


Abstract
Ibritumomab tiuxetan is an anti-CD20 murine IgG1 κ monoclonal antibody (ibritumomab) conjugated to the linker-chelator tiuxetan, which securely chelates 111In for imaging or dosimetry and 90Y for radioimmunotherapy (RIT). Dosimetry and pharmacokinetic data from 4 clinical trials of 90Y-ibritumomab tiuxetan RIT for relapsed or refractory B-cell non-Hodgkin’s lymphoma (NHL) were combined and assessed for correlations with toxicity data. Methods: Data from 179 patients were available for analysis. Common eligibility criteria included <25% bone marrow involvement by NHL, no prior myeloablative therapy, and no prior RIT. The baseline platelet count was required to be ≥100,000 cells/mm3 for the reduced 90Y-ibritumomab tiuxetan administered dose (7.4–11 MBq/kg [0.2–0.3 mCi/kg]) or ≥150,000 cells/mm3 for the standard 90Y-ibritumomab tiuxetan administered dose (15 MBq/kg [0.4 mCi/kg]). Patients were given a tracer administered dose of 185 MBq (5 mCi) 111In-ibritumomab tiuxetan on day 0, evaluated with dosimetry, and then a therapeutic administered dose of 7.4–15 MBq/kg (0.2–0.4 mCi/kg) 90Y-ibritumomab tiuxetan on day 7. Both ibritumomab tiuxetan administered doses were preceded by an infusion of 250 mg/m2 rituximab to clear peripheral B-cells and improve ibritumomab tiuxetan biodistribution. Residence times for 90Y in blood and major organs were estimated from 111In biodistribution, and the MIRDOSE3 computer software program was used, with modifications to account for patient-specific organ masses, to calculate radiation absorbed doses to organs and red marrow. Results: Median radiation absorbed doses for 90Y were 7.42 Gy to spleen, 4.50 Gy to liver, 2.11 Gy to lung, 0.23 Gy to kidney, 0.62 Gy (blood-derived method) and 0.97 Gy (sacral image-derived method) to red marrow, and 0.57 Gy to total body. The median effective blood half-life was 27 h, and the area under the curve (AUC) was 25 h. No patient failed to meet protocol-defined dosimetry safety criteria and all patients were eligible for treatment. Observed toxicity was primarily hematologic, transient, and reversible. Hematologic toxicity did not correlate with estimates of red marrow radiation absorbed dose, total-body radiation absorbed dose, blood effective half-life, or blood AUC. Conclusion: Relapsed or refractory NHL in patients with adequate bone marrow reserve and <25% bone marrow involvement by NHL can be treated safely with 90Y-ibritumomab tiuxetan RIT on the basis of a fixed, weight-adjusted dosing schedule. Dosimetry and pharmacokinetic results do not correlate with toxicity.
Radioimmunotherapy (RIT) with the pure β-emitter 90Y permits efficient delivery of ionizing radiation to targeted cells while limiting radiation to normal tissue. The 90Y-labeled antibody, 90Y-ibritumomab tiuxetan (Zevalin; IDEC Pharmaceuticals Corp., San Diego, CA), directed against the B-lymphocyte CD20 antigen is well tolerated in clinical trials and has demonstrated overall response rates of 67%–83% for relapsed and refractory non-Hodgkin’s lymphoma (NHL) (1,2). 90Y-Ibritumomab tiuxetan is a murine IgG1 κ monoclonal antibody (ibritumomab) conjugated to the linker-chelator tiuxetan (a derivative of diethylenetriaminepentaacetic acid, designated MX-DTPA) for stable retention of 90Y for RIT or 111In for radiation dosimetry and biodistribution studies. Tiuxetan forms a covalent, urea-type bond with ibritumomab and chelates the radionuclide via 5 carboxyl groups (3). Rituximab, the unlabeled human/mouse chimeric anti-CD20 antibody administered before ibritumomab tiuxetan, induces complement-dependent cytotoxicity, antibody-dependent cell-mediated cytotoxicity, and programmed cell death. The CD20 antigen, the target of both rituximab and ibritumomab tiuxetan, is expressed solely on normal and neoplastic pre-B- to mature B-lineage cells. The CD20 antigen represents an optimal target for immunotherapy because it is absent from hematopoietic stem cells and antibody binding does not induce antigen shedding or modulation (4).
Preclinical studies have demonstrated that the biodistribution of 90Y-ibritumomab tiuxetan is adequately predicted by the 111In-labeled antibody (5,6). 111In (half-life = 67.9 h) emits γ-rays, which can be detected scintigraphically for dosimetry and biodistribution studies.
Ibritumomab tiuxetan dosing in these trials was established on the basis of the results of a phase I trial. In this single-center, dose-escalation study, patients with recurrent low- or intermediate-grade NHL received 0.74, 1.11, 1.48, or 1.85 GBq (20, 30, 40, or 50 mCi) of ibritumomab tiuxetan. The only significant toxicity was myelosuppression. The maximum tolerated dose (MTD) without peripheral blood stem cell or bone marrow reinfusion was established as 50 mCi. Doses of ≤40 mCi of ibritumomab tiuxetan were not myeloablative. Hematologic toxicity was found to correlate best with the quantity of radioactivity administered by body weight (mCi/kg) rather than with total radioactivity (mCi) or with radioactivity administered by body surface area (mCi/m2) (7). Therefore, dosing in later studies was determined by body weight.
On the basis of the results of this first study, a phase I/II ibritumomab tiuxetan trial evaluated nonmyeloablative doses ranging from 7.4 to 15 MBq/kg (0.2–0.4 mCi/kg). The MTD was established at 15 MBq/kg (0.4 mCi/kg) for patients with a baseline platelet count of ≥150,000 cells/mm3 and at 11 MBq/kg (0.3 mCi/kg) for patients with a baseline platelet count of ≥100,000 cells/mm3 (1).
