


Abstract
Intramyocardial injection of bone marrow cells has been proposed as a new therapeutic option for patients with chronic ischemic heart disease. We investigated whether autologous bone marrow–derived mononuclear cell injection into the myocardium of patients with drug-refractory ischemia reduces anginal symptoms, improves left ventricular (LV) function, increases myocardial perfusion, and alters the extent of scar tissue. Methods: In 25 patients (mean age ± SD, 64 ± 10 y; 21 male) with drug-refractory angina pectoris (Canadian Cardiovascular Society [CCS] class III–IV), despite optimized medical therapy and without options for conventional revascularization, bone marrow was aspirated from the iliac crest. Mononuclear cell injections were targeted at myocardial regions with stress-induced ischemia on gated 99mTc-tetrofosmin SPECT. Anginal symptoms were reassessed at 3- and 6-mo follow-up. At baseline and 3-mo follow-up, gated 99mTc-tetrofosmin SPECT and 18F-FDG SPECT were performed to assess LV function, LV volumes, myocardial perfusion (stress and rest, 17-segment model), and extent of scar tissue. Results: Mean CCS score improved from 3.4 ± 0.6 at baseline to 2.3 ± 0.6 at 3 mo (P < 0.01) and remained unchanged at 6 mo (2.3 ± 0.6; P < 0.01 vs. baseline and P = not significant [NS] vs. 3 mo). Gated 99mTc-tetrofosmin SPECT demonstrated an increased LV ejection fraction (from 47.6% ± 13.5% to 54.1% ± 16.9%; P < 0.01) and a reduced LV end-systolic volume (from 81 ± 68 mL to 75 ± 70 mL; P < 0.01). Segmental regional wall thickening increased from 34% ± 12% at baseline to 39% ± 17% at 3-mo follow-up (P = 0.01). The number of segments with stress-inducible ischemia per patient decreased from 4.6 ± 3.2 to 2.0 ± 2.6 (P < 0.01). Both segmental stress and segmental rest score improved, although the improvement in stress score was more pronounced (decrease in segmental stress score 0.22 ± 0.20 vs. decrease in segmental rest score 0.04 ± 0.06; P < 0.01). Myocardial perfusion improved in 53% of the injected segments and in 13% of the noninjected segments (P < 0.01). The percentage of myocardial segments with some extent of scar remained unchanged at 3-mo follow-up (13% vs. 12%; P = NS). Conclusion: Autologous bone marrow–derived mononuclear cell injection in patients with drug-refractory angina and chronic ischemia improves anginal symptoms, increases LV function, and predominantly enhances myocardial stress perfusion in injected segments, whereas the extent of myocardial scar tissue remains unchanged.
Bone marrow cell transplantation has been proposed as a new therapeutic option for patients with chronic ischemic heart disease. Previous studies demonstrated the safety of intramyocardial injection of autologous bone marrow–derived mononuclear cells (1–4). Moreover, these initial studies suggested that bone marrow cell transplantation reduced anginal symptoms, enhanced myocardial perfusion, and increased cardiac function (1–4).
Although the potential mechanism of benefit from bone marrow cell transplantation has been evaluated in animal models (5–10), few data are available in patients. It is hypothesized that bone marrow cells promote angiogenesis either through secretion of angiogenic cytokines (11) (resulting in a more-or-less generalized effect) or differentiation in endothelial and vascular smooth muscle cells (6,12) (resulting in a regional effect). Furthermore, it is unclear whether procedural-induced necrosis of ischemic myocardium or regeneration of myocardial tissue (9) (resulting in a reduced scar area and or increased viability) contributes to the beneficial effects.
Nuclear imaging could potentially contribute in the evaluation of the benefit from bone marrow cell injection. Gated 99mTc-tetrofosmin SPECT has a high sensitivity for the detection of myocardial ischemia (13,14), and 18F-FDG imaging is an excellent technique to differentiate viable myocardium from scar tissue, based on the assessment of cellular glucose use (15,16).
The aim of this study was to provide more insight into the mechanism of benefit from bone marrow cell transplantation in patients with chronic ischemia. 99mTc-Tetrofosmin SPECT was used to evaluate changes in myocardial perfusion after cell transplantation and 18F-FDG SPECT was used to evaluate changes in scar tissue after cell transplantation.
