


Abstract
Multimodality imaging, as represented by its greatest exponent, PET/CT, has a firm place in the evaluation of a patient presenting with cancer. With 18F-FDG, PET/CT is rapidly becoming the key investigative tool for the staging and assessment of cancer recurrence. In the last 5 y, PET/CT has also gained widespread acceptance as a key tool used to demonstrate early response to intervention and therapy. In this setting, a major clinical need is being addressed with 18F-FDG PET/CT, because of its inherent ability to demonstrate (before other markers of response) if disease modification has occurred. This review presents available evidence to this effect.
When a patient presents with cancer, the oncologist has a formidable array of diagnostic and treatment procedures at his or her disposal. Many tumors can now be diagnosed early and reliably and a treatment plan discussed and recommended. Remarkable progress has been achieved, especially if one takes a long-term perspective. In the United Kingdom, since the National Health Service commenced 60 y ago (1), the success of early and reliable diagnosis has been clear. Survival rates for breast, colon, rectal, and cervical cancers have more than doubled over this period. Nevertheless, survival rates for stomach, pancreas, and lung cancers have remained troublesomely low.
A treatment plan assumes that a target for treatment has been chosen and that the target may benefit from therapy. Given the short time window available for the assessment of response in patients with, for example, lung or brain cancer, early assessment of therapeutic success is vital. In this context, despite the above-mentioned improvements in some survival rates, the efficacy of many drugs used in treatment plans remains suboptimal. Thus, it has been found that most drugs used in modern cancer treatment plans are effective in fewer than 60% patients treated in the United States (2). In addition, cancer deposits can behave differently from the primary from which they originate, and this different behavior may evolve further with time. The response of 1 cancer in 1 patient will be different from that seen in another individual with the same tumor type. Early understanding and assessment of the response of the individual patient to his or her individualized treatment intervention is, therefore, crucial. No genotype leads to an identical phenotype!
With these ideas in mind, the role of PET and PET/CT in the management of patients presenting with cancer (3,4) is shifting from early staging and later restaging after recurrence to early assessment of treatment response. This review describes the latter use of PET/CT. As molecular imaging will evolve further, with the development of imaging probes that can be used clinically, the use of PET/CT will also clearly continue to expand. This review, however, concerns itself only with the role of 18F-labeled FDG.
If 18F-FDG PET or PET/CT is able to distinguish early responders from patients resistant to the treatment plan, the consequences will be significant. It will be possible to introduce disease-modifying approaches that halt the use of ineffective drugs, thereby achieving relevant cost savings, and to institute alternative therapies. The goal is clear and carries with it significant patient management implications.
METHODOLOGIC ISSUES
Although methodologic issues do not lie within the scope of this review, a few comments appear useful at this stage. PET/CT is safe, accurate, and reproducible. However, known constraints remain, including partial-volume averaging effects and the limited ability to detect small volumes of metabolically active disease (10% of small lung nodules are silent on 18F-FDG PET), lack of consistency of quantitative data between instruments of the same or different origin, and imprecise coregistration and misalignment caused by, among others, respiratory and cardiac motion and the like. Novel resolution-recovery algorithms may permit faster image acquisition and reconstruction but are likely to impede horizontal comparisons of serial data from the individual patient obtained from different reconstruction programs. Furthermore, the best times for imaging after tracer administration (60 vs. 90 min), for dual-time imaging after tracer administration, and for imaging after chemotherapy or radiation treatment or both continue to be the subject of controversy.
Response to treatment is, of course, multidimensional. Responses to treatment include the clinical response (symptom reduction, improved quality of life, disease-free survival, progression-free survival, and overall survival), laboratory-based indices of response, and imaging response based on modern cross-sectional imaging. In this review, we address only the imaging response with PET/CT, but the overall clinical decision-making progress is multifactorial.
We also do not address in detail the significant issues concerning quantitative CT data analysis and the use of traditional response evaluation criteria for solid tumors (RECIST criteria) (5), though the requirement for new RECIST criteria that incorporate metabolic information will be considered. This topic has been discussed by several authors (6). Antoch et al. (7) showed that PET/CT is twice as accurate as is CT when assessing gastrointestinal stromal tumor response at 1 mo using imatinib. Benjamin et al. (8) shared the view that traditional RECIST criteria are insensitive in evaluating imatinib-treated gastrointestinal stromal tumors and argued for wider use of PET/CT in this context. In a practical manner, the International Harmonization Group (9), reporting on the quantitative assessment of PET/CT for lymphoma, proposed a different approach. Shankar et al. (10) recommend the use of standard protocols for 18F-FDG PET/CT imaging in measuring therapeutic response.
Other circumstances may further impede the accurate assessment of treatment response. 18F-FDG uptake varies between tumor types and even within a given type. Prostate, thyroid, and neuroendocrine tumors are usually not 18F-FDG–avid, but more aggressive prostate cancers often are 18F-FDG–avid (11,12). Trapping of 18F-FDG varies markedly, depending on the type of treatment (chemotherapy vs. immunotherapy or radiotherapy). 18F-FDG itself is not a cancer-specific probe, and baseline PET/CT scans are often not obtained, even though such data can be important in the context of response assessment.
Although these methodologic issues are all relevant, it is clearly possible to make clinical progress in treatment response assessment.
THE LYMPHOMAS
The use of PET/CT in lymphoma is now fairly well established. In comparison with other cross-sectional imaging modalities, PET/CT has clear advantages in terms of superior sensitivity and specificity. Lymphoma was among the first tumor types to be investigated with PET/CT, with health care agencies throughout the world approving the reimbursement of these studies (some acted early on, whereas latecomers were seen in the United Kingdom and Canada).
The lymphomas comprise a wide group of cancers, with 2 large subgroupings: Hodgkin lymphoma or disease (HD) and non-Hodgkin lymphoma (NHL). Although the incidence of HD has been stable, that of NHL continues to grow and is now twice as high as that of HD (at about 15 per 100,000). The NHL group of lymphomas (% frequency is given in brackets) (13) includes diffuse large B cell [31], follicular [22], marginal zone or MALT [8], peripheral T cell [7], small lymphocyte B cell [7], mantle cell [6], and others [11]. Several groups in the field have attempted to develop criteria for response assessment that will accommodate most clinical presentations and permit a more uniform evaluation of patient responses. In 1999, the following International Workshop Criteria (IWC) for NHL were published (14): complete remission was the disappearance of all radiographic evidence of disease and clinical symptoms, with normalization of blood tests and clearance of any bone marrow disease; complete remission/unconfirmed was determined when lymph nodes were still enlarged but had shrunk by greater than 75% and bone marrow was indeterminate; partial remission was a 50% or more reduction in the sum of the products of the greatest diameters of the 6 largest nodes or nodal masses; stable disease was classified as neither partial remission nor progressive disease; and progressive disease was a greater than 50% increase in any lesion or new lesions. These criteria represented a useful start but involved mainly CT-only criteria.
