


Abstract
We reviewed 111In-DOTA-anti-CD45 antibody (BC8) imaging and bone marrow biopsy measurements to ascertain the biodistribution and biokinetics of the radiolabeled antibody and to investigate differences based on type of hematologic malignancy. Methods: Serial whole-body scintigraphic images (4 time points) were obtained after infusion of the 111In-DOTA-BC8 (176–406 MBq) into 52 adult patients with hematologic malignancies (lymphoma, multiple myeloma, acute myeloid leukemia, and myelodysplastic syndrome). Counts were obtained for the regions of interest for spleen, liver, kidneys, testicles (in men), and 2 marrow sites (acetabulum and sacrum), and correction for attenuation and background was made. Bone marrow biopsies were obtained 14–24 h after infusion, and the percentage of administered activity was determined. Absorbed radiation doses were calculated. Results: Initial uptake in liver averaged 32% ± 8.4% (SD) of administered activity (52 patients), which cleared monoexponentially with a biologic half-time of 293 ± 157 h (33 patients) or did not clear (19 patients). Initial uptake in spleen averaged 22% ± 12% and cleared with a biologic half-time of 271 ± 185 h (36 patients) or longer (6 patients). Initial uptake in kidney averaged 2.4% ± 2.0% and cleared with a biologic half-time of 243 ± 144 h (27 patients) or longer (9 patients). Initial uptake in red marrow averaged 23% ± 11% and cleared with a biologic half-time of 215 ± 107 h (43 patients) or longer (5 patients). Whole-body retention half-time averaged 198 ± 75 h. Splenic uptake was higher in the AML/MDS group than in the lymphoma group (P ≤ 0.05) or the multiple myeloma group (P ≤ 0.10). Liver represented the dose-limiting organ. For liver uptake, no significant differences were observed among the 3 malignancy groups. Average calculated radiation absorbed doses per unit of administered activity for a therapy infusion of 90Y-DOTA-BC8 were 0.35 ± 0.20 cGy/MBq for red marrow, 0.80 ± 0.24 cGy/MBq for liver, 3.0 ± 1.4 cGy/MBq for spleen, 0.055 ± 0.014 cGy/MBq for total body, 0.21 ± 0.15 cGy/MBq for osteogenic cells, and 0.17 ± 0.15 cGy/MBq for kidneys. Conclusion: 111In-DOTA-BC8 had a long retention time in liver, spleen, kidneys, and red marrow, and the highest absorbed doses were in spleen and liver. Few differences were observed by malignancy type. The exception was greater splenic uptake in the leukemia/MDS group than in the lymphoma or multiple myeloma group.
Radiolabeled monoclonal antibodies approved for treating patients with B-cell non-Hodgkin’s lymphomas have shown both safety and efficacy. These radiopharmaceuticals include ibritumomab tiuxetan (Zevalin; Acrotech Biopharma), which is a 90Y-labeled anti-CD20 monoclonal antibody (1), and tositumomab (Bexxar; GlaxoSmithKline), which is a 131I-labeled anti-CD20 monoclonal antibody (2,3). Since some lymphomas do not express CD20 antigens, the possibility of targeting other antigens has been investigated. Also, some lymphomas that express CD20 may have been modulated by prior extensive exposure to rituximab, therefore exhibiting a decreased response to radioimmunotherapy using anti-CD20 antibodies (4). One such potential monoclonal antibody currently being assessed in clinical trials is BC8, a murine anti-CD45 IgG1 antibody (binding to all CD45 isoforms) that is conjugated with the DOTA chelate (also known as tetraxetan) for binding the radiotracers 90Y and 111In. The CD45 antigen can be found on all hematopoietic cells except mature erythrocytes and platelets.
Both 90Y-DOTA-BC8 and 131I-BC8, directly labeled with iodine, were used in several clinical trials as part of the conditioning regimen before hematopoietic stem cell transplantation (5–10). 111In-DOTA-BC8 was used as a low-activity tracer surrogate for 90Y-DOTA-BC8 to facilitate quantitative imaging for projecting required therapeutic doses.
We report here the biodistribution and dosimetry data obtained from 4 clinical trials using low tracer levels of 111In-DOTA-BC8 before high-dose 90Y-DOTA-BC8 for radioimmunotherapy. We assumed that both indium-labeled and yttrium-labeled conjugates behaved similarly in the same patient. We then looked for differences in radiolabeled antibody biodistribution among patients with different types of hematologic malignancies: lymphoma versus multiple myeloma and acute myeloid leukemia (AML)/myelodysplastic syndrome (MDS). We also looked at 2 potential differences in biodistribution using 2 different antibody BC8 concentrations (0.5 vs. 0.75 mg/kg).
MATERIALS AND METHODS
Patient Population
The clinical studies were approved by the Fred Hutchinson Cancer Research Center Institutional Review Board for protocols 2728, 2450, 2468, and 2361, and written informed consent to participate was obtained from each patient.
Fifty-two patients with hematologic malignancies (lymphoma, multiple myeloma, AML, or MDS) from among 4 separate clinical trials were included in our analysis for biodistribution assessment and dosimetry. Of the 21 patients with lymphoma included in our analysis, there were 18 patients with aggressive forms of lymphoma (8 with diffuse large B-cell lymphoma, 1 with intermediate features between diffuse large B-cell lymphoma and Burkitt lymphoma, 4 with mantle cell lymphoma, 4 with Hodgkin’s lymphoma, and 1 with peripheral T-cell lymphoma) and 3 patents with an indolent type of lymphoma (follicular lymphoma).
Radioimmunotherapy was added as part of the conditioning regimen before hematopoietic stem cell transplantation to reduce the side effects of classic high-dose conditioning therapy. Table 1 shows the patient population by clinical protocol. Patient demographics are summarized in Table 2.
Clinical Protocol and Characteristics
Patient Demographic Data
Study Design
The anti-CD45 mAb BC8 was produced in the Biologics Production Facility (Fred Hutchinson Cancer Research Center) in high purity under current good-manufacturing-practice conditions, as previously described (11). Patient serum was tested for the presence of human antimouse antibody using an enzyme-linked immunosorbent assay before infusion of 111In-DOTA-BC8 and 90Y-BC8-DOTA. Patients in two of the clinical trials (2450 [multiple myeloma] and 2468 [AML/MDS]) received an antibody concentration (radiolabeled DOTA-BC8) of 0.5 mg/kg. A protein concentration of 0.75 mg/kg was used for lymphoma patients (trials 2728 and 2361); this concentration was based on antibody dose-escalation results from a previous trial of 131I-BC8 in lymphoma that used a protein-escalation schema and sought to optimize the protein dose of BC8 (12).