MATERIALS AND METHODS
Patients
The study population consisted of 25 consecutive “no-option” patients with chronic coronary artery disease and ischemia on nuclear (gated 99mTc-tetrofosmin SPECT) imaging. Patients had angina pectoris despite maximally tolerated medical therapy and were ineligible for percutaneous or surgical revascularization as assessed by coronary angiography. Ineligibility for surgical or percutaneous revascularization procedures was determined by an independent expert panel that reviewed the angiograms. The panel comprised 2 cardiovascular surgeons, 2 interventional cardiologists, and a noninvasive cardiologist.
Exclusion criteria were acute myocardial infarction within 6 mo of enrollment in the study, history of malignancy, renal dysfunction (serum creatinine > 200 μmol/L), or unexplained hematologic or biochemical abnormalities. The local ethics committee approved the protocol and all patients gave informed consent.
Study Protocol
At baseline the severity of angina was graded according to the Canadian Cardiovascular Society (CCS) score. The Seattle Angina Questionnaire was used to assess quality of life. Within 2 wk before bone marrow cell injection, gated 99mTc-tetrofosmin SPECT (to assess left ventricular [LV] function and myocardial perfusion) and 18F-FDG imaging (to assess myocardial glucose use and detect viability and scar tissue) were performed.
On the day of the injection procedure, bone marrow was aspired from the iliac crest under local anesthesia. Mononuclear cells were isolated by Ficoll density gradient. During isolation of mononuclear cells, patients underwent nonfluoroscopic LV electromechanical mapping with the NOGA system (NOGA star catheter; Biosense, Johnson & Johnson Co.). After completion of LV mapping, the mapping catheter was replaced by an injection catheter (Myostar catheter, Biosense). Autologous bone marrow–derived mononuclear cell injections were targeted at myocardial regions with stress-induced ischemia (on gated 99mTc-tetrofosmin SPECT). The injection catheter was prepared as described previously (3). Before every injection of cells into the LV myocardium, the following criteria had to be met: unipolar voltage ≥6.9 mV (to identify viable myocardium within the treatment area); perpendicular position of the catheter to the myocardial wall; excellent loop stability (<4 mm); and presence of a premature ventricular contraction on extension of the needle into the myocardium. Subsequently, 8−13 intramyocardial injections of approximately 0.2 mL each were performed.
Immediately after the procedure, continuous heart rhythm monitoring was started for 2 d. Before discharge, 2-dimensional (2D) echocardiography was performed to exclude pericardial effusion. At 3 and 6 mo, angina (CCS score), quality of life (Seattle Angina Questionnaire), and occurrence of ventricular arrhythmias (24-h Holter monitoring) were assessed. In addition, gated 99mTc-tetrofosmin SPECT and 18F-FDG imaging were repeated at 3-mo follow-up to reassess LV function, myocardial perfusion, and myocardial viability (and scar tissue).
99mTc-Tetrofosmin SPECT: Data Acquisition
A 2-d stress–rest protocol was used for the 99mTc-tetrofosmin SPECT examination. The stress protocol included a symptom-limited bicycle exercise test. Whenever possible, β-blockers and calcium antagonists were discontinued for 24 h before 99mTc-tetrofosmin SPECT. Test endpoints were physical exhaustion, angina pectoris, dyspnea, significant decrease in blood pressure (>10 mm Hg), or achievement of maximal age-related heart rate. Blood pressure, heart rate, and electrocardiogram (ECG) findings were monitored during the test. 99mTc-Tetrofosmin (500 MBq) was injected intravenously at peak exercise, which was continued for another 1−2 min after tracer injection. In patients unable to exercise, pharmacologic stress (intravenous administration of adenosine [0.14 mg/kg/min for 6 min] or dobutamine [up to a maximum dose of 40 μg/kg/min in 15 min]) was used. On the second day, resting images were obtained (using 500 MBq 99mTc-tetrofosmin) after the patient's daily dose of nitrates. The resting studies were acquired using ECG gating, for assessment of LV ejection fraction and LV volumes (17). Stress and rest imaging was performed with the same medications and the same type of stressor at baseline and at 3-mo follow-up. In particular, the use (and dosages) of β-blockers, calcium channel blockers, and nitrates was unchanged at 3-mo follow-up.
Imaging was performed using a triple-head SPECT camera (GCA 9300/HG; Toshiba Corp.) equipped with low-energy, general-purpose collimators. A 20% window was used around the 140-keV energy peak of 99mTc. Ninety projections (step-and-smooth mode; 35 s per projection; total imaging time, 23 min) were obtained over a 360° circular orbit. Data were stored in a 64 × 64 matrix. The raw scintigraphic data were reconstructed with filtered back projection using a Butterworth filter (cutoff frequency, 0.26 cycle per pixel, order 9). No attenuation correction was used.
