


Abstract
The recovery of function in myocardium defined as viable by 18F-FDG PET may differ from that defined by dobutamine stress echocardiography (DSE). The aim of this study was to investigate the difference in the oxidative metabolic response between myocardial segments with preserved contractile reserve (CR) and those without CR, in segments with and without preserved glucose metabolism (GM), using 11C-acetate PET. Methods: Twenty patients with previous myocardial infarction (left ventricular ejection fraction, 37.1% ± 16.5%) underwent dynamic 11C-acetate PET at rest and during dobutamine (7.5 μg/kg/min) infusion. GM was evaluated using 18F-FDG PET and CR was evaluated using DSE. Dysfunctional segments were divided into 3 groups: group A (n = 26) with preserved CR and GM, group B (n = 15) without CR but with preserved GM, and group C (n = 41) without CR and without preserved GM. Results: Resting oxidative metabolism (k mono = monoexponential clearance rate) was preserved in group A and group B (0.052 ± 0.011/min vs. 0.051 ± 0.012/min, P = not significant) but was reduced in group C (0.040 ± 0.015/min) (P < 0.03 vs. group A and group B). The change in k mono, as a measure of the metabolic response to low-dose dobutamine, was significantly higher in group A (0.018 ± 0.012) than that in group B (0.0075 ± 0.0096, P < 0.03) and group C (0.0080 ± 0.012, P < 0.005). Conclusion: Viable segments based on 18F-FDG PET have preserved resting oxidative metabolism. However, segments without CR but with preserved GM show a reduction in the oxidative metabolic response to low-dose dobutamine infusion. The decrease in CR may be related to the reduction in the metabolic response to inotropic stimulation despite preservation of tissue viability on 18F-FDG PET.
Several techniques have been developed to identify dysfunctional but viable myocardium (1–8). 18F-FDG PET and dobutamine stress echocardiography (DSE) are considered accurate noninvasive methods for identifying dysfunctional but viable myocardium (9). However, the clinical outcome is somewhat different for patients based on 18F-FDG PET and DSE (10,11). Compared with 18F-FDG PET, DSE has a lower sensitivity but a higher specificity in identifying and predicting improvement in regional left ventricular function after revascularization therapy (9). Therefore, myocardial viability may be overestimated by 18F-FDG PET, whereas it may be underestimated by DSE.
The improvement in wall motion for dysfunctional but viable myocardium is accompanied by increased regional blood flow and oxidative metabolism. The kinetics of 11C-acetate, determined from dynamic PET, can be used to noninvasively measure myocardial oxidative metabolism (12–15).
Resting oxidative metabolism is preserved in segments with viable myocardium (13,15). Myocardial oxidative metabolism is also increased during dobutamine infusion in segments with viable myocardium (15,16). However, the pathophysiologic differences with respect to oxidative metabolism and the metabolic response to dobutamine infusion in these segments have not been well studied.
The aim of this study was to investigate the differences in the oxidative metabolic response in myocardium with and without preserved contractile reserve (CR) and in myocardium with and without preserved glucose metabolism (GM) using 11C-acetate PET.
MATERIALS AND METHODS
Study Population
Twenty sequential patients with old myocardial infarction were prospectively studied between May 2000 and April 2001. There were 17 men and 3 women with a mean age ± SD of 63.0 ± 8.8 y. These patients met the following criteria: (a) the presence of a Q wave infarction caused by total or subtotal occlusion of a coronary artery; (b) the presence of severe segmental dysfunction (severe hypokinesis, akinesis, or dyskinesis) on resting echocardiography; (c) the absence of unstable angina or acute myocardial infarction within the preceding 4 wk; (d) the absence of concomitant cardiopulmonary disease, severe valvular disease, or left ventricular aneurysm. Two patients (10%) were excluded from the final evaluation: 1 patient with inadequate 18F-FDG uptake due to severe diabetes, and 1 patient who did not reach the study protocol dose of 7.5 μg/kg/min dobutamine due to angina. Table 1 summarizes the clinical characteristics of the 18 patients with complete data. The mean left ventricular ejection fraction (LVEF) was 37.1% ± 16.5%. β-Adrenergic blocking agents were withdrawn at least 48 h before both the 11C-acetate PET and the DSE studies. Other cardiac medications were not withheld before dobutamine stress studies to avoid myocardial ischemia. In the dysfunctional segments defined on the routine echocardiography, GM was evaluated using 18F-FDG PET and CR was evaluated using DSE. All patients underwent 11C-acetate PET, 18F-FDG PET, and DSE within a period of 1 wk. 18F-FDG PET was performed on the first day and DSE was performed on the third or fifth day. 11C-Acetate PET was performed on the seventh day. The study was approved by the Ethics Committee of Hokkaido University Hospital. Written informed consent was obtained from each patient.