Subsequent trials included a phase III randomized, controlled study comparing 90Y-ibritumomab tiuxetan RIT with a standard course of rituximab immunotherapy (375 mg/m2/wk × 4); a phase II reduced administered dose (11 MBq/kg [0.3 mCi/kg]) study for patients with mild thrombocytopenia; and a phase III study for rituximab-refractory patients. Companion dosimetry and biodistribution studies were conducted with 111In-ibritumomab tiuxetan for 179 patients enrolled in these 4 clinical trials. Dosimetry and biodistribution studies were required to determine that individualized patient radiation absorbed dose estimates to critical organs, and the dose-limiting marrow compartment met safety guidelines. We have combined results from these 4 trials and performed extensive analyses to determine if radiation absorbed dose estimates correlated with indicators of treatment toxicity.
MATERIALS AND METHODS
Patient Population
One hundred seventy-nine patients from 4 phase I, II, and III trials of 90Y-ibritumomab tiuxetan were evaluated in a central dosimetry analysis. Table 1 describes the 4 trials included in this analysis.
Summary of 90Y-Ibritumomab Tiuxetan Studies
Patients with histologically confirmed, relapsed or refractory B-cell NHL were included, providing they had bidimensionally measurable disease and a monoclonal-positive B-cell population in lymph nodes or bone marrow. In addition, patients had to be at least 18 y old, not pregnant or lactating, and following reliable birth control methods. Within 2 wk before initial treatment, patients were required to have acceptable hematologic status (absolute neutrophil count [ANC], ≥1,500 cells/mm3; platelets, ≥150,000 cells/mm3 in standard-dose studies; and ≥100,000 cells/mm3 in reduced-dose studies), and acceptable renal function (creatinine, ≤177 μmol/L) and liver function (bilirubin, ≤34.2 μmol/L). Patients were excluded if they had a bone marrow biopsy demonstrating ≥25% involvement with NHL or prior external beam radiation therapy to >25% of the patient’s bone marrow. There was no limitation on the number of prior therapies or relapses. All prior chemotherapy had to have been completed ≥3 wk before study treatment (6 wk if nitrosourea or mitomycin C). The studies were approved by the Institutional Review Board at each study site and written informed consent was obtained from all patients.
Study Design
In all 4 trials, patients received 250 mg/m2 rituximab to optimize biodistribution of the radiolabeled antibody on day 0, which was immediately followed by 185 MBq (5 mCi) 111In-ibritumomab tiuxetan (1.6 mg ibritumomab tiuxetan) for dosimetry. Dosimetry was performed over the following 6 d at the clinical site. 90Y-ibritumomab tiuxetan was given only if the estimated radiation absorbed dose was below the protocol-defined upper limits of 3.0 Gy for red marrow and 20 Gy for any other organ not involved with NHL. One week after the 111In-ibritumomab tiuxetan injection, patients meeting these dosimetry criteria received a second infusion of rituximab (250 mg/m2), which was immediately followed by a slow intravenous injection of 90Y-ibritumomab tiuxetan over 10 min. The therapeutic administered dose of 90Y-ibritumomab tiuxetan ranged from 7.4 to 15 MBq/kg (0.2–0.4 mCi/kg) up to a maximum administered dose of 1.2 GBq (32 mCi).
Dosimetry
Initial estimates of radiation absorbed dose to support the treatment decision were made at the clinical sites using quantitative imaging and blood sampling data with the MIRDOSE3 software program (8). Subsequently, centralized dosimetric analyses of all patients were performed at the Radiation Internal Dose Information Center, Medical Sciences Division at the Oak Ridge Associated Universities (ORAU), in collaboration with the Division of Nuclear Medicine at the Mayo Clinic. The following section describes methods used at the clinical sites and later replicated for the central analyses.
Whole-body, lungs, liver, spleen, kidney, and bone marrow radiation absorbed doses were estimated from observed 111In-ibritumomab tiuxetan residence times in the defined regions of interest (ROIs). Initially, the scans were obtained at 8 time points: shortly after injection, 2 h, 4–6 h, 1 d, 2 d, 3 d, 4–5 d, and 6 d after injection. Subsequently, the monitoring schedule was simplified by eliminating the 2-h, 2-d, and 4- to 5-d sampling points. Anterior and posterior images were acquired using a medium-energy collimator, a 256 × 1024 computer acquisition matrix, and photopeak settings of 172 and 247 keV with 15% windows. Examples of whole-body gamma-camera scans at 24, 72, and 120 h after administration of 111In-ibritumomab tiuxetan are displayed in Figure 1.

Whole-body gamma-camera scans at 24, 72, and 120 h after administration of 111In-ibritumomab tiuxetan. Radiolabeled antibody is evident in blood pool at 24 h (A), with tumor localization seen in abdominal mass, liver, and spleen at later time points (B and C).
Blood samples were also drawn immediately after 111In injection and at 7 additional time points, with the times corresponding to the scan times. The sampling schedule was later simplified to 5 sampling times by eliminating the 2-h, 2-d, and 4- to 5-d sampling points. In a subset of patients, blood samples were collected at 4 time points after 90Y-ibritumomab tiuxetan injection (30 min, 90 min, 18–24 h, and 5–7 d).
Organ radioactivity content was estimated from the geometric mean (GM) of anterior and posterior ROI counts. Correction for attenuation for individual organs was estimated using an average correction factor derived from the first 111In-ibritumomab tiuxetan administration whole-body count (before first urination). An 111In imaging standard was included in each whole-body scan to ensure gamma-camera electronics were stable and scan speed was correct.