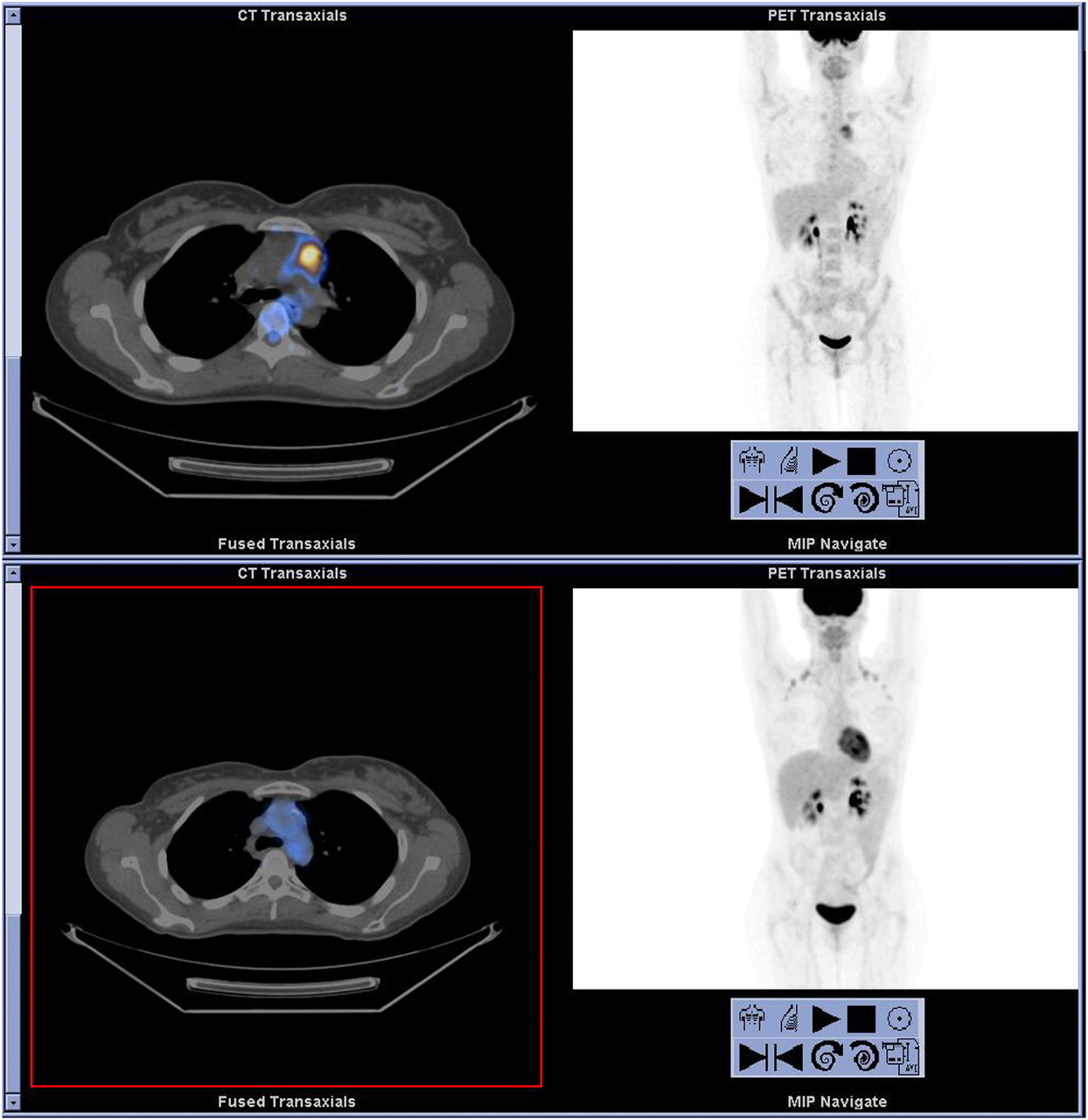
With the rapid acceptance of the utility of PET/CT, novel criteria became imperative. It was finally realized that lymph node size was not a reliable indicator of disease manifestation or regression and that further criteria were needed for disease-response assessment in patients with residual masses after treatment. One of the first reports to address the integration of anatomic and metabolic criteria for disease-response assessment was published by Juweid et al. in 2005 (15). The authors integrated the earlier response criteria for NHL proposed by the IWC (14) with the information obtained from the 18F-FDG PET scan. PET/CT was not used in this protocol, and only visual assessment was used to define patients as having positive or negative results. In doubtful lesions in the lung, the mediastinum was used as a reference point. Subsequently, an international workshop and a subcommittee of the International Harmonization Project in Lymphoma further refined the criteria for response assessment (Table 1; (9,16)). The following are the recommendations of the subcommittee (9): After chemotherapy or immunotherapy, PET should be repeated no sooner than 3 wk and preferably at 6–8 wk; after radiation or chemotherapy plus radiation, PET/CT should be repeated at 8–12 wk; visual assessment alone is sufficient for determining whether a PET scan has positive findings at completion of treatment; mediastinal blood-pool activity as a reference for PET-positive mass greater than 2 cm in the transverse diameter is independent of location; for smaller lesions, the reference should be greater than the surrounding background; and PET should be used for monitoring only as part of a trial or prospective registry. Readers are encouraged to obtain further details from the source references for the proposals (9,16). Figures 1 and 2 illustrate the use of 18F-FDG PET/CT in the assessment of response to therapy in patients with HD and NHL.
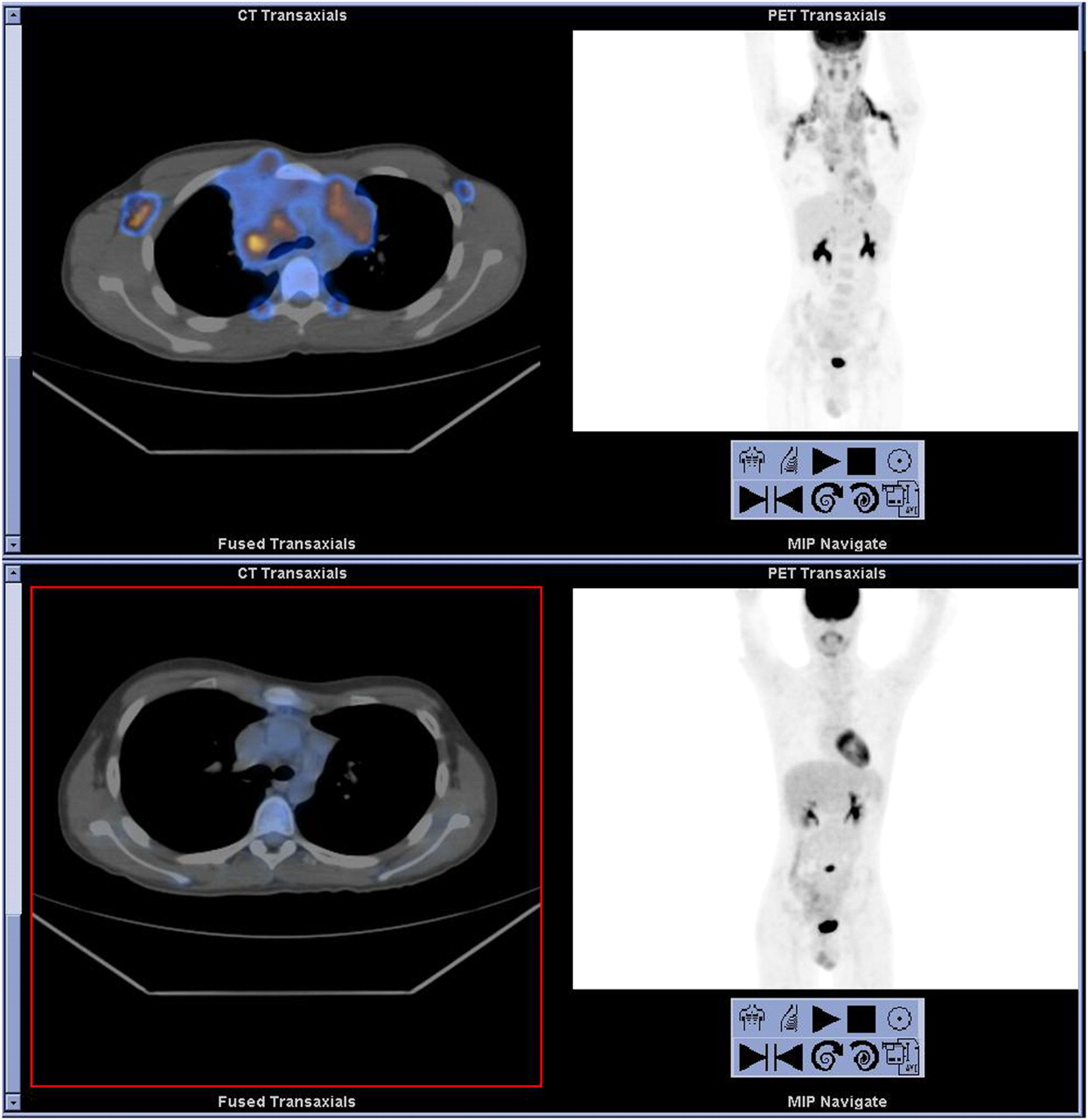
A 15-y-old boy with newly diagnosed HD. On baseline pretherapy 18F-FDG PET/CT (top), maximum-intensity-projection image (top right) and selected transaxial fused PET/CT slice (top left) show 18F-FDG–avid lymphadenopathy in both cervical and supraclavicular regions, extending into mediastinum, both axillae, and right internal mammary chain. 18F-FDG PET/CT was repeated after 3 chemotherapy courses (bottom). CT images (not shown) showed large residual mediastinal lymphadenopathy and cervical and supraclavicular residual disease. MIP image (bottom right) and selected transaxial fused PET/CT slice (bottom left) show no 18F-FDG–avid disease, consistent with complete metabolic response. New focus in mid-abdomen is due to focal inflammation, unrelated to primary tumor. MIP = maximum-intensity projection.
