


Abstract
Conventional imaging techniques have serious limitations in the detection, staging, and restaging of prostate carcinoma. Anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (anti-18F-FACBC)is a synthetic l-leucine analog that has excellent in vitro uptake within the DU-145 prostate carcinoma cell line and orthotopically implanted prostate tumor in nude rats. There is little renal excretion compared with 18F-FDG. The present study examines anti-18F-FACBC uptake in patients with newly diagnosed and recurrent prostate carcinoma. Methods: Fifteen patients with a recent diagnosis of prostate carcinoma (n = 9) or suspected recurrence (n = 6) underwent 65-min dynamic PET/CT of the pelvis after intravenous injection of 300–410 MBq anti-18F-FACBC followed by static body images. Each study was evaluated qualitatively and quantitatively. Maximum standardized uptake values were recorded in the prostate or prostate bed, and within lymph nodes at 4.5 min (early) and 20 min (delayed), and correlated with clinical, imaging and pathologic follow-up. Time–activity curves were also generated for benign and malignant tissue. Results: In the 8 patients with newly diagnosed prostate carcinoma who underwent dynamic scanning, visual analysis correctly identified the presence or absence of focal neoplastic involvement in 40 of 48 prostate sextants. Pelvic nodal status correlated with anti-18F-FACBC findings in 7 of 9 patients and was indeterminate in 2 of 9. In all 4 patients in whom there was proven recurrence, visual analysis was successful in identifying disease (1 prostate bed, 3 extraprostatic). In 3 of these patients, 111In-capromab-pendetide had no significant uptake at nodal and skeletal foci. Malignant lymph node uptake in both the staging and restaging patients was significantly higher than benign nodal uptake. Though uptake faded with time, in all 6 patients with either lymph node metastases or recurrent prostate bed carcinoma, there was intense persistent uptake at 65 min. Conclusion: Anti-18F-FACBC is a promising radiotracer for imaging prostate carcinoma. Radiotracer uptake was demonstrated in primary and metastatic disease. Future research should investigate the mechanism of radiotracer uptake in normal and pathologic tissue and develop a clinical imaging strategy for initial staging and restaging.
Prostate carcinoma is the most common malignancy in men, comprising 33% of newly diagnosed cancers in the United States in 2005 (1). Accurately detecting the presence of disease confined to the prostate bed versus that of extraprostatic spread to lymph nodes or the skeletal system has profound treatment implications.
Currently, there is no definitive imaging technique in the initial staging and restaging of prostate carcinoma. Whereas ultrasound and MRI have proven useful for local (T) staging, they have limitations and are not universally used (2–4). For local recurrence in the prostate bed, ultrasound-guided transrectal biopsy is often used but it is invasive and subject to sampling error (5,6). For lymph node assessment, routine CT and MRI are considered to have poor accuracy (3,7).
Molecular imaging techniques such as 111In-capromab pendetide (ProstaScint; Cytogen Corp.) have been used, but sensitivity is only 62%–75% (3,8,9). 18F-FDG PET is not of sufficient diagnostic accuracy for routine clinical use for prostate carcinoma (5,9–14). Other PET radiotracers, including 11C-acetate, 11C-choline, 11C-methionine, and 18F-fluorocholine (18F-FCH), may characterize different metabolic aspects of prostate carcinoma but have demonstrated mixed results for clinical evaluation (4,5,10,15–25). Of course, the 11C-based radiotracers are impractical without an on-site cyclotron. 18F-FCH also seems to have high urinary excretion starting at 5 min after acquisition (5,19,20,25–28). Thus, there is a need for a better radiotracer, with little or no urinary excretion, for the evaluation and staging of patients with prostate carcinoma.
Anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (anti-18F-FACBC) is a synthetic l-leucine analog that has excellent in vitro uptake within the DU-145 prostate carcinoma cell line and within orthotopically implanted prostate tumors in nude rats (29). The uptake of anti-18F-FACBC is likely mediated via the sodium-independent L large-neutral amino acid transport system (LAT) (30,31). There is little renal excretion compared with 18F-FDG (29). The present study examines anti-18F-FACBC uptake in patients with newly diagnosed and suspected recurrent prostate carcinoma.