99mTc-Tetrofosmin SPECT: Data Analysis and Tissue Characterization
Additional reconstruction yielded standard long- and short-axis projections perpendicular to the heart axis. Reconstructed slices were 6 mm in all projections. The short-axis slices were displayed in polar map format, adjusted for peak myocardial activity (100%). The myocardium was divided into 17 segments, as previously proposed (18).
The 99mTc-tetrofosmin SPECT images were analyzed by 2 experienced observers, who were unaware of the clinical information at the time of 99mTc-tetrofosmin SPECT image review. Quantitative assessment of LV function, LV end-diastolic and end-systolic volumes, and wall thickening was performed using previously validated and automated software (quantitative gated SPECT [QGS]; Cedars-Sinai Medical Center, Los Angeles, CA) (19). By estimating and displaying the endo- and epicardial surfaces, the LV end-systolic and LV end-diastolic volumes are calculated, and LV ejection fraction is derived. Intra- and interobserver reproducibility for LV ejection fraction (intercept = 0.6, slope = 0.01, r = 1.00, mean difference = 0.04% ± 1.2%, resp. intercept = 2.1, slope = 0.06, r = 0.98, mean difference = 0.81% ± 3.9%), LV end-systolic volume (intercept = 1.7, slope = 0.01, r = 1.00, mean difference = 0.8 ± 3.6 mL, resp. intercept = 7.6, slope = 0.04, r = 0.98, mean difference = 4.0 ± 15.8 mL), and end-diastolic volume (intercept = 2.7, slope = 0.01, r = 1.00, mean difference = 1.1 ± 4.5 mL, resp. intercept = 8.1, slope = 0.04, r = 0.99, mean difference = 3.6 ± 13.5 mL) was excellent.
Myocardial wall thickening was assessed as percentage increase (distance between endocardial and epicardial surfaces, normal to the midmyocardial surface) from end-diastole to end-systole (19). Segmental wall thickening scores were summed and divided by 17 to yield the mean segmental wall thickening.
Myocardial perfusion was analyzed quantitatively (QGS software) and segmental tracer activity was categorized on a 4-point scale: 1 = normal tracer activity > 75%; 2 = tracer activity 50%−75%; 3 = tracer activity 25%−50%; 4 = tracer activity < 25%. Perfusion defects on stress images were considered present when tracer activity was <75% of maximum. When significant fill-in (>10%) of perfusion defects was observed on the resting images, segments were classified as ischemic. Patients' segmental stress scores were summed and divided by 17 to yield the patients' segmental stress score (20). Similarly, patients' segmental rest score was calculated. Intra- and interobserver agreement for segmental perfusion scores were 98% and 95%, respectively.
18F-FDG Imaging: Data Acquisition
18F-FDG imaging, to evaluate myocardial glucose use, was performed on a separate day, after acipimox (Byk) administration (a nicotinic acid derivative, 500 mg, oral dose) (21). Acipimox enhances myocardial 18F-FDG uptake by reducing the plasma level of free fatty acids (22). After acipimox administration, the patients received a low-fat, carbohydrate-rich meal. This small meal further enhances myocardial 18F-FDG uptake by stimulating endogenous insulin release (23). Sixty minutes after acipimox administration, a blood sample was taken to assess plasma glucose levels. When plasma glucose was between 5 and 7 mmol/L, 185 MBq 18F-FDG were injected at rest. Forty-five minutes thereafter, data acquisition was begun. Metabolic imaging was performed at rest using the same SPECT system as described for perfusion imaging, and the system was equipped with commercially available 511-keV collimators. Data were acquired over 360° and stored in a 64 × 64, 16-bit matrix.
18F-FDG Imaging: Data Analysis
From the raw scintigraphic data, transaxial slices were reconstructed by filtered back projection using a Butterworth filter (cutoff frequency, 0.17 cycle per pixel, order 8). Attenuation correction was not applied. Further reconstruction yielded standard short- and long-axis projections perpendicular to the heart axis. 18F-FDG short-axis slides were displayed in polar map format, normalized to the maximum activity (set at 100%); the polar maps were divided into 17 segments (18). The quantitatively analyzed segments were divided into 4 groups on the basis of the tracer activity: 1 = normal tracer uptake (activity >75%), 2 = mildly reduced tracer uptake (activity 50%−75%), 3 = moderately reduced tracer uptake (activity 25%−50%), and 4 = severely reduced tracer uptake (activity <25%). Patients' segmental 18F-FDG scores were summed and divided by 17 to yield the patients' segmental 18F-FDG score (indicating extent of reduced glucose use per patient, as a global indicator of the extent of scar tissue per patient). All segments were subsequently evaluated for viability. Segments were considered as viable (normal) when normalized 18F-FDG activity was >75%; segments with tracer uptake of <75% were considered to contain some extent of scar. Intra- and interobserver agreement for segmental assessment was 94% and 97%, respectively.