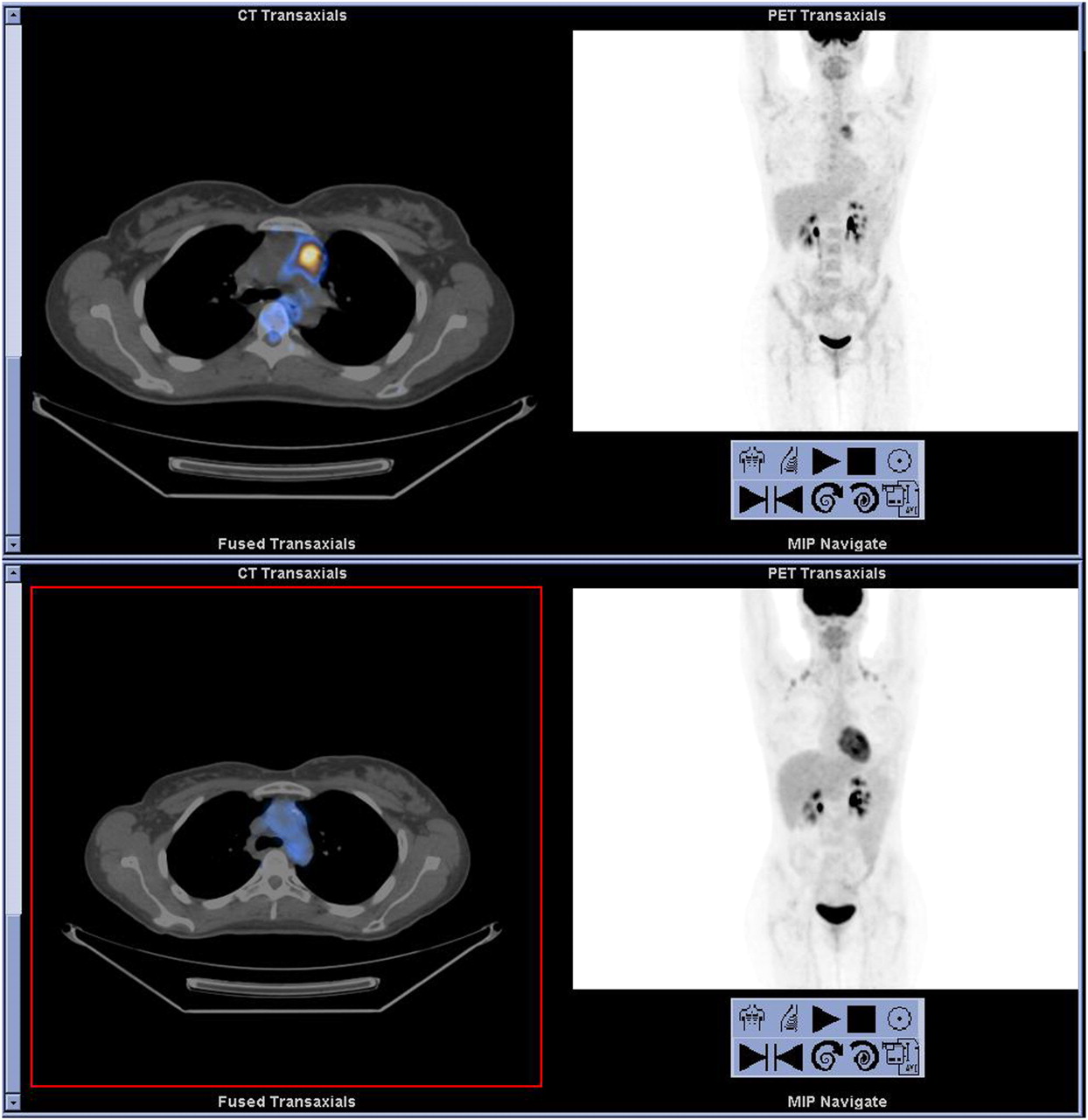
A 31-y-old woman was diagnosed with primary mediastinal B-cell NHL and received 8 courses of R-CHOP (rituximab, cyclophosphamide, hydroxydaunomycin, vincristine [Oncovin; Eli Lilly and Co.], and prednisone). 18F-FDG PET/CT scan obtained after 6 cycles of therapy (not shown) showed residual mass with minimal 18F-FDG activity. Patient was referred for repeated 18F-FDG PET/CT after 8 cycles of chemotherapy and before planned radiotherapy (top). Maximum-intensity-projection image (top right) and selected transaxial fused PET/CT slice (top left) show an 18F-FDG–avid anterior mediastinal mass, compatible with active lymphoma. Further therapy with 2 cycles of ESHAP (etoposide, methylprednisolone, cytarabine, and cisplatin) and consolidation radiotherapy was administered, and repeated PET/CT after 3 mo (bottom) shows no evidence of 18F-FDG–avid disease, consistent with complete metabolic response. MIP = maximum-intensity projection.
Revised Criteria for Complete Remission in Malignant Lymphoma (16)
A clear need has emerged to regularize criteria for response assessment, such that patients can be enrolled in multicenter studies with defined objective guidelines for comparative purposes. RECIST criteria have been deemed insufficient in the new world of molecular imaging. In addition, this topic has been dynamic and is still evolving: The last word has not yet been written on this matter. The development of new probes will clearly add value to these criteria and guidelines. Several unresolved issues remain and will need to be addressed. These include the assessment of minimal residual disease, the best timing for the escalation or de-escalation of therapy regimens, the effects of radiotherapy, and the different responses in follicular lymphomas versus lymphoma of the skin. In HD, minimal residual disease is difficult to assess, because inflammatory cells seem more prevalent than in NHL and these cells show avidity for 18F-FDG. It is still uncertain whether it is appropriate to avoid radiotherapy in HD after 3 cycles of chemotherapy and negative 18F-FDG PET/CT scans results; the role of PET/CT in decisions on when to transplant in advanced disease has not yet been sufficiently addressed. Nevertheless, promising data are beginning to emerge.
A positive 18F-FDG scan finding before autologous stem cell transplantation for aggressive lymphoma has been shown to be linked with a worse outcome than a negative finding on an 18F-FDG scan (17). This outcome may differ from that seen in conventional allogeneic transplantation (18). There is increased interest in the use of reduced-intensity allogeneic stem cell transplantation, and the role of 18F-FDG PET/CT in this context is being defined. Our group showed in a retrospective study that the administration of donor lymphocyte infusions was influenced by the PET/CT scan in 9 of 15 patients (19). In a prospective study (in preparation), we are now investigating the potential role of a pretransplantation 18F-FDG PET/CT scan as a biomarker for predicting the outcome in patients receiving reduced-intensity stem cell transplants.