Clinical Characteristics of 18 Study Patients
Dobutamine Stress Test
Dobutamine was administered intravenously at a starting dose of 5 μg/kg/min for 3 min. It was then increased to a dose of 7.5 μg/kg/min as described previously (15,17). When the heart rate and blood pressure stabilized with a fluctuation of <5%, a second 11C-acetate PET dynamic scan or echocardiogram was obtained. During dobutamine infusion, the 12-lead electrocardiogram and blood pressure results were recorded every minute.
11C-Acetate PET Protocol
1-11C-Acetate was synthesized according to the methods of Pike et al. (18).
For the resting study, the patients were studied after a 5-h fast. PET was performed using a whole-body scanner (ECAT/EXACT HR+; Siemens/CTI). Transmission images were obtained using an external ring of 68Ga to enable correction of the emission images for photon attenuation.
After the 20-min transmission scan, 370 MBq (10 mCi) of 11C-acetate were administered intravenously, and a dynamic PET acquisition was initiated (6 × 10, 4 × 15, 18 × 60 s) (15,17). Four hours after the resting study, a second dynamic scan under dobutamine infusion was performed.
18F-FDG PET Acquisition
The 18F-FDG PET studies were scheduled for the morning after an overnight fast. Images were corrected for attenuation using coefficients determined by a 20-min transmission scan. Sixty minutes after the start of the hyperinsulinemic–euglycemic clamp, 555 MBq (15 mCi) of 18F-FDG were injected. Forty minutes later, exogenous myocardial glucose utilization was determined from a 20-min static scan.
PET Data Analysis
Data analysis of the PET images was accomplished using an image analysis package (Dr. View; Asahi-Kasei) and special dedicated software. The images were iteratively reconstructed and resliced along the short axis (19). Regions of interest were defined for each of these images. The left ventricle was divided according to the 16-segment model recommended by the American Society of Echocardiography (20). These segments included the anterior, anteroseptal, septal, inferior, posterior, and lateral walls, each subdivided into the basal and midventricular portions, and the apical anterior, apical septum, apical inferior, and apical lateral regions. The same anatomic landmark (the insertion of the right ventricle into the interventricular septum) was used in all studies to optimize the image coregistration for the regions of interest in each study (11C-acetate PET, 18F-FDG PET, and DSE) (21).
Regional Oxidative Metabolism
Regional oxidative metabolism was determined from the monoexponential function (k mono) fit to the linear portion of the semilogarithmic plot. The start of the curve was visually defined corresponding to when the blood-pool activity had cleared (usually 3–5 min) as previously described (22). The curve fitting was automated (17,22,23). The oxidative metabolic reserve was defined by change in the k mono with stress as follows: k mono during dobutamine infusion minus the k mono at baseline (15,16).
Regional Myocardial Perfusion
Regional myocardial perfusion was based on the early myocardial uptake of 11C-acetate (14,24). The regional tracer distribution in the myocardium, 60–180 s after the administration of 11C-acetate, has been shown to reflect regional perfusion in relative terms (24). Segments with reduced perfusion were defined as relative tracer uptake < 50% of the maximum uptake (1,25).
Quantitative Assessment of Segmental 18F-FDG Uptake
Quantitative assessment of segmental 18F-FDG uptake was performed as previously described (6). Preserved GM for a given segment was defined when the mean segmental 18F-FDG uptake was ≥50% of the maximal myocardial uptake taken from a region with normal wall motion (6).
DSE
Ventricular function was assessed by 2-dimensional echocardiography using a Sonos 5500 ultrasound system (Phillips Medical Systems) equipped with a 2- to 4-MHz transducer. Echocardiography was performed under resting conditions and during the last 3 min of each dobutamine infusion rate. Images were obtained in the standard parasternal long-axis and short-axis views.