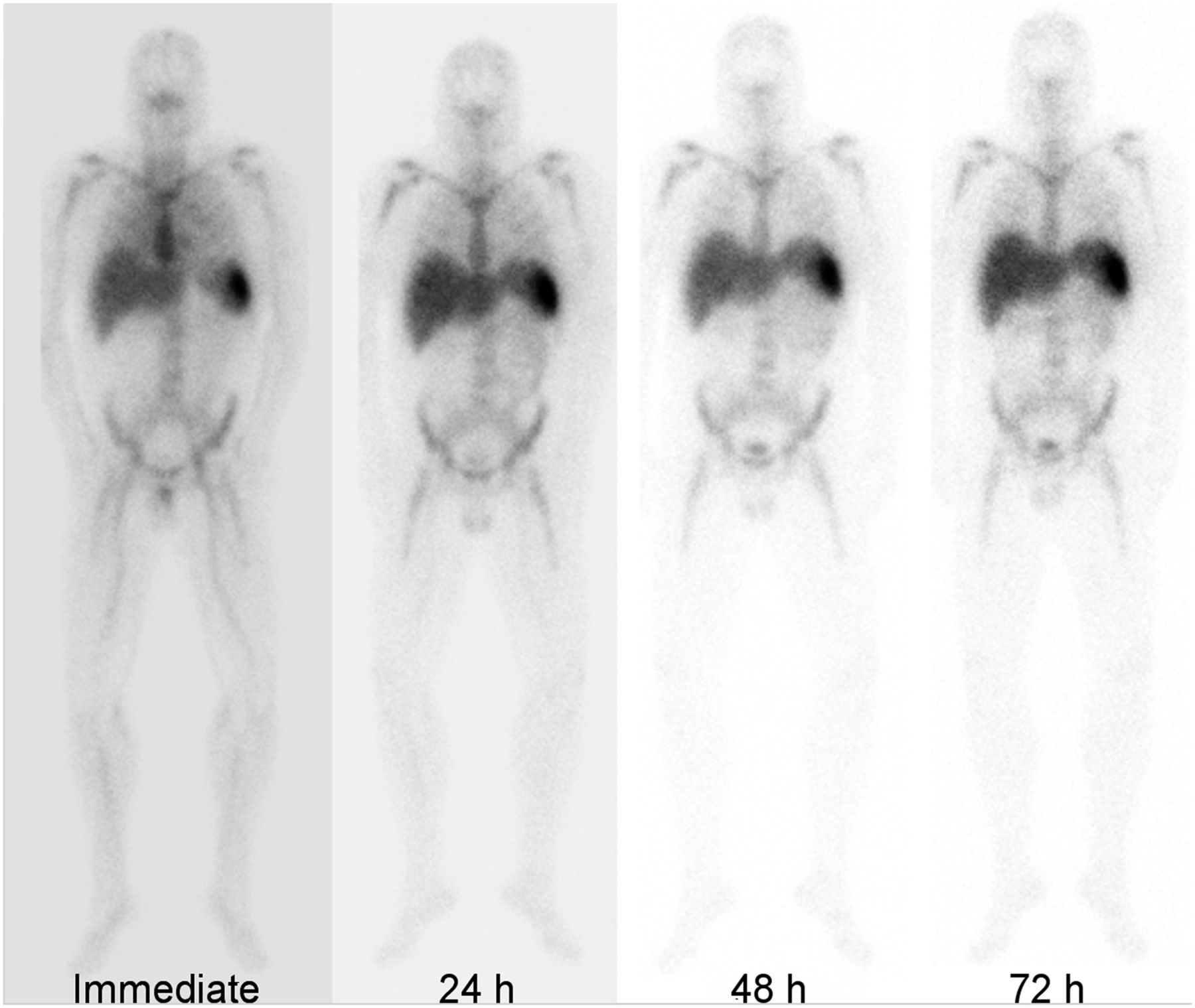
111In-DOTA-BC8 (185–370 MBq [5–10 mCi]) was administered at the rate of 7.5 mg/h after premedication with acetaminophen, diphenhydramine, and hydrocortisone. To determine radiolabeled antibody biodistribution kinetics, 4-time-point whole-body planar anterior and posterior γ-camera images were obtained at the end of infusion (hour 0) and on the subsequent 3 d (usually 24, 48, and 72 or 120 h) using a Philips Brightview XCT camera with medium-energy collimators (Fig. 1). Acquired count data were corrected for attenuation and radioactive decay against a known counting standard. Organ volumes (liver, lungs, spleen, and kidney) were calculated from CT images for correcting the standard organ volumes (13,14).
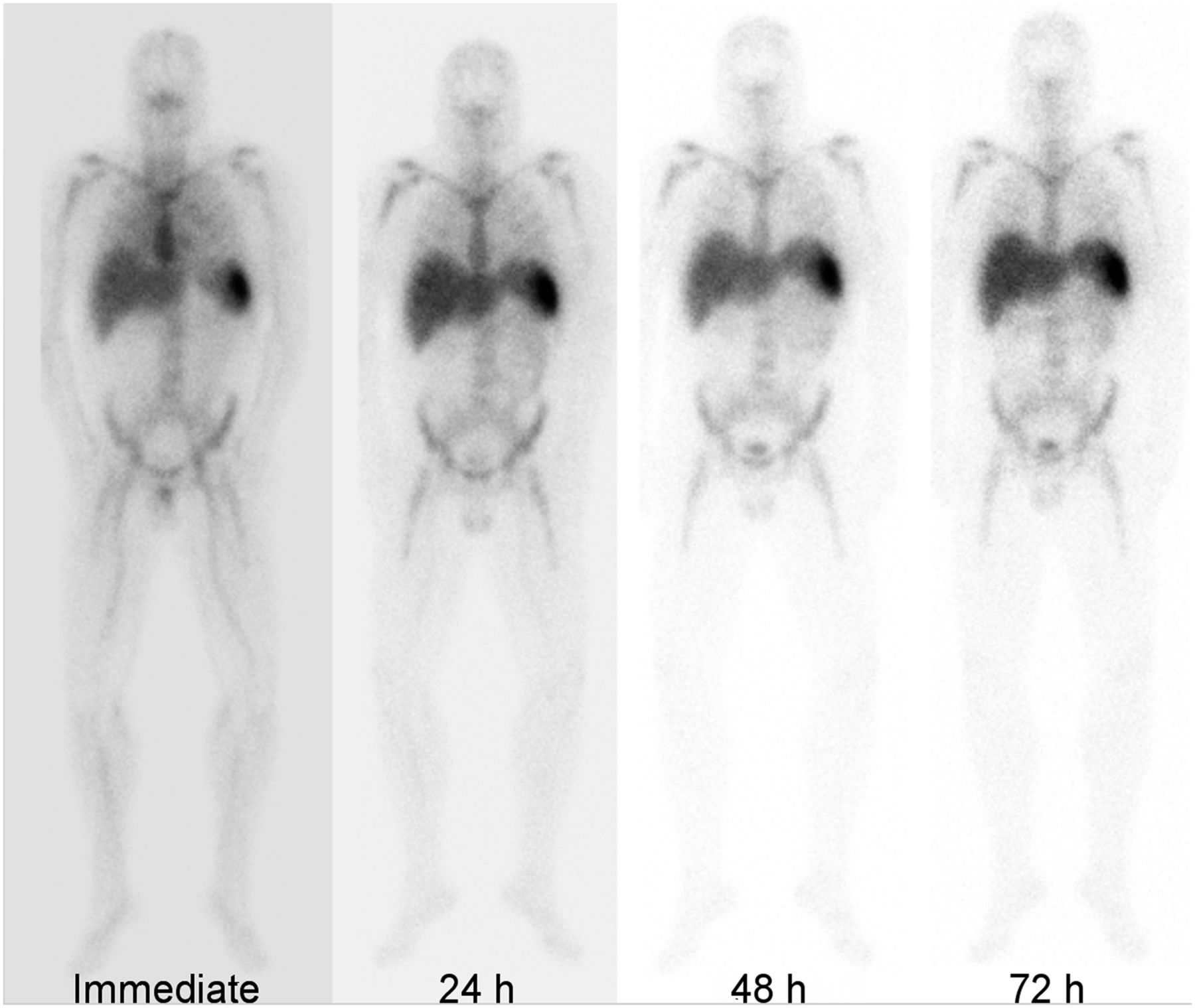
Whole-body anterior planar images of patient with B-cell non-Hodgkin’s lymphoma after injection of low activity of 111In-DOTA-BC8 for dosimetric calculations before treatment with 90Y-DOTA-BC8.