The issue of a quantitative analysis of 18F-FDG PET data was addressed de novo by Weber in 2007 (20). Weber pointed out that recommendations from the International Harmonization Project refer only to the investigation of patients after completion of therapy, that experience has shown that early responders need to be defined, and that the use of only visual assessment remains essentially a subjective and poorly reproducible methodology. Quantitative assessments are needed to ensure reproducibility of analysis across centers. In 2007, Lin et al. (21) published data suggesting that the use of standardized uptake values (SUVs) in the assessment of response to first-line chemotherapy improves the prognostic value of early 18F-FDG PET/CT. The predictive accuracy for event-free survival in patients with diffuse large B-cell lymphoma improved from 65% to 76% when quantitative analysis was added to a visual score. An SUV score of greater than 5 improved the positive predictive value from 50% to 92%, without a change in the negative predictive value (at 74%). Transformed lymphomas have been detected with lower SUVs, and SUVs obtained in patients who experience lymphoma transformation can overlap with SUVs in patients who do not, although broad guidelines for the prediction of histologic transformation based on SUV data have been published (22). SUVs greater than 17 are associated with histologic transformation, whereas SUVs less than 12 are linked with an indolent cancer. We know little about the majority of patients who present with SUVs in between these values. Finally, Juweid et al. have recently addressed the unresolved issue of biopsy (yes/no) in the posttreatment assessment of lymphomas (23). Although concordance on this issue has not yet been reached on the 2 sides of the Atlantic, the recommendations of these authors are listed in Table 2.
18F-FDG PET for Posttreatment Assessment of HD and NHL
Much has been learned, and useful guidelines have been discussed. These should aid in improving the interpretation of 18F-FDG PET/CT scans in the longitudinal management of patients with lymphoma.
BREAST CANCER
Breast cancer is the most common cancer in women in the Western world and in most Western countries. This type of cancer is the second leading cause of cancer-related death in women, with an age-adjusted incidence of 126.1 per 100,000 women per year in 2005 in the United States. The highest incidence occurs in women 40–55 y old. The National Cancer Institute estimates that in 2008 in the United States, 194,450 women will be diagnosed with breast cancer and 40,930 women will die of breast cancer, most of them of progressive metastatic disease (24).
The clinically relevant classification of breast cancer is based on the biologic behavior and prognosis and includes invasive or infiltrating carcinoma, ductal carcinoma in situ, microinvasive carcinoma, Paget disease, inflammatory carcinoma, and lobular carcinoma in situ. Invasive ductal carcinoma is the most common type, occurring in 70%−80% of all cases; it commonly spreads to regional lymph nodes and carries the worst prognosis. Ductal carcinoma in situ consists of malignant epithelial cells confined to the mammary ducts, without microscopic evidence of invasion through the basement membrane into the surrounding tissue. Invasive lobular carcinoma is relatively uncommon, accounting for only 5%−10% of breast tumors. Patients are prone to have bilateral carcinoma, and prognosis is similar to that of infiltrating ductal carcinoma. Lobular carcinoma in situ generally lacks specific clinical or mammographic signs and occurs more frequently in premenopausal women. These cancer cells are confined to the mammary lobules without invasion. Treatment decisions are guided by tumor stage. Early stages are treated with surgery, and advanced stages with chemo- and radiotherapy. The size of the primary tumor is a risk factor for nodal involvement, and the extent of axillary nodal involvement is the best predictor for recurrence and an important factor for planning therapy (25).
At the time of initial diagnosis and staging of breast cancer, 18F-FDG imaging has limited diagnostic value in detecting small noninvasive primary breast tumors, in staging the axillary region, or in the detection of osteoblastic metastases. Better performance has been demonstrated for the detection of primary invasive breast cancer, mainly for infiltrating ductal carcinoma (26–28), and in the detection of internal mammary and mediastinal metastases (26,28). Local or regional disease recurs in 7%−35% of patients with breast cancer (29). 18F-FDG PET performs better than do conventional imaging modalities in the assessment of disease recurrence, with an overall accuracy of 90% (30), and has been shown to guide changes in the management of up to 50% of these patients (31).
18F-FDG PET has been used to assess the response in patients treated for advanced disease and in patients receiving preoperative primary chemotherapy for inoperable localized tumors (32). Few clinical data are available on the assessment of response to radiotherapy alone. In these patients, increased 18F-FDG uptake may indicate tumor progression (32); however, radiotherapy-induced inflammatory changes may cause increased 18F-FDG activity both in the region of the tumor and in other radiosensitive tissues.
More data are available in patients with breast cancer treated with chemotherapy (32,33) (Fig. 3). Vranjesevic et al. compared the value of 18F-FDG PET and conventional imaging modalities in predicting outcome (34). In a retrospective study of 61 patients who completed therapy for breast cancer, 18F-FDG PET was more accurate than were other imaging modalities, with positive and negative predictive values of 93% and 84%, respectively, versus 85% and 59% for conventional imaging modalities; 18F-FDG PET had a prognostic accuracy of 90% (34).
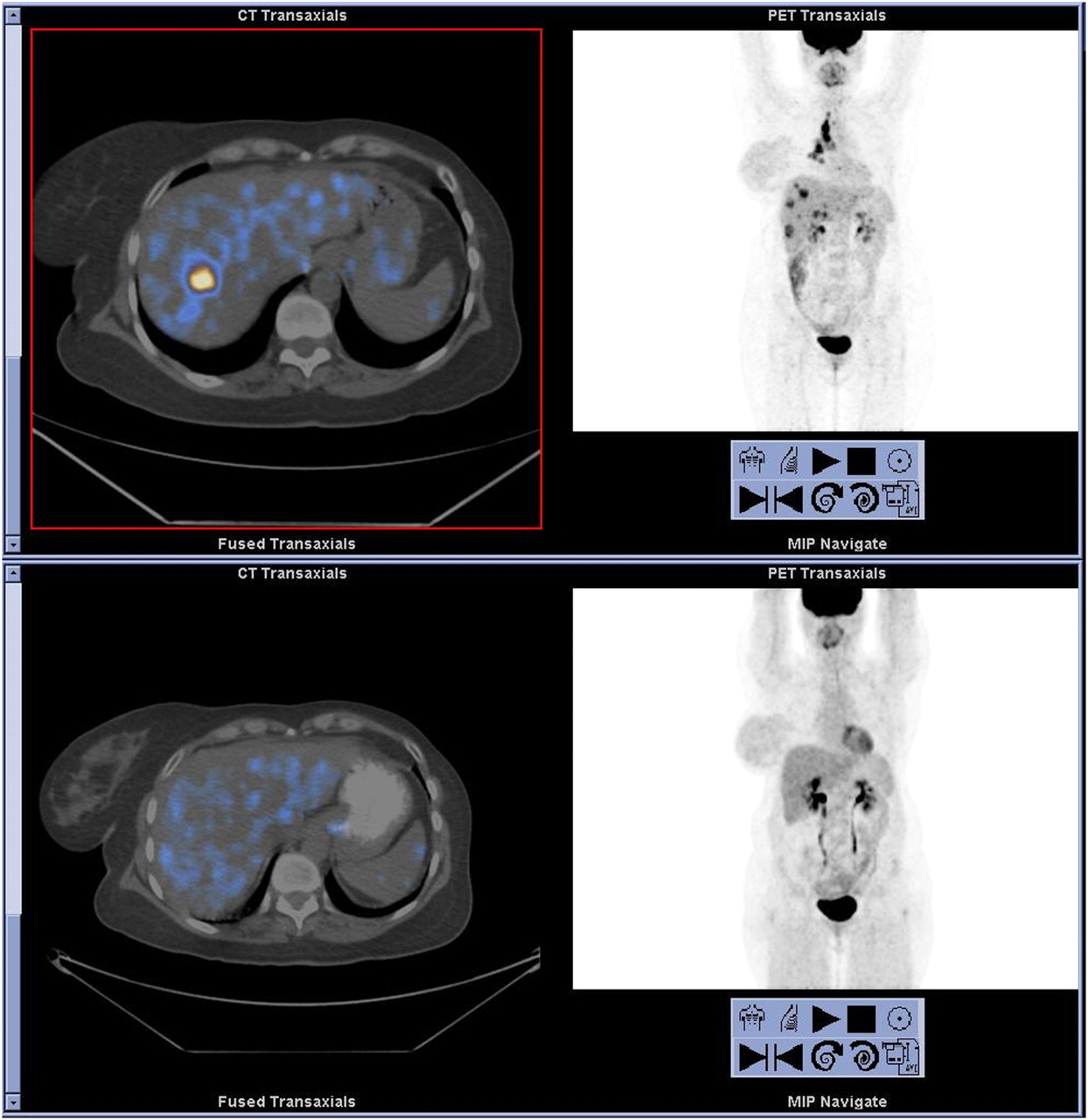
A 50-y-old woman with T4 left breast cancer was treated with adjuvant chemotherapy and radiotherapy to chest wall, followed by modified left mastectomy. 18F-FDG PET/CT was performed after 5 y for assessment of elevated Ca-15.3 serum marker (top). Maximum-intensity-projection image (top right) shows 18F-FDG–avid mediastinal and right hilar lymphadenopathy and 18F-FDG–avid lesions in both lobes of liver. Selected transaxial fused PET/CT slice (top left) shows largest 18F-FDG–avid liver lesion. Further chemotherapy was given, and 18F-FDG PET/CT repeated 3 wk after completion of 6 courses of docetaxel (bottom) shows no evidence of 18F-FDG–avid disease, compatible with excellent response to therapy. MIP = maximum-intensity projection.