MATERIALS AND METHODS
Preparation of Anti-18F-FACBC
The preparation of anti-18F-FACBC has been previously reported (32). The decay-corrected radiochemical yield of the desired product was 24% and its radiochemical purity was 99% at 80 min after the end of bombardment. The injected mass was approximately 5 mg, or 38 μmol, and the specific activity was 136.9–192.4 GBq/mmol (3.7–5.2 Ci/mmol).
Patient Selection
All studies were performed under the auspices of the Emory University Institutional Review Board, Radioactive Drug Research Committee, and the Atlanta Veterans Affairs Medical Center Research and Development Committee. Inclusion criteria included any patient with histologically confirmed prostate carcinoma eligible for prostatectomy and possible lymph node biopsy/dissection or with a prior history of histologically confirmed prostate carcinoma with suspected recurrence or metastatic disease. One patient had been recruited under a prior protocol for imaging renal masses who also happened to have prostate carcinoma. This patient underwent dynamic imaging of the abdomen at the level of the kidneys (otherwise the same protocol as in this study). All newly diagnosed patients were imaged 4–8 wk after the initial prostate biopsy. Prostate-specific antigen (PSA) values were obtained within 4 mo of the anti-18F-FACBC scan. Patient demographics are as follows: mean age ± SD is 62.0 ± 8.8 y with a range of 45–76 y; mean PSA ± SD is 15.0 ± 18.6 ng/mL with a range of 1.9–71 ng/mL; and median Gleason score is 7 with a range of 6–10. The original Gleason scores are used for the patients with suspected recurrence.
PET Imaging Protocol
All scanning was conducted on a Discovery DLS or DST integrated PET/CT scanner (GE Healthcare), and the images were interpreted on a combination of an AW workstation with Volume Viewer Plus (GE Healthcare) as well as a program developed by the authors on the IDL platform (RSI Inc.) running on a Pentium 4 (Intel Corp.) computer (operating system, Microsoft; computer hardware, IBM). All patients fasted for 4–6 h before the anti-18F-FACBC scan. This is our standard practice for 18F-FDG PET, though it has not been established if a fasting or nonfasting state optimizes anti-18F-FACBC imaging. The patient first underwent a CT scan of the abdomen and pelvis (80–120 mA) without oral or intravenous contrast for anatomic correlation and attenuation correction of emission data. The patient then received a bolus of anti-18F-FACBC (300–410 MBq) injected intravenously over 1–2 min. PET consisted of a 15-frame dynamic sequence lasting 65 min (number of frames × time [min]: 6 × 0.5, 4 × 3, and 5 × 10) followed by a static scan of the abdomen and pelvis at 4 min per bed position.
Image Analysis
The PET/CT studies were assessed by 1 experienced nuclear radiologist in a prospective manner. For patients with newly diagnosed prostate carcinoma, the prostate was visually divided into 6 sextants (right and left apex, mid, and base). Three equally spaced regions of interest (ROIs) conforming to the axial dimensions of the sextant were drawn, and the pixel with the greatest standardized uptake value (SUV) in the ROI was noted. The highest of these 3 SUVs was recorded as the maximum SUV (SUVmax) for that sextant at the 4.5-min midpoint (3-min frame spanning a dynamic acquisition from 3 to 6 min) and at the 20-min midpoint (10-min frame at 15–25 min). The 4.5-min (early) and 20-min (delayed) frames were chosen based on preliminary analysis of the time–activity curves. In addition, each sextant was visually assessed for the presence of focal activity. A region was considered positive if there was asymmetric focal activity exceeding prostate background activity, similar to the criteria used by Yamaguchi et al. in studying 11C-choline PET (18). We augmented visual interpretation by deriving a ratio of sextant SUVmax divided by muscle mean SUV (SUVmean) in each patient. The SUVmean was obtained by drawing a 3-cm ROI in each gluteus muscle. SUVmean in muscle was chosen because it remained fairly constant with time and best-simulated typical soft-tissue background. Ideally, we would have chosen a prostatectomy-proven normal sextant as background but this was not possible in most patients.
A lymph node or treated prostate bed was considered visually positive if there was sustained focal activity over expected soft tissue or blood pool. Intensity was recorded as follows: mild (above blood pool but less than muscle), moderate (above muscle but less than marrow), and intense (above marrow). Values of SUVmax were also obtained from these lymph nodes or for those of >1 cm in short axis.