To determine the uptake and retention of radiolabeled antibody, regions of interest were drawn over the major imageable source organs, including 2 marrow sites (right or left acetabulum and sacrum), spleen, liver, and kidneys using the 180° opposing-view quantitative planar technique as described by Eary et al. (15) and shown in Figure 2. Initial uptake and biologic retention half-times were determined from fitting mathematic functions (usually a single exponential) to the time–activity data. The best-fit functions were integrated to determine the time-integrated activity coefficients.
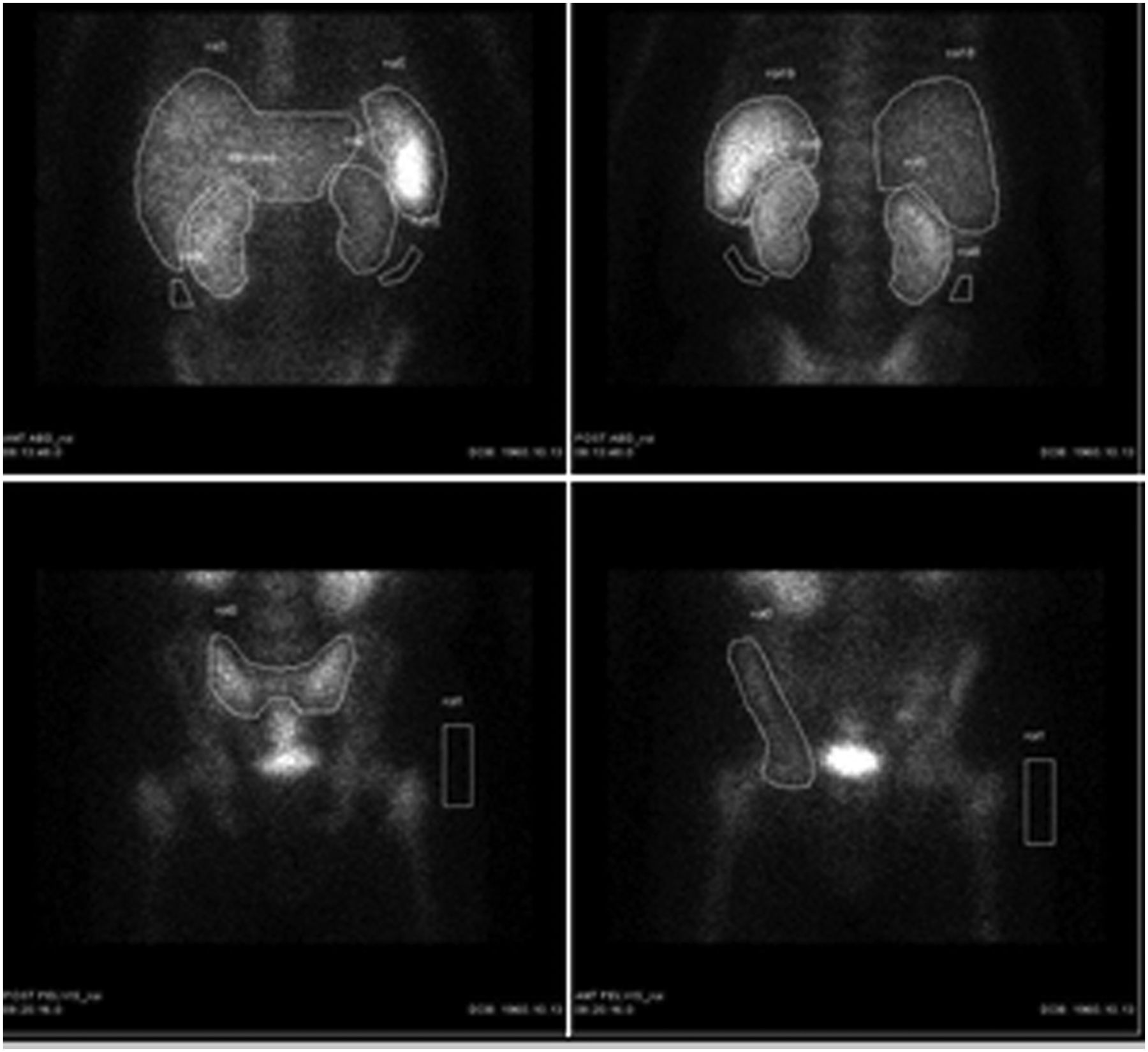
Imaging for dose calculation. Counts were obtained from regions of interest drawn over liver, spleen, and kidneys on anterior (A and D) and posterior (B and C) planar 111In-DOTA-BC8 images and used for dosimetry estimations together with counts per gram of tissue obtained from measurement of bone marrow biopsy specimen.
