


Abstract
During the noninvasive assessment of myocardial viability with 18F-FDG metabolic imaging, adequate regulation of metabolic conditions is needed to ensure optimal image quality. The aim of this study was to compare the feasibility and image quality of cardiac 18F-FDG SPECT imaging using acipimox in patients with diabetes and patients without diabetes. Methods: Seventy patients with ischemic cardiomyopathy underwent 18F-FDG SPECT using acipimox for the assessment of myocardial viability, followed by resting 2-dimensional echocardiography to identify dysfunctional myocardial tissue. The image quality was scored visually and quantitatively; the myocardium-to-background ratio was determined by region-of-interest analysis. The plasma concentrations of glucose and free fatty acids were determined to evaluate the metabolic conditions before and during 18F-FDG imaging. Results: Thirty-four patients had diabetes mellitus; of these, 12 had insulin-dependent diabetes mellitus and 22 had non-insulin-dependent diabetes mellitus. The remaining 36 patients had no diabetes. During 18F-FDG SPECT, no severe side effects occurred. Acipimox significantly lowered plasma levels of free fatty acids in both groups. Fifteen of 34 patients with diabetes had a plasma glucose level > 9 mmol/L, which was lowered successfully in all patients with additional insulin. Visual evaluation of the 18F-FDG images showed good, moderate, and poor image quality in 27, 5, and 2 patients, respectively, with diabetes mellitus and in 32, 4, and 0 patients, respectively, without diabetes (P = not statistically significant). The myocardium-to-background ratio of 18F-FDG SPECT images was comparable in patients with and without diabetes mellitus (3.1 ± 1.0 vs. 3.5 ± 0.9, P = not statistically significant). The type of diabetes had no influence on 18F-FDG image quality. Conclusion: 18F-FDG SPECT metabolic imaging after acipimox is safe and practical for routine assessment of viability in patients with ischemic cardiomyopathy. Image quality is good, even in patients with diabetes, although additional insulin is sometimes needed.
Diabetes mellitus is an independent predictor of morbidity and mortality in patients with chronic left ventricular (LV) dysfunction (1,2). Patients with dysfunctional but viable myocardium may considerably benefit from coronary revascularization in terms of functional outcome and survival, but revascularization procedures are associated with a higher morbidity and mortality in patients with diabetes mellitus than in nondiabetic patients (3). Therefore, the assessment of myocardial viability is particularly relevant in these patients, for selection of the appropriate management strategy. Metabolic imaging with 18F FDG is an accepted technique for the assessment of myocardial viability (4–7). However, adequate regulation of metabolic conditions is needed to ensure optimal image quality. Hyperinsulinemic-euglycemic clamping guarantees excellent image quality but is impractical. The use of nicotinic acid derivatives (acipimox; Byk) is a practical alternative that increases patient throughput in busy nuclear cardiology laboratories. Preliminary data suggest that 18F-FDG imaging after acipimox administration is of good quality (8–10). However, the image quality of this protocol in patients with diabetes is unclear and remains to be evaluated. The aim of this study was to compare the feasibility and image quality of cardiac 18F-FDG SPECT imaging using acipimox in patients with diabetes and patients without diabetes. In addition, subsets of patients with insulin-dependent diabetes mellitus (IDDM) and with non-insulin-dependent diabetes mellitus (NIDDM) were studied.
MATERIALS AND METHODS
Patient Population and Study Protocol
The study population consisted of 70 patients with chronic coronary artery disease and a moderately to severely impaired LV function. The patients were prospectively studied according to a structured protocol. This consecutive group of patients was referred for assessment of myocardial viability, and all patients were considered for myocardial revascularization. Thirty-four patients had diabetes mellitus; of these, 12 had IDDM and 22 had NIDDM. All patients with diabetes mellitus were controlling their disease with diet. The remaining 36 patients had no diabetes. Patients with primary cardiomyopathy or concomitant significant valvular disease were not included. All patients were in a clinically stable condition at the time of the study. All patients underwent dual-isotope SPECT with 99mTc tetrofosmin to evaluate perfusion and 18F-FDG imaging to evaluate glucose use, followed by resting 2-dimensional echocardiography to identify dysfunctional myocardial tissue. The precise LV ejection fraction was assessed by radionuclide ventriculography. The local ethics committee approved the protocol, and all patients gave informed consent.
Assessment of Regional Contractile Dysfunction: 2-Dimensional Echocardiography
For echocardiography, a Sonos-5500 imaging system (Hewlett-Packard) was used, equipped with a 1.8-MHz transducer using second-harmonic imaging to optimize endocardial border visualization. Cine loops in 4 standard views were digitized (parasternal long and short axes, apical 2- and 4-chamber views), and 2 experienced reviewers scored the regional contractile function. The left ventricle was divided according to the standard 16-segment model suggested by the American Society of Echocardiography (11). Regional wall motion and systolic wall thickening were scored using a 5-point grading scale: 1 = normal, 2 = mildly hypokinetic, 3 = severely hypokinetic, 4 = akinetic, and 5 = dyskinetic. Segments with severe hypokinesia, akinesia, or dyskinesia were evaluated for myocardial viability.
The LV ejection fraction was assessed by radionuclide ventriculography. A small-field-of-view gamma camera (Orbiter; Siemens) was used, oriented in a 45° left anterior oblique position with a 5°–10° caudal tilt. After injection of 99mTc-pertechnate labeled autologous erythrocytes (550 MBq), radionuclide ventriculography was performed at rest with the patient supine. The LV ejection fraction was calculated by standard methods (Odyssey VP; Picker).