Statistical Analysis
All continuous data are expressed as mean ± SD. Continuous variables were compared using the paired, 2-tailed Student t test. Differences between proportions were compared using the χ2 test with Yates correction. The intra- and interobserver reproducibility of LV ejection fraction and LV volumes was determined by linear regression analysis (Pearson correlation coefficient). For all tests, a P value < 0.05 was considered statistically significant.
RESULTS
Twenty-five patients were included in this study (mean age ± SD, 64 ± 10 y; 21 male). The baseline clinical characteristics are summarized in Table 1. During the 6-mo follow-up period, the type and dose of medications remained unchanged. Two patients did not tolerate β-blockers because of chronic obstructive pulmonary disease. Another patient did not tolerate statins due to myalgia. All patients were ineligible for surgical revascularization or percutaneous coronary intervention as they had diffuse coronary artery disease with poor target vessels (small caliber).
Clinical Characteristics of Study Population
Safety Data and Clinical Outcome
Patients received 10.3 ± 1.8 (range 8−13) injections of approximately 0.2 mL each in 29 regions with stress-inducible ischemia (11 inferior, 7 lateral, 8 anterior, 3 septal). In 4 patients with >1 ischemic region, 2 different ischemic regions were injected (number of injections was equally distributed). With each intramyocardial injection, 8.17 ± 3 × 106 cells were injected. The total number of bone marrow–derived mononuclear cells in the injected suspension was 84.1 ± 28.7 × 106.
Autologous bone marrow–derived mononuclear cell injection was safe: Ventricular arrhythmias were not observed and no postprocedural pericardial effusion was detected on 2D echocardiography.
Mean CCS score improved from 3.4 ± 0.6 at baseline to 2.3 ± 0.6 at 3 mo (P < 0.01) and remained unchanged at 6 mo (2.3 ± 0.6; P < 0.01 vs. baseline and P = not significant [NS] vs. 3 mo). Quality of life improved from 53% ± 10% to 72% ± 11% at 3 mo (P < 0.01) and 73% ± 14% at 6 mo (P < 0.01).
Stress Test Data
Imaging was performed with the same medications and the same type of stressor (bicycle exercise test n = 11; adenosine n = 12; dobutamine n = 2) at baseline and at 3-mo follow-up. Although there was a trend toward an increase in the level of stress achieved at 3-mo follow-up, this did not reach statistical significance (130 ± 32 W vs. 135 ± 35 W; P = 0.10). The maximal heart rate and maximal blood pressure were similar at baseline and at 3-mo follow-up (Table 2). In the week before the baseline 99mTc-tetrofosmin SPECT study, patients experienced 17 ± 27 episodes of angina, as compared with 5 ± 8 episodes in the week before the 3-mo follow-up 99mTc-tetrofosmin SPECT study (P = 0.01).
Stress Test Data
Blood samples taken before each 99mTc-tetrofosmin SPECT study indicated that the plasma levels of total cholesterol (4.7 ± 1.2 mmol/L vs. 4.8 ± 1.3 mmol/L; P = NS) and C-reactive protein (5 ± 5 mg/L vs. 5 ± 4 mg/L; P = NS) remained unchanged. Also, body mass indices remained unchanged: 28 ± 4 kg/m2 at baseline versus 28 ± 4 kg/m2 at 3-mo follow-up (P = NS).
LV Function and Volumes
Gated 99mTc-tetrofosmin SPECT demonstrated a significant increase in LV ejection fraction from 47.6% ± 13.5% at baseline to 54.1% ± 16.9% at 3-mo follow-up (P < 0.01). LV end-systolic volume decreased (from 81 ± 68 mL to 75 ± 70 mL after 3 mo; P < 0.01), whereas LV end-diastolic volume remained unchanged (Table 3). Segmental regional wall thickening at rest increased from 34% ± 12% at baseline to 39% ± 17% at 3-mo follow-up (P = 0.01).