A bone marrow biopsy was obtained at approximately 24 h after the end of infusion, and the biopsy sample was weighed and counted against a weighed reference aliquot (counting standard) of the administered 111In activity to calculate the percentage administered activity per gram in marrow at the time of biopsy. The bone marrow biopsy results were then used as calibration points to quantitate the radioactivity observed in red marrow.
Images and bone marrow biopsy results obtained after 111In-DOTA-BC8 administration were used to calculate radiation absorbed doses to normal organs and tissues, including marrow. For calculation, methods recommended by the special committee on Medical Internal Radiation Dose (MIRD) of the Society of Nuclear Medicine and Medical Imaging were applied to obtain radiation dose per 90Y nuclear transformation for each organ, including self-organ and cross-organ energy contributions and, ultimately, the absorbed dose to target organs of the body per unit of administered activity (cGy/MBq). Reported dosimetry for the marrow, spleen, liver, other nontarget organs, and the whole body delivered per MBq of 90Y-DOTA-BC8 (cGy/MBq) is presented in Table 3. Differences in biodistribution based on the type of disease were also assessed. Calculated therapy activity for 90Y-DOTA-BC8 was based on maximizing radiation dose to the critical limiting normal nontarget organ (usually liver) starting at 10 Gy for all patients to a level that would not exceed normal-organ toxicity, escalating the maximum normal-organ dose by 2 Gy per group. For example, for a multiple myeloma patient, the estimated dose to the liver (the dose-limiting organ), was 0.98 cGy/MBq (36.1 cGy/mCi). For a desired therapy dose of 26 Gy to the dose-limiting organ, the calculated 90Y activity was 2,650 MBq (72 mCi).
Calculated Absorbed Doses per Unit of Administered Activity for 90Y-DOTA-BC8 in Selected Target Organs
We then looked at clinical outcomes for patients with high-risk lymphoma (8), AML/MDS (9), and multiple myeloma (10).
RESULTS
Initial Uptake of 111In-Labeled-BC8
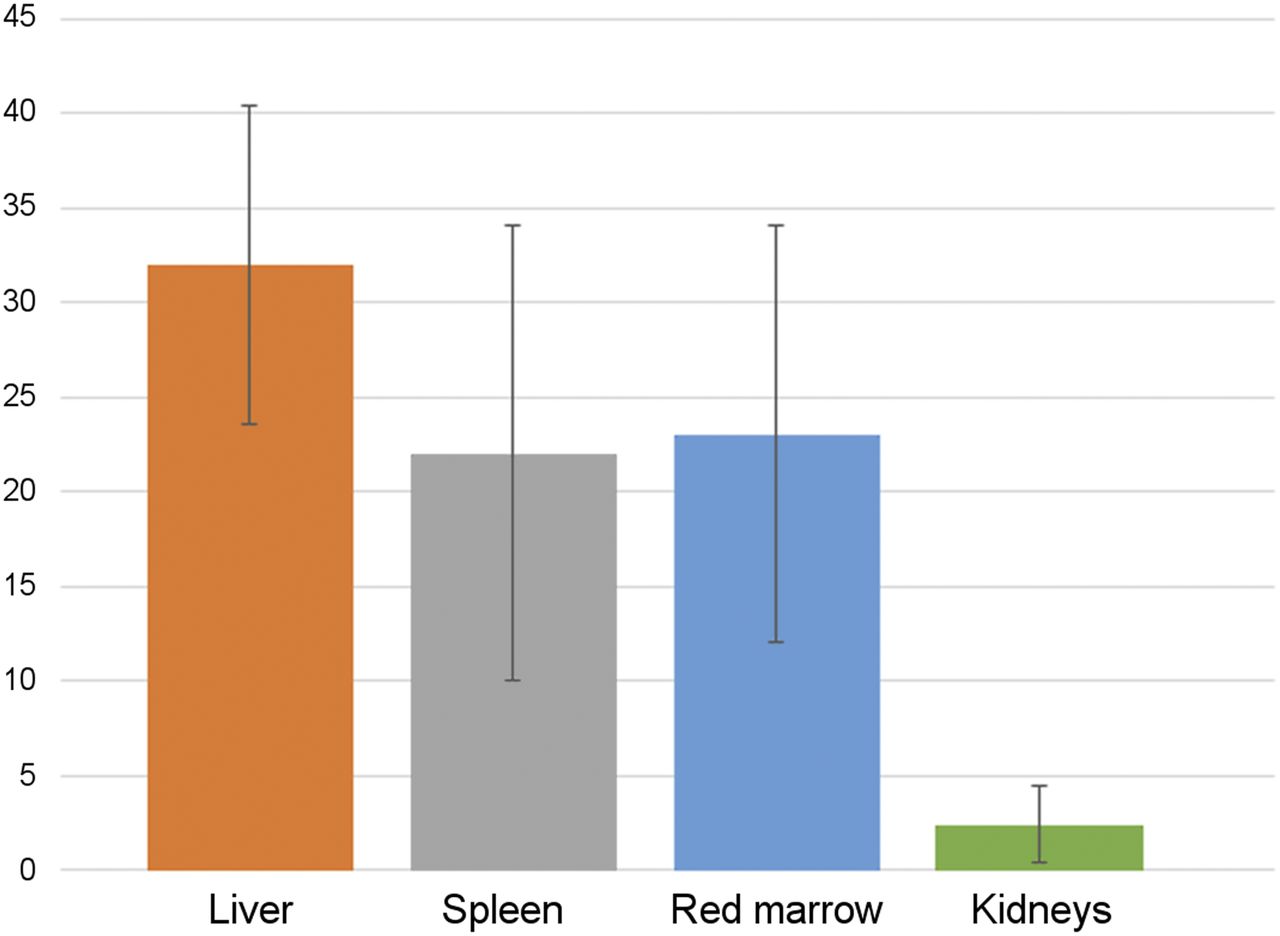
Initial uptake of 111In-DOTA-BC8 in liver averaged 32% ± 8.4% of administered activity (52 patients). The radioimmunoconjugate cleared from liver monoexponentially with a biologic half-time of 293 ± 157 h (33 patients) or longer to infinity (19 patients). Initial uptake in spleen averaged 22% ± 12% and cleared with a biologic half-time of 271 ± 185 h (36 patients) or longer (6 patients). Initial uptake in kidney was 2.4% ± 2.0% and cleared with a biologic half-time of 243 ± 144 h (27 patients) or longer (9 patients). Initial uptake in red marrow was 23% ± 11% and cleared with a biologic half-time of 215 ± 107 h (43 patients) or longer (5 patients) (Fig. 3). Whole-body biologic retention half-times averaged 198 ± 75 h. The radiolabeled 111In-DOTA-BC8 was tenaciously retained in major source organs and the whole body. In some patients, no biologic clearance was observed.