SPECT: Data Acquisition and Analysis
Patients received, after a light breakfast, an intravenous injection of 99mTc-tetrofosmin (600 MBq) to evaluate resting perfusion as described previously (10). Patients with diabetes mellitus were instructed to continue their antidiabetic medication. To determine the plasma concentration of glucose and free fatty acids, venous blood samples ware taken at baseline and once immediately before the 18F-FDG injection. In patients with a plasma glucose level > 9 mmol/L at baseline, 6 units of insulin were administered subcutaneously. When plasma glucose levels remained >9 mmol/L, additional insulin was administered. 18F-FDG imaging, to evaluate myocardial glucose use, was performed after acipimox administration (500 mg, oral dose) in all patients. Acipimox enhances myocardial 18F-FDG uptake by reducing the plasma level of free fatty acids (12–14). After the acipimox administration, the patients received a low-fat, carbohydrate-rich meal. This small meal further enhanced myocardial 18F-FDG uptake by stimulating endogenous insulin release. Sixty minutes after the meal, 18F-FDG (185 MBq) was injected, and after an additional 45 min to allow cardiac 18F-FDG uptake, dual-isotope simultaneous acquisition SPECT was performed. Perfusion and metabolic imaging were performed at rest without stressors.
A triple-head gamma camera (Prism 3000XP; Philips Medical Systems) was used. The camera was equipped with commercially available high-energy 511-keV collimators (15). The energies were centered on the 140-keV photon peak of 99mTc-tetrofosmin with a 15% window and on the 511-keV photon peak of 18F-FDG with a 15% window. Data were acquired over 360° (120 sectors of 3°) with the patients supine. Total imaging time was 32 min. Data were stored in a 64 × 64, 16-bit matrix.
From the raw scintigraphic data, 6-mm-thick (1 pixel) transaxial slices were reconstructed by filtered backprojection using a Butterworth filter (cutoff frequency, 0.17 cycle per pixel; order, 3.5). Attenuation correction was not applied. Further reconstruction yielded standard short- and long-axis projections perpendicular to the heart axis. The 99mTc-tetrofosmin and 18F-FDG data were reconstructed simultaneously, to obtain an exact alignment of the perfusion and metabolic images.
The perfusion and 18F-FDG short-axis slices were plotted in polar maps, which were normalized to maximum activity (set at 100%); the polar maps were divided into 16 segments matching the echocardiographic segments (10,16). The spatial resolution of our system is 1.8 cm in full width at half maximum, as determined with a line source in air. The final spatial resolution also depends on the absorption and scatter in the chest wall. The 18F-FDG SPECT images were scored by 2 experienced observers. The segments were divided into 4 groups, based on the tracer activities: 0 = normal tracer uptake (activity > 75%), 1 = mildly reduced tracer uptake (activity ≤ 75% and > 50%), 2 = moderately reduced tracer uptake (activity ≤ 50% and > 25%), and 3 = severely reduced or absent tracer uptake (activity ≤ 25%). Dysfunctional segments (identified by resting echocardiography) were subsequently evaluated for viability. Segments with normal perfusion (99mTc-tetrofosmin score ≤ 1) and segments with a perfusion defect (score ≥ 2) but relatively increased 18F-FDG uptake (18F-FDG score higher than perfusion score, mismatch pattern) were considered viable. Segments with a perfusion defect and concordantly reduced 18F-FDG uptake (match pattern) were considered nonviable.
Assessment of Image Quality
The image quality was scored visually using a 3-point grading scale: 1 = good (high target-to-background ratio), 2 = moderate but interpretable (moderate target-to-background ratio), and 3 = uninterpretable (poor target-to-background ratio). To quantitatively assess the quality of the 18F-FDG images, the myocardium-to-background (M/B) ratio was measured in the midventricular short-axis plane. A 2 × 2 pixel region of interest was drawn over the myocardium with the highest activity, and a similar region of interest was placed in the center of the LV cavity. From these activities, the M/B ratio was calculated. The measurements were repeated 3 times, and the results were averaged.
Plasma Samples and Analytic Techniques
Venous blood samples were obtained at baseline and immediately before 18F-FDG injection to measure plasma levels of glucose and free fatty acids. Plasma glucose was determined with an analyzer using the glucose oxidase method (YSI). The free fatty acid levels were assessed by enzymatic colorimetric methods (NEFAC; Wako Chemicals).
Statistical Analysis
All continuous data are expressed as mean ± SD; percentages are rounded. Continuous variables were compared using the Student t test. Differences between proportions were compared using the χ2 test. A value of P < 0.05 was considered statistically significant.
RESULTS
Patient Characteristics and Plasma Substrate Levels
Clinical characteristics were comparable between the group of patients with diabetes mellitus and the group without diabetes mellitus (Table 1). All patients presented with symptoms of heart failure and had severely impaired LV function due to chronic coronary artery disease.
Clinical Characteristics of the 70 Study Patients
Glucose.
Figure 1 demonstrates the plasma glucose levels measured at baseline and immediately before 18F-FDG injection. At baseline, the patients with diabetes had higher plasma glucose levels than did the patients without diabetes. After subcutaneous administration of insulin, glucose levels decreased significantly in patients with diabetes mellitus (Fig. 1). Fifteen of 34 patients with diabetes (7 IDDM, 8 NIDDM) had a plasma glucose level > 9 mmol/L, which was lowered successfully in all patients with additional insulin. Still, 4 patients had a plasma glucose level > 9 mmol/L.

Bar graft demonstrates plasma glucose levels measured at baseline (white bars) and immediately before 18F-FDG injection (black bars). *P < 0.0001 vs. no diabetes. **P < 0.005 vs. no diabetes. †P < 0.001 vs. immediately before 18F-FDG injection. Values are expressed as mean ± SD.
Free Fatty Acids.