Quantitative assessment has been used for the assessment of early response to therapy. In 11 patients with newly diagnosed breast cancer who had a baseline and 4 follow-up quantitative PET scans during the first 3 cycles of therapy, Wahl et al. reported decreasing 18F-FDG uptake as early as 8 d after initiation of therapy, preceding anatomic changes. This reduction was also highly accurate in the prediction of treatment response (35).
SUVs have been used for serial follow-up studies. In patients receiving hormonal therapy, metabolic flare occurs 7–10 d after initiating the administration of tamoxifen, with an increase in tumor SUVs of 1.4 ± 0.7 (32,33,36). In 11 patients with metastatic breast cancer, Dose Schwarz et al. reported a significant decrease in SUV after the first and second cycles of chemotherapy, compared with baseline, to a mean of 72% and 54%, respectively, in patients who responded to chemotherapy; nonresponders showed no significant change (36). Rousseau et al. prospectively assessed 64 patients treated with neoadjuvant chemotherapy for stage II and III breast cancer. The patients underwent PET/CT at baseline; after the first, second, and third courses of chemotherapy; and before surgical excision. SUVs decreased markedly in 34 of the 36 responders and did not change in nonresponders (37), as determined by surgical findings. When using a cutoff value of 60% of baseline SUV, 18F-FDG PET/CT after 2 courses of chemotherapy had the best performance, with an accuracy of 87% for predicting a pathologic response, significantly higher than that of conventional imaging (37). Recently, Berriolo-Riedinger et al. prospectively evaluated the predictive value of reduced 18F-FDG uptake after the first course of neoadjuvant therapy in 47 patients with large or locally advanced breast cancer. Patients who achieved a complete response had a mean decrease in SUV of 85%, compared with a 22% decrease in nonresponders. Moreover, in multivariate analysis the change in SUV was the only factor predictive of complete response (38).
18F-FDG PET/CT can provide early information on tumor response to therapy in patients with breast cancer and may permit choice of the optimal treatment strategy. More prospective studies are needed to establish these findings and to assess their prognostic value.
NON–SMALL CELL LUNG CANCER
Lung cancer is the leading cause of cancer death in men and women, with an annual age-adjusted rate of 64.3 and an annual age-adjusted death rate of 54.4 (24). It is estimated that in 2007 in the United States, there were 213,380 new cases and 160,390 deaths from this disease (39). Small cell carcinoma accounts for 15% of all lung cancers, and the remaining 85% are non–small cell cancers (NSCLCs), including squamous cell and adeno- and large cell carcinomas (24). In the United States, adenocarcinoma is the most common type, accounting for more than 40% of lung cancers, and it also has the worse prognosis. Approximately 30% of NSCLC patients are candidates for curative resection.
18F-FDG PET/CT has a well-established role in the diagnosis and staging of lung cancer. For diagnosis of lung nodules larger than 1 cm, the overall sensitivity, specificity, and positive and negative predictive values are 96%, 78%, 91%, and 92%, respectively. False-positives are mostly due to benign or inflammatory lesions, and false-negatives are due to small or well-differentiated malignancies, such as bronchioloalveolar carcinoma or carcinoid (40). Furthermore, 18F-FDG PET/CT has been shown to be significantly more sensitive and specific than conventional imaging for the detection of mediastinal nodules and distant metastases (41); it is, therefore, routinely used for the preoperative staging of these patients. 18F-FDG PET/CT effectively changes management in 25%−52% of cases and has a major role in reducing the number of futile thoracotomies (42,43).
In addition, 18F-FDG PET/CT performed at baseline may also provide prognostic information. Pillot et al. have summarized the literature assessing the relationship between tumor SUV and outcome (44), suggesting the SUV to be a powerful surrogate marker for outcome in NSCLC. Recently, Goodgame et al. retrospectively analyzed 136 patients with stage I NSCLC. A total of 32 patients had recurrence of their disease during a median follow-up time of 46 mo. In multivariate analysis, a preoperative maximum SUV (SUVmax) of 5.5 or higher was found to be an independent predictor of relapse and death in patients with resected stage I NSCLC (45). Tann et al. also conducted a retrospective study in 51 patients with stage I lung cancer and compared 18F-FDG PET/CT findings with growth rates and tumor doubling times obtained from pretreatment chest CT examinations more than 25 d apart. Rapid, moderate, and slow doubling times correlated with the SUVs (8.2 + 4.8, 5.5 + 4.5, and 2.2 + 1.1, respectively) (46). If this correlation is proven in large prospective trials, a single pretreatment 18F-FDG PET/CT study could be used to predict the rate of tumor growth and might permit the choice of an individualized approach to therapy.
In patients with NSCLC, the response rate is 20%−40%, and tumor progression after first-line chemotherapy occurs in a third of patients (42). There are, however, second-line therapies that could be offered to nonresponding patients if it were possible to predict tumor response early. Indeed, 18F-FDG PET has been used to assess the changes in glucose metabolism and to predict tumor response early (42,43,47). Weber et al. assessed 57 patients with advanced NSCLC before and after the first cycle of platinum-based chemotherapy. There was a close correlation of the change in SUV and the tumor response to therapy using a reduction of 20% in tumor SUV as a criterion for metabolic response. Median time to progression and overall survival were significantly longer for the 28 patients with a metabolic response than for the metabolic nonresponders (163 and 252 d in metabolic responders vs. 54 and 151 d in metabolic nonresponders) (42). In 56 patients with NSCLC who underwent 18F-FDG PET and CT before and after neoadjuvant chemotherapy followed by tumor resection, the change in SUV correlated much better with the percentage of nonviable tumor cells in the resected tumors than did the change in size on CT. A decline of 80% or more in SUV predicted a complete pathologic response with a sensitivity, specificity, and accuracy of 90%, 100%, and 96%, respectively (47). In a prospective study of 47 patients with stage III NSCLC, 18F-FDG PET was performed before and after 1 and 2 cycles and at the end of induction chemotherapy (48). At the end of therapy, nodal stage at CT was not predictive of outcome, but focal increased 18F-FDG uptake on PET was associated with a 2-fold risk of death. A decline in SUV of 50% or more predicted survival significantly. A similar trend was noted after 1 and 2 courses of chemotherapy (48). Eschmann et al. performed 18F-FDG PET before and 2 wk after completion of neoadjuvant radiation and chemotherapy and before resection in 70 patients with stage III NSCLC. Negative 18F-FDG PET scan findings or a reduction in SUV of more than 80% from baseline was the best predictor for good response to further treatment, whereas progressive disease on PET correlated with an unfavorable outcome (43).