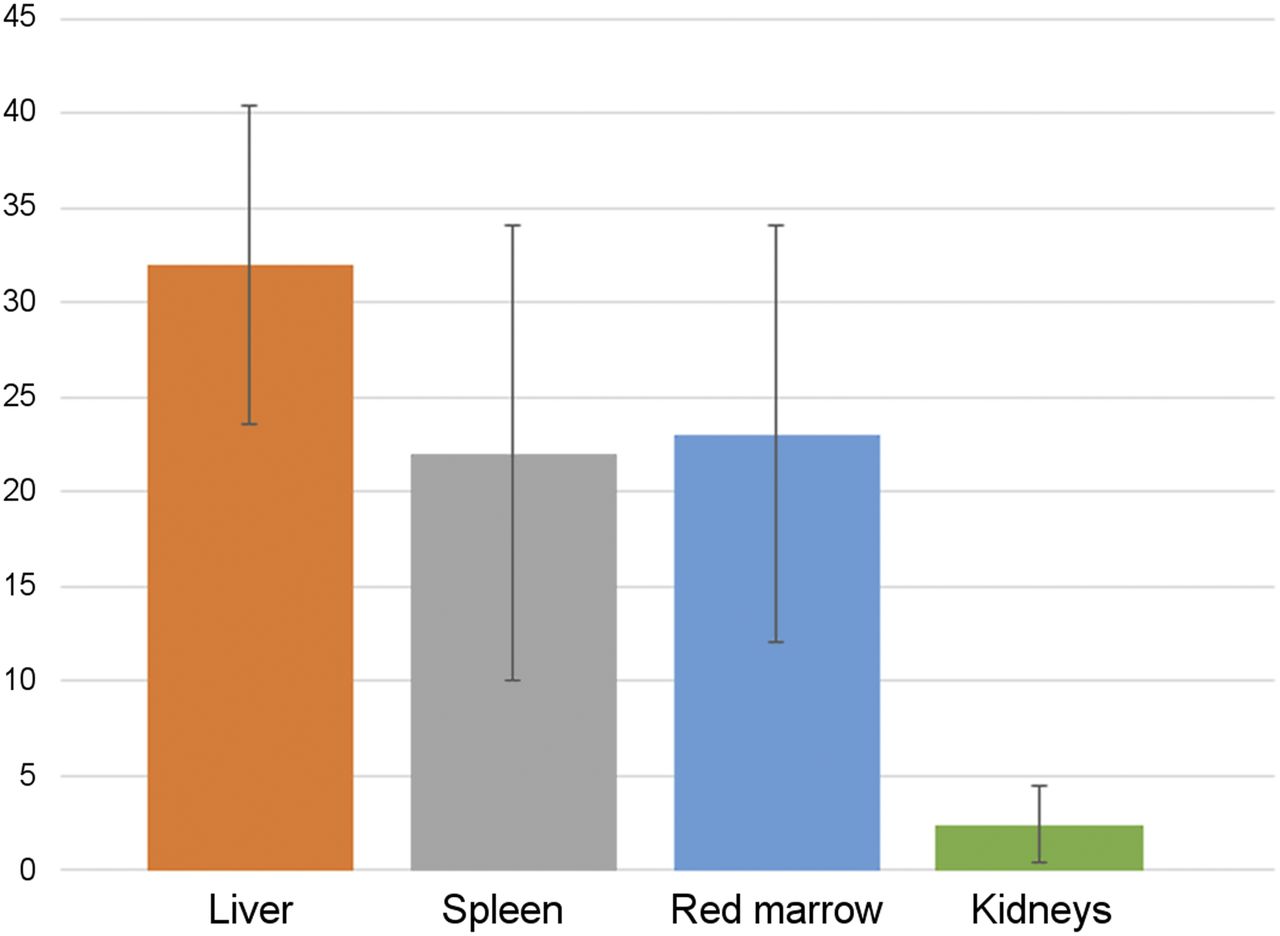
Chart illustrating initial percentage of administered activity taken up initially by the liver, spleen, red marrow, and kidneys.
Radiation Absorbed Doses
We calculated radiation absorbed doses per unit of administered activity of 90Y-DOTA-BC8 from analysis of the 111In-DOTA-BC8 serial planar imaging data and bone marrow radioactivity measurements: 0.35 ± 0.20 cGy/MBq for red marrow, 0.80 ± 0.24 cGy/MBq for liver, 3.0 ± 1.4 cGy/MBq for spleen, 0.055 ± 0.014 cGy/MBq for total body, 0.21 ± 0.15 cGy/MBq for osteogenic cells, and 0.17 ± 0.15 cGy/MBq for kidneys (Table 3; Fig. 4).