Time–Activity Curves
ROIs were defined by hand on transaxial planes over areas of focal uptake or drawn on the CT scan in regions of mild or diffuse uptake. The ROIs included prostate, benign and malignant lymph nodes, bone marrow (ilium), blood pool (femoral artery), muscle (gluteus), bowel (sigmoid), and bladder. Regions of <2 cm in diameter used CT for correction of partial-volume and tissue spillover effects (33).
Correlation of Imaging to Clinical Data
Anti-18F-FACBC imaging findings were correlated with pathologic, clinical, biochemical, and imaging follow-up for up to 1 y after scanning. For local disease, this included pathologic analysis of prostatectomy as well as prostate biopsy tissue. A lymph node was considered clinically positive if there was pathologic proof of neoplasia or progressive increase in lymph node size in the presence of elevated PSA. The absence of lymph node involvement was confirmed if there was a negative surgical lymph node dissection or biopsy or, if lymph node dissection was not performed, PSA declining to nadir (<0.05) after definitive therapy, or if there were no enlarged lymph nodes on follow-up imaging at 6 mo. If a pelvic lymph node dissection was not performed and the patient was placed on hormonal therapy, lymph node status was considered indeterminate.
Statistical Analysis
Nonparametric statistical methods were applied for analyses, given the limited sample size in our study. We assessed all between-group differences in SUVmax using the Wilcoxon rank sum test. Statistical significance was determined using a type-I error rate of α = 0.05, and specific P values are reported with the results. The statistical analyses were performed using SAS version 9.1 software. Statistical significance was reported only if n > 2 in each comparison group.
RESULTS
Initial Staging
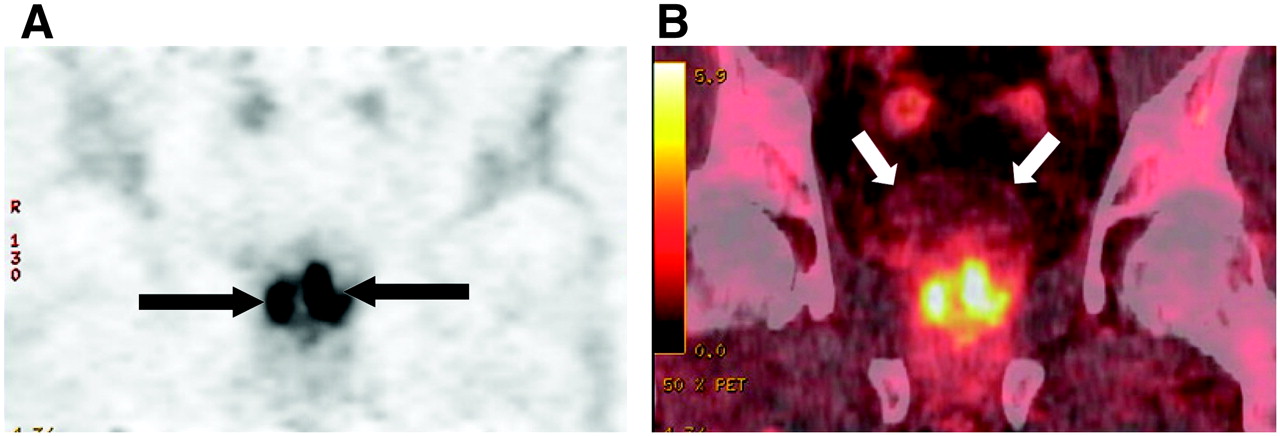
Eight patients underwent dynamic prostate imaging and were correlated with either sextant biopsy (n = 4) or histologic examination of the surgically removed prostate (n = 4). Thirty-nine sextants were positive for carcinoma (1 with a minute focus) and 9 were negative (1 with chronic inflammation). Visual analysis predicted the presence or absence of carcinoma in 40 of 48 sextants. Table 1 is a listing of sextant values of SUVmax and ratios of SUVmax to muscle SUVmean for each patient. A typical patient example is presented in Figure 1.

Coronal PET (A) and CT fused (B) anti-18F-FACBC images of 63-y-old male patient with pathologically proven bilateral prostate carcinoma (arrows in A). Note little bladder activity (white arrows in B).