LV Ejection Fraction and Volumes as Assessed by Gated 99mTc-Tetrofosmin SPECT
Myocardial Perfusion
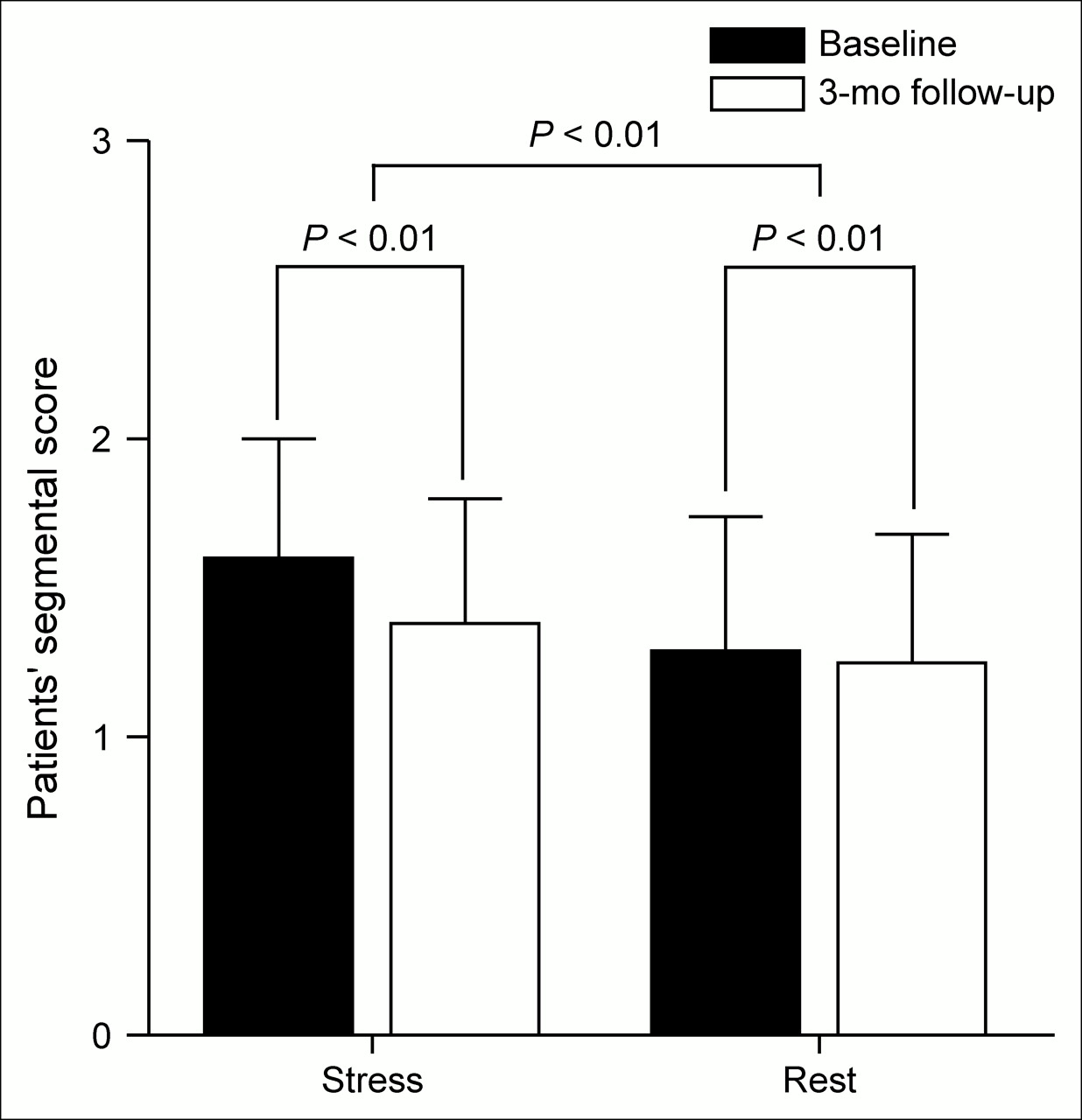
At 3-mo follow-up, the number of segments with stress-inducible ischemia per patient decreased from 4.6 ± 3.2 to 2.0 ± 2.6 (P < 0.01). An example of resolution of inferior ischemia (baseline to 3-mo follow-up) is shown in Figure 1. The segmental stress score per patient improved from 1.60 ± 0.40 to 1.38 ± 0.42 (P < 0.01). Similarly, resting perfusion improved, as evidenced by a decrease in segmental rest score from 1.29 ± 0.45 to 1.25 ± 0.43 (P < 0.01). The improvement in stress score was more pronounced than the improvement in rest score (Fig. 2).

SPECT images (vertical long axes) from representative patient. 99mTc-Tetrofosmin SPECT shows stress-induced ischemia at baseline in inferior wall (arrow). At 3-mo follow-up, ischemia in inferior wall has resolved. Metabolic imaging shows normal 18F-FDG uptake at baseline and 3-mo follow-up in that region, indicating no scar formation after intramyocardial injection of bone marrow–derived mononuclear cells.