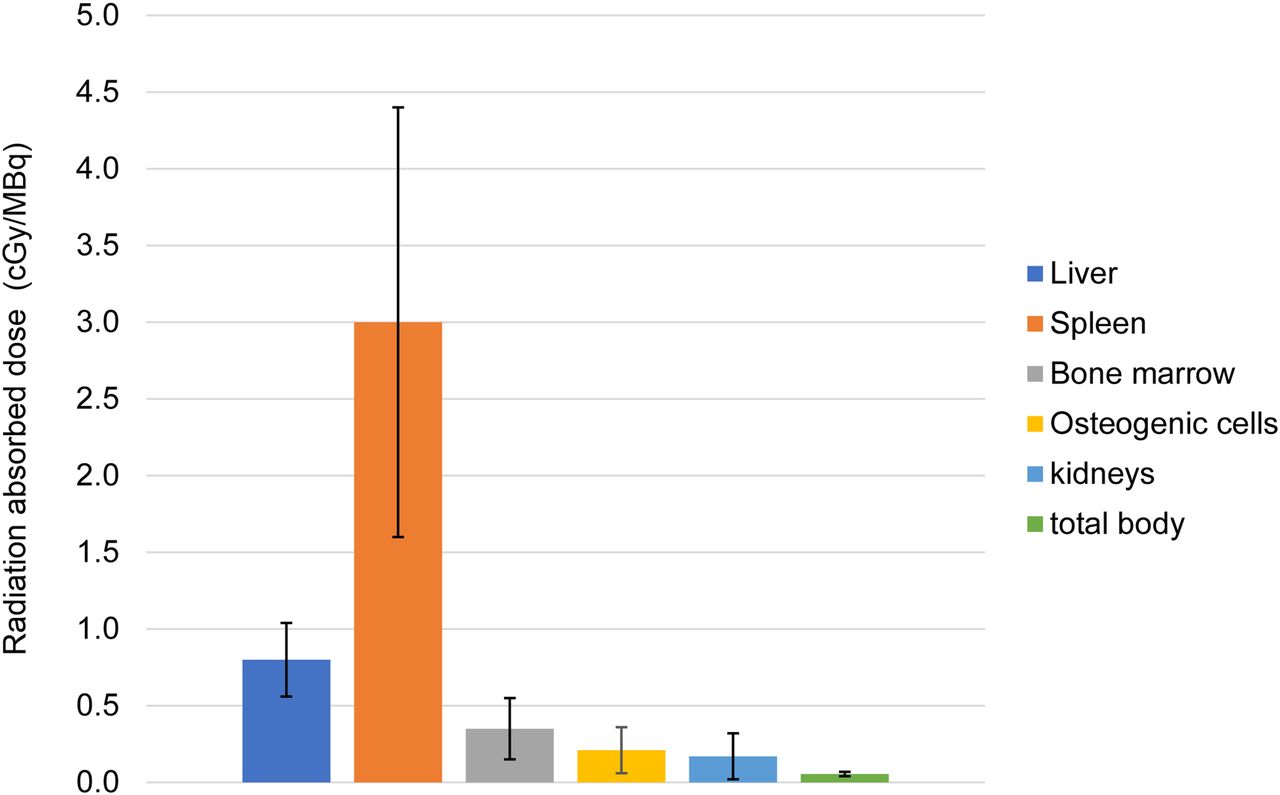
Absorbed doses per unit of administered activity (cumulative data for all groups of patients). Liver was dose-limiting normal organ in all patients; maximum dose to liver was 32 Gy for multiple myeloma and lymphoma groups and 28 Gy for AML/MDS group. No dose-limiting toxicities were observed.
Differences Among Different Groups of Hematologic Diseases
Initial Uptake
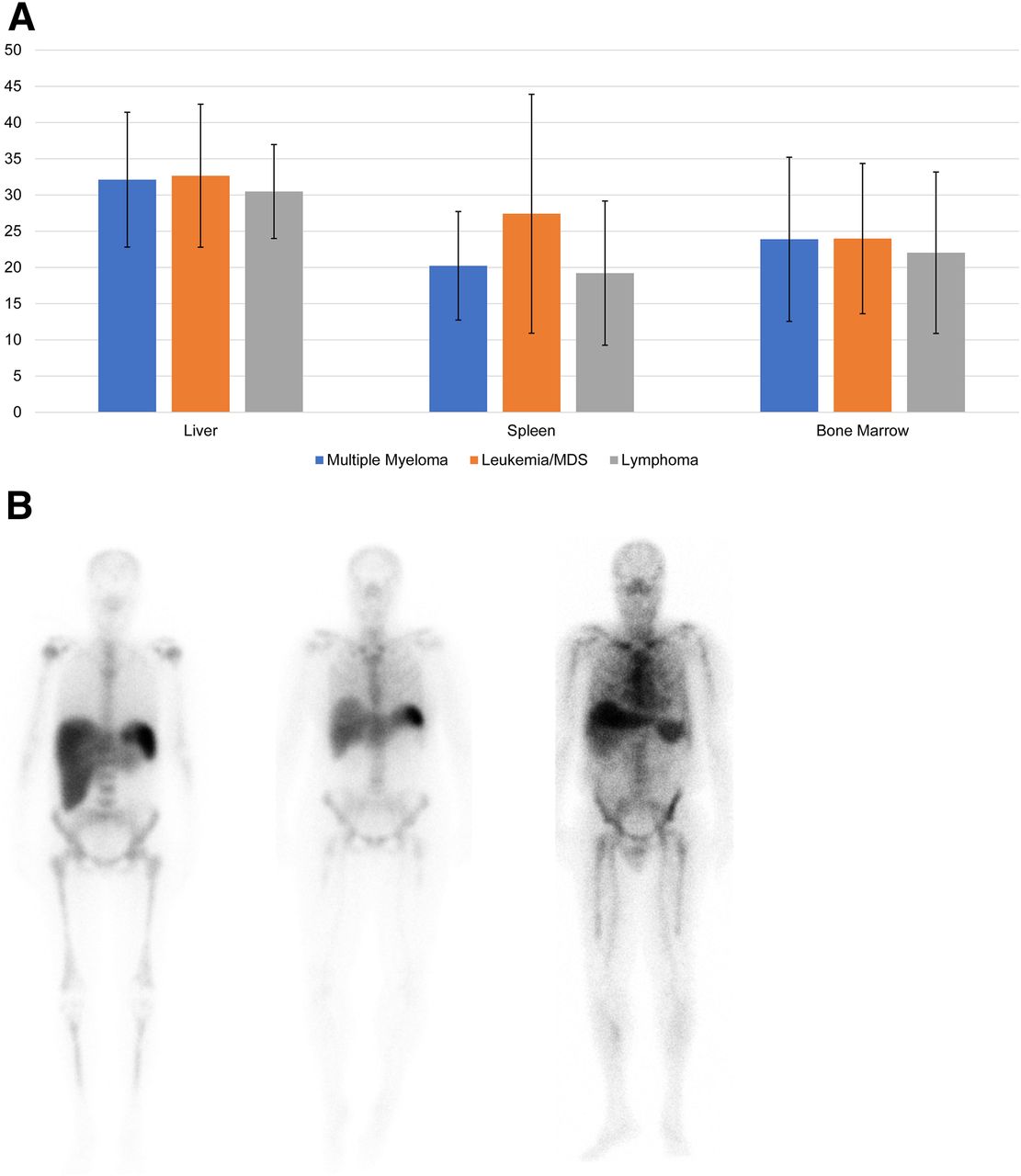
Further analysis of differences in biodistribution based on the patient’s disease (lymphoma vs. multiple myeloma vs. AML/MDS) showed a statistical significantly higher initial splenic uptake in the AML/MDS group than in the lymphoma group (P ≤ 0.05) or multiple myeloma group (P ≤ 0.1). At the P ≤ 0.10 level of significance, we observed no significant differences in initial liver uptake or bone marrow uptake among the 3 groups (Fig. 5).