18F-FDG PET has a well-established role in the diagnosis and staging of lung cancer. Preliminary data from quantitative analysis suggest that 18F-FDG PET performed at baseline and during and after completion of neoadjuvant radiation and chemotherapy may also provide prognostic information. Large prospective clinical trials are needed to establish the role of 18F-FDG PET for management decisions and prediction of prognosis in these patients.
ESOPHAGEAL CANCER
Esophageal cancer is relatively rare and represents about 7% of all gastrointestinal malignancies. It is more common in India, China, and southern Africa. This type of cancer has an unfavorable prognosis, with a long-term survival of only 25%, and is the fifth most common cause of cancer-related deaths. Esophageal cancer usually presents as advanced-stage disease. A total of 75% of patients have involved lymph nodes at presentation and a 5-y survival of 3%, whereas the 5-y survival is 42% for patients with no initial nodal involvement (49).
A total of 30% of esophageal cancers are adenocarcinomas, commonly associated with Barrett esophagus and usually involving the distal third of the esophagus. Squamous cell carcinomas, associated with alcohol and tobacco use, involve mainly the mid third of the esophagus. Other rare esophageal malignancies include sarcomas, lymphomas, melanomas, and carcinoid tumors. Distant metastases are present in 18% of patients at presentation, most commonly in abdominal lymph nodes, liver, and lungs; less commonly, the tumor spreads to supraclavicular nodes, bones, and adrenals (49). Staging is based on the TNM system. In general, stages I–III are treated with surgery as well as chemotherapy and radiation; stage IV (distant metastatic disease), however, is inoperable, and chemotherapy and radiation are used for palliation. A total of 50% of patients are inoperable at presentation.
18F-FDG PET/CT is used mainly for accurate localization of the tumor, for staging, for detection of recurrence, and, recently, also in the assessment of treatment response after chemotherapy or radiotherapy. 18F-FDG PET has an incremental value of 14% over CT in the accuracy of staging (49). Guo et al. assessed 45 patients with suspected recurrence of squamous cell esophageal cancer and reported sensitivity, specificity, and positive and negative predictive values of 94%, 92%, 75%, and 98%, respectively (50). 18F-FDG PET/CT is superior to combined CT and endoscopic ultrasonography in the diagnosis of stage IV disease and in the detection of regional lymph nodes and distant metastases. Chalabi et al. assessed 74 patients, 18 of whom had discordant findings on 18F-FDG PET/CT, CT, and endoscopic ultrasonography. In correlation with postsurgical findings, PET was correct in 16 of these discrepant cases (51).
Patients with locally advanced disease are treated with neoadjuvant therapy. However, for patients who do not respond to neoadjuvant therapy the prognosis might be worse than after primary surgery. In a systematic review of the literature, Westerterp et al. assessed response to neoadjuvant therapy in patients with esophageal cancer (52). The sensitivity of CT, endoscopic ultrasound, and 18F-FDG PET ranged from 33% to 55%, from 50% to 100%, and from 71% to 100%, respectively. Specificities ranged from 50% to 71%, from 36% to 100%, and from 55% to 100%, respectively. The accuracy of CT for therapeutic response assessment was significantly lower than that of endoscopic ultrasound, and the accuracy of endoscopic ultrasound was similar to that of 18F-FDG. However, the use of multisection CT scanners may improve the performance of CT.
Wieder et al. assessed chemotherapy-induced changes in tumor glucose use of esophageal squamous cell cancer (53). The reduction of metabolic activity was correlated with histopathologic tumor response and patient survival in 38 patients. 18F-FDG PET was performed before therapy, at 2 wk and 3–4 wk after chemotherapy, and before surgery (Fig. 4). Mean tumor uptake of 18F-FDG decreased by 38% 14 d after the initiation of therapy and decreased by a further 37% on the preoperative scan. Patients with a histopathologic response had a mean decrease in 18F-FDG uptake of 44% after 2 wk, compared with 21% in nonresponders. On receiver-operating-characteristic curve analysis, a cutoff value of 30% decrease from baseline 18F-FDG uptake was the most accurate in differentiating subsequently responding and nonresponding tumors. On the preoperative scan, 18F-FDG activity in tumors decreased by a mean of 70% in responders and 51% in nonresponders. Changes in tumor 18F-FDG uptake between baseline and 14 d were a slightly better predictor for histopathologic tumor response than were changes in 18F-FDG uptake between baseline and preoperative studies. Metabolic changes were also correlated with patient survival for a median follow-up of 33 mo. Patients with a decrease in 18F-FDG uptake of less than 30% had a median survival of 18 mo, compared with 38 mo for patients with a decrease in uptake of more than 30%. These findings suggest that 18F-FDG PET can be used to identify early nonresponders, allowing early modifications of therapy (53).
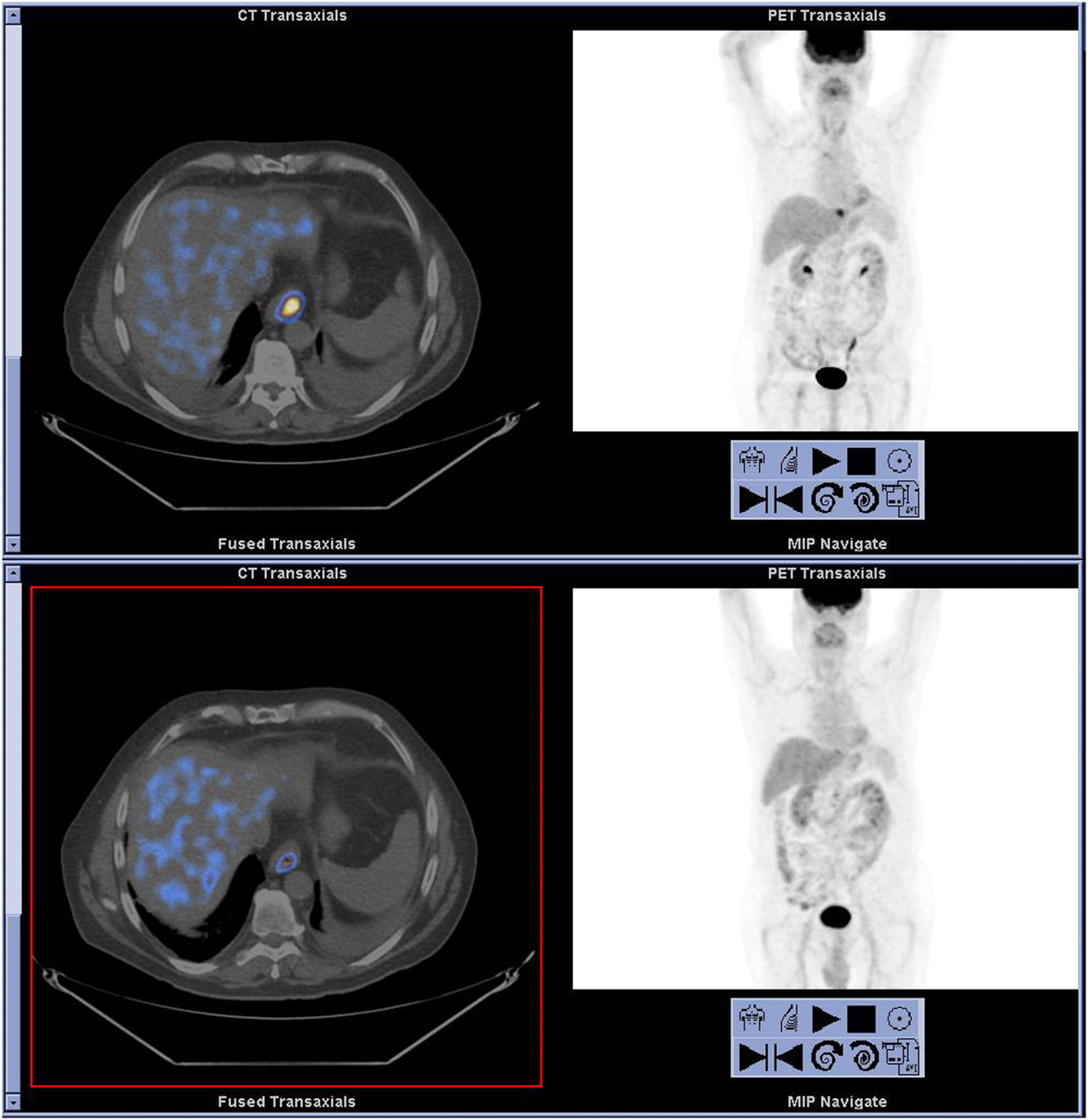
A 67-y-old man with newly diagnosed esophageal cancer. 18F-FDG PET/CT scan was obtained at presentation (top). Maximum-intensity-projection image (top right) and selected transaxial fused PET/CT slice (top left) show 18F-FDG–avid primary (SUVmax, 9) and no evidence of spread. 18F-FDG PET/CT was repeated after 3 mo of neoadjuvant chemotherapy for presurgical assessment (bottom). MIP image (bottom right) and selected transaxial fused PET/CT slice (bottom left) show reduced 18F-FDG uptake in distal esophagus (SUVmax, 5.6) and no 18F-FDG–avid disease elsewhere, indicating good response and favorable prognosis. Patient was therefore referred for surgery. MIP = maximum-intensity projection.