The activity (A) in organ i at time t was calculated from GM counts of the organ region (GMi(t)) and the first whole-body count (GMwb(0)) as:
 Eq. 1 van Reenen et al. (9) showed this method to be accurate in the quantification of uptake in the spleen, liver, and whole-body remainder in experimental baboons, and it is assumed to provide a reasonable approximation for other organs.
Eq. 1 van Reenen et al. (9) showed this method to be accurate in the quantification of uptake in the spleen, liver, and whole-body remainder in experimental baboons, and it is assumed to provide a reasonable approximation for other organs.
The fraction of injected activity (FIA) in organ i at time t for 90Y, FIAi, 90Y(t), is computed as:
 Eq. 2 where Ai,111In(t) = activity of 111In measured in organ i at time t, λ111In = decay constant for 111In (0.0102 h−1), λ 90Y = decay constant for 90Y (0.0108 h−1), t = time after injection (h), and Ainj,111In = injected activity of 111In.
Eq. 2 where Ai,111In(t) = activity of 111In measured in organ i at time t, λ111In = decay constant for 111In (0.0102 h−1), λ 90Y = decay constant for 90Y (0.0108 h−1), t = time after injection (h), and Ainj,111In = injected activity of 111In.
The whole-body remainder was calculated by subtracting the combined activities of the lungs, liver, kidneys, spleen, and urinary bladder from the whole-body 90Y activity.
The FIA for specific organs and the whole-body remainder was plotted versus the imaging time (h). The data were fit to a function with the sum of exponentials depending on the degree of correlation. The area under the curve (AUC) was analytically determined and expressed as the residence time of the organ or the remainder tissue (10).
Residence times in red marrow were derived from blood time-activity curves following the method of Sgouros (11). Whole blood 111In concentration (μCi/mL) was measured, decay corrected to simulate 90Y concentration, and plotted as a function of the time of blood draw. The curve was fit with either a mono- or a biexponential function, which was then integrated to obtain cumulated activity per milliliter of blood (Ãb). The blood residence time (τblood) was then obtained by multiplying the Ãb times the blood volume/activity injected.
Red marrow residence time (τm) was then estimated as:
 Eq. 3
Eq. 3
The red marrow mass (mrm) used in the residence time calculation was derived from the phantom-specific marrow mass provided by MIRDOSE3, adjusted for ideal body weight using the following equation:
 Eq. 4 where reference red marrow mass is 1,120 g for an adult man and 1,050 g for an adult woman (12). The ideal body mass was calculated from Metropolitan Life Foundation tables using patient height and medium frame (13). The reference body mass is 70 kg for men and 58 kg for women.
Eq. 4 where reference red marrow mass is 1,120 g for an adult man and 1,050 g for an adult woman (12). The ideal body mass was calculated from Metropolitan Life Foundation tables using patient height and medium frame (13). The reference body mass is 70 kg for men and 58 kg for women.
Sacral image-based bone marrow dosimetry was also performed by measuring the FIA in a defined marrow region using serial whole-body images obtained after injection of 111In-ibritumomab tiuxetan (14). The sacral ROI was quantified in the same manner as that used for soft-tissue regions. The fraction of total-body red marrow mass included in these regions has been previously defined (15). The fractional value was converted to 90Y μCi/g red marrow and multiplied by the appropriate factor using the phantom-specific total-body marrow mass to determine the 90Y FIA for the total-body red marrow. The total-body red marrow residence times were calculated by determining the AUC of the FIA-versus-time curves.
Residence times for the lungs, liver, spleen, kidneys, urinary bladder contents, red marrow, and remainder tissue were entered into the MIRDOSE3 computer software program to calculate the estimated radiation absorbed dose to these specified organs per unit 90Y injected activity (mGy/MBq [cGy/mCi]). This value was multiplied by the total activity of 90Y-ibritumomab tiuxetan (MBq [mCi]) delivered to the patient to determine radiation absorbed dose (cGy). Dose projections made at clinical sites were based on the reference organ masses incorporated into MIRDOSE3. Spleen and liver radiation absorbed dose projections calculated in the central analysis were adjusted linearly on the basis of the difference between patient spleen and liver masses obtained from baseline CT scans and those in the standard adult male and female models.
Blood and plasma half-life and the AUC were calculated as follows.
The predicted 90Y FIA for whole blood and plasma for each patient was entered into an Excel worksheet (Microsoft, Redmond, WA) and analyzed separately using a noncompartmental logarithmic-linear regression fit of the data using the equation:
 Eq. 5 where λe is the total (effective) elimination rate constant and t is the time after injection.
Eq. 5 where λe is the total (effective) elimination rate constant and t is the time after injection.
Effective half-life (effective t1/2) was calculated as:
 Eq. 6
Eq. 6
Biological half-life (t1/2b) was calculated from the effective (λe) and physical (λp) rate constants as:
 Eq. 7
Eq. 7
The AUC, from t = 0 extrapolated to infinity, was calculated as:
 Eq. 8 where tlast is the time at which the last measurement-based FIA data point was obtained.
Eq. 8 where tlast is the time at which the last measurement-based FIA data point was obtained.
Urinary Clearance
Total urine volume was collected from patients during 7 consecutive days after ibritumomab tiuxetan RIT in 2 of the 4 clinical trials described here. Urinary clearance of 90Y was either estimated from urinary 111In activity after 5 mCi 111In-ibritumomab tiuxetan or directly measured after a therapeutic dose of 0.2–0.4 mCi/kg 90Y-ibritumomab tiuxetan.
Statistical Methods
Summary statistics (median and range) were generated for estimated 90Y radiation absorbed doses to organs using data from the central (ORAU) analysis. Statistics were based on 179 patients. Two types of statistical tests were used to examine possible correlations between dosimetric or pharmacokinetic parameters and safety parameters. The Kruskal-Wallis test (3 or more group comparisons) was used to identify significant differences in the median dosimetric or pharmacokinetic variables by clinical parameters. The Pearson correlation coefficient test was used to determine whether linear correlations existed between safety parameters (hematologic nadir and days to recovery) and dosimetric parameters (blood-derived marrow dose, sacral image-derived marrow dose, and total-body dose) or pharmacokinetic parameters (whole blood half-life and AUC).
