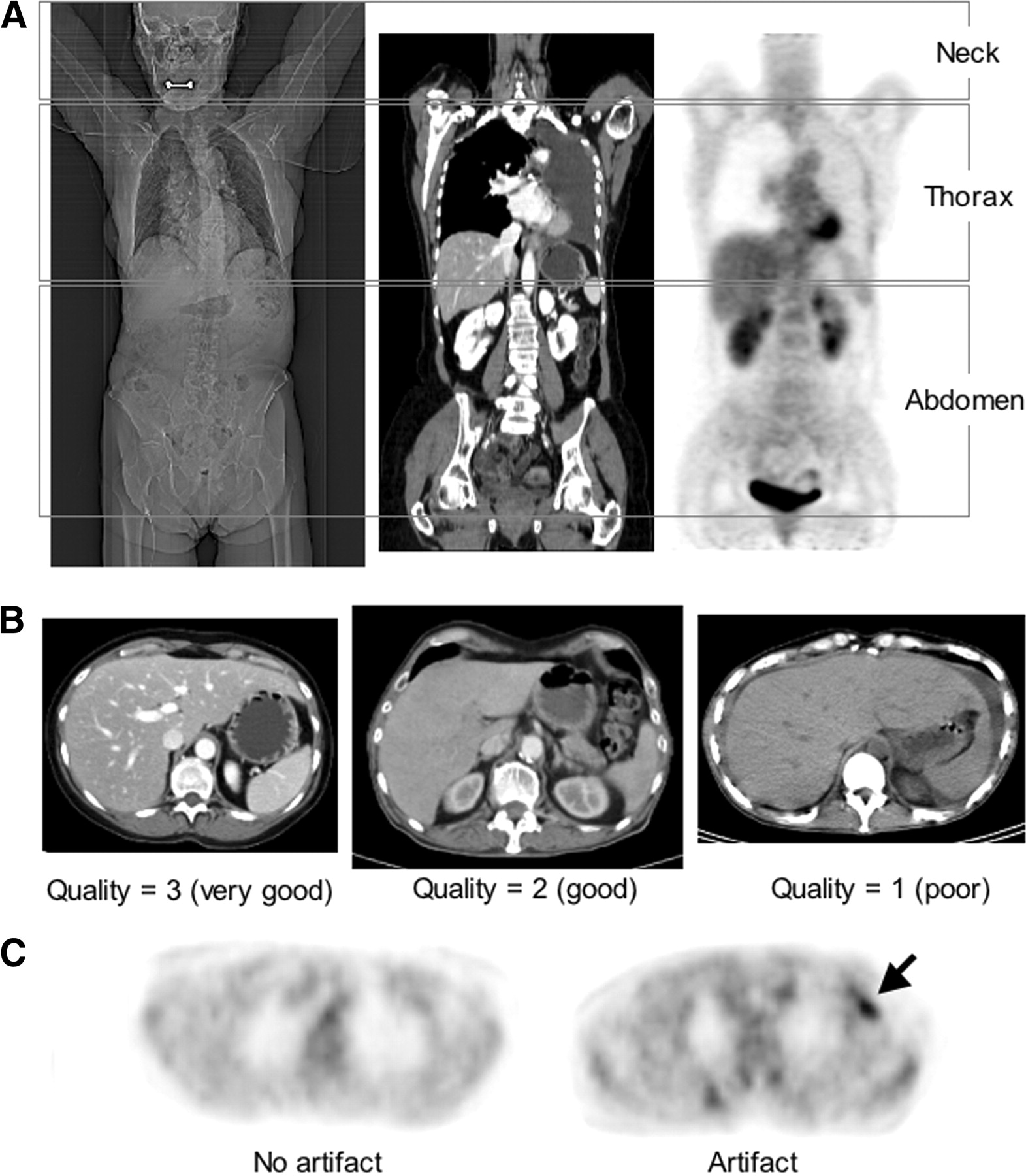
Image analysis was performed on a syngo viewing station (Siemens Medical Solutions). CT and PET images were assessed independently. Image quality assessment was reported for the neck, thorax, and abdomen (Fig. 1A). Three independent radiology readers with at least 18 mo of PET/CT experience graded the diagnostic quality of the CT images. We used a 3-point scale (Fig. 1B) in reference to image quality from dedicated CT in radiology practice at our hospital. If CT image quality and intravenous contrast enhancement were perceived as equivalent to separate, dedicated CT, then image quality was graded as 3 (very good). If intravenous contrast enhancement and CT image quality were not optimal, but contrast between enhanced and nonenhanced structures was acceptable, then image quality was graded as 2 (good). In all other cases, image quality was graded as 1 (poor). An average CT image quality score was calculated for each of the 3 regions (neck, thorax, and abdomen) and each of the 4 scan protocols (A–D) as the average of the readings from the 3 radiology readers.

(A) Diagnostic image quality and contrast-induced abnormalities were assessed independently for 3 axial imaging ranges: neck, thorax, and abdomen. (B) Examples of diagnostic quality of thoracic CT images: 3 (very good), 2 (good), 1 (poor). (C) Examples of PET images after CT-based attenuation correction without and with artifact from intravenous contrast (arrow) are shown.