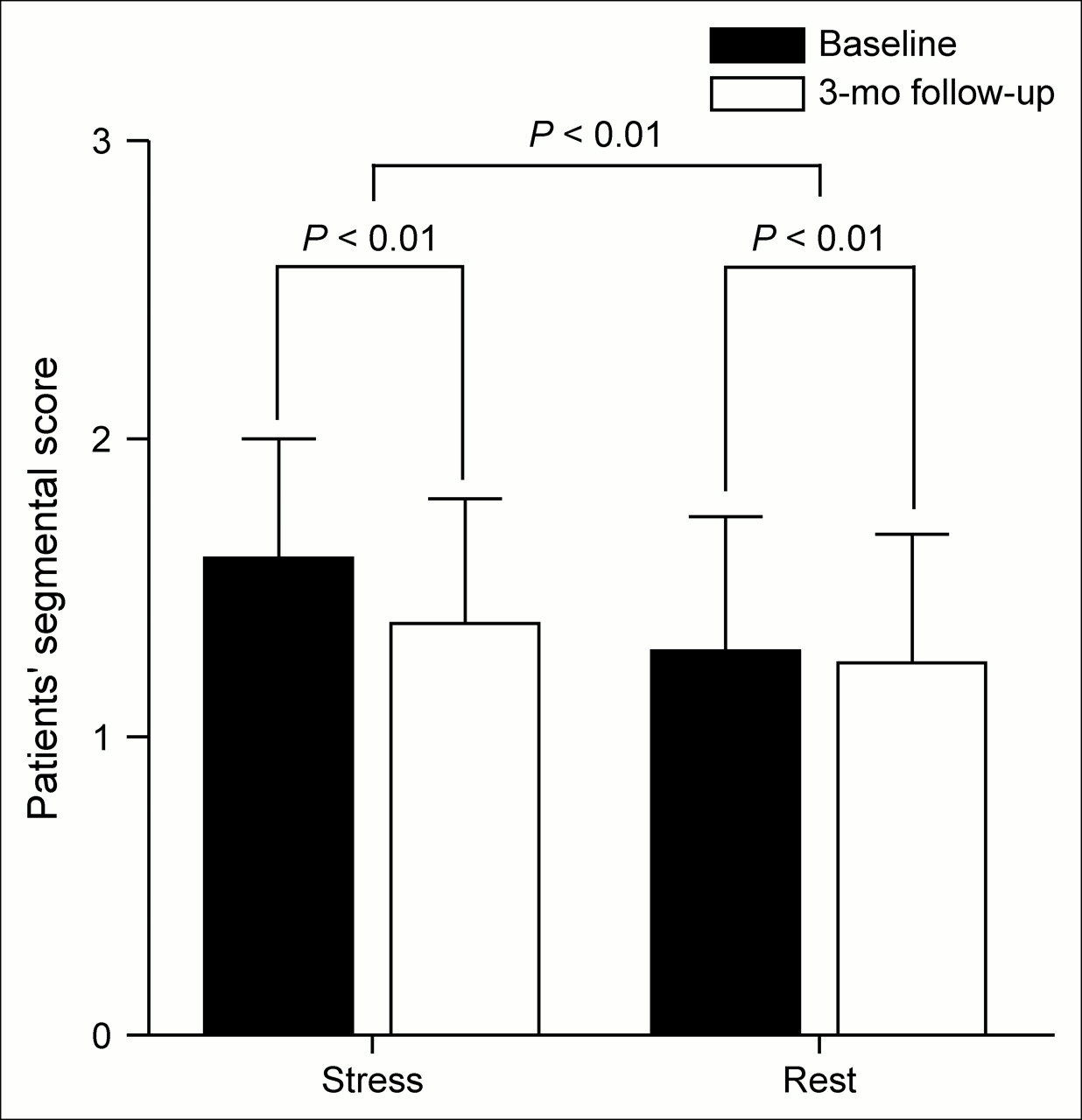
Patients' segmental stress and rest scores improved significantly 3 mo after autologous bone marrow–derived mononuclear cell injection. Magnitude of increase in stress score was significantly higher as observed for rest score.
Perfusion and Function in Injected Versus Noninjected Segments
In 25 patients, 257 injections were targeted at 91 myocardial segments (3.6 ± 1.4 injected segments per patient). Of the 91 injected segments, 48 segments increased at least 1 point in rest or stress perfusion (53%), whereas 45 of 334 (13%) of the noninjected segments improved (P < 0.01; Table 4).