RESULTS
Demographics
The patient population was 43% female and had a median age of 59 y (range, 24–85 y). The majority of patients (78%) had follicular NHL (International Working Formulation [IWF] B, C, D), 8% had small lymphocytic lymphoma (IWF A), and 6% were identified as having transformed NHL. Most patients (89%) were stage III or stage IV at study entry and the baseline World Health Organization performance status was 0 or 1 in 98% of patients. Eighty-seven patients (49%) had bone marrow involvement at baseline. More than half of the patients (53%) had tumors of ≥5 cm in maximum diameter. The median number of prior therapeutic regimens, including rituximab, was 2 (range, 1–9).
Organ and Bone Marrow Dosimetry
For each of the 179 patients undergoing ibritumomab tiuxetan dosimetry, projected radiation absorbed doses were below the protocol-defined upper limits of 3.0 Gy to red marrow and 20 Gy to normal organs. Radiation absorbed dose estimates are presented in Tables 2 and 3.
Organ Radiation Absorbed Dose (Gy) from 90Y
Organ Radiation Absorbed Dose Factor (mGy/MBq) from 90Y
Analyses were performed to estimate the radiation absorbed dose to red marrow based on both blood-derived and sacral image-derived methods. The median values for 90Y for all patients were 0.62 Gy (range, 0.06–2.21 Gy) for the blood-derived method and 0.97 Gy (range, 0.06–2.57 Gy) for the sacral image-derived method. The median value for the 111In radiation absorbed dose to bone marrow using the blood-derived method was 0.02 Gy. The median 90Y radiation absorbed dose was highest to the spleen: 7.42 Gy (range, 0.23–24.48 Gy). The median 111In radiation absorbed dose was also highest to the spleen, 0.15 Gy.
90Y-Ibritumomab Tiuxetan Pharmacokinetics
The median effective half-life for 90Y-ibritumomab tiuxetan in blood was 27 h (range, 14–44 h). The median biologic blood half-life of the antibody was 46 h (range, 18–140 h). The median residence time for 90Y-ibritumomab tiuxetan in blood was 26 h (Table 4). The median values for plasma effective half-life, biologic half-life, and AUC were similar to the corresponding median values for whole blood.
90Y Effective Half-Life, Biologic Half-Life, and 90Y AUC Derived from 111In Activity in Blood
Urinary Clearance
In the 2 studies in which urinary clearance was measured, the mean fraction ± SD of injected 90Y activity excreted in urine was 9.2% ± 3.2% and 11.5% ± 4.5% when estimated from 111In activity. The mean fraction of injected 90Y activity obtained through direct measurement of 90Y was 5.8% ± 1.6%.
Correlation of 90Y-Ibritumomab Tiuxetan Dosimetry and Pharmacokinetics with Hematologic Toxicity
Observed toxicity of 90Y-ibritumomab tiuxetan was primarily hematologic and reversible. Multiple analyses were performed to determine whether dosimetric or pharmacokinetic data correlated with hematologic toxicity. Dosimetric parameters analyzed included blood-derived red marrow radiation absorbed dose, sacral image-derived red marrow radiation absorbed dose, and total-body radiation absorbed dose. Pharmacokinetic parameters analyzed included 90Y effective half-life and AUC in blood. Hematologic parameters included hematologic nadir, nadir grade, and days to recovery for the ANC and platelets.
Dosimetric Parameters Versus Hematologic Nadir and Recovery
Tables 5 and 6 present the results of analyses examining correlations between hematologic toxicity and dosimetric parameters using the Kruskal-Wallis test, and Figure 2 presents the results of the Pearson correlation coefficient test. With 1 exception, no significant P values (P ≤ 0.05) were obtained. The single significant P value was noted in the correlation of total-body radiation absorbed dose and days to recovery for platelets (Kruskal-Wallis test); however, the data indicated that a higher body dose correlated with a shorter time to recovery (Table 6). This relationship is not considered clinically meaningful because a higher total-body radiation absorbed dose would be expected to result in a more prolonged recovery time.

Scattergrams with linear correlation analysis show no correlation between bone marrow radiation absorbed dose and hematologic nadir value.
Radiation Absorbed Dose vs. Hematologic Nadir Grade
Radiation Absorbed Dose vs. Hematologic Recovery
Similar results were obtained when correlation analyses were performed by individual dose group (11 MBq/kg [0.3 mCi/kg] and 15 MBq/kg [0.4 mCi/kg]).
Pharmacokinetic Parameters Versus Hematologic Toxicity
Table 7 presents the results of analyses examining correlations between hematologic toxicity and pharmacokinetic parameters using the Kruskal-Wallis test, and Figure 3 presents the results of the Pearson correlation coefficient test. None of these analyses produced significant P values.