Radiology readers also reviewed the CT images for potential intravenous contrast-induced artifacts (yes/no) in the 3 regions (Fig. 1A). Furthermore, average CT attenuation values were estimated in major vessels in the neck, the thorax, and the abdomen by placing individual circular regions of interest (ROI) inside the internal jugular vein (IJV) and common carotid artery (CCA), the brachiocephalic vein (BV) and ascending aorta (AA), and the portal vein (PV), in the corresponding axial CT images of the neck, thorax, and abdomen, respectively. For each contrast protocol (Table 1) and vessel, an average CT attenuation value was calculated as the average of the independent readings of the 3 radiology readers, before calculating the mean CT attenuation in each vessel as the mean of the average attenuation values in all 10 subjects belonging to a particular contrast protocol. The variability of contrast enhancement from each protocol (A–D, Table 1) was described as the range of percent SD of the average CT attenuation value in the 5 vessels.
Two certified nuclear medicine physicians with at least 18 mo of PET/CT experience reviewed the attenuation-corrected PET images for potential artifacts from intravenous contrast agents without consulting the CT (Fig. 1C). In case of apparent image artifacts in the corrected PET that could be associated with intravenous contrast enhancement, lesion-to-background values were calculated from the ratio of a manually defined ROI, tightly including the potential artifact, and a similar-size ROI covering a physiologic uptake area in the vicinity of the same axial imaging plane. Lesion-to-background ratios were chosen as a simple descriptor of focal tracer enhancement. After identifying all potentially contrast-induced abnormalities on the corrected PET, PET/CT fusion images were used to jointly interpret the PET findings in the context of the correlated CT.
RESULTS
CT image quality was rated poorest for the nonenhanced protocol A: 1 ± 0, 1.1 ± 0.1, 1 ± 0 in the neck, thorax, and abdomen, respectively (Fig. 2A). Average CT image quality scores in these areas increased to 2.8 ± 0.3, 2.8 ± 0.2, and 2.8 ± 0.1 when using intravenous contrast (protocols B–D). Of all 3 contrast-enhanced protocols, B yielded the lowest CT image quality. Example CT images of the abdomen from patients enrolled in protocols A–D are shown in Figure 2B.
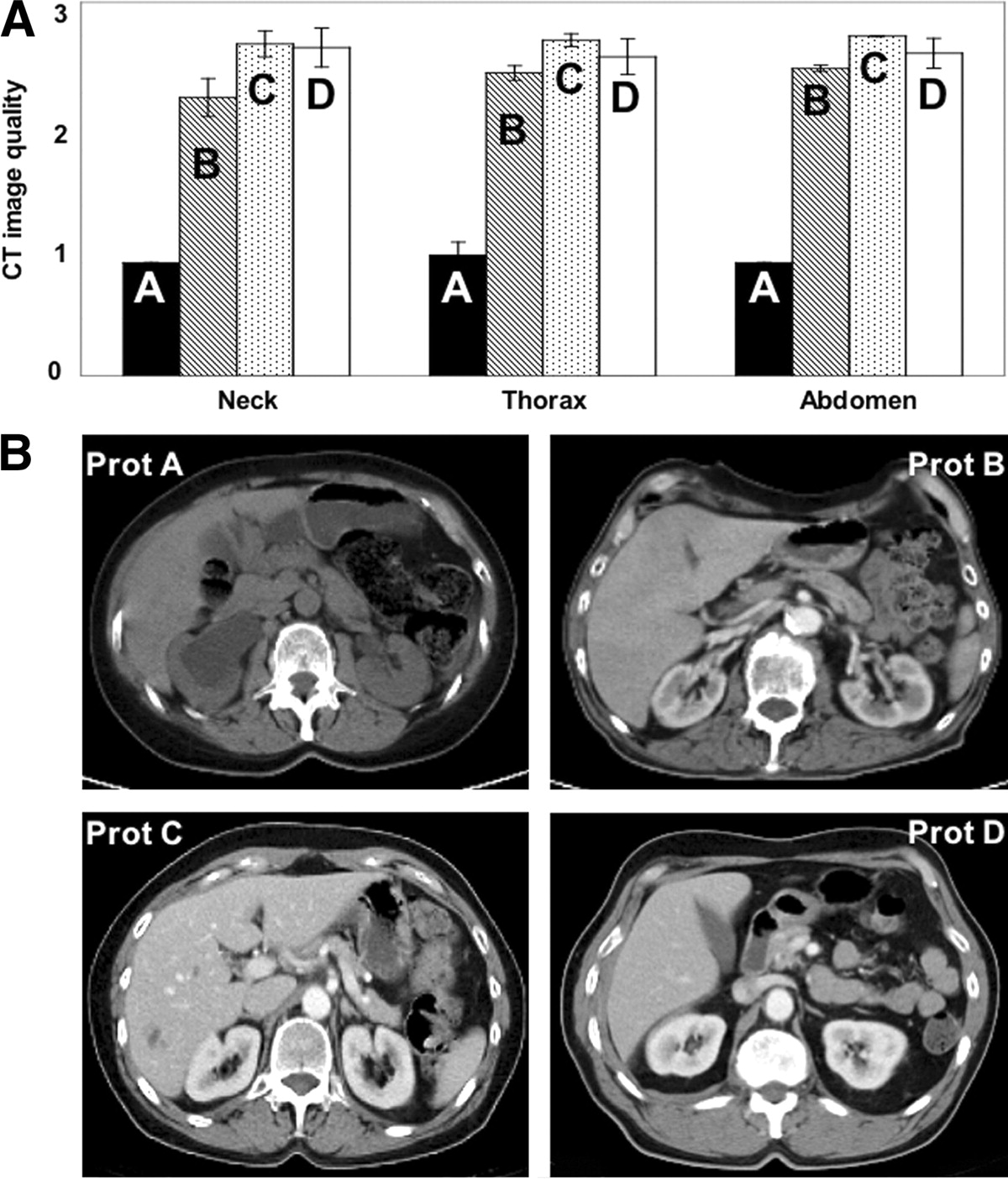
(A) Diagnostic quality of CT images averaged over ratings by 3 radiology reviewers. CT image quality was lowest for nonenhanced studies (protocol A) but increased throughout whole-body imaging range when intravenous contrast was used (protocols B–D). Examples of CT images (B) of abdomen for subjects enrolled in protocols A (nonenhanced) and B–D (intravenous contrast according to Table 1) are shown. Prot = protocol.