Echocardiographic images were recorded digitally in quadscreen, cine loop format on magnetic optical disks using an echocardiographic image analysis system (Prism 5000; Tom Tec Imaging Systems).
Echocardiograms were read by 2 experienced investigators who were unaware of the clinical data and the results of PET. For the analysis of wall motion, the left ventricle was divided into 16 segments as previously described (20). The basal and middle thirds are divided into 6 segments for the short-axis image. Apical 2- and 4-chamber views were used to visualize the apical segments. Wall motion was assessed visually, using both endocardial motion and wall thickening, and was quantified using a 5-point scoring system: 1, normal; 2, mild hypokinesia; 3, severe hypokinesia; 4, akinesia; 5, dyskinesia. In the dysfunctional segments, improvement of segmental wall motion by at least one grade was considered significant. The interobserver and intraobserver variabilities for the wall motion score were 94% and 96%, respectively.
LVEF Assessment
LVEF was defined from available measurements for a given patient using radionuclide angiography (n = 11) or quantitative gated SPECT (n = 7) (26,27).
Subgroups
On the basis of the results of 18F-FDG PET and DSE, dysfunctional segments (grade 3, 4, or 5 on resting echocardiography) were divided into 3 groups: group A, segments with preserved CR and GM (n = 26); group B, segments without CR but with preserved GM (n = 15); and group C, segments without CR and without preserved GM (n = 41).
Statistical Analysis
All data are presented as the mean ± SD. The 11C-acetate PET-derived parameters (k mono and change in k mono) were compared among the 3 groups using repeated-measures ANOVA, with the Scheffé F test applied when ANOVA results were statistically significant. A comparison of proportions was made using the χ2 test or the Fisher exact probability test where appropriate. P < 0.05 was considered statistically significant.