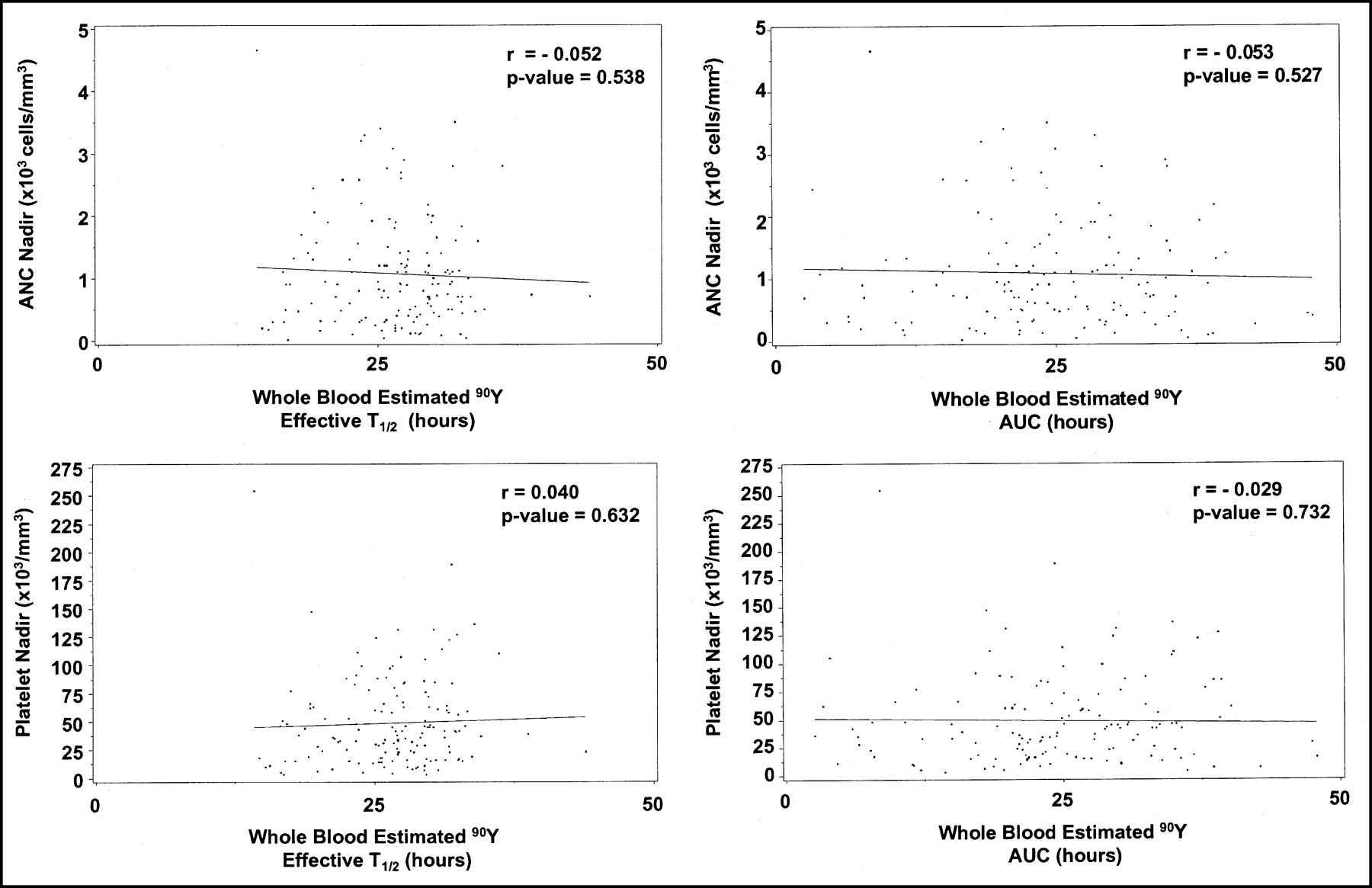
Scattergrams with linear correlation analysis show no correlation between pharmacokinetic parameters and hematologic nadir value.
Pharmacokinetic Parameters vs. Hematologic Nadir Grade
Similar results were obtained when correlation analyses were performed by individual dose group (11 MBq/kg [0.3 mCi/kg] and 15 MBq/kg [0.4 mCi/kg]).
Liver Dosimetry Versus Toxicity
The majority of patients in all studies had unchanged or improved liver and kidney function laboratory test values throughout the treatment and follow-up period. Because abnormalities occurred in so few patients, statistical analyses correlating chemistry parameters and liver and kidney radiation absorbed dose were not performed.
Six of 179 patients (3%) had a clinically significant shift from baseline in the liver chemistry values. All were documented by the investigator to be related to disease progression or preexisting conditions. The median radiation absorbed dose to the liver for these 6 patients was 4.15 Gy (range, 2.68–9.75 Gy), similar to the median (4.50 Gy) and range (0.64–18.56 Gy) for the population as a whole. Five patients had radiation absorbed doses to the liver of ≥12 Gy (range, 12–18.56 Gy), the highest of the range of calculated whole liver radiation absorbed dose estimates observed, and none exhibited abnormalities in liver function tests.
Kidney Dosimetry Versus Toxicity
The maximum estimated radiation absorbed dose to the kidneys was 0.76 Gy, and no renal dysfunction was observed.
DISCUSSION
Radiation dosimetry provides an estimate of the radiation absorbed doses from RIT to solid organs and red marrow. Dosimetry is critical during phase I and II trials of radiolabeled antibodies to determine biodistribution, establish a dosimetry database, and examine potential correlations between dosimetry parameters and clinical outcome within a defined patient population. Even outside of a clinical trial, dosimetry may be helpful to customize radiopharmaceutical administered doses for individual patients. This is particularly important if a radioimmunoconjugate has significant interpatient variability in urinary clearance, such as with 131I-labeled antibodies (16,17). Kaminski (16) reported urinary excretion rates of 46%–90% within 48 h of antibody administration. In the studies discussed in this article and in additional ibritumomab tiuxetan trials, interpatient variability was low with the SD <5% in all cases. In addition, in all studies evaluated, the mean level of urinary excretion in the first 7 d was also low, never exceeding 11%.
As techniques for accurately predicting bone marrow radiation absorbed dose evolve, dosimetry could potentially play a greater role in the use of RIT. However, as more experience is gained with a radiopharmaceutical, dosimetry evaluations may not be necessary in certain situations, just as pharmacokinetic assessments are not necessary in every patient treated with a chemotherapeutic or other therapeutic agent.