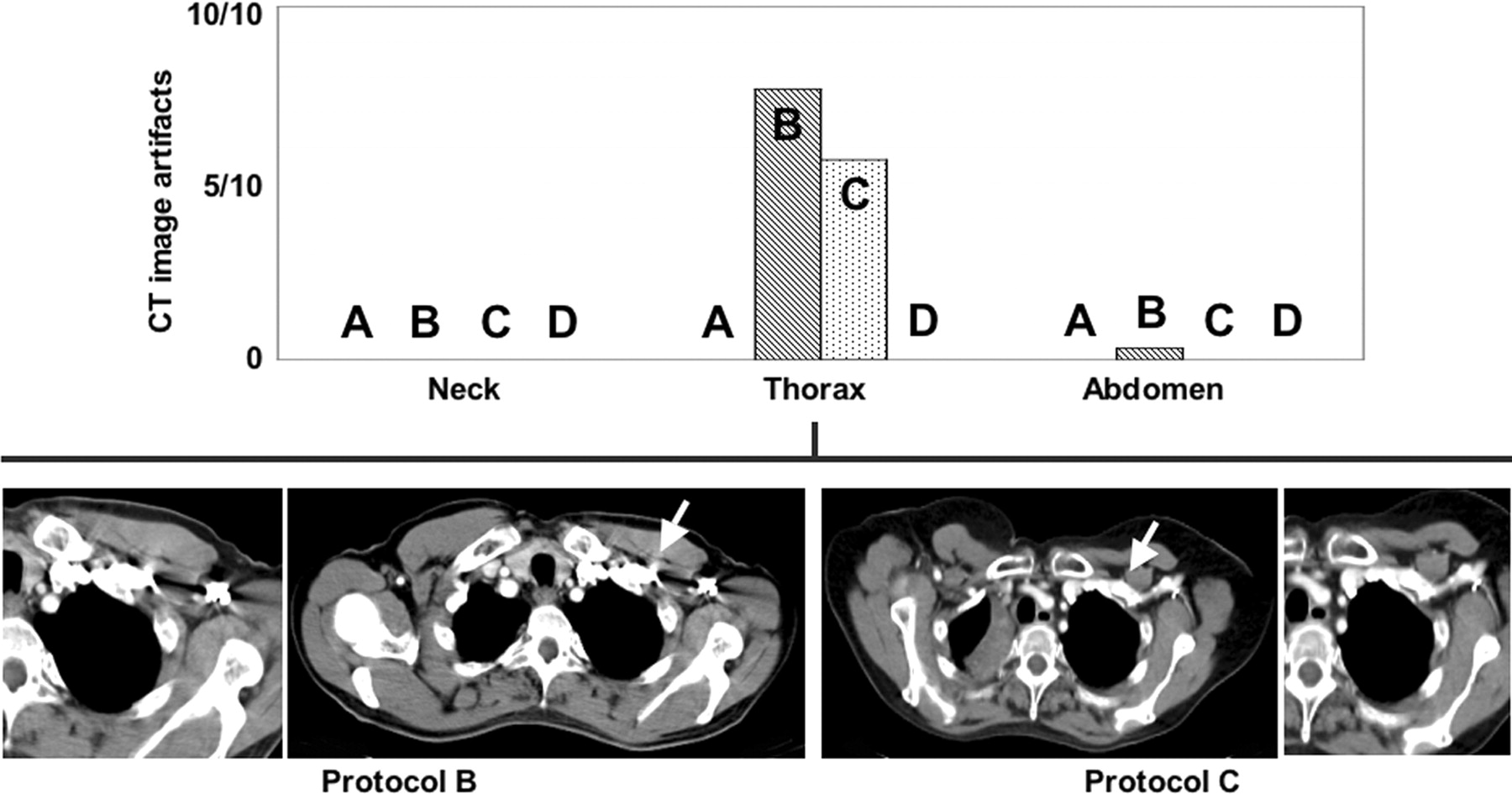
The fraction of CT images with high-density artifacts from intravenous contrast, averaged over the readings of the 3 radiology readers, is shown in Figure 3 for each of the 4 CT protocols (A–D). Neither protocol generated contrast-induced abnormalities in CT images of neck. Both the standard and the extended protocols caused high-density CT image artifacts in the thorax in 8 of 10 (protocol B) and 6 of 10 (protocol C) patients, respectively. Neither the nonenhanced protocol A nor the modified protocol D led to similar reports on contrast-induced artifacts on CT images of thorax. Only 1 case (standard protocol B) with contrast-induced artifacts on CT of abdomen was reported.