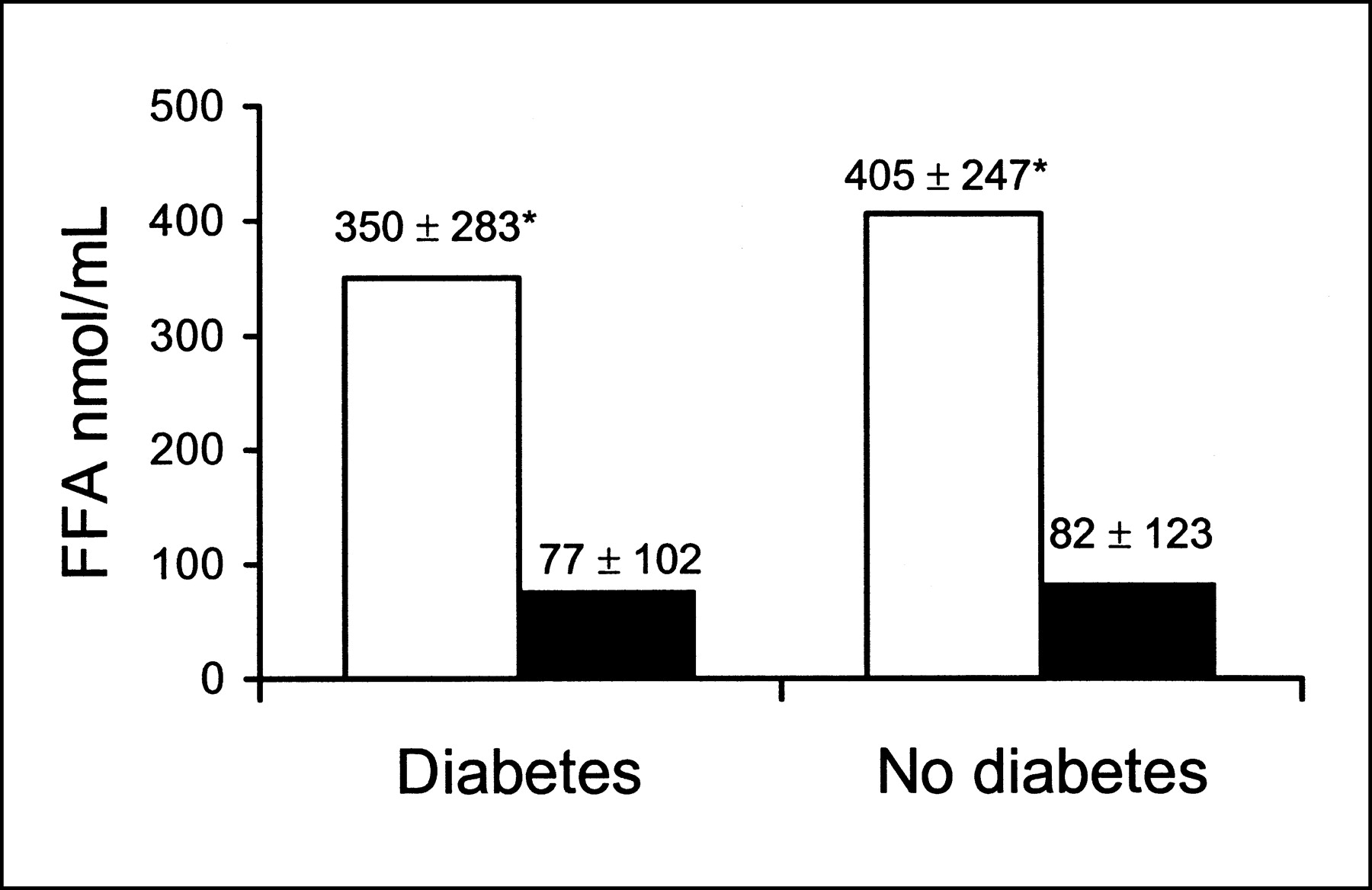
At baseline, the patients with diabetes had plasma levels of free fatty acids similar to those of the nondiabetic patients; at the time of 18F-FDG injection, plasma levels of free fatty acids had declined significantly in both groups (Fig. 2).

Plasma concentration of free fatty acids (FFA) in patients with diabetes mellitus and those without diabetes, at baseline (white bars) and after oral administration of acipimox (black bars). *P < 0.0001 vs. after acipimox.
Safety and 18F-FDG SPECT Image Quality Using Acipimox
No serious side effects (evaluated by direct questioning and physical examination) occurred during 18F-FDG SPECT imaging. Nineteen patients had a mild and transient skin flush after acipimox administration. Mild skin flushing occurred in 5 of 34 (15%) patients with diabetes and in 14 of 36 (39%) patients without diabetes (P < 0.05).