Anti-18F-FACBC Pathologic Malignant vs. Benign Sextant SUVmax and SUVmax/Muscle SUVmean Ratios at Early (4.5 Minutes) and Delayed (20 Minutes) Time Points for Initial Staging of Patients
In correlation of lymph node status, 7 of 9 patients had excellent concordance of anti-18F-FACBC pelvic nodal findings with clinical follow-up. Two of 9 were indeterminate. Table 2 is a summary of lymph node concordance and Figure 2 is an example of a patient with lymph node metastases. Both patients with malignant lymph nodes had intense persistent uptake, even at 65 min, though less intense than on earlier sequences.
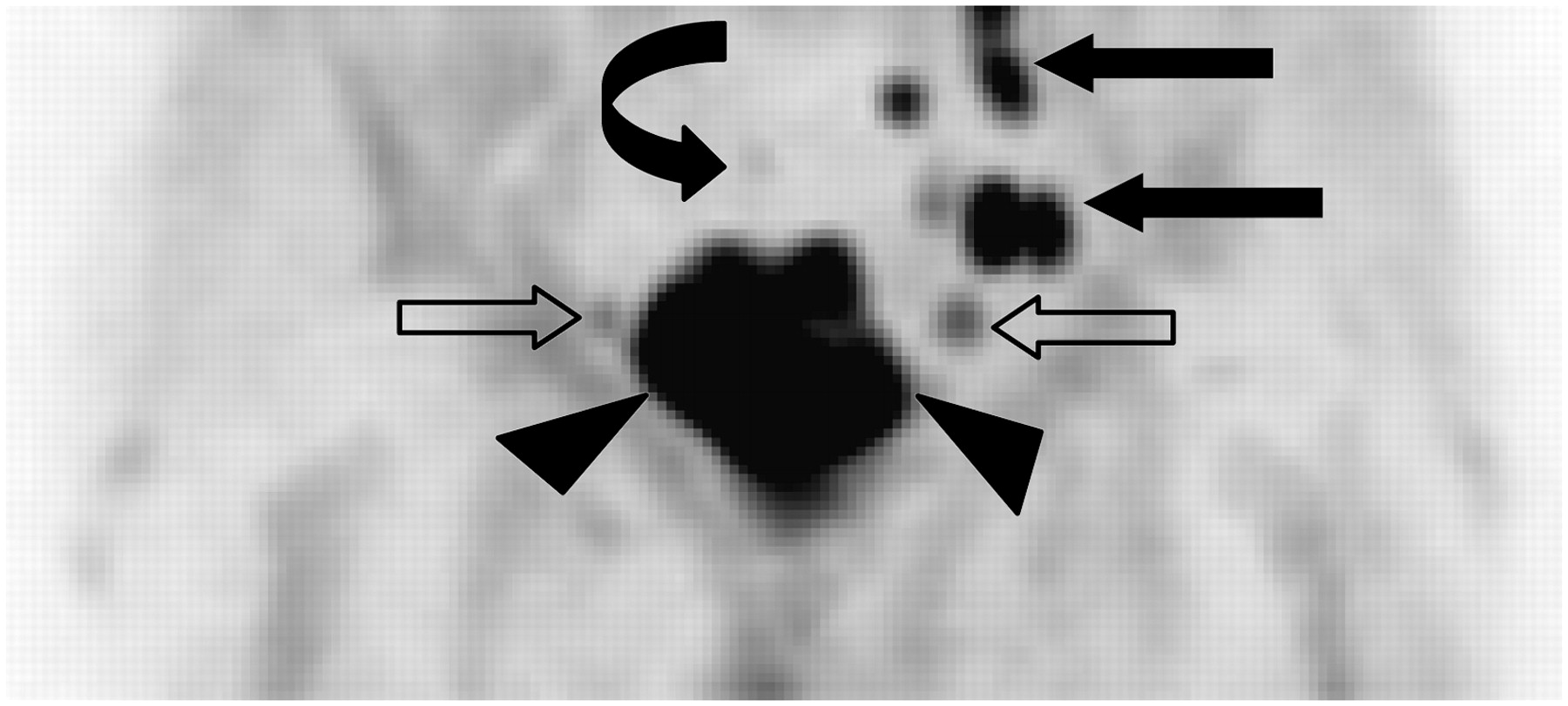
A 73-y-old man with extensive invasive prostate carcinoma, with bilateral obturator and left iliac chain lymph nodal involvement. Maximum-intensity-projection image demonstrates extent of large prostate primary (arrowheads) as well as bilateral obturator (open arrows) and left iliac (solid straight arrows) nodes. Bladder activity is not present (curved arrow at bladder location).