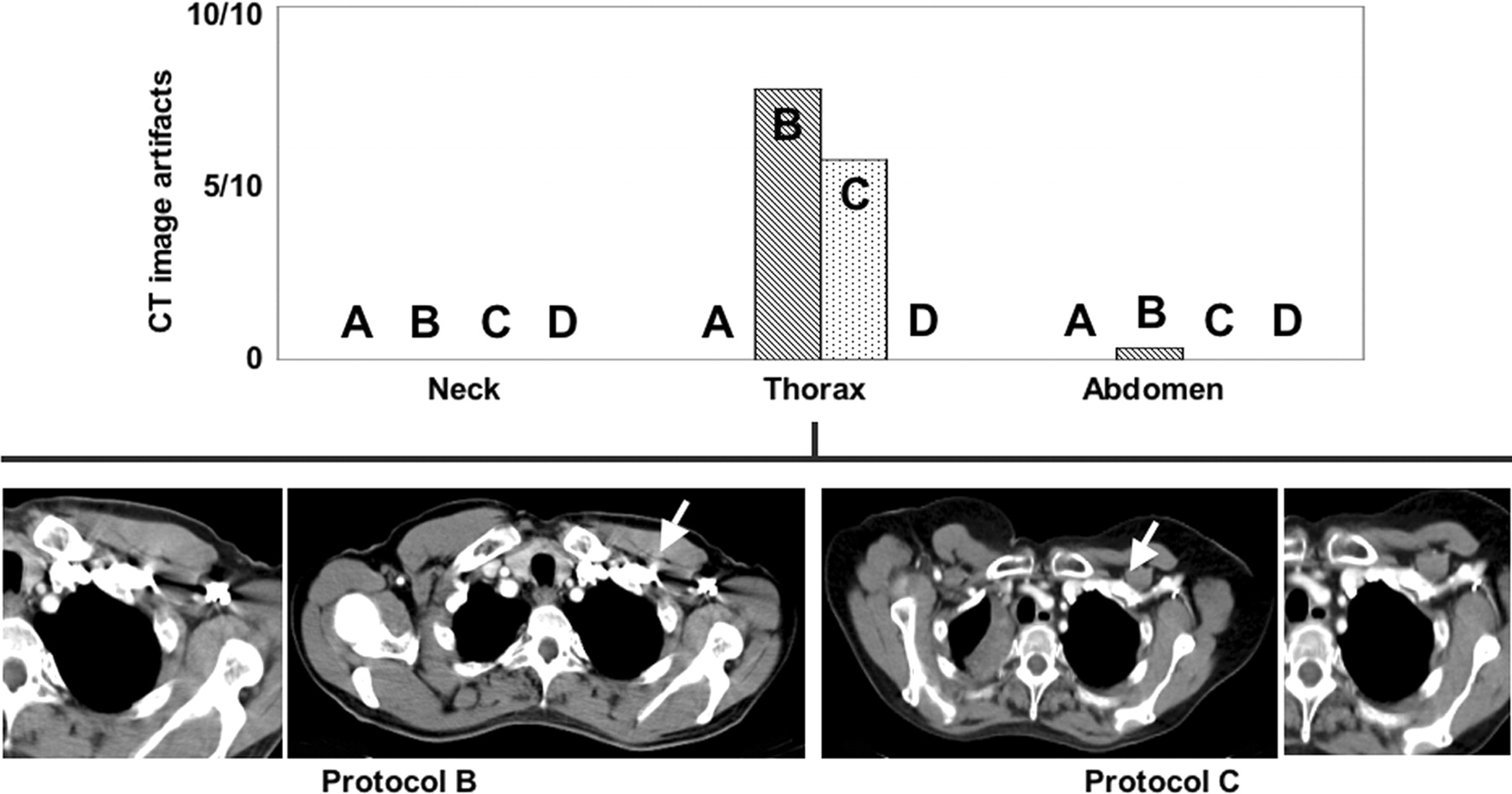
Average number of CT image artifacts attributed to intravenous contrast in neck, thorax, and abdomen. Examples of CT images are shown to illustrate artifacts (arrows) for protocols B and C. Zoomed inserts are shown to the left and right for B and C, respectively. Protocol B also resulted in 1 case with reported high-density artifacts in abdomen as reported by 1 radiology reader (example not shown).
Mean CT attenuation in all vessels of interest was lowest for the nonenhanced protocol A. Protocols B–D produced similar levels of higher vessel enhancement in both the neck and the abdomen (Fig. 4). In the thorax, and more specifically in the BV, the standard and the extended protocols (B and C) yielded exceptionally high CT attenuation values of about 1,300 and 600 Hounsfield units (HU), respectively. Furthermore, we observed a trend toward a larger variability of the contrast enhancement in the thorax (Table 2, BV) for protocols B and C compared with the modified protocol D. Overall, the range of variability of contrast enhancement was largest for the extended protocol C (Table 2).

Average CT attenuation in major vessels of whole-body CT images from PET/CT examinations with contrast administration protocols A–D (Table 1).