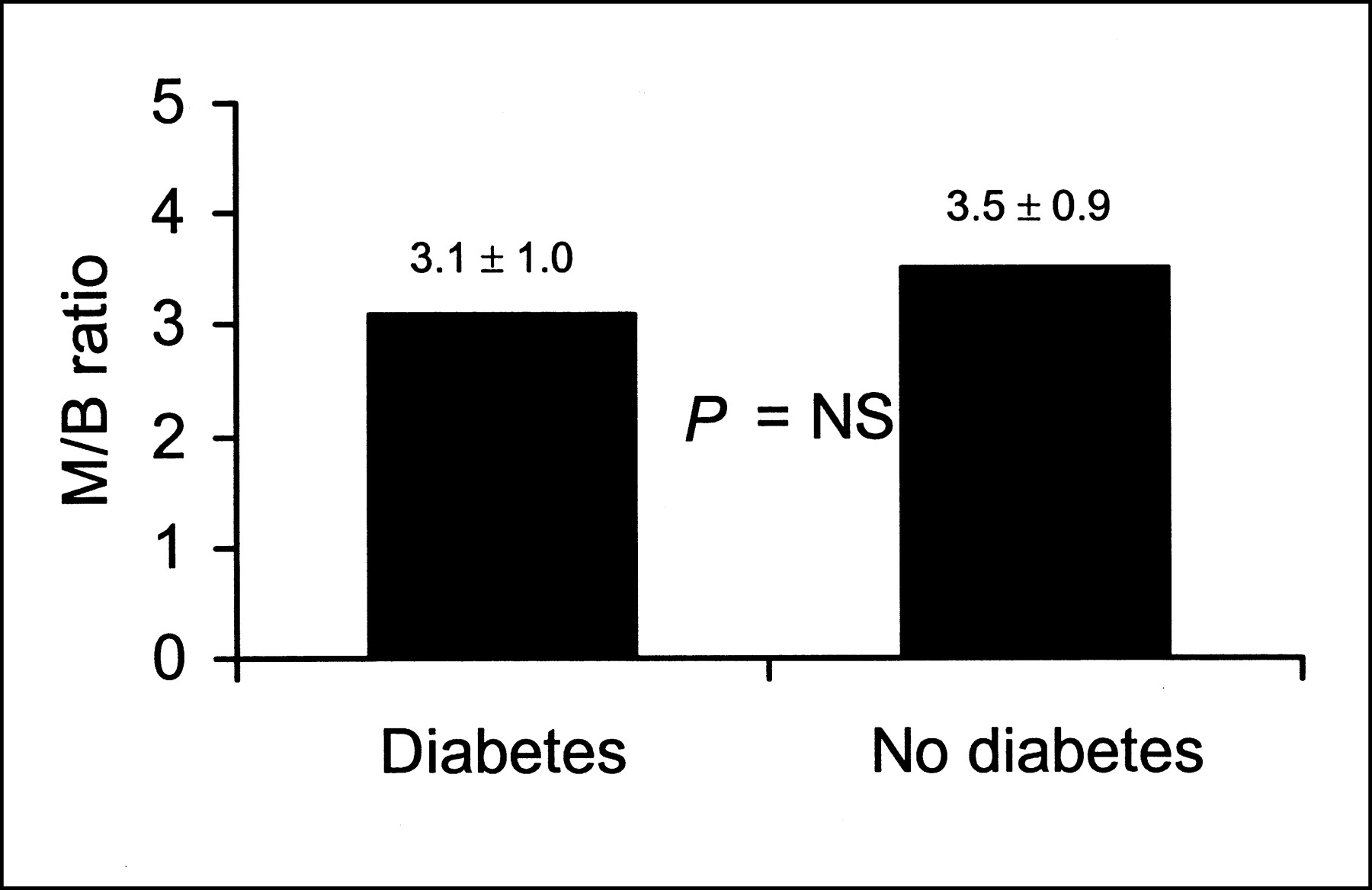
Visual evaluation of the 18F-FDG images showed good, moderate, and poor image quality in 27, 5, and 2 patients with diabetes mellitus, respectively, and in 32, 4, and 0 patients without diabetes, respectively (not statistically significant). In the patients with 18F-FDG SPECT images of moderate or poor quality, the fasting blood glucose was, on average, 9.1 ± 4.8 mmol/L, free fatty acid levels were 404 ± 277 nmol/mL at baseline and 77 ± 49 nmol/mL after acipimox, and the ejection fraction was 35% ± 12%. The M/B ratio of 18F-FDG SPECT images was comparable in patients with and without diabetes mellitus (Fig. 3). Examples of the image quality obtained with 18F-FDG SPECT after oral administration of acipimox are presented in Figure 4.
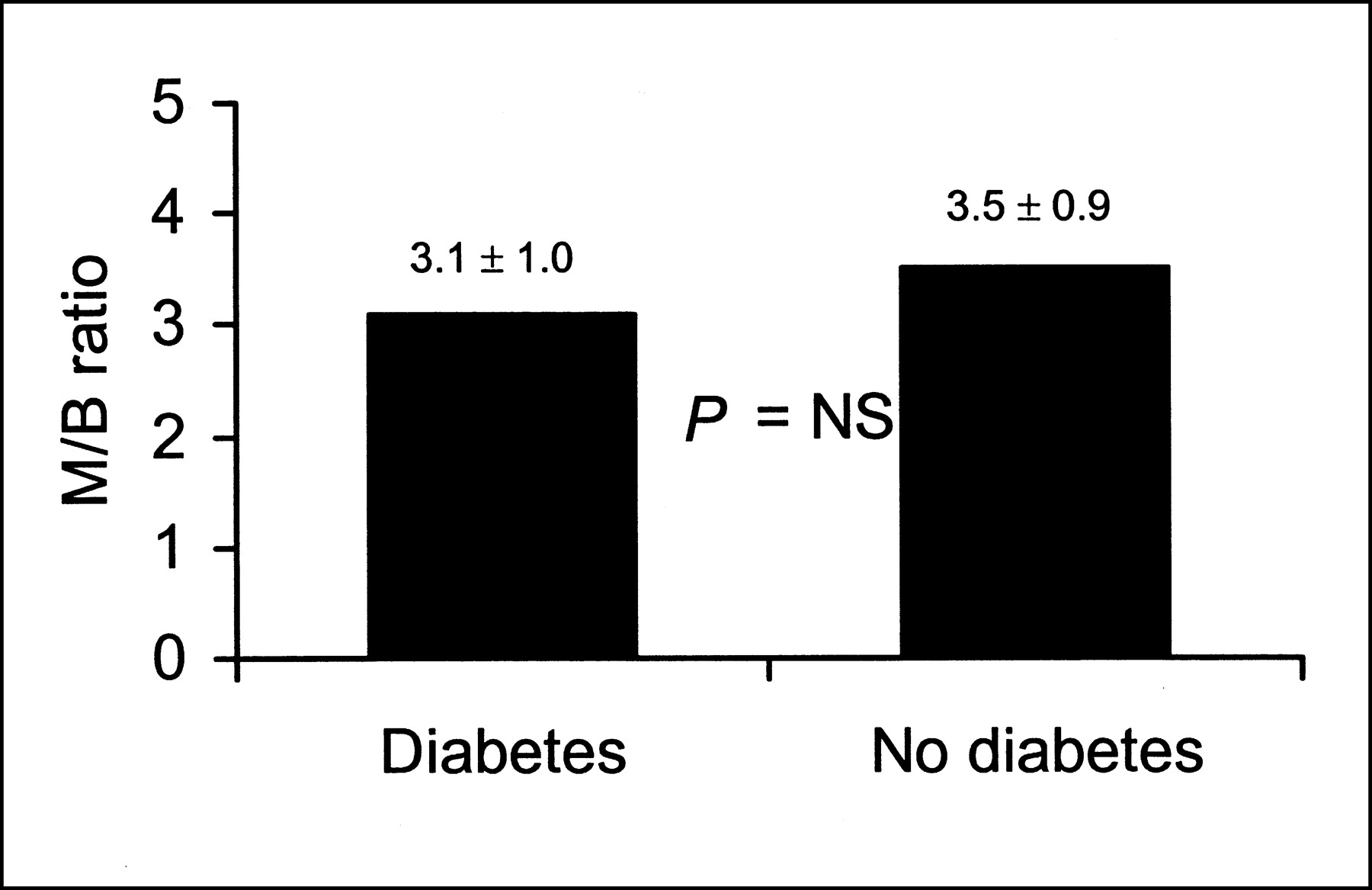
Quality of 18F-FDG SPECT images (M/B ratio) was comparable in patients with and without diabetes mellitus.