(A) Percentage of initial uptake for patient groups. Initial splenic uptake was higher in AML/MDS group than in lymphoma group (P ≤ 0.05) or multiple myeloma group (P ≤ 0.1). No significant intergroup differences were observed for initial liver uptake or bone marrow uptake (P ≤ 0.10). (B) Anterior whole-body images obtained immediately after 111In-DOTA-BC8 infusion (time 0: initial uptake) in 3 different patients: 1 with AML (A), 1 with multiple myeloma (B), and 1 with diffuse large B-cell lymphoma (C). Although for liver there were no significant differences in initial uptake, lower radiation dose (at P ≤ 0.1) was found for AML/MDS group than for other 2 groups (probably because radiation absorbed dose is inversely proportional to mass).
Radiation Absorbed Dose
For the liver, at the P ≤ 0.10 level of significance, we did not observe significant differences between the multiple myeloma and lymphoma groups; however, we observed a lower liver radiation dose for AML/MDS patients than for multiple myeloma patients (P ≤ 0.1) or lymphoma patients (P ≤ 0.10) (Fig. 6).

Differences in radiation absorbed dose among groups. In spleen, dose was higher for multiple myeloma group than for lymphoma group (P ≤ 0.05), and in bone marrow, dose was higher for AML/MDS group than for lymphoma group (P ≤ 0.05).
For the spleen, at the P ≤ 0.05 level of significance, we observed differences between the multiple myeloma and lymphoma groups. At the P ≤ 0.10 level of significance, we observed differences between the multiple myeloma and AML/MDS groups. However, we did not see significant differences between the AML/MDS and lymphoma groups (P ≤ 0.01) (Fig. 6).
For the red marrow, at the P ≤ 0.05 level of significance, we did see significant differences between the AML/MDS and lymphoma groups. We did not observe significant differences between the multiple myeloma and AML/MDS groups or between the multiple myeloma and lymphoma groups at the P ≤ 0.10 level of significance (Fig. 6).
Differences Based on Protein Concentration Administered
We also compared the biodistribution of radiolabeled antibody in patients who received 0.5 mg/kg (multiple myeloma and AML/MDS groups) and patients who received 0.75 mg/kg (lymphoma group) (Figs. 7A and 7B). At the P ≤ 0.10 level of significance, we did not observe differences in initial uptake by liver or marrow, but we did observe a greater splenic uptake for the group that received 0.5 mg/kg (multiple myeloma plus AML patients) than for the group that received 0.75 mg/kg (lymphoma patients).

Differences in initial uptake and radiation absorbed dose based on protein concentration (0.5 vs. 0.75 mg/kg). (A) Statistical significance was not reached (P > 0.05) for differences in initial uptake in liver, spleen, or bone marrow. (B) No significant differences based on protein concentration were obtained for radiation dose absorbed by liver (which was critical limiting nontarget organ for all patients).
Regarding the radiation absorbed dose at the P ≤ 0.05 level of significance, we did find significant differences in protein concentration (0.5 vs. 0.75 mg/kg) between dose to spleen and dose to marrow (cGy/MBq administered), but we found no significant differences at the P ≤ 0.10 level for dose to liver. Therefore, protein concentration did not influence the liver dose.
DISCUSSION
Preclinical studies on the biodistribution of radiolabeled anti-CD45 were published previously (16). For example, the biodistribution of 90Y-labeled anti-CD45 antibody was demonstrated in a nonhuman primate model (macaques), a model that also predicted 131I-labeled anti-CD45 antibody biodistribution in humans (17). The results showed that the 90Y-labeled anti-CD45 antibody BC8 can deliver relatively selective radiation to hematopoietic tissues, with similar ratios of radiation delivered to target versus nontarget organs, as compared with the 131I-immunoconjugate in the same animal model. Another study, performed on mice, used 30F11, an antibody with a slightly different structure (rat anti-CD45 antibody IgG2b) (18). Targeting with 30F11 also showed a favorable biodistribution, with effectively targeted bone, marrow, and spleen and minor uptake in nonhematologic organs. In humans, prior studies with anti-CD45 antibody were performed, either with a 90Y-conjugated rat IgG2a monoclonal antibody (YAML568) or with a murine anti-CD45 IgG1 antibody (BC8).
Given that 90Y is a pure β-emitting radioisotope, in our clinical studies a different radiotracer (111In bound to DOTA-BC8) was used as a surrogate to determine the 90Y-antibody biodistributions needed to calculate internal radiation doses as previously performed with other radiolabeled antibodies (19,20). After the dosimetry step was performed using 111In-DOTA-BC8, the patients received a treatment dose calculated by escalating the maximum normal organ doses by 2 Gy per group. The maximum dose received by the dose-limiting normal organ was set at 32 Gy for the multiple myeloma group (14 patients) and the lymphoma group (19 patients) and 28 Gy for the AML/MDS group (15 patients) (21). No dose-limiting toxicities were observed. One patient from the multiple myeloma group and 1 from the AML/MDS group did not receive treatment because human antimouse antibodies developed after the tracer (low-level)-labeled imaging dose of 111In-BC8 was given. One subject from the lymphoma group had grade 4 hypotension during and after infusion.
Dosimetry showed that the radiolabeled antibody (111In-DOTA-BC8) was retained with a very long or infinitely long biologic retention half-time (corrected for physical decay of 111In) in liver, spleen, red marrow, and kidneys, with the highest doses being in spleen and liver. The long biologic retention half-times (approaching 10 days and longer) resulted in a more efficient delivery of radiation to the patient, because decay occurred in vivo rather than after excretion. Long biologic retention times were common to all patients from the 4 studies included in this analysis. The reason for this behavior is unknown but is probably due to the fact that the 111In remains conjugated to the antibody and is not metabolized or catabolized. This finding was not seen in the animal model when AC8 or 30F11 was used, nor was it seen in clinical studies when biodistribution of radiolabeled anti-CD20 antibody (111In-ibritumomab) was determined (20,22,23) or when radiolabeled andi-CD45 antibody 131I-BC8 or YAML568 dosimetric calculations were made (24,25). We could achieve desired doses to the nontarget limiting organ (liver in all patients) of 32 Gy for multiple myeloma patients and 28 Gy for AML/MDS and lymphoma patients without dose-limiting toxicity seen. Also, our results showed a higher calculated radiation dose to liver than to bone marrow—a finding that was not seen on preclinical studies or clinical studies that used 111I-BC8 or YAML568. For instance, when 90Y-AC8 antibody was used in preclinical studies, the delivered estimated radiation absorbed doses were 5–7 times higher to spleen and 2–4 times higher to marrow than to lungs or liver (17). However, the murine antihuman antibody used (BC8) has a structure that differs from the murine anti-CD45 antibody, called 30F11, and the nonhuman primate anti-CD45 called AC8. This difference might be explained by the differences in antibody structure or in species (18). Another potential explanation is the changes in biodistribution that are known to occur when cold antibody is not used before administration of the labeled one. Addition of supplemental unlabeled antibodies was shown to be necessary to achieve optimal biodistribution when another anti-CD45 monoclonal antibody with a structure different from BC8, called YAML568, was used (26). However, the unlabeled antibodies were not given in these 4 clinical trials because, in humans, prior biodistribution studies using 131I-BC8 without a preloading dose of unlabeled antibodies showed a favorable distribution, with the highest dose being to bone marrow and spleen, followed by the normal organs (liver was the highest dose-limiting normal organ) (24,25).