Mean CT Attenuation (HU) and SD (%) in Major Vessels of Interest in Neck, Thorax, and Abdomen in Whole-Body PET/CT Studies with Intravenous Contrast Injection According to Administration Protocols A–D
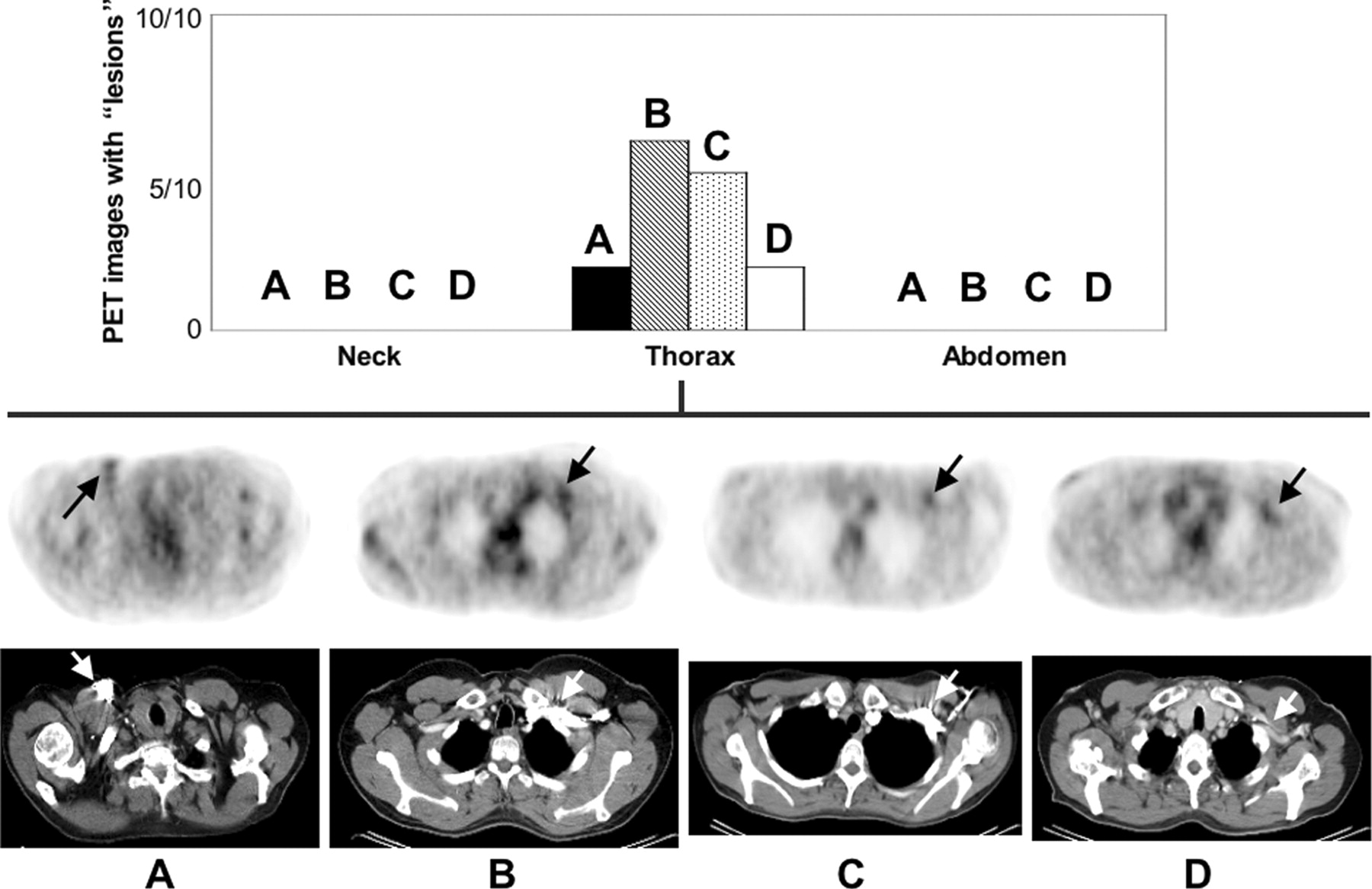
When reviewing the attenuation-corrected PET images without consulting the CT, contrast-induced abnormalities were reported only for the thorax (Fig. 5), but not for the neck or for the abdomen. Protocols A, B, C, and D resulted in focal abnormalities in the corrected PET images of the thorax in 2 of 10, 6 of 10, 5 of 10, and 2 of 10 studies, with average lesion-to-background ratios of 2.0 ± 0.3, 2.1 ± 0.1, 2.3 ± 0.6, and 2.2 ± 0.1, respectively.