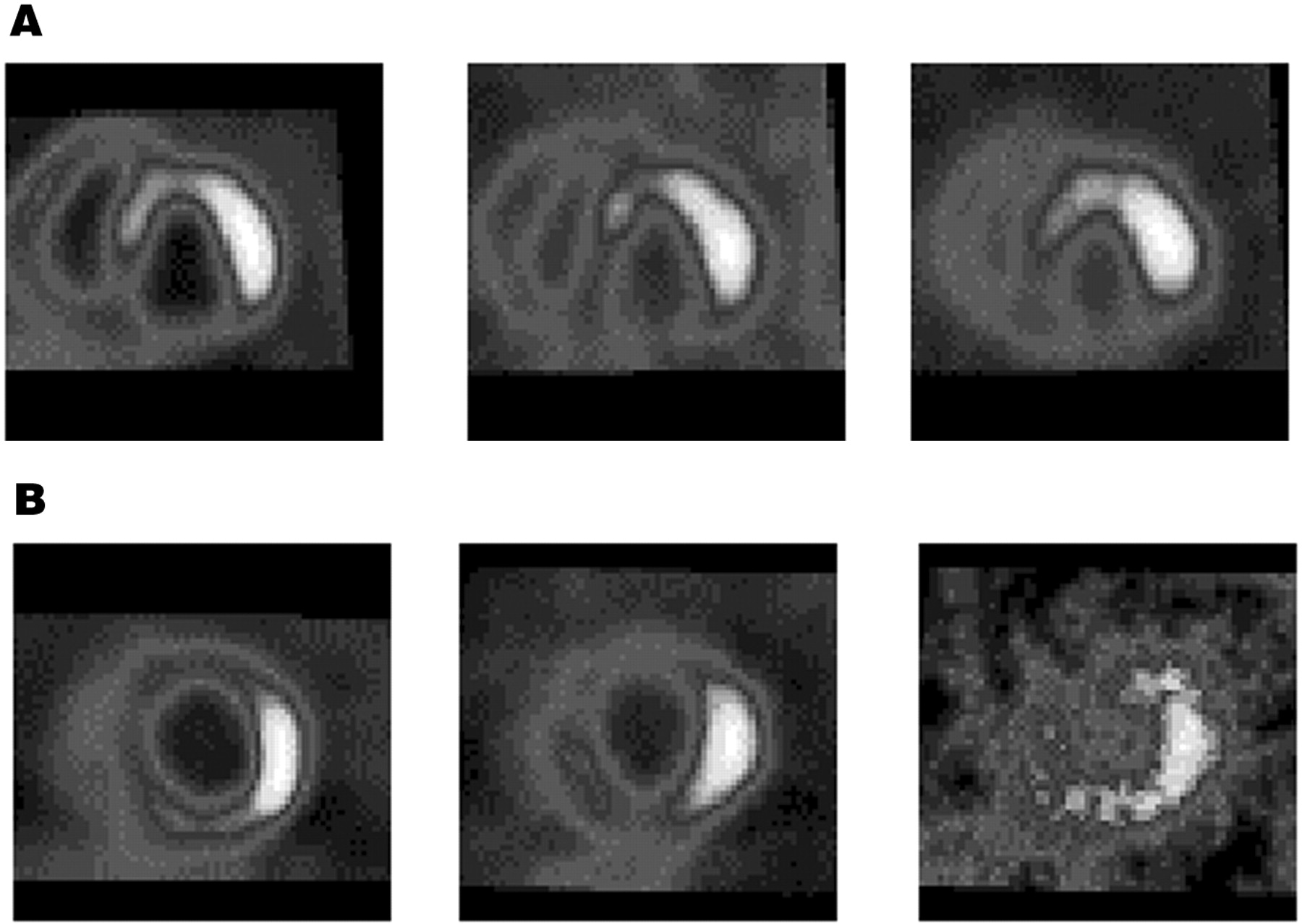
Examples of image quality obtained with 18F-FDG SPECT after oral administration of acipimox. (A) Baseline 99mTc-tetrofosmin (left), dual-isotope simultaneous acquisition (DISA) 99mTc-tetrofosmin (middle), and DISA 18F-FDG (right) short-axis images of patient with NIDDM. All images are of good quality; this patient had M/B ratio of 4.2. (B) Baseline 99mTc-tetrofosmin (left), DISA 99mTc-tetrofosmin (middle), and DISA 18F-FDG (right) short-axis images of patient with IDDM. 18F-FDG images are of poor quality. This patient had M/B ratio of 2.1.