Since the patients with multiple myeloma and AML/MDS received a 0.5 mg/kg amount of protein and lymphoma patients received 0.75 mg/kg, we also analyzed differences in biodistribution based on the protein concentration. Comparison of the initial uptake and radiation absorbed dose to liver between these 2 groups (0.5 vs. 0.75 mg/kg) did not show a statistically significant difference in liver initial uptake or (average) liver-absorbed radiation dose. This information is important because liver was the dose-limiting organ in all 3 groups of patients and because the radiation dose to liver was therefore used to calculate the treatment dose.
Initial uptake in spleen was higher for the multiple myeloma and AML/MDS groups (which received 0.5 mg/kg) than for the lymphoma group (0.75 mg/kg). It is likely that increasing the amount (mg) of protein in lymphoma patients might have increased splenic uptake (since higher protein improved tumor dosimetry (12)); however, it did not reach the level observed in patients with leukemia where there is a significant increase in cellularity due to tumor cell infiltration.
Differences in biodistribution based on different groups of disease were also found. There was higher initial splenic uptake in leukemia patients than in lymphoma or multiple myeloma patients, probably because there was also a high percentage of patients with enlarged spleen due to disease infiltration. In addition, the number of target sites is greater in spleen of leukemia patients. Even though the amount of BC8 protein was greater in lymphoma patients than in leukemia patients, the overriding factor appears to be the greater number of binding sites in the leukemia patient spleen. Thus, the effect of a higher number of target sites in spleens of leukemia patients is stronger than merely the milligrams of protein administered. However, when the radiation absorbed dose in spleen was calculated, it was higher in multiple myeloma patients than in AML/MDS or lymphoma patients, likely because radiation absorbed dose is inversely proportional to mass.
Radiation absorbed dose in liver was higher for multiple myeloma patients than for AML/MDS patients. Similarly, for bone marrow there was a higher radiation absorbed dose in AML/MDS patients than in lymphoma patients.
For patients treated with 111In-DOTA-BC8, our group previously published data on the influence of splenic size on the bone marrow dose received. Increasing spleen size reduced bone marrow dose, but measurement uncertainties associated with the marrow content of biopsy specimens may have reduced the correlation coefficient (r = 0.25). The spleen acts as a natural sink for radiolabeled antibody, reducing uptake and retention of radiolabeled antibody in red marrow (27). Other authors have also discussed the possibility that spleen has a role in antibody biodistribution (28).
CONCLUSION
Compared with other radiolabeled anti-CD45 antibodies, 111In-DOTA-BC8 was retained longer in liver, spleen, red marrow, and kidneys, with the highest doses being in spleen and liver. These long biologic half-times (approaching 10 days and longer) result in a more efficient delivery of radiation to the patient because decay takes place in vivo rather than after excretion. This pattern of biodistribution was not seen on preclinical or clinical studies that targeted CD45 (using other radiolabeled antibodies) and might be partially due to DOTA chelator, which is present in the structure of this radiolabeled antibody.
Liver, having the highest calculated radiation absorbed dose after spleen, represented the critical nontarget organ for all patient cases and was the designated limiting normal organ for determining administered radioactivity. This finding might have been related to the DOTA chelator presence and the fact that, in these studies, a cold antibody pretreatment was not given. Regarding the protein concentration (0.5 vs. 0.75 mg/kg), we did not observe significant differences in radiation absorbed dose to the liver (at P ≤ 0.10). Therefore, protein concentration did not influence liver absorbed dose.
Few differences in 111In-DOTA-BC8 biodistribution were observed by malignancy type. The exception was greater initial splenic uptake in the AML/MDS group than in the lymphoma or multiple myeloma groups.
DISCLOSURE
This work is supported by program project grant P01 CA 44991, and the grant principal investigator is Oliver Press, MD, PhD. This work is also supported by R21 grant CA155911, and Damian J. Green, MD, is the principal investigator. Darrell Fisher is an employee of Versant Medical Physics and Radiation Safety, which provides contract professional services for various clients, including radiopharmaceutical suppliers and others involved in development and testing of diagnostic and therapeutic medical devices. Ryan Cassaday received research funding from Amgen, Kite/Gilead, Merck, Pfizer, and Vanda Pharmaceuticals; is on the advisory boards for Amgen and Adaptive Biotechnologies; and received honoraria from Pfizer. His spouse is employed by and has stock options with Seattle Genetics. Damian J. Green receives research funding from Juno Therapeutics, a Celgene Company; Seattle Genetics; Cellectar Biosciences; and Janssen. He is a consultant to Celgene, GlaxoSmithKlein, and Seattle Genetics. Johnnie Orozco received research funding from Actinium Pharmaceuticals, Inc. John Pagel is a consultant for Pharmacyclics, Gilead, and Astra Zeneca. Brenda Sandmaier has research funding from Bellicum Pharmaceuticals and is a consultant for Actinium, Bristol-Meyers Squibb, and Kiadis. Her spouse is a consultant for AbbVie, AnaptysBio, Frazier Healthcare Ventures, Inipharm, and Oncoresponse; has equity ownership in AnaptysBio, Blaze Bioscience, EpiThany, Inipharm, Oncoresponse, and Mavupharma; and was formerly employed by Mavupharma. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can treatment be performed with 90Y-anti-CD45 radioimmunotherapy to safely deliver the desired radiation doses without significant side effects?
PERTINENT FINDINGS: No dose limited toxicities occurred. The long biologic half-times observed using 111In-DOTA-BC8 for dosimetry estimates (approaching 10 days and longer) result in a more efficient delivery of radiation to the patient because decay takes place in vivo rather than after excretion.
IMPLICATIONS FOR PATIENT CARE: Radioimmunotherapy using preformed antibodies (such as that used in these 4 clinical trials—a preformed antibody against CD45 antigen) has potential in patients for whom other treatments for hematologic diseases failed. This treatment has the advantage of using passive immunotherapy (preformed antibodies) without the risk of activating the immune side effects that are seen with some of the active immunotherapies.
Footnotes
↵† Deceased.
Published online Mar. 13, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication August 30, 2019.
- Accepted for publication January 3, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.