Abdominal/Pelvic Lymph Node Imaging Findings for Initial Staging of Patients at Early (4.5 Minutes) and Delayed (20 Minutes) Time Points with Clinical/Pathologic Correlation
The representative time–activity curve taken from patient 3 (Fig. 3) shows rapid uptake of anti-18F-FACBC in prostate carcinoma to a maximum at 4.5 min, followed by gradual clearance (9.5%/min) beyond 20 min. Regions in marrow (ilium), muscle (gluteus), and bladder reached a plateau at 4.5 min, which remained constant throughout the imaging period. This activity time course was consistent across the patient population for malignant prostate and normal tissues.
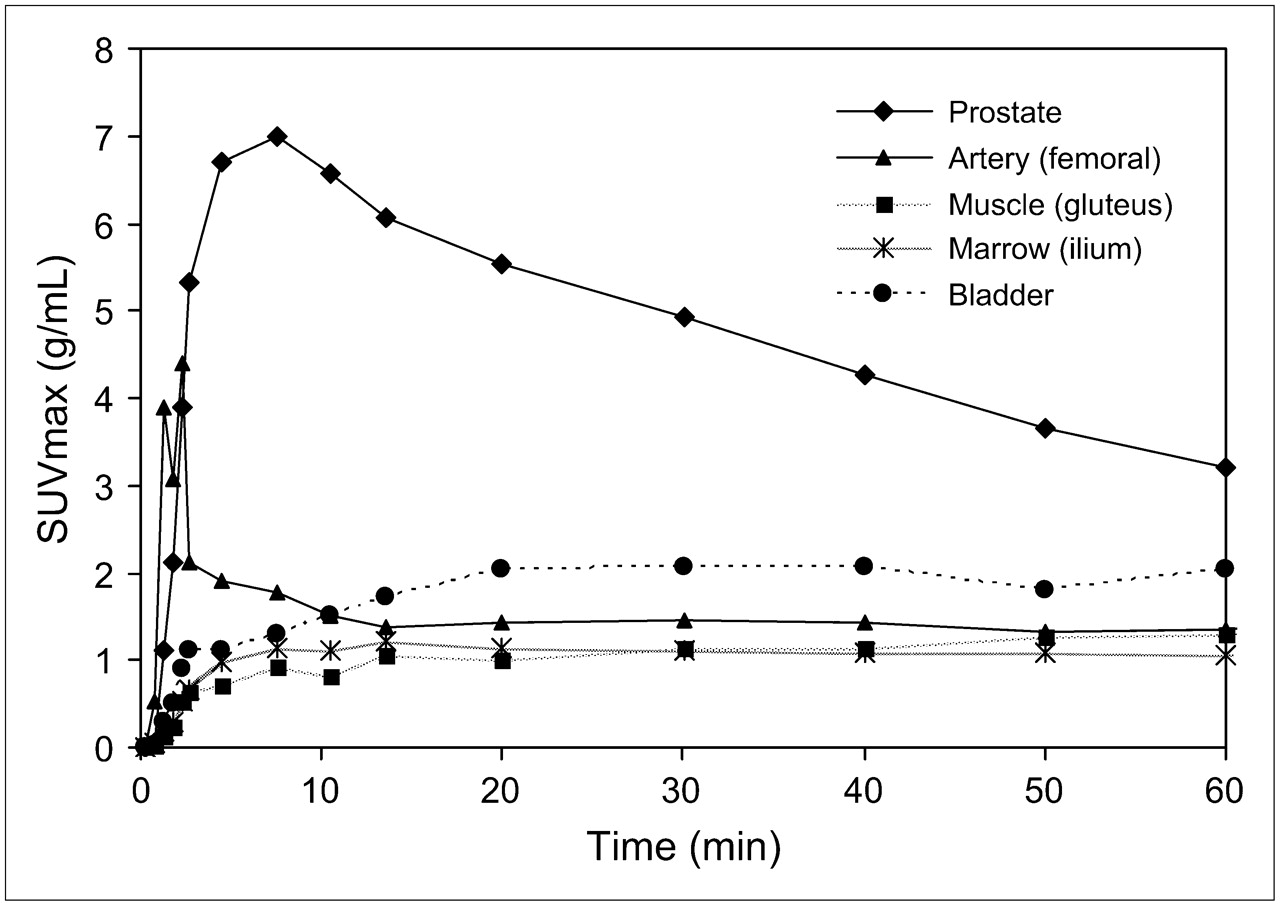
Time–activity curves for initial staging data. Time–activity curve compares uptake in whole prostate with known bilateral carcinoma vs. bladder, marrow, muscle, and femoral artery in initial staging of patient 3.