RESULTS
None of the 18 patients who completed the study experienced chest pain or significant ST depression during the 11C-acetate PET or the low-dose DSE. Three segments (1.04%) could not be well visualized by DSE.
Of the remaining 285 segments analyzed, 82 had severe resting dysfunction (echocardiographic score ≥ 3). On the basis of the results of 18F-FDG PET and DSE, group A was 26 segments in 12 patients, group B was 15 segments in 7 patients, and group C was 41 segments in 11 patients.
Hemodynamics
The heart rate, systolic blood pressure, and rate · pressure product were similar for DSE and 11C-acetate PET both at rest and during dobutamine infusion. The heart rate, systolic blood pressure, and rate · pressure product significantly increased during dobutamine infusion in both studies (Table 2).
Comparison of Hemodynamics at Rest and During Dobutamine Infusion
Oxidative Metabolism
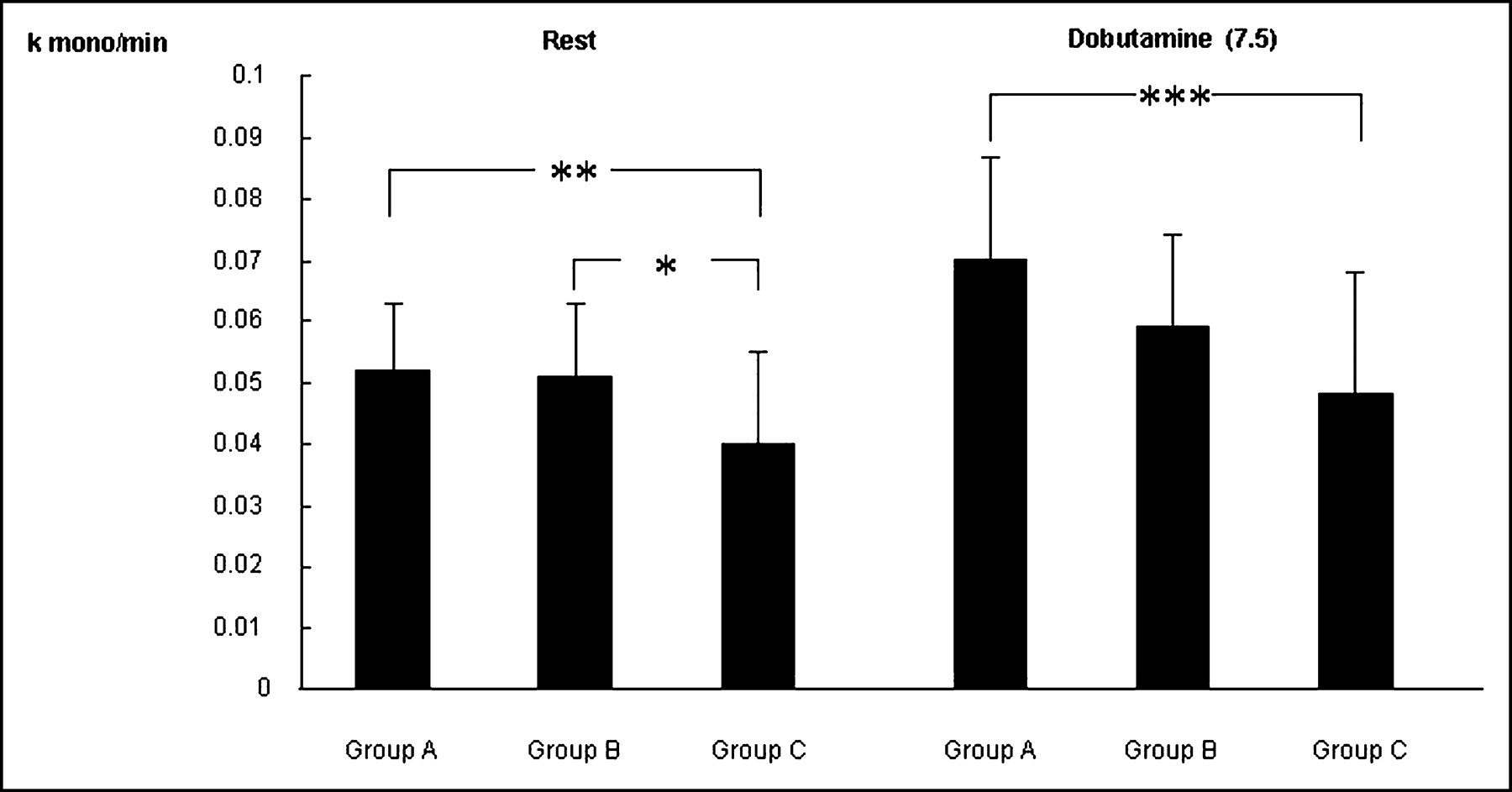
The resting k mono value, used as a measure of oxidative metabolism, was similar in group A (0.052 ± 0.011/min) and group B (0.051 ± 0.012/min, P = not significant). The resting k mono was lower in group C (0.040 ± 0.015/min) than that in group A (P < 0.005) or group B (P < 0.03; Fig. 1). In addition, the k mono during dobutamine infusion in group C (0.048 ± 0.020/min) was significantly lower than that in group A (0.070 ± 0.017/min, P < 0.001) and tended to be lower than that in group B (0.059 ± 0.015/min, P = 0.15; Fig. 1). There was no significant difference between group A and group B.

Comparison of myocardial oxidative metabolism at rest and during dobutamine (7.5 μg/kg/min) infusion. *P < 0.03; **P < 0.005; ***P < 0.001.