The same authors recently assessed the time course of 18F-FDG uptake in patients with locally advanced esophageal adenocarcinomas treated with preoperative chemotherapy (54) and found similar results. Twenty-four patients underwent 18F-FDG PET before therapy, at 2 wk after initiation of therapy, and preoperatively. Baseline tumor SUV decreased by a mean of 37% after 2 wk and by a further 28% before surgery. The reduction between the first 2 studies was significantly correlated with histopathologic response and with survival, and there was a similar trend for changes between the first and third studies. However, no correlation was found with absolute SUV. Therefore, early changes in tumor 18F-FDG uptake could potentially be used to adjust the treatments individually, so that metabolic responders continue to receive therapy and an alternative treatment is offered to nonresponders.
The MUNICON trial was the first prospective trial designed to show the use of 18F-FDG PET results for modifying treatment in patients with esophagogastric adenocarcinoma (55). A total of 110 patients were prospectively recruited and received 2 wk of induction chemotherapy. Fifty-four patients had a decrease of 35% or more in tumor SUV and were defined as metabolic responders; these patients continued to receive neoadjuvant chemotherapy and proceeded to surgery. Metabolic nonresponders proceeded directly to surgery. After a median follow-up of 2.3 y, median overall survival was not reached in metabolic responders and was 25.8 mo in nonresponders; major histologic remissions were noted in 58% of metabolic responders, but none was seen among the metabolic nonresponders.
18F-FDG PET has a well-established role in the diagnosis and staging of gastroesophageal cancer. Preliminary data suggest that 18F-FDG PET performed at baseline, during neoadjuvant chemotherapy, and after completion of chemotherapy may also provide prognostic information. If this is proven in larger prospective trials, early metabolic assessment with 18F-FDG PET may have an important role in the treatment algorithm of gastroesophageal cancers and may help to select patients who will benefit from chemotherapy as well as avoid the administration of inefficient chemotherapy in patients with no metabolic response.
COLORECTAL CANCER
Colorectal cancer is the third most common cancer, affecting 5% of the population in the United States and Western countries. It is the second most common cause of cancer death. Colon cancer is more common in women, and rectal cancer is more common in men. It is estimated that there are 135,000 new cases of colorectal cancer per year in the United States, and about 57,000 patients die yearly. Potential curative resection is achieved in 70%−80% of patients, and the overall 5-y survival is less than 60% (56). Although a cure can be achieved, about half of the patients will relapse within 5 y.
Endoscopic ultrasound, pelvic CT, and MRI are helpful in the initial staging of the tumor. 18F-FDG PET is not routinely used for diagnosis of colorectal cancer; however, incidental focal increased gastrointestinal 18F-FDG activity occurs in 3%−5% of studies in patients with cancer with unrelated malignancies and in about half of the cases is due to malignant or premalignant etiology (57). Although not routinely performed for preoperative staging, 18F-FDG PET has an established role in staging before surgical resection of metastases, also improving patient management. The detection of disease spread may lead to cancellation of resection in patients with increased surgical risk (58). In addition, 18F-FDG PET is useful in the diagnosis of recurrent disease in patients with unexplained rising serum carcinoembryonic antigen levels (59,60), in the assessment of residual masses after therapy (61), and in the monitoring of response after ablative therapy of liver metastases (62,63).
Preoperative chemoradiotherapy is increasingly used in patients with locally advanced colorectal carcinoma. Chemotherapeutic options include 5-fluorouracil, sometimes with oxiliplatin or fluoropyrimidines, in combination with radiotherapy. This combination reduces the incidence of local recurrence at 5 y to 6% and of distant recurrence to 36% with an overall 5-y survival of 76%. Anatomic imaging modalities are unable to accurately differentiate postradiation changes from active residual tumor (64), whereas 18F-FDG PET is more useful in assessment of response to therapy. Increased 18F-FDG activity after radiation may also be due to inflammatory changes, and false-positive results may persist for 6 mo after completion of radiotherapy (65).
Several studies have assessed the role of 18F-FDG PET in the prediction of response to therapy. In patients with locally advanced rectal cancer, a 36% reduction in SUV enabled the discrimination of responders from nonresponders (66,67), predicting response to treatment better than endorectal ultrasound (66), CT, and MRI (67). Guillem et al. demonstrated that 18F-FDG PET can predict long-term outcome (68). At a median follow-up of 42 mo, patients without disease recurrence had a mean decrease in SUVmax of 69%, compared with 37% in patients with recurrent disease. Recently, Capirci et al. assessed 48 patients with locally advanced rectal cancer or recurrent disease, who were treated with radio- and chemotherapy followed by surgery with curative intent. All patients underwent 18F-FDG PET/CT before therapy and 5–6 wk after completion of chemoradiation, and results were compared with histologic findings at surgery (69). A cutoff value of 66% SUVmax decrease for defining response to therapy resulted in an accuracy of 80% for the prediction of response. The SUVmax at diagnosis did not correlate with outcome (69).
18F-FDG PET has been recently used for early prediction of response to therapy in locally advanced (70) and metastatic (71) colorectal cancer. Cascini et al. evaluated 33 patients who were treated with radiochemotherapy followed by surgery. 18F-FDG PET was performed at baseline and 12 d after the start of chemotherapy. The decrease in mean SUV in responders by a mean of 62% significantly differed from nonresponders (mean, 22% decrease). A cutoff of 52% decrease in the mean SUV resulted in an accuracy of 100%, for the diagnosis of response. In 17 patients who also had preoperative 18F-FDG PET, findings were less predictive of pathologic response (70). Dynamic 18F-FDG PET with quantitative Patlak analysis was used for the assessment of chemotherapy response in 50 patients with advanced colorectal carcinoma who were imaged before and at 2 mo after the start of therapy. Changes in tumor metabolism were highly predictive of overall survival as well as progression-free survival, and semiquantitative analysis using SUVmax changes gave similar results (71).