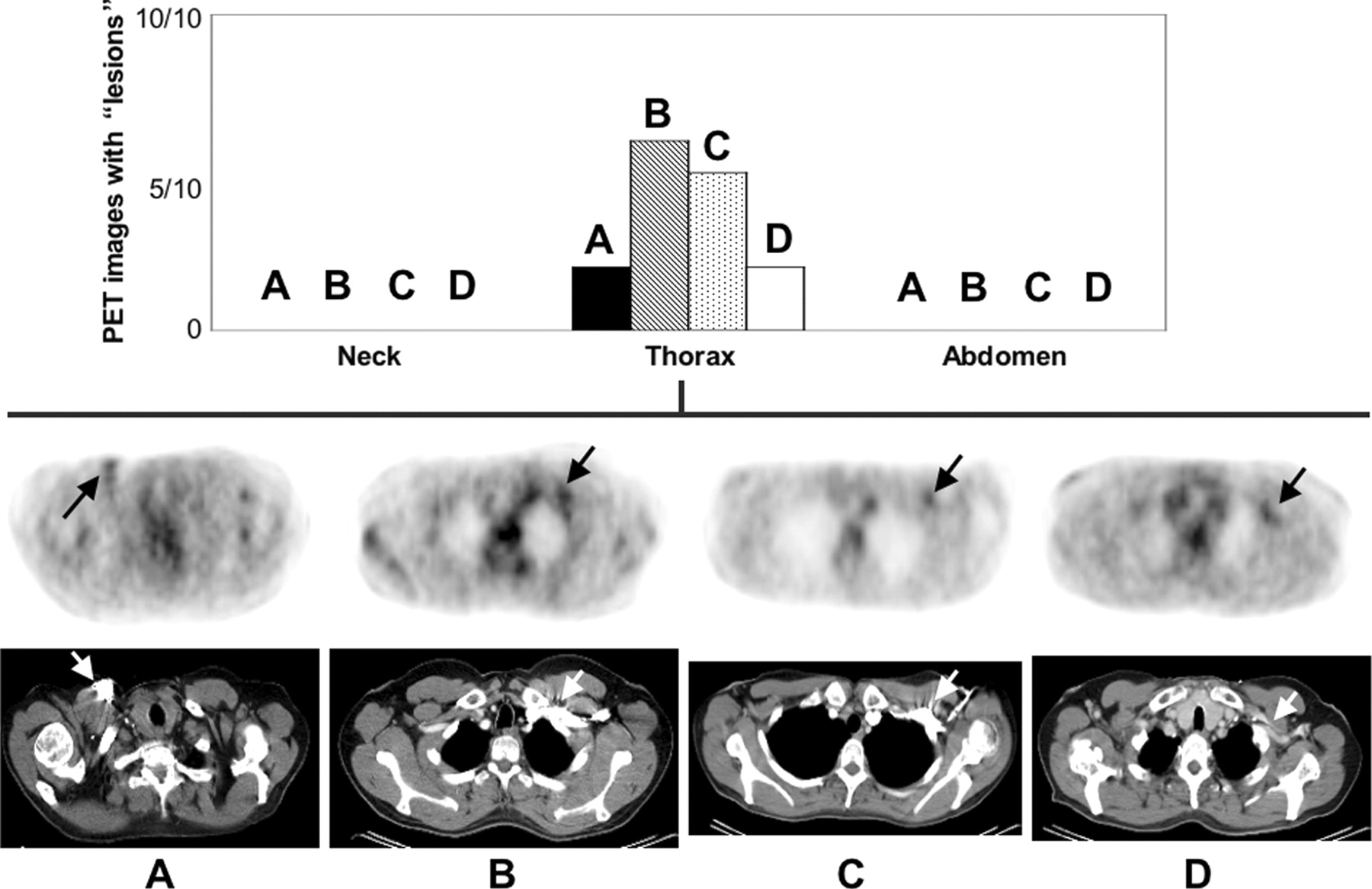
Number of attenuation-corrected PET studies with abnormal tracer uptake attributed to focal accumulations of intravenous contrast through protocols A–D. Axial PET images (after CT-based attenuation correction) through apex of lungs are shown for protocols A–D with arrows pointing to reported artifactual findings on PET.
Upon reviewing the fused PET/CT images, neither the nonenhanced protocol A nor the modified protocol D resulted in correlated artifactual findings on CT and attenuation-corrected PET. In both cases, the artifacts on PET were caused either by metal implants or physiologic uptake. For the standard protocol B, all studies with an intravenous contrast-induced artifact on CT had a correlated artifact on the corresponding PET image, except for 2 studies for which all 3 radiology reviewers reported a CT artifact that had no PET correlate reported. For the extended protocol C, only 3 of the 5 PET studies that were reported to contain contrast-induced image artifacts had correlated reports on CT. In the remaining 2 studies, the corresponding CT images were free of image artifacts with a maximum CT attenuation of only 250 and 170 HU in the BV and the AA, respectively. In the remaining 3 artifactual CT studies from protocol C, the corresponding PET images were free of any apparent contrast-induced artifacts.