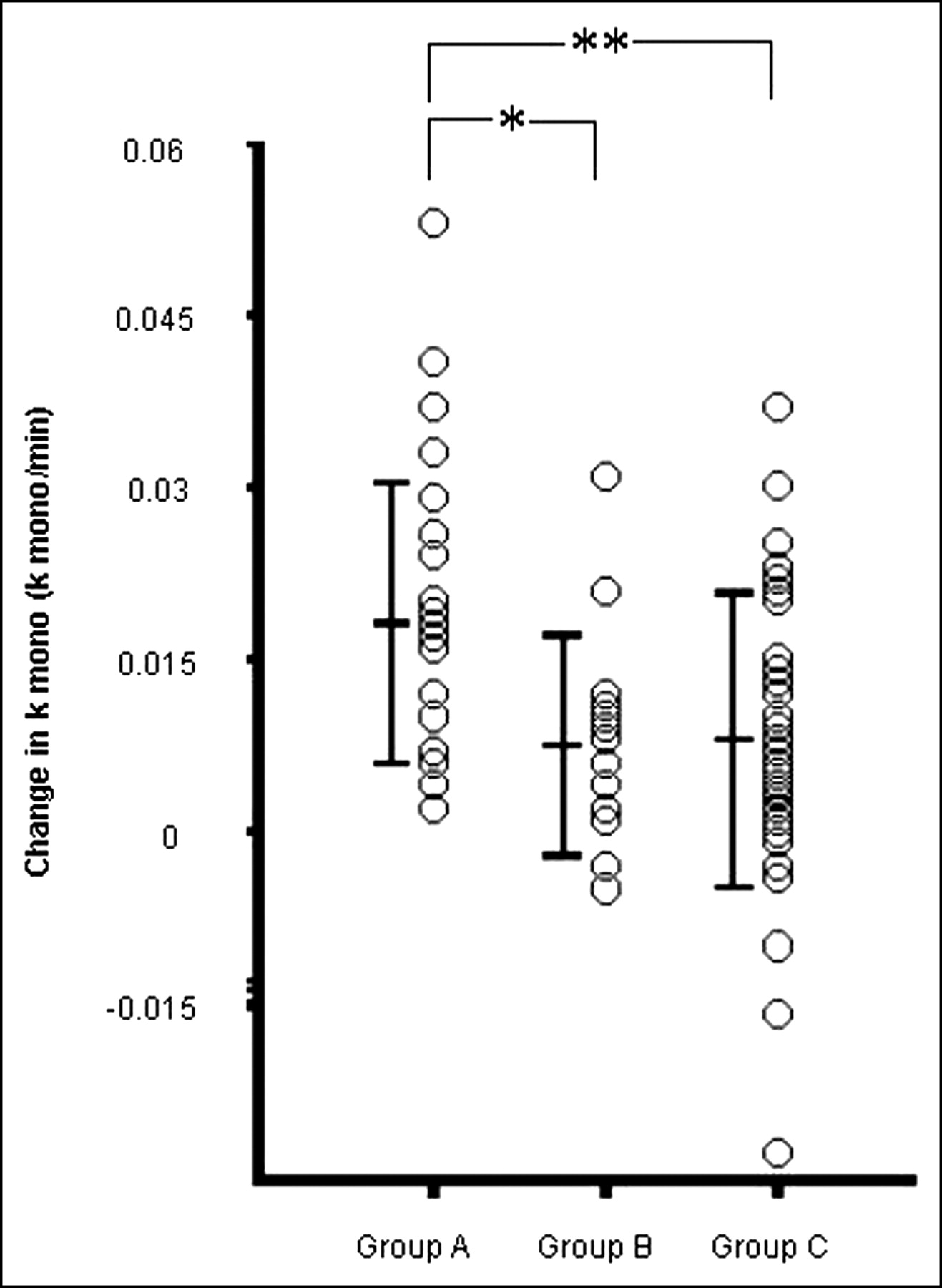
Change in the k mono with dobutamine (as a measure of metabolic reserve) was significantly greater for group A patients (0.018 ± 0.012) than that for group B patients (0.0075 ± 0.0096, P < 0.03) or group C patients (0.0080 ± 0.012, P < 0.005). There was no significant difference between group B and group C (Fig. 2).

Oxidative metabolic response to dobutamine (change in k mono). *P < 0.03; **P < 0.005.
Myocardial Perfusion
In the regions with dysfunctional myocardium, 3 of 26 segments (12%) had reduced perfusion in group A compared with 8 of 15 segments (53%) in group B (P < 0.01) and 37 of 41 segments (90.2%) in group C (P < 0.001). Reduced perfusion was more often seen in group C (90.2%) than in group B (53%) (P < 0.01) (Table 3).
Myocardial Perfusion in Dysfunctional Myocardium
DISCUSSION
These data indicate that myocardium with preserved GM has preserved resting oxidative metabolism. However, myocardial segments without CR have a reduced oxidative metabolic reserve during low-dose dobutamine infusion, even when GM was preserved. The loss in CR may be related to the reduction in the metabolic reserve in severely dysfunctional myocardium despite preservation of tissue viability based on 18F-FDG PET.