Suspected Recurrence
On a per-patient basis, the anti-18F-FACBC scan detected neoplasia in 4 of 4 patients with proven recurrence. In 3 of these patents, 111In-capromab-pendetide was unrevealing. In 2 of 6 patients, mild-to-moderate uptake in the prostate bed resulted in false-positive scans, presumably from the radiation effect noted on biopsy. These 2 patients also had negative anti-18F-FACBC and conventional imaging of extraprostatic sites. A summary of each patient's case is presented in Table 3.
Imaging Findings for Suspected Recurrence in Prostate Beds and in Lymph Nodes at Early (4.5 Minutes) and Delayed (20 Minutes) Time Points with Clinical/Pathologic Correlation
There was intense, easily identifiable uptake in the one recurrent prostate bed (Fig. 4) and in the 3 patients with nodal/skeletal metastases (Fig. 5). Uptake in the 2 false-positive prostate beds was less intense and less focal than that in the 1 true recurrent site. Mild diffuse uptake below blood-pool background was present in the other treated beds. Similar to the initial staging of patients, intense uptake persisted on the 65-min images in all 3 patients with lymph node/skeletal metastases and in the 1 patient with recurrent prostate bed carcinoma (though less intense than on the earlier sequences).

Coronal PET (A) and CT fused (B) anti-18F-FACBC images in 71-y-old male patient (restaging patient 1) with biopsy-proven prostate bed recurrence extending toward left seminal vesicle (arrow in A). Maximum-intensity-projection image at 20 min (C) demonstrates uptake in prostate bed (arrow) but little bladder uptake (arrowhead).

Axial PET (A) and fused (B) anti-18F-FACBC images in 67-y-old male patient (restaging patient 2) with intense activity in left external iliac nodes (black arrow in A). SPECT/CT 111In-capromab-pendetide axial 111In (C) and CT fused (D) images demonstrate no significant activity in this region (white arrow in C).
The representative time–activity curve taken from restaging patient 1 (Fig. 6A) shows rapid uptake of anti-18F-FACBC in known prostate carcinoma recurrence to a maximum at 4.5 min with a plateau to 30 min, which is followed by gradual clearance (9%/min) out to 60 min. Regions in marrow (ilium), muscle (gluteus), and bladder reached a plateau at 4.5 min that remained constant throughout the imaging period. The time–activity curve for patient 3 (Fig. 6B) compares uptake in a malignant right internal iliac lymph node with benign right inguinal and obturator nodes. The clearance of the benign regions is more abrupt between 4.5 and 10 min (30%/min) and then slows to that of the malignant region.

Time–activity curve for restaging patient 1 (A) compares uptake in known prostate bed carcinoma recurrence vs. bladder, marrow, muscle, and femoral artery. Time–activity curve in restaging patient 3 (B) compares uptake in a 14 × 11 mm right internal iliac malignant node with benign right inguinal 12 × 18 mm node and benign right obturator 7 × 18 mm conglomerate.
DISCUSSION
On the basis of in vitro and in vivo studies (29,34,35), we hypothesized that anti-18F-FACBC would be able to serve as a valuable adjunct in the initial staging of prostate carcinoma, as well as detecting the presence of local versus metastatic prostate carcinoma in the setting of biochemically recurrent disease. The present study demonstrates encouraging but preliminary initial results.
Anti-18F-FACBC seems to share characteristics with other PET radiotracers used for prostate scanning. Similar to 11C-acetate and 18F-FCH (4,20,36), we observed a certain degree of nonspecific uptake, including relatively intense incidental bowel uptake as well as occasional low-level uptake in benign inguinal lymph nodes.