Perfusion in Injected and Noninjected Segments
The stress score significantly improved in both injected and noninjected segments, although the improvement in injected segments was more pronounced (decrease in injected segments 0.42 ± 0.39, vs. decrease in noninjected segments 0.14 ± 0.18; P < 0.01; Figure 3). There was a trend toward an improvement in rest score in injected (P = 0.05) and noninjected segments (P = 0.06). The magnitude of the improvement in rest score was similar in injected and noninjected segments (injected segments 0.07 ± 0.16, vs. noninjected segments 0.02 ± 0.05; P = NS; Fig. 3).
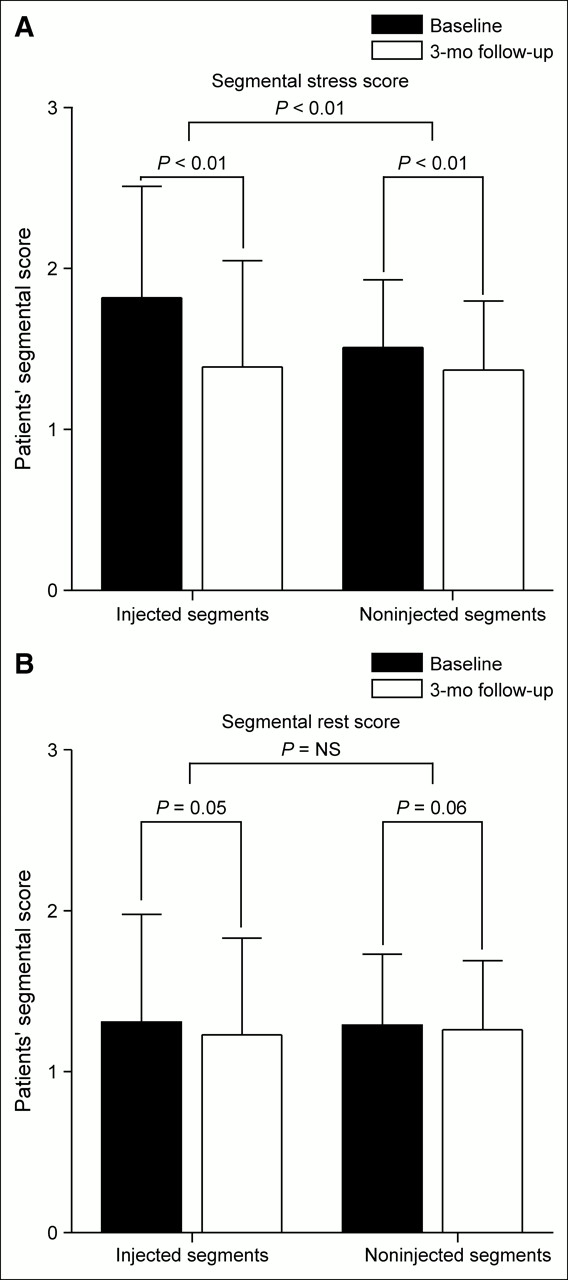
Patients' gated 99mTc-tetrofosmin SPECT segmental stress and rest scores in injected and noninjected segments. (A) Patients' segmental stress score improved in injected and noninjected segments. Improvement in injected segments was more pronounced than improvement in noninjected segments. (B) There was a trend toward improvement in rest score in injected and noninjected segments. Magnitude of improvement in rest score was similar in injected and noninjected segments.
Regional wall thickening at rest increased in both injected segments (from 37% ± 17% to 42% ± 22%; P = 0.02) and noninjected segments (from 33% ± 12% to 38% ± 17%; P = 0.03). The magnitude of improvement was similar in injected and noninjected segments (P = NS).
Viability
18F-FDG image quality was poor in 1 patient with diabetes mellitus and was subsequently excluded from analysis, leaving 408 segments for the final analysis. An example of 18F-FDG imaging at baseline and at 3-mo follow-up is shown in Figure 1. The amount of scar segments was similar at baseline and 3-mo follow-up (55/408 [13%] vs. 48/408 [12%]; P = NS). The patients' segmental 18F-FDG score remained unchanged (1.20 ± 0.3 at baseline vs. 1.18 ± 0.3 at 3-mo follow-up; P > 0.05). The 18F-FDG score improved in 10 of 408 segments (6/24 patients), whereas the 18F-FDG score decreased in 0 of 408 segments (0/24 patients).