Discrepancy Between Accuracy of DSE and 18F-FDG PET Findings
Although 18F-FDG imaging and DSE are considered accurate noninvasive methods for identifying viable myocardium, previous reports indicate that there are discrepancies between the 2 methods in the evaluation of myocardial viability (9–11,28). In the present study, there were 15 segments with a loss of CR in spite of preserved GM.
It has been suggested that segments with both preserved CR and GM have improved regional function earlier after revascularization. In contrast, segments without CR but with preserved GM may require a longer period before improvement in regional function becomes apparent after revascularization (29). Camici and Dutka (30) suggested that there are 2 phases of myocardial hibernation: “functional hibernation” with preserved CR and “structural hibernation” without CR in segments with preserved GM. In the present study, group A would correspond to functional hibernation and group B would correspond to structural hibernation as defined by Camici and Dutka (30).
The present data suggest that, in addition to a loss of CR, there is a reduction in the oxidative metabolic response in the structural hibernating-type myocardium. To the best of our knowledge, the oxidative metabolic response in myocardium with preserved CR and in myocardium without CR but with preserved GM has not been previously described.
Oxidative Metabolism in Hibernating Myocardium
11C-Acetate PET permits the evaluation of flux through the tricarboxylic acid cycle (TCA) in mitochondria and, therefore, reflects oxidative metabolism and myocardial oxygen consumption (11). Using 11C-acetate PET, oxidative metabolism has been shown to be significantly greater in hibernating myocardium than that in scar tissue (13,15,31). Budinger et al. (32) reported that the mitochondrial potential was maintained during hypoxia in dysfunctional but viable myocardium in cultured myocytes. This may account for the preserved oxidative metabolism observed in the current study.
Inotropic Response in Hibernating Myocardium
Inotropic stimulation using dobutamine increases regional myocardial blood flow and oxygen consumption (15,16,33). Therefore, myocardial contraction can improve in both normal and viable myocardium. Myocardial oxidative metabolism increases during low-dose dobutamine infusion in viable segments (15,16). Data from the current study are consistent with these previous reports. However, in the current study, the value for change in the k mono in segments without CR but with preserved GM was lower than that in segments with preserved CR and GM in spite of preserved resting oxidative metabolism.
The metabolic responses observed in this study are lower than those previously reported by Hata et al. (15). These differences may relate to a variation in the patient population. In the present study, 13 patients (72%) had multivessel disease (39% with 2-vessel disease and 33% with triple-vessel disease). Hata et al. evaluated oxidative metabolism in patients with single-vessel disease. The mean LVEF in the present study was 37.1% and was lower than that in the Hata et al. study (LVEF of the “viable” group was 45%). Our study extended the assessment of oxidative metabolic responses by comparing 11C-acetate PET in segments with CR measurements using DSE as well as GM using 18F-FDG PET.
In histopathologic studies, sarcomere loss and myocardial fibrosis were observed in the segments with hibernating myocardium. The presence of sarcomere loss and fibrosis correlated inversely with functional recovery after revascularization (31,32). The degree of fibrosis is also associated with loss of CR (34). Mitochondria structure is altered. Small mitochondria and degenerative mitochondria are seen in hibernating myocardium (35,36). Although the pathophysiologic significance of mithochondrial degeneration has not been well established, the degeneration might be one possible explanation of our findings.
11C-Acetate clearance from the myocardium via the TCA cycle in mitochondria has been shown to correlate with myocardial oxygen consumption (12). Decrease of the metabolic response in the segments without CR but with preserved GM may be due to the mitochondrial dysfunction including a reduction of TCA cycle activity.
Limitations
We did not assess the recovery of regional wall motion abnormalities or global function after revascularization. This study did not provide any information on the relative merits of dobutamine stimulation versus PET for predicting improvement in contractile function after revascularization. This topic is important for investigation but was not the aim of this study. The primary purpose of the present study was to examine oxidative metabolism and metabolic responses of myocardium with and without CR in the setting of preserved GM. In addition, some patients could not be revascularized; therefore, wall motion recovery data were not available. However, evaluation of wall motion recovery after revascularization is important and requires further investigation in future studies.