DISCUSSION
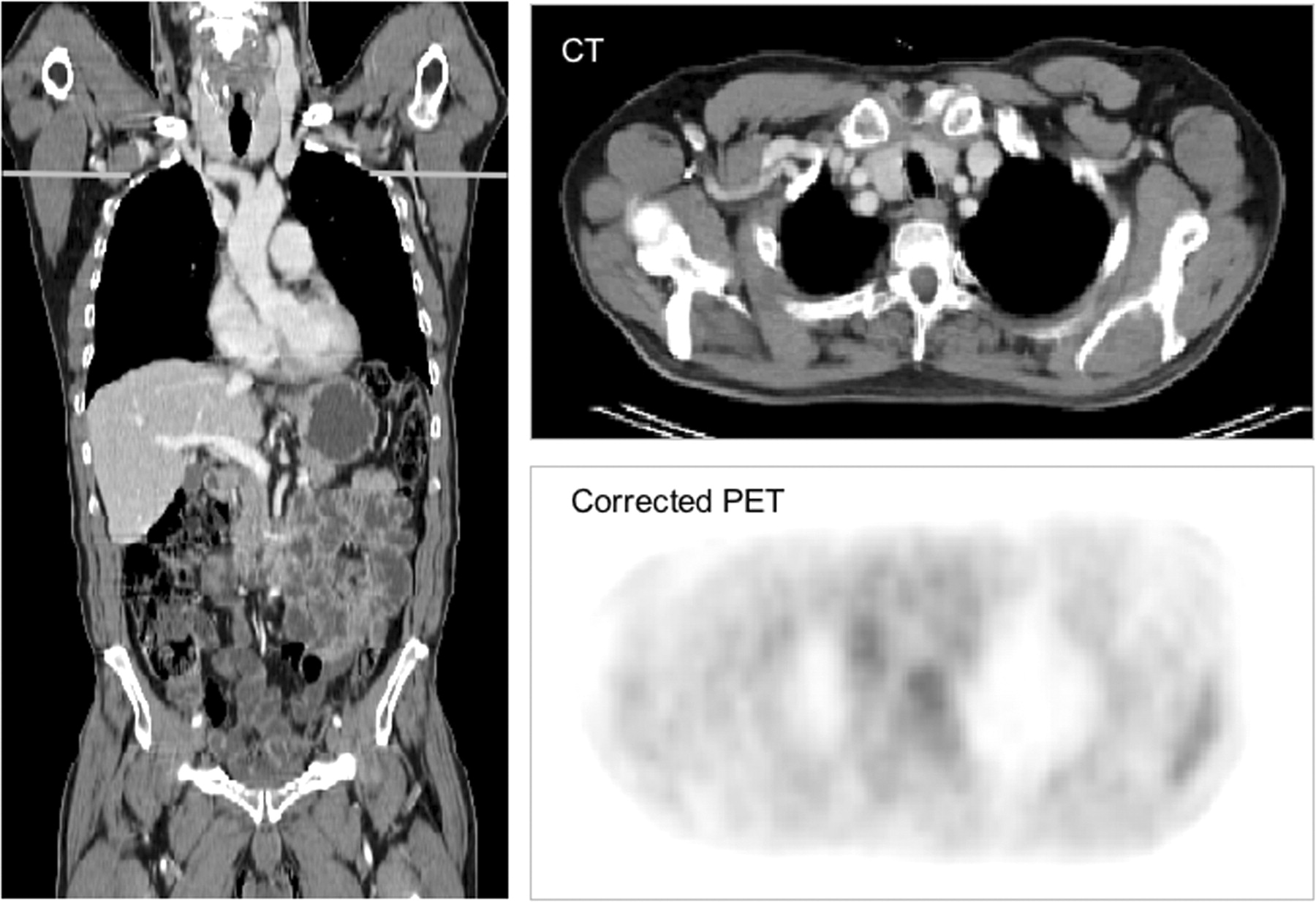
In this study we have defined and compared 4 whole-body 18F-FDG PET/CT protocols with and without intravenous contrast enhancement. Of the 3 intravenous contrast-enhanced protocols, only the modified protocol D yielded reproducible, high-quality whole-body PET/CT images without generating intravenous contrast-related artifacts in either the CT or the PET image volume (Fig. 6). Since the phasing and timing of the contrast injection in protocol D were tailored toward a 2-row CT as part of the combined PET/CT tomograph, our conclusions are limited to PET/CT tomographs with similar CT components. Alternative PET/CT devices using multirow CT and faster CT options may require adjustments of these injection parameters.

18F-FDG PET/CT study following the modified contrast injection protocol D. Coronal CT view illustrates uniform vessel enhancement throughout whole-body imaging range. Axial CT and corrected PET images are shown through area of subclavian vein to demonstrate absence of contrast-induced abnormalities.
Although it was not the main purpose of this study, we further conclude that the application of intravenous contrast improves the overall perception and, subsequently, the diagnostic quality of the CT images compared with nonenhanced CT studies. This point is in agreement with our clinical experiences with contrast-enhanced PET/CT (5,21)—particularly, in the case of absent tracer uptake (21).
All 3 intravenous contrast-enhanced protocols resulted in similar CT image quality of the thorax and abdomen. In protocol B, image quality and enhancement of the neck were limited due to the 30-s delay and the lower flow rate of the second phase of intravenous contrast compared with either protocol C or protocol D. Contrast-induced artifacts on CT were limited to the thorax and generated only by protocols B and C. Likewise, artifactual tracer uptake on the attenuation-corrected PET images was reported for the thorax only.
However, we found a discrepancy in the number of artifactual CT and PET studies. Standard protocol B resulted in correlated reports from CT and PET on contrast-induced artifacts in 6 of 10 studies and 2 additional CT studies without a correlated report from PET. In comparison, the extended protocol C resulted in correlated reports of contrast artifacts in only 3 studies, but with an additional 3 CT studies without a PET artifact. In all cases, where the CT had no correlated artifacts on PET, the maximum attenuation was <1,000 HU and, therefore, below the threshold of CT attenuation given by Antoch et al. to produce false-positive tracer uptake on attenuation-corrected PET images in clinical PET/CT (11).