Myocardial Viability
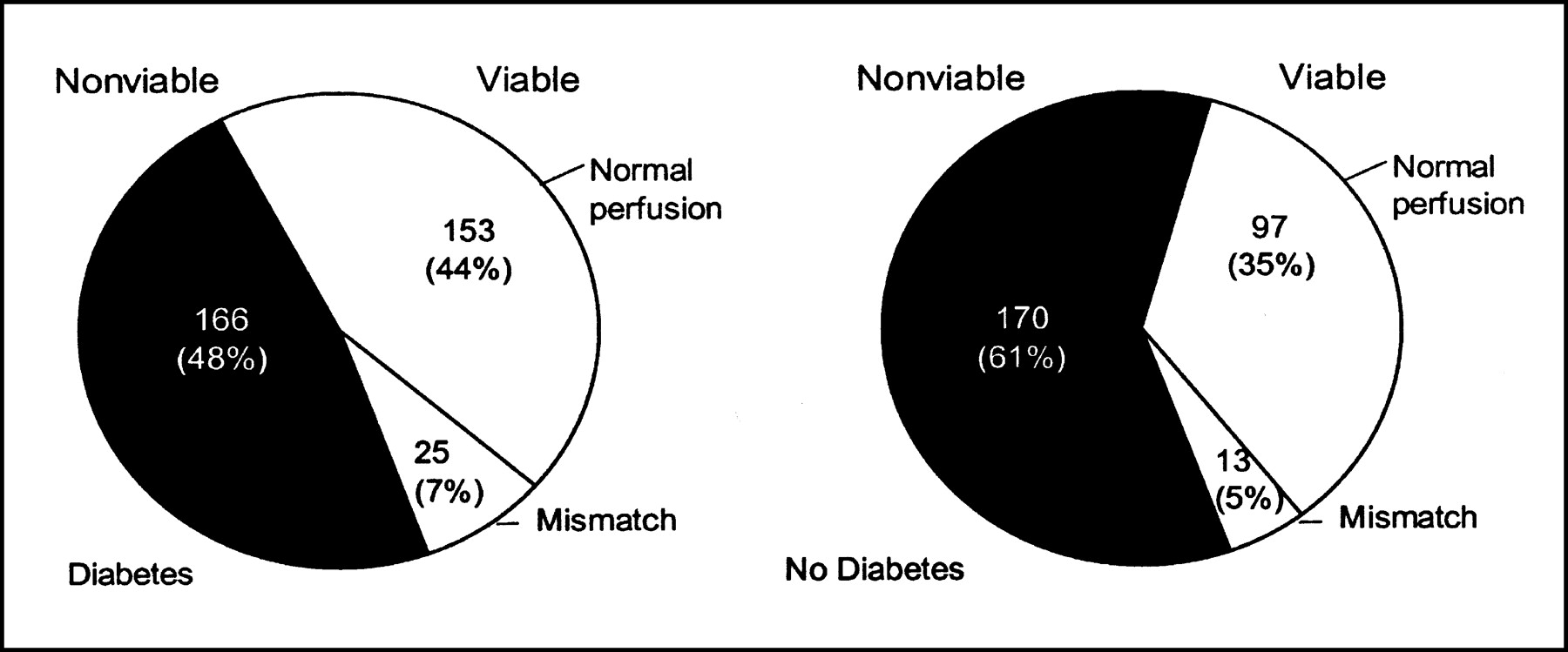
Figure 5 shows the number of viable and nonviable dysfunctional myocardial segments as assessed by 18F-FDG SPECT in patients with and without diabetes mellitus. The 2 patients with poor 18F-FDG image quality were excluded from the analysis of myocardial viability. The number of dysfunctional segments was comparable in patients with and without diabetes mellitus (10.2 ± 5.4 vs. 8.3 ± 4.1, not statistically significant). According to metabolic imaging with 18F-FDG SPECT, patients with diabetes had more dysfunctional but viable myocardial tissue than did patients without diabetes. Patients with diabetes had, on average, 5.3 ± 4.4 dysfunctional but viable segments, whereas those without diabetes had 3.3 ± 3.3 viable segments (P < 0.05).
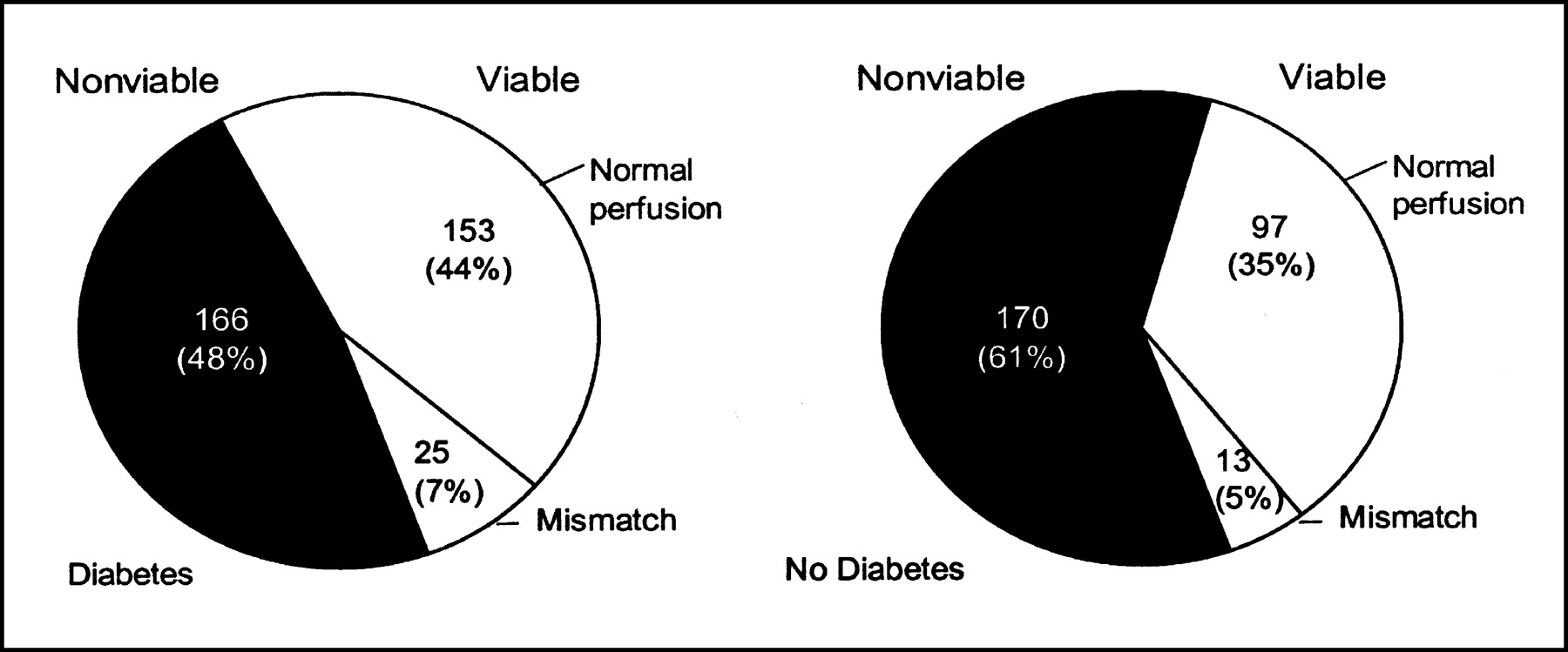
Number of viable (normal perfusion or blood-flow-metabolism mismatch) and nonviable dysfunctional myocardial segments as assessed by 18F-FDG SPECT in patients with and without diabetes mellitus.