Although, the study population was small (n = 20), the current study demonstrated impaired metabolic response in the segments without preserved CR but with preserved GM. Large clinical trials may be required for a more comprehensive comparison of the GM, CR, and metabolic responses and their role in understanding dysfunctional myocardium and its recovery.
Previous studies reported that CR correlated with regional myocardial blood flow and flow reserve in the dysfunctional myocardium (16). The current study did not quantify flow. Therefore, stress flow and reserve could not be determined. Thus, their contribution to the blunted oxidative metabolic response was not evaluated.
In the present study, we analyzed segmental myocardial conditions. This segmental analysis is a well-established method applied in many previous studies. Viability assessment is also helpful for predicting improvement in overall patient outcome. Therefore, patient-related analysis becomes an important method to evaluate myocardial viability and should be considered in future studies.
The anatomic correlation between echocardiographic segment location, 11C-acetate PET, and 18F-FDG PET segment location may not be precise. However, we used the same standard 16-segmentation model and the same anatomic landmark for the 3 studies to minimize anatomic mismatching—thus reducing misalignment among these studies (20,21).
Partial-volume effects due to differences in wall motion may affect imaging data. To address this potential limitation, we performed subsequent analysis considering the wall motion score. The mean regional wall motion score in group A was lower than that in group B (P < 0.05) and group C (P < 0.01), but there was no significant difference between group B and group C. This may have impacted the partial-volume effect. However, as all segments in all 3 groups had a regional wall motion score ≥ 3, this effect was likely small.
11C-Acetate PET k mono data have a narrow range. Due to this narrow range in data, many groups have suggested several parameters, such as segmental ratio, clearance rate, normalized oxidative metabolism, and percentage increase. In the present study, we evaluated the metabolic response by change of the k mono, which was k mono during dobutamine infusion minus k mono at rest (15,16). This parameter is a relatively simple measurement to perform and reflects the metabolic response of the myocardium to dobutamine. Therefore, we adopted this parameter for the present study.
DSE was performed at baseline and during the low-dose dobutamine infusion (7.5 μg/kg/min). The ability of low-dose DSE to detect the hibernating myocardium has been reported in several studies. These studies evaluated the response of regional wall motion during the dobutamine infusion of 5–10 μg/kg/min. Afridi et al. reported that the optimal dose of dobutamine for the prediction of myocardial hibernation was 7.5 μg/kg/min (3). Therefore, we used this dose to evaluate the wall motion by the DSE. We did not evaluate the biphasic response to dobutamine, which can also be useful as a predictor for the functional recovery after revascularization (1). Evaluation of the oxidative metabolic reserve in the segments with biphasic response would also be relevant but requires further clinical studies.
CONCLUSION
Viable myocardium, defined by 18F-FDG PET, has preserved resting oxidative metabolism. However, myocardium without CR but with preserved GM has a reduced oxidative metabolic response to low-dose dobutamine infusion. The loss of CR may be related to alterations in the metabolic response in severely dysfunctional myocardium despite preservation of tissue viability. One theoretic explanation of the reduced metabolic reserve may be the impaired mitochondrial response to inotropic stimulation. Further studies are warranted to investigate this and the role of the metabolic reserve in the continuum of recoverable ventricular dysfunction.
Acknowledgments
The authors thank Ken-ichi Nishijima, MS, Hidehiko Omote, RT, Hiroshi Arai, RT, and Kotaro Suzuki, RT, for their technical assistance and Eriko Suzuki, Mutsumi Satoh, Stephanie Thorn, MSc, and Sherri Nipius for their help in preparing the manuscript.
Footnotes
Received Feb. 9, 2004; revision accepted Apr. 29, 2004.
For correspondence or reprints contact: Nagara Tamaki, MD, Department of Nuclear Medicine, Hokkaido University Graduate School of Medicine, Kita-Ku, Kita 15 Nishi 7, Sapporo, 060-8638, Japan.
E-mail: natamaki{at}med.hokudai.ac.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effects of Surgical Ventricular Reconstruction and Mitral Complex Reconstruction on Cardiac Oxidative Metabolism and Efficiency in Nonischemic and Ischemic Dilated Cardiomyopathy
- The Effects of Continuous Positive Airway Pressure on Myocardial Energetics in Patients With Heart Failure and Obstructive Sleep Apnea