In 4 clinical trials of 90Y-ibritumomab tiuxetan RIT, dosimetry has provided valuable information in establishing a robust database of expected organ radiation absorbed doses. One hundred seventy-nine patients were required to undergo dosimetry evaluation before the therapeutic 90Y-ibritumomab tiuxetan administered dose was delivered.
The MTD for 90Y-ibritumomab tiuxetan was determined in a phase I/II nonmyeloablative dose-finding study conducted for patients with low-grade, intermediate-grade, or mantle-cell NHL (n = 50; 7.4–15 MBq/kg [0.2–0.4 mCi/kg]). Subsequently, patients with baseline platelet counts of ≥150,000 cells/mm3 were treated at the 15 MBq/kg (0.4 mCi/kg) level. This included all patients enrolled in a phase III randomized, controlled trial comparing rituximab with 90Y-ibritumomab tiuxetan and a phase III trial for patients with rituximab-refractory NHL. Patients with platelet counts of 100,000–149,000 cells/mm3 received a reduced administered dose of 11 MBq/kg (0.3 mCi/kg) in a phase II single-arm study. No patient was permitted to receive an administered dose of >1.2 GBq (32 mCi).
Treatment was allowed in these 4 studies, only if estimated organ radiation absorbed doses were below protocol-defined maximum limits (20 Gy to uninvolved organs, 3 Gy to red marrow). All 179 patients met these safety criteria to proceed to receive the therapeutic administered dose of 90Y-ibritumomab tiuxetan. The median radiation absorbed doses to critical organs were considerably below maximum limits: 7.42 Gy to spleen, 4.50 Gy to liver, 2.11 Gy to lungs, 0.23 Gy to kidneys, and 0.62 Gy to red marrow.
Initial estimates of the radiation absorbed dose calculated at the clinical site were used to determine whether the patient would proceed to 90Y-ibritumomab tiuxetan RIT. After treatment, a central analysis was performed where organ radiation absorbed dose estimates were recalculated at the Mayo Clinic and at ORAU. This allowed for a rigorous evaluation of the data and provided a consistent analysis of all patient radiation absorbed doses based on uniform assumptions and techniques.
For the most part, toxicity associated with 90Y-ibritumomab tiuxetan RIT was hematologic and reversible. Although mild abnormalities in liver function tests occurred in a few patients, these were also noted on the rituximab control arm of the randomized study and most were attributed to other causes (i.e., lymphoma, intravenous drug abuse, hepatitis, Gilbert syndrome). These patients had estimated radiation absorbed doses to the liver in the same range as the overall patient population. Lung and renal toxicity related to 90Y-ibritumomab tiuxetan was not observed.
Extensive analyses were performed to determine whether a correlation could be established between dosimetric or pharmacokinetic parameters and hematologic toxicity associated with 90Y-ibritumomab tiuxetan treatment. No clinically significant correlations could be established.
Both platelet and neutrophil counts were followed to assess acute hematologic toxicity because these parameters are most significantly affected by irradiation of blood and bone marrow. Several analyses were performed using different expressions of hematologic change that reflect severity of toxicity. The degree to which platelet and ANC values drop and the duration of time during which the levels remain low are of greatest concern. To that end, hematologic toxicity was assessed by the nadir value and by days to recovery of that value. Two types of statistical analyses were used to tease out possible correlations. In these studies, the Kruskal-Wallis test was used to group patients either by grade of nadir or by defined number of days to hematologic recovery. The Pearson correlation analysis further evaluated correlations seen among groups by treating the hematologic nadir and days to recovery as continuous variables. These approaches produced the following categories:
-
Patients grouped by grade of hematologic nadir
-
Hematologic nadir value evaluated as a continuous variable
-
Patients grouped by days to hematologic recovery
-
Days to hematologic recovery evaluated as a continuous variable
In turn, each of these evaluations was correlated with several different parameters. Dosimetric parameters included red marrow radiation absorbed dose and total-body radiation absorbed dose. Pharmacokinetic parameters included blood effective half-life and the AUC.
Dosimetric parameters were evaluated to determine whether they could serve as predictors of toxicity. Two different methods of calculating red marrow radiation absorbed dose were used: the blood-derived method and the sacral image-derived method. Although these methods of measuring red marrow radiation absorbed dose can predict hematologic toxicity in other situations, none of the analyses performed in this study of 179 patients produced clinically relevant correlations between hematologic toxicity and red marrow radiation absorbed dose.
In addition to red marrow radiation absorbed dose, total-body radiation absorbed dose was also tested as a predictor of hematologic toxicity. Again, none of the analyses produced clinically significant results. Total-body radiation absorbed dose has been suggested as a surrogate for red marrow and a replacement for organ dosimetry for other radiopharmaceuticals, particularly γ-emitters such as 131I, where the radionuclide targeting specific sites also emits penetrating radiation throughout the entire body. In contrast, 90Y-ibritumomab tiuxetan carries a β-emitting radionuclide; thus, emissions remain confined to targeted areas. Results of the analyses demonstrate that total-body radiation absorbed dose does not correlate with hematologic toxicity in this setting.
Finally, hematologic toxicity was analyzed in relation to traditional pharmacokinetic parameters of blood effective half-life and AUC. Again, no relevant correlation was noted between these pharmacokinetic parameters and platelet or neutrophil toxicity. In summary, both dosimetric and pharmacokinetic parameters were unable to serve as predictors of hematologic toxicity.
Sgouros et al. (18) have detailed complex patient factors that can contribute to inaccuracies in bone marrow radiation absorbed dose estimates and the resulting failure of red marrow dosimetry to predict hematologic toxicity. These include spatial relationship of bound radiolabeled antibody to the dose-limiting marrow stem cells, variable radiosensitivity within marrow cell populations, and interpatient variability in the bone marrow reserve. In addition, Bolch et al. (19) have reported on the value of including marrow cellularity in models designed to estimate bone marrow absorbed dose. In this patient population, variable loss of marrow function is common as a result of bone marrow damage from prior chemotherapy and external beam radiation therapy or from marrow involvement by NHL.