We also noted regions of false positivity and negativity within the prostate. Though malignant sextants had statistically significant higher SUVmax than benign sextants, there was little separation between benign and malignant sextant values of SUVmax. Yet, visual analysis revealed that there was agreement of 40 of 48 sextants with pathologic results, and ratios of sextant uptake to mean muscle SUVmax demonstrated improved, though still incomplete, separation of malignant from benign tissue. Some pathologically identified benign prostate tissue, including that with inflammation, had focal uptake but these were visually less intense than malignant disease. Future studies will be designed to better examine the question of uptake in inflammatory versus neoplastic foci within the same prostate.
Uptake within the prostate in areas of inflammation, hyperplasia, and high-grade prostatic intraepithelial neoplasia has also been reported with 18F-FCH, 11C-choline, and 11C-acetate (4,5,21,24,37). Kwee et al. (25) noted better discrimination between malignant and benign prostatic regions using early and 1-h delayed prostate imaging with 18F-FCH. It remains to be seen whether anti-18F-FACBC imaging may be useful for primary tumors and to separate areas of inflammation and hyperplasia from neoplasia.
Anti-18F-FACBC demonstrates potential clinical benefit for nodal staging. Formal lymph node dissection is a highly morbid procedure, and anti-18F-FACBC may prove valuable in directing biopsy. For both staging and restaging, SUVmax of malignant nodes was significantly higher than that of benign nodes and anti-18F-FACBC helped discriminate prostatic from extraprostatic involvement. It is also interesting to note that 3 patients with negative 111In-capromab-pendetide studies had positive anti-18F-FACBC imaging, proven to be true positive.
Choline-based compounds have also shown similar promise in nodal staging and in detecting recurrence (4,15). Although intense bladder activity has been reported 5 min after injection with 18F-FCH (5,19,26), anti-18F-FACBC demonstrates relatively little, though variable, renal excretion and bladder activity. Even the most intense bladder activity did not interfere with scan interpretation as has been reported with choline-based PET radiotracers. Yet, the mechanism of anti-18F-FACBC uptake in prostate carcinoma cells is not well understood and is the basis of ongoing studies. Preliminary data suggest a major role for an LAT transporter (30,31).
The time–activity curves of Figures 3 and 6 show rapid uptake of anti-18F-FACBC to 4.5 min, which is followed quickly by a fast and then slow washout rate out to 60 min. Tracer retention in background structures for all cases approaches a plateau after the first 4.5 min. More detailed analysis of the uptake mechanisms awaits further study, but metabolite analysis of arterial plasma samples in human subjects indicates that anti-18F-FACBC does not undergo metabolism (Mark M. Goodman, unpublished data, July 2006).
These findings also suggest that anti-18F-FACBC may be less useful for delayed imaging in some patients because of washout of radiotracer. Yet, all 6 patients with either locally recurrent prostate carcinoma or lymph node metastases did have persistent and often striking uptake, even at 1 h, which may reflect increased uptake in neoplastic cells prone to metastasize or recur. More comprehensive studies must be undertaken to further determine the significance of these findings, to define the optimal time course of imaging, and to find out if comparing early to delayed imaging could increase specificity.
One shortcoming of our study is that step-section pathology was not obtained, and some cases only had sextant biopsy for correlation. There may be a discrepancy between what is perceived as a certain sextant on transrectal ultrasonography biopsy and sextant pathologic analysis after prostatectomy (38). Another shortcoming was our methodology using SUVmax. We chose SUVmax because this is the most common clinical method of SUV use. However, it is less suitable when evaluating regions with low uptake. We attempted to overcome this limitation by applying a ratio of SUVmax to muscle SUVmean, which more closely approximated results with visual interpretation. Future studies will be designed to incorporate more sophisticated tools, such as 3-dimensional mapping, as well as correlation with step-section pathology.
This study is a pilot investigation with a small and heterogeneous patient population. Tests for statistical significance, therefore, were based on a limited sample size. Because of clinical exigencies, not all patients underwent prostatectomy and lymph node dissection, and not all lymph nodes were biopsied. All benign causes of uptake, including that from inflammation, were grouped together, and a definitive subanalysis of benign inflammatory versus noninflammatory uptake was not possible.