Results in Patients with NIDDM versus IDDM
Patients with IDDM had clinical characteristics similar to those of patients with NIDDM (Table 2). Glucose levels were comparable in patients with IDDM and NIDDM (10.1 ± 4.8 mmol/L vs. 7.6 ± 2.6 mmol/L at baseline, P = 0.06, and 8.6 ± 3.2 mmol/L vs. 7.8 ± 3.0 mmol/L at the time of 18F-FDG injection, P = 0.49). At baseline, free fatty acid levels were comparable in patients with IDDM and NIDDM (242 ± 189 nmol/mL vs. 404 ± 305 nmol/mL, P = 0.13). However, after the administration of acipimox, at the time of 18F-FDG injection, free fatty acid levels were lower in patients with IDDM than in those with NIDDM (27 ± 17 nmol/mL vs. 102 ± 116 nmol/mL, P < 0.05). Region-of-interest analysis demonstrated that the type of diabetes (IDDM vs. NIDDM) had no influence on 18F-FDG image quality (Fig. 6). Also, patients with IDDM and NIDDM had a comparable number of dysfunctional segments (10.4 ± 5.8 vs. 10.1 ± 5.1, P = 0.81). Patients with IDDM and NIDDM had a comparable number of dysfunctional but viable segments (6.5 ± 4.8 vs. 4.6 ± 3.9, P = 0.37).
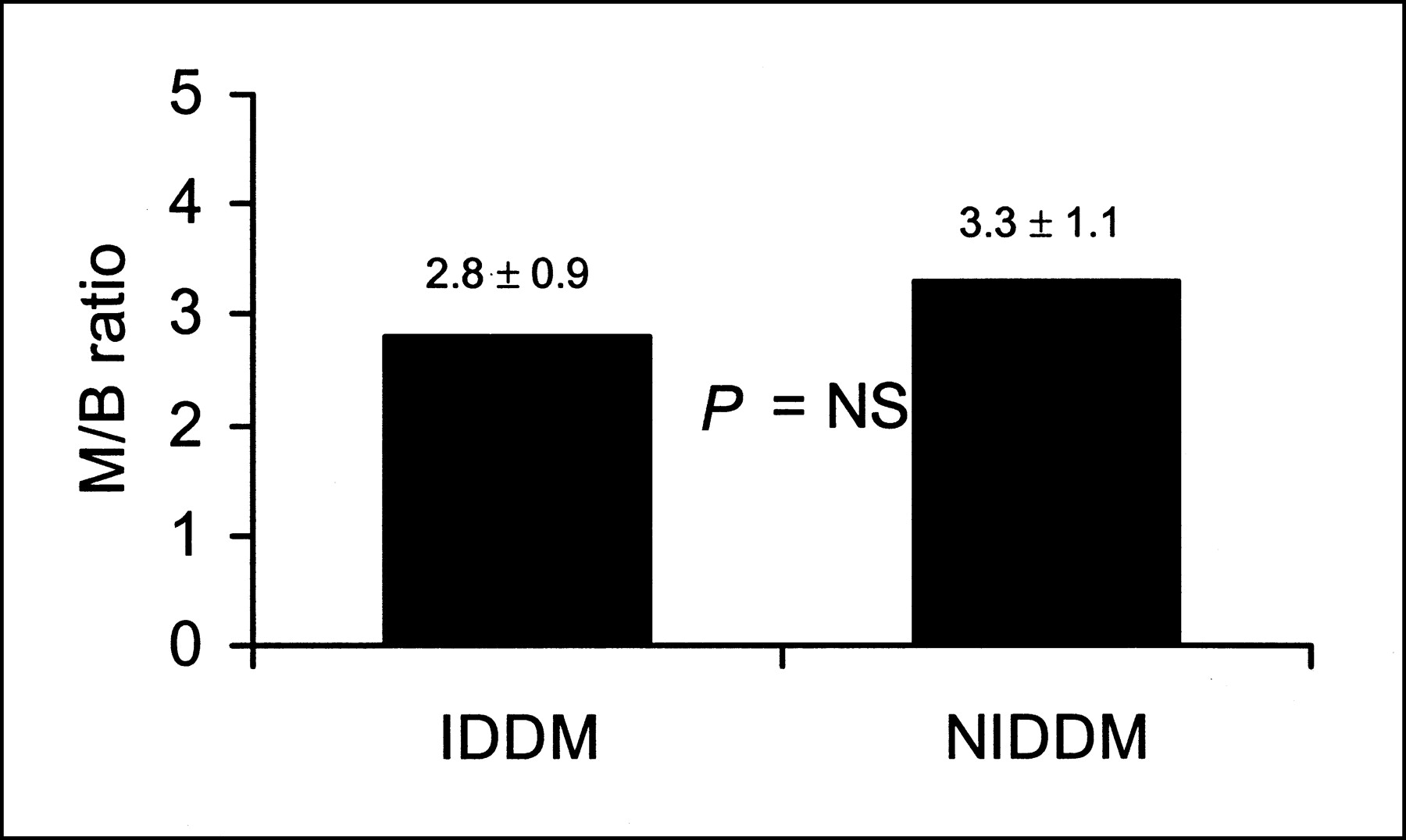
Region-of-interest analysis demonstrated that type of diabetes, IDDM vs. NIDDM, had no influence on 18F-FDG image quality. NS = not statistically significant.