Another major limitation is that blood-derived red marrow dosimetry considers only radioactivity in the blood and is unable to account for the secondary irradiation of hematopoietic cells from radiopharmaceutical targeting of NHL within the marrow. In these studies of 90Y-ibritumomab tiuxetan, 49% of patients had bone marrow involvement with NHL. Thus, it is possible that blood-derived red marrow radiation absorbed dose calculations were underestimated in almost half of the patients.
Unlike the blood-derived method, sacral image-based red marrow dosimetry accounts for direct targeting of NHL within the bone marrow. However, it also has shortcomings. Red marrow radiation absorbed dose can be under- or overestimated because of the difficulty in separating sacral marrow regions of interest from overlying or adjacent lymphomatous adenopathy. This phenomenon was observed in a phase I/II 90Y-ibritumomab tiuxetan study (20). Juweid et al. (21) have also reported similar obstacles using sacral imaging techniques to estimate red marrow radiation absorbed dose from the radiolabeled anti-antibody.
Because of the many factors limiting the effectiveness of bone marrow dosimetry as confirmed by the extensive correlative analyses presented here, we conclude that currently available dosimetric and pharmacokinetic techniques cannot reliably predict which patients are at risk for severe hematologic toxicity in this defined population of relapsed or refractory NHL patients. This is confirmed by the extensive correlative analyses presented here. In the future, as internal radiation absorbed dose models improve and become more patient specific, dosimetry may provide more accurate estimates of bone marrow radiation absorbed dose and resulting toxicity. However, internal radiation treatment for other diseases, such as radioiodine therapy for thyroid malignancy, successfully relies on clinical parameters other than individualized dosimetry to ensure safety. This approach is now being taken with 90Y-ibritumomab tiuxetan. Six clinical studies performed on 306 patients have resulted in the development of an 90Y-ibritumomab tiuxetan weight-adjusted regimen associated with an acceptable safety profile. Patients enrolled in these trials were required to have adequate marrow reserve as follows:
-
Less than 25% bone marrow involvement with lymphoma by bone marrow biopsy
-
Baseline platelet count of ≥150,000 cells/mm3 (15 MBq/kg [0.4 mCi/kg] 90Y-ibritumomab tiuxetan) or 100,000–149,000 cells/mm3 (11 MBq/kg [0.3 mCi/kg] 90Y-ibritumomab tiuxetan)
-
No prior autologous bone marrow transplantation or peripheral blood stem cells
On the basis of the findings of these studies, 90Y-ibritumomab tiuxetan RIT is now administered without dosimetry at administered doses of 15 MBq/kg (0.4 mCi/kg) and 11 MBq/kg (0.3 mCi/kg) to patients who fit these screening requirements. Whereas dosimetry is no longer required in this defined patient population, dosimetry will continue to contribute to investigational studies expanding the role of 90Y-ibritumomab tiuxetan in NHL for myeloablative trials and for patients with extensive disease burden who do not meet established criteria. In addition, the role of dosimetry may change as internal radiation absorbed dose models are developed that can account for patient-specific differences.
CONCLUSION
90Y-Ibritumomab tiuxetan RIT delivers a safe range of estimated radiation absorbed doses to organs and red marrow. Toxicity, which is primarily hematologic and reversible, did not correlate with dosimetric or pharmacokinetic results, and these results could not be used to sort out patients who would be candidates for administered dose escalation or reduction. Therefore, baseline blood counts, indicative of marrow reserve in this heavily pretreated population, and the extent of marrow involvement remain parameters for patient selection for nonmyeloablative treatment. As a result of these findings, dosimetry is no longer required before 90Y-ibritumomab tiuxetan treatment for this defined patient population. Imaging is still included in the treatment regimen as a visual evaluation of biodistribution.
Acknowledgments
The authors sincerely thank the following investigators for participating in these studies: Gregory P. Adams, PhD; Nancy L. Bartlett, MD; Kirkman Baxter, MD; Thomas M. Beck, MD; Vincent Caggiano, MD; A. Cahid Civelek, MD; P. Duffy Cutler, PhD; Myron Czuczman, MD; Magnus Dahlbom, PhD; Delva Deauna-Limayo, MD; Robert O. Dillman, MD; Walter Drane, MD; William L. Dunn, MS; Christos Emmanouilides, MD; Louis Fehrenbacher, MD; Ian W. Flinn, MD; Stanley Goldsmith, MD; Leo I. Gordon, MD; Mark W. Groch, PhD; John Gutheil, MD; Michael Haseman, MD; John Hilton, MD; Robert S. Hurwitz, MD; Nalini Janakiraman, MD; Judith Joyce, MD; Robin M. Joyce, MD; Kastytis Karvelis, MD; Michael Katin, MD; Randolph Knific, MD; Brian Kraviski, MD; Dominick Lamonica, MD; Robert S. Lenobel, MD; John P. Leonard, MD; Richard L. Levy, MD; John Lister, MD; James W. Lynch, Jr., MD; Ruby F. Meredith, MD, PhD; Philip Moldofsky, MD; James L. Murray, MD; Daniel Navarro, MD; Donald Neumann, MD, PhD; J. Anthony Parker, MD; Brad L. Pohlman, MD; William Porter, PharmD; Andrew Raubitschek, MD; Henry Royal, MD; Alfred Saleh, MD; Mansoor Saleh, MD; Russell J. Schilder, MD; Timothy Schultheiss, PhD; Aldo N. Serafini, MD; Daniel H.S. Silverman, MD; Barry Skikne, MD; William Spies, MD; Lewis N. Terry, MD; Ray Thorpe, MD; Jean-Luc Urbain, MD, PhD; James Welsh, MD; Richard Wendt, PhD; and Michael Zimmer, PhD. The authors also thank the following individuals for assisting with this manuscript: Jerry Amberg; Richard Belanger, MS; Judy Berlfein; Shirley T. Vitas; Marci White; Margaret Whiteley; Christina Wong; and Charlie Zhang, PhD. Support for these trials has been provided by IDEC Pharmaceuticals Corporation, San Diego, California.