In all 4 protocols (A–D), several PET studies were considered to be affected by intravenous contrast but did not have correlated reports on CT alone. Upon retrospective review of the fused images, as well as in the absence of intravenous contrast in the nonenhanced protocol A, chemotherapy ports were determined as the cause of the artifactual tracer uptake in 2 PET studies. Chemotherapy ports and other metal implants have been reported to lead to a local overestimation of the attenuation properties and to a false focal tracer uptake on PET if CT is used for attenuation correction (22,23). PET/CT image fusion also helped describe the reported artifacts in the 2 PET studies from protocol C as physiologic uptake with a corresponding maximum CT attenuation of 250 HU, which is below the threshold for generating relevant artifacts (11). Finally, protocol D generated reports on 2 artifactual PET studies without correlated reports on CT alone. On fused PET/CT, artifactual tracer uptake in one case was shown to correspond to brown fat (24). In the other study, PET image artifacts were attributed to bilateral tracer accumulation in the subclavian veins. The veins were likely compressed from keeping the arms above the head for the duration of the combined scan. Since the tracer accumulation was seen also on the noncorrected emission images, we conclude that this study was not affected by intravenous contrast and, therefore, protocol D did not lead to intravenous contrast-induced image distortions.
In our study the assessment of contrast-induced artifacts on PET was different from clinical practice, where PET and CT images of the same dual-modality examination are viewed jointly on a routine basis, and, therefore, misinterpretation of focal uptake patterns on PET as contrast-induced artifacts can be avoided. Conversely, by means of PET/CT image fusion, a focal intravenous contrast enhancement on CT can be correlated with the PET to exclude contrast-induced artificial tracer uptake. It is, of course, advisable to include also the uncorrected emission images in the review process to rule out artifacts from attenuation correction.
The absence of an evaluation of lesion detectability as a function of the different contrast protocols is a limitation of our study, as is the small size of the 4 different protocol groups (A–D), which did not allow for a statistical comparison between them. However, within our study design, protocol D appears favorable for high-quality PET/CT in cases in which PET/CT is ordered instead of separate CT and PET examinations (22).
The advantage of protocol D over the other contrast-enhanced protocols B and C is based on both the absence of contrast-related artifacts on CT and the reproducible high levels of PET image quality after CT-based attenuation correction using the contrast-enhanced CT images. Subsequently, in the case of PET/CT with only a single, contrast-enhanced CT scan, patient exposure is limited by avoiding the acquisition of 2 independent CT scans: one for attenuation correction and one for diagnostic purposes. Furthermore, the chance of patient motion during the combined examination is minimized because additional, postemission CT scans can be avoided. Finally, combined, contrast-enhanced PET/CT could replace separate CT and PET scans without jeopardizing the quality of the image-based diagnosis (22) and, therefore, lead to an overall reduction of patient exposure during the diagnostic work-up, or follow-up.
CONCLUSION
We have assessed PET and CT image quality from whole-body PET/CT acquisitions incorporating different intravenous contrast injection protocols, which were adopted from standard CT practice. We conclude from this study that the well-known CT artifacts in the thoracic veins from unmodified single-bolus injection of intravenous contrast can be avoided in whole-body PET/CT by acquiring the spiral CT data after a dual-phase contrast injection and scanning the coaxial whole-body imaging range in the reverse, caudocranial, direction with a longer delay. For clinical PET/CT scenarios, this intravenous contrast protocol yields reproducible high-quality CT and artifact-free PET images. Nevertheless, contrast administration parameters may need adjusting when CT components differ from those used in this study.
Acknowledgments
We thank Lutz Freudenberg, MD, Thomas Fehlings, MD, and Sandra Rosenbaum, MD, for assisting with evaluation of the data; our technologists Angelika Bildstein, Sandra Pabst, Dorothea Porsch-Plottek, and Bärbel Terschüren as well as Slavko Maric for their cooperation during these studies; and Roman Pink, MD, for helpful discussions.
Footnotes
Received Jul. 28, 2004; revision accepted Oct. 21, 2004.
For correspondence contact: Thomas Beyer, PhD, Department of Nuclear Medicine, University Hospital Essen, Hufelandstrasse 55, D 45122 Essen, Germany.
E-mail: thomas.beyer{at}uni-essen.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantitative Evaluation of Segmentation- and Atlas-Based Attenuation Correction for PET/MR on Pediatric Patients
- Standards for PET Image Acquisition and Quantitative Data Analysis
- Limitations of CT During PET/CT
- FDG-PET/CT in restaging of patients with recurrent breast cancer: possible impact on staging and therapy
- Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging
- Can PET/CT Replace Separate Diagnostic CT for Cancer Imaging? Optimizing CT Protocols for Imaging Cancers of the Chest and Abdomen
- PET/CT in Lymphoma: Prospective Study of Enhanced Full-Dose PET/CT Versus Unenhanced Low-Dose PET/CT
- Reply: Adequate Evaluation of Image Registration in Hybrid PET/CT.
- The Role of PET in Lymphoma
- Optimized Contrast-Enhanced CT Protocols for Diagnostic Whole-Body 18F-FDG PET/CT: Technical Aspects of Single-Phase Versus Multiphase CT Imaging
- Whole-Body 18F-FDG PET/CT in the Presence of Truncation Artifacts
- CT in PET/CT: Essential Features of Interpretation
- Radiation Exposure of Patients Undergoing Whole-Body Dual-Modality 18F-FDG PET/CT Examinations