Initial studies evaluating the role of 18F-FDG PET for the assessment of response to therapy in patients with advanced colorectal cancer, and mainly for early assessment of response, show promising results. 18F-FDG PET–based decisions may prove to be useful in patient management, changing therapy to prevent toxicity and reducing the cost of ineffective therapy. Further, large prospective trials are needed to validate the use of 18F-FDG PET response criteria for individual patient management decisions.
MISCELLANEOUS
There are a few reports on the use of 18F-FDG PET for the assessment of early prediction of response to therapy and outcome in patients with other malignancies, such as ovarian cancer (72,73), uterine cancer (73), head and neck squamous cell carcinoma (74,75), sarcoma (76), mesothelioma (77), and melanoma (78).
Patients with ovarian cancer usually present with advanced-stage disease and tumor spread in the abdominal cavity. Neoadjuvant preoperative chemotherapy or chemoradiotherapy may enhance the surgical results in these patients. 18F-FDG PET is highly accurate in the initial staging of primary and recurrent ovarian cancer and has also been shown to be useful in predicting patient outcome after neoadjuvant chemotherapy (72,73). In uterine cancer, a decrease in SUV after neoadjuvant chemotherapy before surgery was found to correlate better than MRI with histologic response (79). Among 152 patients with cervical cancer who had pre- and posttreatment 18F-FDG PET, patients without residual abnormalities on 18F-FDG PET had an estimated 80% 5-y survival, compared with 32% in patients with residual abnormalities (80). In 33 patients with advanced-stage ovarian cancer who underwent 18F-FDG PET before treatment and after the first and third cycles of chemotherapy, Avril et al. found that change in the SUV as early as the first cycle of chemotherapy predicted patient outcome more accurately than did clinical or histopathologic response criteria. Metabolic responders, who were defined as patients with a decrease in SUV from baseline of 20% or more after the first cycle and 55% or more after the third cycle, had a median overall survival of 38.9 mo, compared with 19.7 mo in nonresponders (72). Postchemotherapy cytoreductive surgery in metabolic responders achieved complete tumor resections in 33% of metabolic responders, compared with 13% of nonresponders; optimal tumor debulking was achieved in 15 of 18 responders but in only 7 of 15 nonresponders (72). Recently, Nishiyama et al. retrospectively assessed 13 patients with advanced uterine cancer and 8 patients with advanced ovarian cancer who had 18F-FDG PET before and after completion of therapy (73). Patients were defined as responders or nonresponders on the basis of histopathologic analysis of surgical specimens. There was a significantly higher change in SUVs in responders than in nonresponders. A 65% reduction in SUV from baseline had a sensitivity of 90% and a specificity of 82% in differentiating between responders and nonresponders (73).
Metabolic response criteria may have an important role in the posttherapy monitoring of patients with gynecologic cancer and need to be further validated in a larger group of patients.
Patients with locally advanced head and neck squamous cell carcinoma often receive combined-modality treatment with chemotherapy and radiotherapy, with or without surgery. Sequential therapy with induction chemotherapy followed by chemoradiotherapy allows for adjustments during treatment. Then patients are monitored with conventional imaging techniques and sometimes with repeated biopsy. Recently, 18F-FDG PET has been added to the assessment. McCollum et al. assessed 40 patients with advanced head and neck squamous cell cancer who were treated by induction chemotherapy followed by chemoradiotherapy. 18F-FDG PET was performed after induction chemotherapy and 4–12 wk after completion of chemoradiotherapy (75). After induction chemotherapy, 18F-FDG PET had a sensitivity of 100% and a specificity of 65% for detecting persistent disease at the primary tumor site. After the completion of chemoradiotherapy, 18F-FDG PET had a sensitivity and specificity of 67% and 53%, respectively, for the detection of occult disease in cervical lymph nodes, possibly due to ongoing inflammatory changes causing false-positive results and requiring that PET images be interpreted with no clinical or radiographic correlation.
In 47 patients with head and neck squamous cell carcinoma who underwent 18F-FDG PET before and after 1–3 wk of radical therapy, the change in metabolic rate of 18F-FDG of the primary tumor was useful in identifying patients in complete remission and predicting overall survival, whereas SUV had a poorer correlation with survival (74).
Prediction of therapy outcome during the early phase of treatment of patients with head and neck cancer seems to be promising, but additional studies are needed to define the long-term prognostic significance of 18F-FDG PET in these patients.
CONCLUSION
18F-FDG PET/CT has a well-established role in the diagnosis and staging of a wide variety of cancers. Preliminary data and quantitative analysis show it can also provide early information on tumor response to therapy, potentially enabling personalized patient management. Large prospective trials are needed to establish these findings and to assess the effect of changing management after PET/CT on long-term outcome.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH JANUARY 2010.
-
The authors have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest. No other potential conflict of interest relevant to this article was reported.
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- Received for publication September 4, 2008.
- Accepted for publication November 13, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Growth Signaling Networks Orchestrate Cancer Metabolic Networks
- Oncogenic Control of Metabolism
- Improving 18F-FDG PET Quantification Through a Spatial Normalization Method
- Approaches to Study Tumor Metabolism in Mice
- Automatic Whole Body FDG PET/CT Lesion Segmentation using Residual UNet and Adaptive Ensemble
- Caloric restriction alters lipid metabolism to contribute to tumor growth inhibition
- Measurement Repeatability of 18F-FDG PET/CT Versus 18F-FDG PET/MRI in Solid Tumors of the Pelvis
- Time-of-Flight Information Improved the Detectability of Subcentimeter Spheres Using a Clinical PET/CT Scanner
- 99mTc-Duramycin SPECT Imaging of Early Tumor Response to Targeted Therapy: A Comparison with 18F-FDG PET
- Smaller Agents for Larger Therapeutic Indices: Nanoscale Brachytherapy with 177Lu-Labeled Gold Nanoparticles
- miR-155 Drives Metabolic Reprogramming of ER+ Breast Cancer Cells Following Long-Term Estrogen Deprivation and Predicts Clinical Response to Aromatase Inhibitors
- A Systematic Comparison of 18F-C-SNAT to Established Radiotracer Imaging Agents for the Detection of Tumor Response to Treatment
- Oncogene Pathway Activation in Mammary Tumors Dictates FDG-PET Uptake
- Differential 18F-FDG and 18F-FLT Uptake on Serial PET/CT Imaging Before and During Definitive Chemoradiation for Non-Small Cell Lung Cancer
- Serial Diffusion MRI to Monitor and Model Treatment Response of the Targeted Nanotherapy CRLX101
- Apoptosis Imaging Probe Predicts Early Chemotherapy Response in Preclinical Models: A Comparative Study with 18F-FDG PET
- Cancer Cell Metabolism: One Hallmark, Many Faces
- Early FDG/PET Scanning as a Pharmacodynamic Marker of Anti-EGFR Antibody Activity in Colorectal Cancer
- Biologic Imaging of Head and Neck Cancer: The Present and the Future
- Detection and Characterization of Tumor Changes in 18F-FDG PET Patient Monitoring Using Parametric Imaging
- Intratumor Heterogeneity Characterized by Textural Features on Baseline 18F-FDG PET Images Predicts Response to Concomitant Radiochemotherapy in Esophageal Cancer
- European Organisation for Research and Treatment of Cancer Recommendations for Planning and Delivery of High-Dose, High-Precision Radiotherapy for Lung Cancer
- In Vivo Imaging in Cancer
- High 18F-FDG Uptake in Microscopic Peritoneal Tumors Requires Physiologic Hypoxia
- Glioblastoma Cells Require Glutamate Dehydrogenase to Survive Impairments of Glucose Metabolism or Akt Signaling
- Understanding the Warburg Effect: The Metabolic Requirements of Cell Proliferation