Footnotes
Received Dec. 31, 2001; revision accepted Oct. 24, 2002.
For correspondence or reprints contact: Gregory A. Wiseman, MD, Department of Diagnostic Radiology, Mayo Clinic, 200 First St., S.W., Rochester, MN 55905.
E-mail: gwiseman{at}mayo.edu
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- Biokinetics of Radiolabeled Monoclonal Antibody BC8: Differences in Biodistribution and Dosimetry Among Hematologic Malignancies
- Biodistribution and Dosimetry Results from a Phase 1 Trial of Therapy with the Antibody-Radionuclide Conjugate 177Lu-Lilotomab Satetraxetan
- Red Marrow-Absorbed Dose for Non-Hodgkin Lymphoma Patients Treated with 177Lu-Lilotomab Satetraxetan, a Novel Anti-CD37 Antibody-Radionuclide Conjugate
- Study of the Impact of Tissue Density Heterogeneities on 3-Dimensional Abdominal Dosimetry: Comparison Between Dose Kernel Convolution and Direct Monte Carlo Methods
- Treatment of Advanced Pancreatic Carcinoma with 90Y-Clivatuzumab Tetraxetan: A Phase I Single-Dose Escalation Trial
- Predicting Hematologic Toxicity in Patients Undergoing Radioimmunotherapy with 90Y-Ibritumomab Tiuxetan or 131I-Tositumomab
- Detection of 90Y Extravasation by Bremsstrahlung Imaging for Patients Undergoing 90Y-Ibritumomab Tiuxetan Therapy
- Radioimmunotherapy with yttrium-90-ibritumomab tiuxetan as part of a reduced- intensity conditioning regimen for allogeneic hematopoietic cell transplantation in patients with advanced non-Hodgkin lymphoma: results of a phase 2 study
- Arterial Wall Dosimetry for Non-Hodgkin Lymphoma Patients Treated with Radioimmunotherapy
- Dosimetry of 90Y-Ibritumomab Tiuxetan as Consolidation of First Remission in Advanced-Stage Follicular Lymphoma: Results from the International Phase 3 First-Line Indolent Trial
- Harnessing the Energy: Development of Radioimmunotherapy for Patients with Non-Hodgkin's Lymphoma
- Yttrium-90 Ibritumomab Tiuxetan Doses Calculated to Deliver up to 15 Gy to Critical Organs May Be Safely Combined With High-Dose BEAM and Autologous Transplantation in Relapsed or Refractory B-Cell Non-Hodgkin's Lymphoma
- MIRD Dose Estimate Report No. 20: Radiation Absorbed-Dose Estimates for 111In- and 90Y-Ibritumomab Tiuxetan
- Phase 1/2 study of fractionated 131I-rituximab in low-grade B-cell lymphoma: the effect of prior rituximab dosing and tumor burden on subsequent radioimmunotherapy
- High-Dose Yttrium-90-Ibritumomab Tiuxetan With Tandem Stem-Cell Reinfusion: An Outpatient Preparative Regimen for Autologous Hematopoietic Cell Transplantation
- Fully human monoclonal antibodies and targeted radionuclide therapy
- Evaluation of response to fractionated radioimmunotherapy with 90Y-epratuzumab in non-Hodgkin's lymphoma by 18F-fluorodeoxyglucose positron emission tomography
- High-Dose Radioimmunotherapy with 90Y-Ibritumomab Tiuxetan: Comparative Dosimetric Study for Tailored Treatment
- A Phase I Study of 90Yttrium-Ibritumomab-Tiuxetan in Children and Adolescents with Relapsed/Refractory CD20-Positive Non-Hodgkin's Lymphoma: A Children's Oncology Group Study
- Microscopic Intratumoral Dosimetry of Radiolabeled Antibodies Is a Critical Determinant of Successful Radioimmunotherapy in B-Cell Lymphoma
- Spatial Dose Mapping for Individualizing Radioiodine Treatment
- Bone Marrow Transplantation Nephropathy after an Intensified Conditioning Regimen with Radioimmunotherapy and Allogeneic Stem Cell Transplantation
- The Role of Imaging with 111In-Ibritumomab Tiuxetan in the Ibritumomab Tiuxetan (Zevalin) Regimen: Results from a Zevalin Imaging Registry
- Quantitative Immuno-Positron Emission Tomography Imaging of HER2-Positive Tumor Xenografts with an Iodine-124 Labeled Anti-HER2 Diabody
- Radioimmunotherapy of Non-Hodgkin's Lymphoma Revisited
- Dosimetry of Internal Emitters
- The Promise of Immuno-PET in Radioimmunotherapy
- Perspectives on Cancer Therapy with Radiolabeled Monoclonal Antibodies
- Bone Marrow Dosimetry Using Blood-Based Models for Radiolabeled Antibody Therapy: A Multiinstitutional Comparison
- Radioimmunotherapy of Non-Hodgkin's Lymphoma
- Radioimmunotherapy of Non-Hodgkin's Lymphoma with 90Y-DOTA Humanized Anti-CD22 IgG (90Y-Epratuzumab): Do Tumor Targeting and Dosimetry Predict Therapeutic Response?
- Underestimation of Absorbed Dose to Kidney