DISCUSSION
The aim of this study was to provide more insight into the mechanism of benefit from bone marrow cell transplantation in patients with chronic ischemia despite optimal pharmacologic and nonpharmacologic treatment. The findings of the current study can be summarized as follows:
A significant improvement in anginal symptoms and LV function was observed after autologous bone marrow cell transplantation.
Myocardial perfusion and function increased predominantly in injected segments but also, to some extent, in noninjected segments. The main improvement was detected in stress perfusion, indicating relief of ischemia.
No increase in extent of scar tissue was observed after bone marrow cell transplantation.
Comparison with Previous Studies
Various studies have suggested a beneficial effect of bone marrow cell transplantation in patients with chronic ischemic heart disease (1–4). Two studies described an improvement in anginal symptoms and myocardial perfusion in patients with severe angina pectoris (1,2). In heart failure patients, an increase in LV function was described after 4-mo follow-up (3). The findings of our study are in line with these previously published clinical studies. Perin et al. demonstrated in 21 patients with ischemic heart failure that bone marrow cell transplantation improved myocardial perfusion but did not alter the percentage of scar tissue (3,4). Similarly, a safety study in 8 patients with severe angina pectoris described a decrease in the area of hypoperfused myocardium assessed by MRI (1). However, both studies did not report whether the increase in perfusion occurred in injected areas only or in the entire left ventricle (1,3,4). Only one safety study in 10 patients with severe angina reported an improved perfusion stress score (assessed by SPECT) within the injected territories, whereas the rest score of these segments remained unchanged (2). In addition, a trend toward improvement in perfusion in the remote myocardium was observed, but the study population was too small to reach statistical significance (2).
Mechanism of Benefit from Bone Marrow Cell Transplantation
The findings of our study are consistent with the hypothesis that bone marrow cells promote angiogenesis, resulting in increased myocardial perfusion and function. As improvement was observed in both injected and noninjected areas, differentiation of bone marrow cells in endothelial and vascular smooth muscle cells cannot solely explain the observed effects. The promotion of angiogenesis could be caused by the production of angiogenic cytokines and upregulation of endogenous cytokine expression, as previously proposed (11).
The area of scar tissue remained unchanged after bone marrow cell injection. This finding indicates that procedural-induced necrosis or embolization of ischemic myocardium could not have contributed to the relief of angina. In addition, regeneration of cardiomyocytes did not result in resolution of scar tissue or an increase in viable tissue.
This study was a prospective, observational study, without a control group or randomization procedure. As a consequence, a placebo effect from bone marrow cell transplantation cannot be ruled out. However, it should be emphasized that all scintigraphic studies were analyzed quantitatively using commercially available software. Large placebo-controlled, randomized trials with long-term follow-up should be performed to confirm the current findings. Furthermore, to clarify the precise cellular mechanism of action underlying the benefit of bone marrow cell injections, future clinical studies are warranted to track the trafficking of bone marrow cells in vivo over long periods of time. From a methodologic point of view, it is important to emphasize that attenuation correction was not used in the SPECT studies, which may have influenced results to some extent.
CONCLUSION
In summary, intramyocardial bone marrow cell transplantation in patients with chronic ischemic heart disease was safe, improved anginal symptoms, and increased LV function. Also, bone marrow cells appear to promote angiogenesis as evidenced by the improvement in perfusion in injected and noninjected segments. Scar formation was not observed. Additional randomized, placebo-controlled trials are warranted to further evaluate this approach of cell-based angiogenic therapy.
References
- Received for publication September 14, 2005.
- Accepted for publication December 19, 2005.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Repeat Cell Therapy for Refractory Angina: Deja vu All Over Again?
- Repeated Intramyocardial Bone Marrow Cell Injection in Previously Responding Patients With Refractory Angina Again Improves Myocardial Perfusion, Anginal Complaints, and Quality of Life
- In Vivo Functional and Transcriptional Profiling of Bone Marrow Stem Cells After Transplantation Into Ischemic Myocardium
- Imaging: Guiding the Clinical Translation of Cardiac Stem Cell Therapy
- Treatment of Refractory Angina
- Effect of Progenitor Cells on Myocardial Perfusion and Metabolism in Patients After Recanalization of a Chronically Occluded Coronary Artery
- Direct Intramyocardial But Not Intracoronary Injection of Bone Marrow Cells Induces Ventricular Arrhythmias in a Rat Chronic Ischemic Heart Failure Model
- Role of Imaging in Cardiac Stem Cell Therapy
- Extent of Viability to Predict Response to Cardiac Resynchronization Therapy in Ischemic Heart Failure Patients