CONCLUSION
Imaging with anti-18F-FACBC demonstrated uptake in both primary and metastatic prostate carcinoma on initial staging as well as uptake in recurrent prostate carcinoma within the prostate bed, lymph nodes, and bone. Anti-18F-FACBC PET/CT succeeded in identifying neoplastic foci, even when 111In-capromab-pendetide was negative, and was instrumental in directing biopsy to prove neoplastic recurrence in one patient in whom lymph nodes were not obviously enlarged. Thus, it is feasible that anti-18F-FACBC could improve diagnostic imaging of prostate carcinoma both before and after therapy. A larger cohort study will be designed to establish the clinical utility of anti-18F-FACBC PET/CT in primary and suspected recurrent prostate carcinoma.
Acknowledgments
This research was sponsored by Nihon Medi-Physics Co., Ltd. We acknowledge the hard work of Fenton G. Ingram, CNMT, on this protocol as well as all of our technologists at Emory HealthCare and the patients who volunteered for the study. We also gratefully acknowledge the contributions of Ron Crowe for radiotracer synthesis, Drs. Adam Kuehn and Mahul B. Amin for histologic interpretation, Dr. Raghuveer K. Halkar for imaging consultation, and Dr. Fray F. Marshall for clinical urologic guidance.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 20, 2006.
- Accepted for publication October 12, 2006.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Detection of Additional Primary Neoplasms on 18F-Fluciclovine PET/CT in Patients with Primary Prostate Cancer
- Characterizing and Mitigating Bladder Radioactivity on 18F-Fluciclovine PET/CT
- 18F-Fluciclovine Parameters on Targeted Prostate Biopsy Associated with True Positivity in Recurrent Prostate Cancer
- Update on 18F-Fluciclovine PET for Prostate Cancer Imaging
- Molecular Imaging of Prostate Cancer: Choosing the Right Agent
- Impact of 18F-Fluciclovine PET on Target Volume Definition for Postprostatectomy Salvage Radiotherapy: Initial Findings from a Randomized Trial
- Evaluation of Prostate Cancer with Radiolabeled Amino Acid Analogs
- Comparison of Prostate-Specific Membrane Antigen-Based 18F-DCFBC PET/CT to Conventional Imaging Modalities for Detection of Hormone-Naive and Castration-Resistant Metastatic Prostate Cancer
- Boramino acid as a marker for amino acid transporters
- Anti-1-Amino-3-18F-Fluorocyclobutane-1-Carboxylic Acid: Physiologic Uptake Patterns, Incidental Findings, and Variants That May Simulate Disease
- Interrogating Tumor Metabolism and Tumor Microenvironments Using Molecular Positron Emission Tomography Imaging. Theranostic Approaches to Improve Therapeutics
- 11C-Acetate PET/CT Before Radical Prostatectomy: Nodal Staging and Treatment Failure Prediction
- Biodistribution, Tumor Detection, and Radiation Dosimetry of 18F-DCFBC, a Low-Molecular-Weight Inhibitor of Prostate-Specific Membrane Antigen, in Patients with Metastatic Prostate Cancer
- 2-(3-{1-Carboxy-5-[(6-[18F]Fluoro-Pyridine-3-Carbonyl)-Amino]-Pentyl}-Ureido)-Pentanedioic Acid, [18F]DCFPyL, a PSMA-Based PET Imaging Agent for Prostate Cancer
- In Vivo Imaging of Intraprostatic-Specific Gene Transcription by PET
- Putative Transport Mechanism and Intracellular Fate of Trans-1-Amino-3-18F-Fluorocyclobutanecarboxylic Acid in Human Prostate Cancer
- New Agents and Techniques for Imaging Prostate Cancer
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET
- Novel Tracers and Their Development for the Imaging of Metastatic Prostate Cancer
- Humanized Radioiodinated Minibody For Imaging of Prostate Stem Cell Antigen-Expressing Tumors
- Tumor Cell Metabolism Imaging
- The Impact of Urinary Excretion of 18F-Labeled Choline Analogs
- Biodistribution and Radiation Dosimetry of the Synthetic Nonmetabolized Amino Acid Analogue Anti-18F-FACBC in Humans
- A Preliminary Study of Anti-1-Amino-3-18F-Fluorocyclobutyl-1-Carboxylic Acid for the Detection of Prostate Cancer