Clinical Characteristics of the 34 Patients with Diabetes Mellitus
DISCUSSION
Noninvasive assessment of myocardial viability in patients with ischemic cardiomyopathy has major implications for clinical decision making. When a substantial amount of dysfunctional but viable myocardium is present, coronary revascularization may improve LV function and long-term survival. Currently, both the number of patients with heart failure due to coronary artery disease and the prevalence of diabetes mellitus are increasing rapidly (17,18). Diabetes mellitus is a well-known risk factor for coronary artery disease. Patients with diabetes have a 4-fold increased risk for development of heart failure after myocardial infarction (19). The assessment of myocardial viability is particularly relevant in these patients, since coronary revascularization in patients with diabetes mellitus is associated with a high morbidity and mortality (3). Currently, 18F-FDG PET is considered the gold standard for the assessment of myocardial viability (4–7). Recently, 18F-FDG metabolic imaging has become widely available with the introduction of 18F-FDG SPECT using dedicated collimators (20–25). The image quality of 18F-FDG imaging is influenced by metabolic conditions (8,9). Several protocols were introduced to lower free fatty acid levels, which appear the main determinant of image quality during 18F-FDG imaging (8). 18F-FDG imaging after oral glucose loading is practical, but the image quality varies substantially, with 20%–30% of the images being uninterpretable (particularly in patients with diabetes). The hyperinsulinemic-euglycemic clamp ensures excellent image quality but is labor intensive and time consuming. Recently, 18F-FDG SPECT after oral administration of nicotinic acid derivatives (acipimox) has been suggested as a clinically useful protocol that increases patient throughput in busy nuclear cardiology laboratories (8,9). Acipimox is a nicotinic acid derivative that inhibits lipolysis and decreases plasma concentrations of free fatty acids (12–14). Two preliminary studies showed that 18F-FDG imaging using acipimox was of good quality (8,9). However, the image quality with this protocol in patients with diabetes is unclear; this patient subset is the most challenging for obtaining good image quality.
The present study assessed the feasibility and image quality of 18F-FDG SPECT after oral administration of acipimox for the assessment of myocardial viability in patients with diabetes mellitus. Metabolic conditions (plasma substrate levels) were monitored. As anticipated, baseline glucose levels were higher in patients with diabetes. In patients with plasma glucose levels > 9 mmol/L, additional insulin was added. An oral dose of acipimox effectively lowered the free fatty acid concentrations in both patient groups. No serious side effects of acipimox were observed. The image quality was comparable in patients with and without diabetes mellitus, and the type of diabetes mellitus (IDDM or NIDDM) did not influence 18F-FDG image quality. These findings demonstrate that 18F-FDG SPECT after oral administration of acipimox is a safe and clinically useful method for the assessment of myocardial viability and offers good image quality, even in patients with diabetes mellitus.
Acipimox is currently not available in the United States. Recently, Vitale et al. (26) studied 10 patients with ischemic LV dysfunction and NIDDM using 18F-FDG PET. In that study, 18F-FDG imaging was performed after administration of niacin (a nicotinic acid), yielding suboptimal results. However, nicotinic acid derivatives (e.g., acipimox), are known to be 20 times as potent as nicotinic acids, which may explain the lesser results in the study by Vitale et al. using niacin (12,26).
Of interest, patients with diabetes had more dysfunctional but viable myocardial tissue than did patients without diabetes. This observation is in line with our previous work (27). The reason for this finding is unclear. Further studies including follow-up data on functional recovery (the final proof of myocardial viability) are needed to elucidate this issue.
Some limitations of the present study need to be addressed. First, although the same 16-segment model was used for analysis, some misalignment between echocardiograms and SPECT images may have occurred. Second, the findings in our study did not include the results of recovery of function after revascularization. Previous studies by Altehoefer et al. (28) and by Zanco et al. (29) demonstrated that in patients with left bundle branch block, regional 18F-FDG uptake in the septum may be affected without a correlating change in perfusion. This is a limitation of 18F-FDG imaging that should be considered in the evaluation of myocardial viability.
CONCLUSION
18F-FDG SPECT metabolic imaging after acipimox is safe and practical for routine assessment of viability in patients with ischemic cardiomyopathy. Image quality is good, even in patients with diabetes, although additional insulin is sometimes needed.
Footnotes
Received Oct. 2, 2002; revision accepted Jan. 21, 2003.
For correspondence or reprints contact: Don Poldermans, MD, PhD, Thoraxcenter Room Ba 300, Department of Cardiology, Erasmus Medical Center, Dr. Molewaterplein 40, 3015 GD Rotterdam, The Netherlands.
E-mail: poldermans{at}hlkd.azr.nl
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Extent of Viability to Predict Response to Cardiac Resynchronization Therapy in Ischemic Heart Failure Patients
- Nitrate Administration Increases Blood Flow in Dysfunctional but Viable Myocardium, Leading to Improved Assessment of Myocardial Viability: A PET Study
- Effect of Intramyocardial Injection of Autologous Bone Marrow-Derived Mononuclear Cells on Perfusion, Function, and Viability in Patients with Drug-Refractory Chronic Ischemia
- Impact of Diabetes Mellitus on Prediction of Clinical Outcome After Coronary Revascularization by 18F-FDG SPECT in Patients with Ischemic Left Ventricular Dysfunction
- Diabetic cardiomyopathy: mechanisms, diagnosis and treatment
- Reduced Oxidative Metabolic Response in Dysfunctional Myocardium with Preserved Glucose Metabolism but with Impaired Contractile Reserve